
Abstract
Objectives
We aim to describe real-world outcomes from multicenter data about the efficacy of adjunct Heli-FX EndoAnchor usage in preventing or repairing failures during infrarenal endovascular aneurysm repair (EVAR), so-called EndoSutured-aneurysm-repair (ESAR).
Methods
The current study has been assigned an identifier (NCT04100499) at the US National Library of Medicine (https://ClinicalTrials.gov). It is an observational retrospective study of prospectively collected data from seven vascular surgery departments between June 2010 and December 2019. Patients included in the ANCHOR registry were excluded from this analysis. The decision for the use of EndoAnchors was made by the treating surgeon or multidisciplinary aortic committee according to each center’s practice. Follow-up imaging was scheduled according to each center’s protocol, which necessarily included either abdominal ultrasound or radiography or computed tomographic scan imaging. The main outcomes analyzed were technical success, freedom from type Ia endoleaks (IaEL), all-cause and aneurysm-related mortality, and sac variation and trends evaluated for those with at least six months imaging follow-up.
Results
Two hundred and seventy-five patients underwent ESAR in participating centers during the study period. After exclusions, 221 patients (184 males, 37 females, mean age 75 ± 8.3 years) were finally included for analysis. Median follow-up for the cohort was 27 (interquartile range 12–48) months. A median 6 (interquartile range 3) EndoAnchors were deployed at ESAR, 175 (79%) procedures were primary and 46 (21%) revision cases, 40 associated with type IaEL. Technical success at operation (initial), 30-day, and overall success were 89, 95.5, and 96.8%, respectively; the 30-day success was higher due to those with subsequent spontaneous proximal endoleak seal. At two years, freedom from type IaEL was 94% for the whole series; 96% and 86% for the primary and revision groups, respectively; whereas freedom from all-cause mortality, aneurysm-related mortality, and reintervention was 89%, 98%, and 87%, respectively. Sac evolution pre-ESAR was 66 ± 15.1 vs. post ESAR 61 ± 17.5 (p < 0.001) and for 180 patients with at least six-month follow-up, 92.2% of them being in a stable (51%) or regression (41%) situation.
Conclusions
This real-world registry demonstrates that adjunct EndoAnchor usage at EVAR achieves high rates of freedom from type IaEL at mid-term including in a high number of patients with hostile neck anatomy, with positive trends in sac-size evolution. Further data with longer follow-up may help to establish EndoAnchor usage as a routine adjunct to EVAR, especially in hostile necks.
Introduction
Endovascular aneurysm repair (EVAR) has proven to be an effective treatment for the exclusion of abdominal aortic aneurysms (AAAs) becoming the worldwide technique of choice. 1 Patients with challenging neck anatomies, the so-called hostile neck, are at high risk of proximal failure as noted in previous studies.2,3
The Heli-FX EndoAnchor System (Medtronic Vascular, Santa Rosa, CA, USA) was designed to reinforce the seal and fixation of abdominal aortic endografts at the proximal landing zone (PLZ) 4 and prevent PLZ-related adverse events by robust transmural aorto-prosthetic apposition and providing high resistance to pull-out forces mimicking the corresponding mechanical properties of a surgical anastomosis.5,6 Some small cohort studies and reports from single centers have proven its utility during EVAR. 7 Recently, the term EndoSutured aneurysm repair (ESAR) has been proposed to describe the technique. 8
Whilst open surgical repair has been considered the gold standard for fit surgical patients for several years, EVAR continues as the preferred modality but is recognizably vulnerable to variation in patient anatomy, particularly, the aneurysm neck. Previous studies 2 have shown the high risk of type Ia endoleak (IaEL) after EVAR, where hostile neck anatomy (HNA) has been encountered, and alternative endovascular aortic techniques like chimney/fenestrated/branched (Ch/F/B) EVAR have demonstrated validity for AAA treatment in such cases. The high risk of type IaEL is historically linked to lack of coherence to the instructions for use (IFU) in the presence of HNA3,9 albeit in a pre-EndoAnchor era. Of relevance is the recent change in IFU permitting ESAR, where neck length is 4–10 mm when using the Endurant (Medtronic, Santa Rosa, USA) endograft, 10 though analyses of such an approach are yet to emerge. Ongoing studies include the industry-controlled Aneurysm Treatment Using the Heli-FX Aortic Securement System Global Registry (ANCHOR) registry 11 which was designed to assess worldwide use of EndoAnchors, including a very high proportion (more than 80%) of patients with unfavorable aortic neck anatomy.
Methods
The aim of the present study was to describe the real-world outcomes about the performance of EndoAnchors during primary EVAR (primary indication, to prevent future failure, or to treat acute IaELs) or remotely after the primary EVAR (revision) to rescue failure like migration and/or type IaEL from multicenter data so-called the PERU registry.
Patient population
The study was conducted in adherence to the principles of the Declaration of Helsinki; all patients provided consent for inclusion into research. The current study has been assigned an identifier (NCT04100499) at the US National Library of Medicine (https://ClinicalTrials.gov). The design was that of an observational retrospective study using prospectively collected data from seven vascular surgery departments between June 2010 and December 2019. Patients included in the ANCHOR registry were excluded from this analysis. The decision for the use of EndoAnchors was made by the treating surgeon or multidisciplinary aortic committee according to each center’s practice. All on-label cases are included while hostile neck conditions (as defined below) including severely angulated (infrarenal/β angle > 60°) necks were not considered a reason for exclusion.
Definitions
The term “hostile neck” describes several anatomical features, seven of them were included in the current study such as neck length < 10 mm and one or more of the following criteria: infrarenal angle > 60°, thrombus with >2 mm thickness in >50% circumference or circumferential calcification >50%, conical neck (gradual neck dilation >2 mm) along the 10 or 15 mm infrarenal neck length, and diameter >28 mm or asymmetric neck bulge(s).
The primary group included all patients receiving EndoAnchors as a preventive maneuver or for an intraoperative IaEL and the revision group accounts for those cases where EndoAnchors were used (either alone or with adjunctive endografts) to treat a post-EVAR failure (migration alone, IaEL, or IaEL-associating migration).
EndoAnchor-related issues during deployment were described as fracture, loss, or device twisting. These issues were only considered as failures if they were causative of any intraoperative complication or follow-up reintervention. Technical success was denoted as freedom from type I at the end of the primary procedure, where EndoAnchors were deployed, at 30 days follow-up, and during any period of continued follow-up.
Aneurysm-related mortality (ARM) was defined as any death because of post-ESAR rupture or death within 30 days of ESAR (30-day mortality).
Freedom from type IaEL, neck-related, or any reintervention and sac diameter evolution data was provided for all those who reached at least one control imaging follow-up.
Sac regression was defined as aneurysm shrinkage >5 mm, stable sac as all those AAA in between –5 mm and +5 mm and sac growth for those >5 mm.
Endpoints
Primary outcomes
Technical success, freedom from type IaEL (overall, and also primary and revision groups), and sac diameter evolution, herein comparison of maximum pre-operative versus final sac diameters at the latest follow-up point, for those with a minimum of six months imaging.
Secondary outcomes
Description of complications, reinterventions, adjunct procedures, EndoAnchor deployment issues, aneurysm-related, and all-cause mortality.
EVAR procedure
Anatomical data were obtained pre- and postoperatively. Dedicated software was used to complete the three-dimensional (3D) reconstruction using the center-line method for the measurements. Planning of the aortic endograft in relation to the proximal seal was undertaken according to the sizing parameters of each device, given that some devices use outer-to-outer, whilst others use inner-to-inner wall measurements of diameter. All endografts were implanted in a surgical theatre equipped with a conventional C-arm or in a hybrid endovascular operating room. The standard treatment protocol included balloon dilatation at the proximal neck and a prolonged dilatation in case of intraoperative IaEL before any other adjunctive maneuver, with or without the use of cuffs if there was any perception of suboptimal neck length coverage.
Heli-FX EndoAnchor system
The technique and other aspects regarding implantation have been previously described in detail. 4 Briefly, the EndoAnchor applier is advanced through a 16-F steerable sheath, the Heli-FX Guide, and each EndoAnchor (4.5 mm in length and 3 mm in diameter) is implanted in a controlled two-stage process to allow, if necessary, the retraction of the EndoAnchor and the repositioning in the desired position before final deployment. Each deployment was planned preoperatively according to clock face orientation. 12
Surveillance protocol
Computed tomography angiography (CTA), abdominal ultrasound, and plain abdominal radiography of the device in two projections were performed as appropriate before hospital discharge, and follow-up imaging was scheduled according to each center’s protocol. Unscheduled CTA was performed only in cases of complications and/or at surgeon/center discretion.
Statistical analysis
Categorical variables are presented as counts and percentages. Continuous variables are presented as mean ± standard deviation if the data are normally distributed, or as median with interquartile range (IQR) if the data are skewed. Continuous data were compared with non-parametric Mann–Whitney U-test or Student’s t-test as appropriate. Categorical variables were compared with Pearson’s chi square test. Estimations of mortality, freedom from IaEL, and reintervention rates were performed by Kaplan–Meier life table analysis. p-Values were considered significant for values <0.05. Data were analyzed using SPSS 25.0 (IBM, Armonk, NY, USA).
Results
Two hundred and seventy-five patients underwent ESAR in the participating centers during the study period.
Thirty-six patients had been included in the ANCHOR registry, and another 18 patients who underwent EVAR with off-label device deployments (13 planned chimneys and 5 funnel technique EVAR—combined use of standard and proximal thoracic endograft to treat a large diameter infrarenal AAA) were excluded, and therefore, 221 patients were finally included for analysis.
Baseline characteristics of the whole series, primary (175, 79%) and revision groups (and a comparison between them), are shown in Table 1, where 199 (90%) of patients were considered high-risk by ASA classification (ASA 3–4). Conical shape was the most frequent hostile neck condition, noted in 82 (38%) overall patients’ series.
Demographics and neck anatomy description.
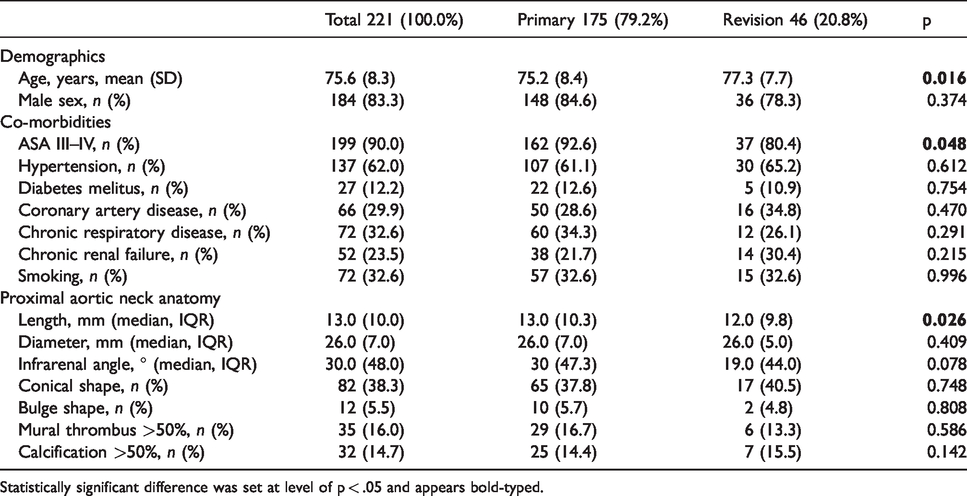
Statistically significant difference was set at level of p < .05 and appears bold-typed.
Table 2 describes the operative data; 193 (87.3%) received suprarenal fixation endografts, with the Endurant endograft (Medtronic, Santa Rosa, CA) being the most frequently used; 112 (50.7%), and with less frequency other Endografts such as Incraft (Cordis Corporation, Bridgewater, NJ) or E-Tegra (JOTEC GmbH, Hechingen, Germany) in 10 and 3 cases, respectively.
Operative details.

Statistically significant difference was set at level of p < 0.05 and appears bold-typed.
aN.A.: not analyzed.
The median number of EndoAnchors deployed per patient was 6 (IQR 3). The median device oversize applied at the PLZ for the whole group was 19.5% IQR 9 with no statistical difference between groups.
Technical success and IaELs
The initial technical success overall was 89.1% (n = 197) (Table 3) as 23 patients had persistent type IaEL at final angiography, all of them were managed conservatively with the expectation of eventual spontaneous resolution. One of these patients suffered immediate post-operative death due to multi-organ failure. Thirty-day technical success was 95.5% (n = 211), as 19 of these endoleaks showed spontaneous resolution at first control CTA. Six patients presented with proximal type IaEL at first CTscan, four from the previous type IaEL at final angiography and two new not noticed at the end of the index procedure. Two received aortic banding by open surgery, three were treated with a large balloon-expanding stent, and the remaining one was treated conservatively showing spontaneous resolution at six-month CT-scan. Follow-up primary technical success was 95.5% (n = 211). During a median follow-up of 27 (IQR 12–48) months, six more IaELs (three receiving surgical treatment and three of them conservative due to the absence of sac enlargement) and four IaELs appeared, all treated with iliac endograft extension.
Technical success results of EndoAnchors placements in 221 patients.

aIaEL: type Ia endoleak.
bOne patient with IaEL died intraoperatively and three patients died during first month of follow-up.
cEV: endovascular.
dIbEL: type Ib endoleak.
eThis patient was kept under close observation because the aneurysm maximum diameter remained stable at 71 months of follow-up. Statistically significant difference was set at level of p < 0.05.
Freedom from IaEL at 24 months was 94% for the whole group, 96% for primary cases, and 86% for revision cases, with statistically significant difference between them (p = 0.036, log-rank; Figure 1).

Kaplan–Meier estimation of freedom from type Ia endoleak for the three groups: global group, primary and revision arms; at 24 months of follow-up.
Freedom from neck-related reinterventions and any reintervention was 98% and 87%, respectively, at 24 months (Figure 2).
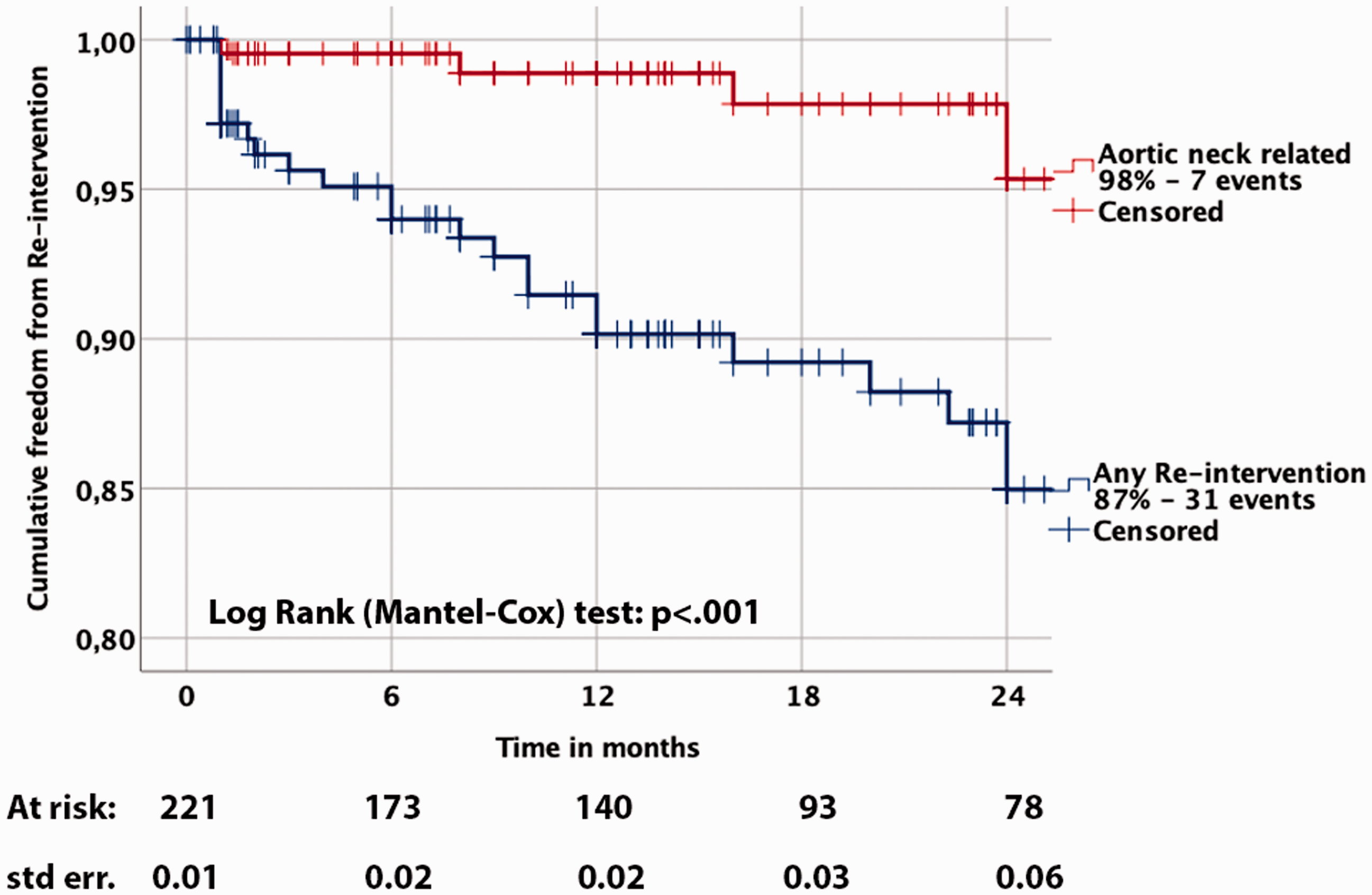
Kaplan–Meier estimation of the freedom from proximal neck-related and any reintervention of the entire cohort, at 24 months of follow-up.
EndoAnchor deployment issues were encountered in 10 patients, namely four fractures, four losses, and two twisted devices (Table 3); none of them was causative of any type of intraoperative and/or follow-up complication or failure.
Sac evolution
Analysis of sac evolution for the whole series showed pre-ESAR sac size to be 66.3 mm ± 15.1 versus post-ESAR 61.7 mm ± 17.5 (p < 0.001, paired t-test) (Figure 3) and for those 180 patients with at least six-month imaging follow-up (41.1%) showed sac regression, whereas 51.1% remained stable, totaling 92.2% (n = 166), and sac growth was encountered in 7.8% (n = 14) (Table 4) and Figure 4.
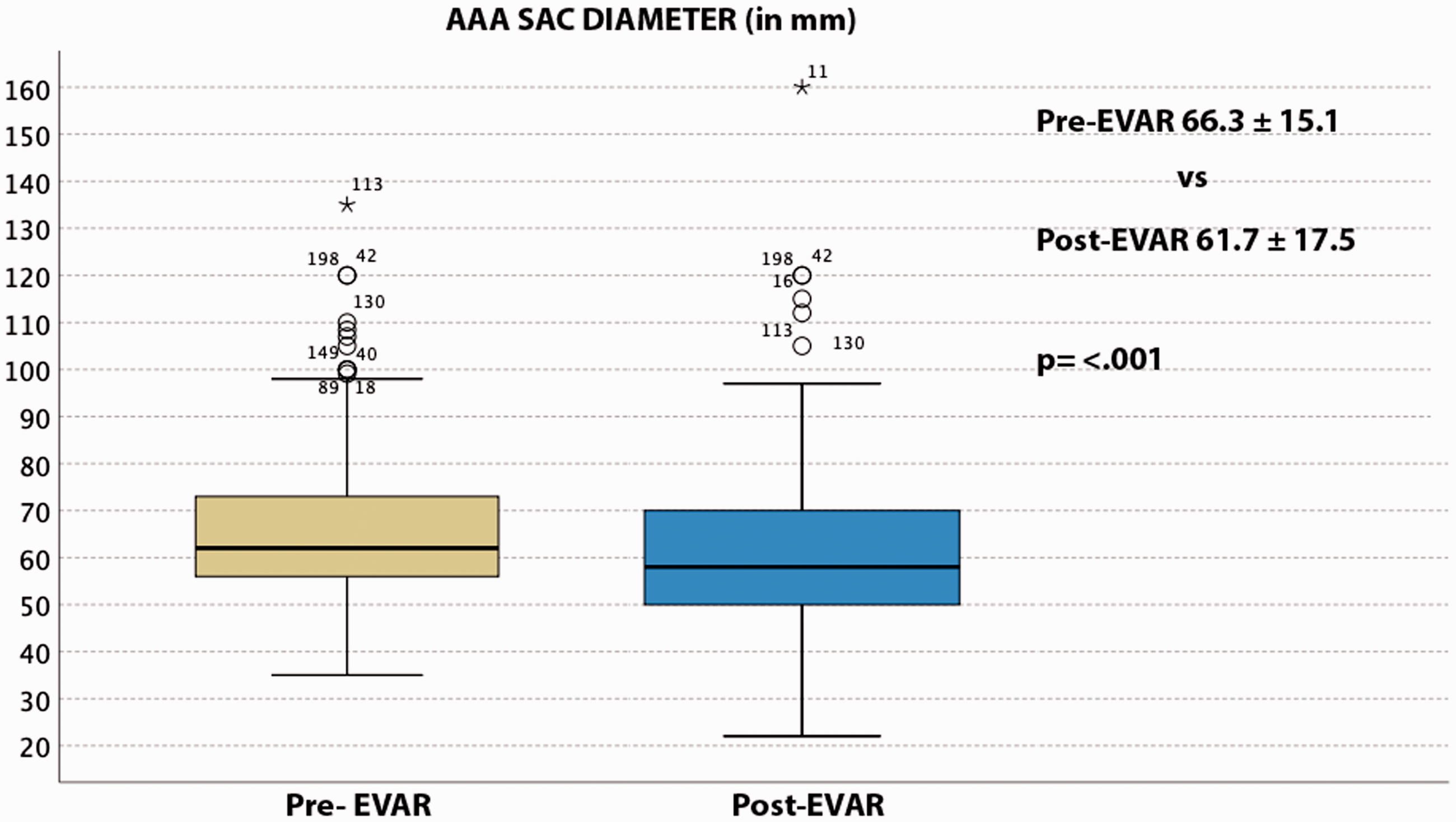
Box plot comparing sac sizes pre and post-EVAR with EndoAnchors for the global series.
Sac evolution in 180 patients with at least six-months imaging follow-up.

Statistically significant difference was set at level of p < 0.05 and appears bold-typed.
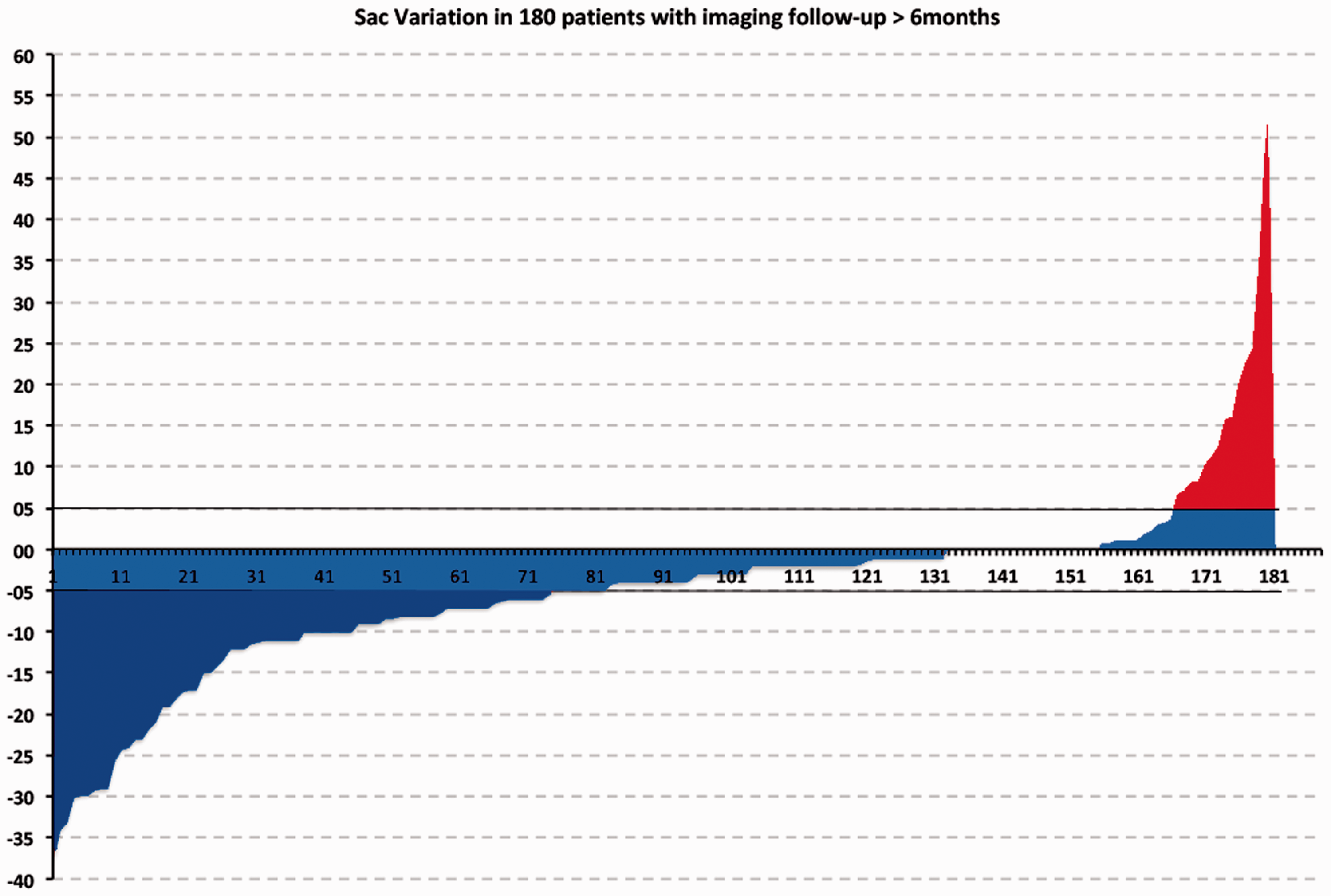
Sac variation in 180 patients with at least six-month imaging follow-up.
Mortality
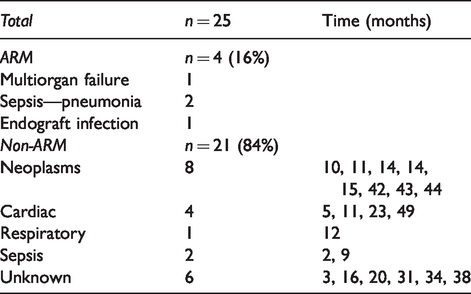
Cumulative survival and aneurysm-related survival were found to be 89 and 98%, respectively, at two years as shown in Figure 5. There were 25 deaths (11.3%) described for the whole series. Table 5 describes specific causes of mortality and the time of occurrence.
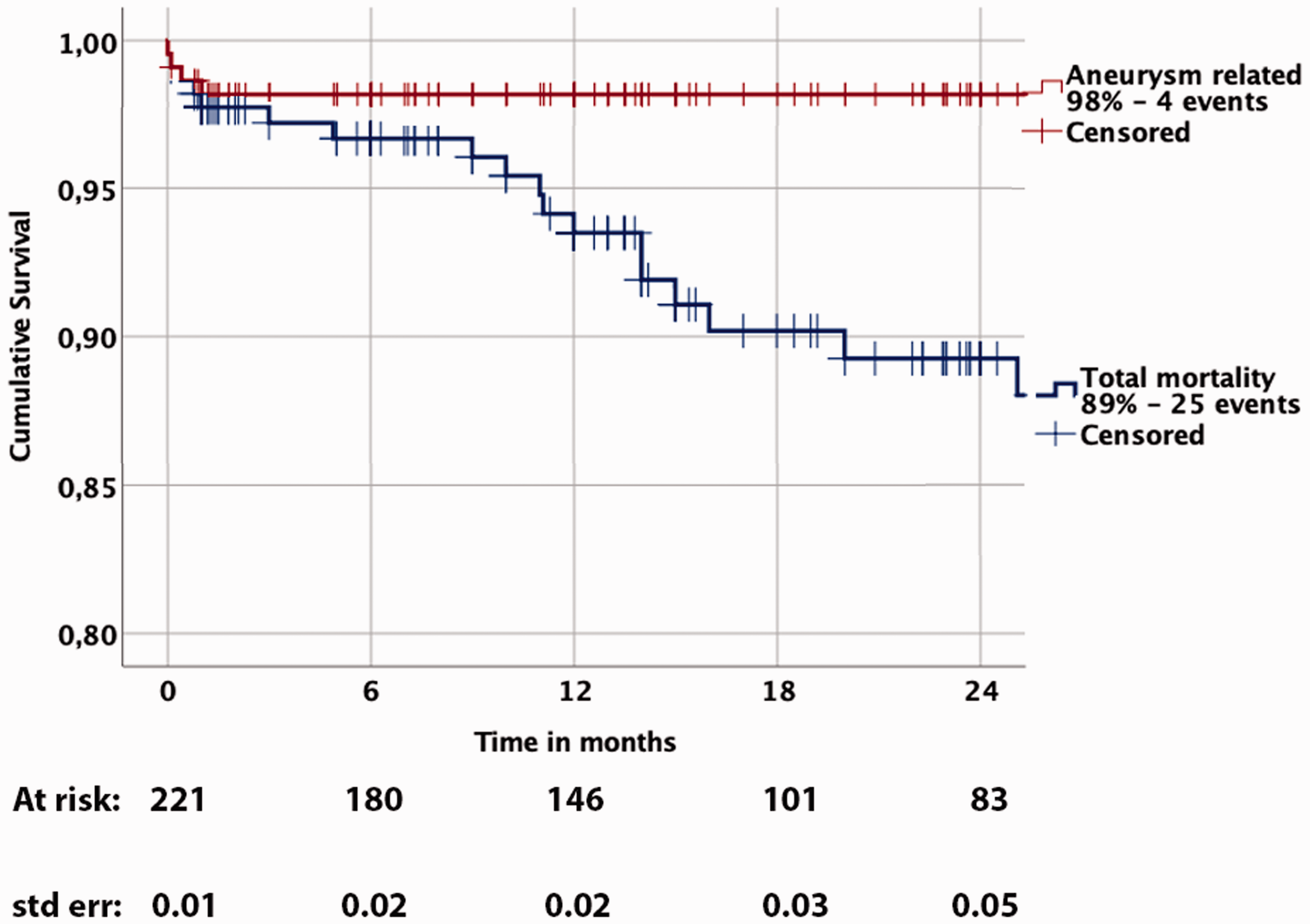
Kaplan–Meier estimation of cumulative survival and aneurysm-related mortality at 24 months.
Mortality data.
Discussion
Despite the inflow of results from industry-sponsored studies such as the ANCHOR registry, 11 current recommendations from the ESVS guidelines for the treatment of AAAs indicate secondary usage of the Heli-FX EndoAnchor System and usage in the juxtarenal AAA context within trial constraints. The recent meta-analysis by Qamhawi et al. 13 echoed this, stating that EndoAnchor use in routine clinical practice could not be recommended without support from trial data. However, this flies in the face of the fact that such new technology has already become part of our endovascular armamentarium; 14 use of such advances get (safely) entrenched into practice with supportive data indicating that type IA endoleakage is reduced with EndoAnchor usage,12,15 whether the desirable trials occur or not. This is exemplified by the uptake of fenestrated endovascular aneurysm repair (FEVAR) and chimney EVAR. Whilst common EndoAnchor usage seems somewhat away from a mainstream recommendation, continued data collection and reporting on those patients in EAs have been deployed should contribute to the body of knowledge in this area.
To our knowledge, the PERU registry is one of the largest physician-initiated series in the literature describing the adjunctive use of EndoAnchors for primary and revision indications in combination with standard EVAR. The current registry intends to run in parallel with the ANCHOR registry and likewise includes high rate of patients with HNA and a substantial number of patients at high risk for open repair. The overall 94% freedom from IaELs achieved at mid-term follow-up (24 months) in both primary and revision arms is in accordance with the same percentage described in the ANCHOR registry at a similar follow-up period.
The 89% all-cause survival rate at two years correlates with the previous studies. Overall mortality in the current study was annotated for 25 patients (Table 5), with neoplasms being the leading cause of non-ARM. These results were not affected by the current COVID-19 outbreak, as analysis was stopped in early January 2020; however, as continuous reporting on the registry results is warranted, this will be described factoring in any suggested/accepted new standards on pandemic reporting.
Interestingly, a considerable number of patients with persistent IaEL at completion angiography and accepted as such resolved spontaneously, one of them showing recurrence and treated conservatively due to absence of sac expansion. This is not an unusual finding, though. Persistent type IaEL at completion angiography has been described for standard EVAR,16,17 FEVAR, 18 ESAR therapy 19 and in a higher rate, ChEVAR. 20 Although this conservative approach is supported by other studies which also indicate that not all on-table IaELs need active intervention, 16 this decision needs to be individually analyzed, and the risk of rupture needs to be taken into consideration.
The proposed benefits of the use of EndoAnchors are not only related to the reduction in IaEL or migration rates, but a decreased rate of neck dilatation, 21 demonstrating a protective neck effect of the Heli-FX device as has been recognized. Moreover, the recent focus on correlation on sac regression and improved survival 22 may also be a benefit derived from the use of EndoAnchors, as Muhs et al. 23 described in a propensity-matched cohort of patients treated by EVAR with and without prophylactic EndoAnchors with HNA conditions; a significant higher sac regression was noted at two-year follow-up in favor of the EndoAnchor group, probably due to immediate control of what would likely be unnoticed IaELs despite standard CTA after standard endovascular treatment.
Understanding the anatomical situations in which EndoAnchor placements are unfavorable, related to aortic wall penetration (AWP) is mandatory, as the success of ESAR is strictly proportional to achieving the greater strength in fixation with robust seal by optimal penetration of the aortic wall. Besides, much controversy comes derived from the 4-mm neck length CE approval; however, one should think that a degree of apposition might come from the lower aspect of what is considered the real neck (in some patients) and that may introduce a better concept such a “sealing zone.”
A previous study derived from the ANCHOR registry about a group of patients with IaELs (revision cases) indicated 48% of EndoAnchors lacking adequate AWP, demonstrating that there is still much to learn on the appropriate use of the device from an anatomical and technical perspective. 24
Although ESAR could be interpreted as an easy technique, it should not be considered always as such. 25 The chance of inappropriate patient selection, use, failure, complications as in every endovascular procedure is extremely related with experience, and thus, such condition should be considered if one wants to implement the technique in daily routine. Some interesting in vitro studies analyze mechanical forces related to EndoAnchor placements.26,27 Moreover, the importance of proper use may be related to the economic gain in terms of less neck-related reinterventions during follow-up, 28 but an economic assessment was outside the scope of this study.
ESAR should not be considered a competitive but indeed a complementary technique that is both useful and accessible/available when hostile neck anatomic features are encountered, and correct technical deployments are accomplished,4,29 avoiding potential complications of other complex techniques.30,31
We aim to keep data inclusion open for all centers that want to participate on this multicenter collaboration.
Limitations
Despite the retrospective nature of the study, this is a prospective multicenter collaboration from those centers achieving some experience with the Heli-FX EndoAnchor System which could induce a bias, particularly as this is undertaken effectively as a single cohort study without a control EVAR group without EndoAnchors. Moreover, the study results are limited to two years follow-up.
The large time frame for patient inclusion does not correlate with the still mid-term analysis, and this is explained by two centers being early adopters of the technique including very low number of patients in those early years (2011–2015); then the vast majority of patients are included in the latest period time-frame (2015–2019).
The follow-up imaging is performed as per center discretion; thus, there is no imaging core laboratory for centralization. However, all centers included have already been involved in several single and multicenter publications on EVAR topics making our data reliable and clearly representing real-world conditions.
Conclusions
This real-world registry demonstrates adjunct EndoAnchor usage at EVAR achieves high rates of freedom from type IaEL at mid-term including in a high number of patients with HNA, with positive trends in sac-size evolution. Further data with longer follow-up may help to establish EndoAnchor usage as a routine adjunct to EVAR, especially in hostile necks.
Footnotes
Declaration of conflicting interests
Andrés Reyes Valdivia, Giovanni Pratesi, Michel Reijnen, Giovanni Tinelli, Ross Milner, Yamume Tshomba and Jean Paul de Vries are consultants for Medtronic.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.