
Abstract
Objectives
The significant effects on the treatment of severe carotid stenosis by carotid endarterectomy have been widely recognized. However, it is controversial whether patients with severe contralateral carotid stenosis or occlusion (SCSO) can benefit from carotid endarterectomy surgery. This study aimed to estimate the SCSO effects on early outcomes after carotid endarterectomy with selective shunting.
Methods
Between August 2011 and October 2019, a total of 617 patients who underwent carotid endarterectomy with selective shunting were analyzed. SCSO was defined as >70% luminal narrowing of the contralateral extracranial carotid stenosis or occlusion. Of these patients, 116 were categorized into an SCSO group while the rest were assigned to the non-SCSO group. Primary study outcomes were the occurrence of major adverse events, defined as stroke, all-cause mortality, and myocardial infarction during the perioperative period after carotid endarterectomy. Traditional multivariable logistic regression model and logistic regression model adjusted for propensity scores were used to estimate the SCSO effects on primary outcomes. Interaction and stratified analyses were conducted according to age, sex, comorbidities (hypertension, diabetes), preoperative neurological deficit, preoperative symptoms, and shunt use.
Results
Mean age was 68.5 ± 9.2 years (86.1% men). Overall major adverse events rate within 30 days was 2.5%. Major adverse events rates in SCSO and non-SCSO groups were 9.5% and 1.6%, respectively. This difference was statistically significant (p < 0.001). In multivariable regression analysis, patients with SCSO had a higher risk of major adverse events (non-SCSO vs. SCSO: aOR 5.05 [95% CI, 1.78–14.55]). In 342 propensity score matched patients, results were consistent (propensity score: aOR, 3.78 [95% CI, 1.13–12.64]).
Conclusions
SCSO is an independent predictor of 30-day major adverse events. Whether these patients with SCSO are suitable for carotid endarterectomy should be carefully considered.
Introduction
Carotid endarterectomy (CEA) has proven to be an effective intervention to prevent stroke in patients with symptomatic and asymptomatic high grade internal carotid artery stenosis.1–3 Among the potential risk factors that influence outcomes after CEA, severe contralateral carotid stenosis or occlusion (SCSO) status has always been studied for its significance. In approximately 10% of patients of carotid stenosis, there is also an SCSO.4,5
However, the reported effects of SCSO on perioperative stroke after CEA are controversial. Several multicenter clinical trials showed that patients with preexisting SCSO have an increased risk of perioperative stroke after CEA.5–7 It is speculated that the increased stroke incidence in SCSO patients may be due to their impaired cerebral functional reserves. 6 While many single-center studies reported different results,8–11 Jeong et al. 9 have found no significant differences in stroke or death incidence after CEA between non-SCSO and SCSO groups, and preexisting SCSO was not associated with an increased risk of perioperative or long-term stroke or death occurrence.
Reasons for the differing results may be related to ethnic disparities, sample size, whether or not shunt was implanted during surgery, etc. In addition, the interaction of SCSO after CEA with other cerebrovascular risk factors such as age, hypertension, and diabetes is still unknown. Therefore, this study aimed to compare 30-day outcomes after CEA with selective shunting between SCSO and non-SCSO groups. The effects of other classical cerebrovascular risk factors on the association were also evaluated by interaction and stratified analyses.
Methods
Study design and participants
In accordance with the STROBE statement, we retrospectively reviewed data from all patients who underwent CEA with selective shunting at our institution from August 2011 to October 2019. Our institution is the Neurosurgery Department of Zhejiang Provincial People’s Hospital. Our hospital is one of the largest public hospitals with 2830 beds and four campuses in Zhejiang Province.
Clinical characteristics and morphologic variables including age, sex, history of smoking, drinking, comorbidities (diabetes mellitus, hypertension, coronary artery disease (CAD)), preoperative symptoms, preoperative neurological deficits, degree of bilateral carotid artery stenosis, and intraoperative monitoring (IOM) were collected.
Patients diagnosed with carotid stenosis by digital subtraction angiography (DSA) and/or magnetic resonance angiography (MRA) and/or computed tomography angiography (CTA) at the neurosurgery department in our institute were retrospectively screened. The diagnosis and the vascular morphological features of carotid stenosis were based on the guideline from the North American Symptomatic Carotid Endarterectomy Trial (NASCET). 12 The definition of severity of stenosis was classified as follows: those with moderate stenosis, defined as <70% of the luminal diameter, and those with severe stenosis, defined as stenosis of 70–99%. Surgical criteria were as follows: 50–99% luminal narrowing in patients with symptomatic carotid stenosis and >70% in those with asymptomatic carotid stenosis. SCSO was defined as >70% luminal narrowing of the contralateral extracranial carotid stenosis or occlusion based on the diagnostic criteria described above. Patients were considered to be symptomatic if they had one of the following neurologic events within the previous six months before surgery: transient ischemic attack (TIA), amaurosis fugax, or non-disabling stroke ipsilateral to significant carotid stenosis.13,14 Preoperative neurological deficit was graded with the modified Rankin scale (mRS) as good (mRS score < 3) or poor (mRS score ≥3). 7 Patients were stratified by SCSO (non-SCSO group vs. SCSO group) and retrospectively analyzed. We only included the first surgery for bilateral carotid procedures. Patients were excluded if they had chronic atrial fibrillation, paroxysmal atrial fibrillation within the preceding six months, myocardial infarction within the previous 30 days, or unstable angina.
Outcome events and definitions
The primary endpoint was the occurrence of major adverse events (MAEs), the composite of fatal or nonfatal stroke (ischemic or hemorrhagic), myocardial infarction (MI), and all-cause mortality within 30 days after CEA with selective shunting. Secondary endpoints were TIA, cranial nerve injury, and incision-related complications within 30 days after surgery.
Postoperative stroke was defined as a clinical neurological dysfunction over 24 h after operation, according to NASCET. 12 Myocardial infarction was defined by a cardiac troponin I level twice the upper limit of the normal range or higher according to the center’s laboratory, in addition to either chest pain or symptoms consistent with ischemia or electrocardiographic evidence of ischemia, including new ST segment depression or elevation, or elevation >1 mm in two or more contiguous leads according to the core laboratory. 15 Cranial nerve injury was identified if postoperative clinical examination showed symptoms and signs consistent with it. Incision-related complications included incision infection, subcutaneous hematoma requiring surgical treatment, and poor wound healing. Patients were assessed by a neurologist following surgery and before discharge.
Surgical procedures
Carotid revascularization followed the guidelines of the European Society of Vascular and Endovascular Surgery. 16 All CEAs were performed under general anesthesia. Surgery type was either primary closure or patch angioplasty as chosen by the surgeon. All patients received CEA surgery for the first time. Patients received 100 mg oral aspirin or 75 mg clopidogrel daily from five days before surgery, until at least two months after surgery. After the procedure, all patients were taken to postoperative intensive care unit until hemodynamically stable.
IOM and shunting selection
For intracranial blood perfusion observation during CEA, different IOM modalities including transcranial Doppler (TCD), somatosensory evoked potentials (SEP), stump pressure (SP), electroencephalography (EEG), and/or multimodal monitoring modalities were adopted during surgery for a selective use of intraluminal shunting. In this study, patients received shunting prospectively based on any of the following conditions according to various CEA monitoring modalities: (1) carotid artery SP ≤50 mmHg, (2) TCD showing the middle cerebral artery blood flow velocity drop by >50% and no effect after elevating blood pressure, (3) SEP monitoring showing 50% reduction in amplitude and no effect after elevating blood pressure, and (4) continuous intraoperative EEG showing a slowing in the alpha and beta frequencies or 50% reduction in amplitude.
Statistical analysis
Patients with missing data were excluded from analysis. Mean ± standard deviations were used for quantitative variables. Qualitative variables were expressed as frequency and percentage. Data were compared with a U test for continuous variables and a chi-square test or Fisher’s exact test for categorical variables. The association between multiple risk factors and 30-day MAEs was assessed by univariate analysis, and multivariate analyses were performed by regression model. Odds ratios (ORs) with 95% confidence intervals (CIs) comparing event rates between groups (non-SCSO group vs. SCSO group) were derived. We adjusted multivariable logistic regression models for all the covariates. Given the differences in baseline characteristics among eligible participants in the two groups (non-SCSO group vs. SCSO group), propensity-score matching was additionally employed to identify a patient cohort with similar baseline characteristics to minimize selection bias. SCSO group patients were matched 1:2 to non-SCSO on propensity score to overcome the bias arising from the lack of randomization and the heterogeneity of the two groups by using a greedy, nearest neighbor matching algorithm, and all the baseline characteristics were chosen for the matching. Caliper size was 0.2. Covariate balance between groups was assessed by using standardized differences (Table 1). We estimated the standardized difference of all baseline covariates before and after matching. Accordingly, a standardized difference <0.1 indicates a relatively small imbalance. 17 In the matched cohort, we further adjusted the propensity score using a Cox proportional-hazards regression model.
Baseline characteristics before and after propensity-score matching.

Values are presented as mean ± standard deviation or number (%).
SCSO: severe contralateral carotid stenosis or occlusion; non-SCSO: without severe contralateral carotid stenosis or occlusion; CAD: coronary artery disease; mRS: modified Rankin scale; TIA: transient ischemic attack; IOM: intraoperative monitoring.
All tests were two-sided, and statistical significance was set at p < 0.05. All analyses were performed with the statistical software package R (http://www.R-project.org, The R Foundation) and EmpowerStats (http://www.empowerstats.com, X&Y Solution, Inc., Boston, MA).
Follow-up
After discharge, follow-up was performed in outpatient clinics or per telephone interview. Patients lost to follow-up were not included in this study.
Results
Altogether, 617 cases who underwent CEA with selective shunting procedures at Zhejiang Provincial People’s Hospital between August 2011 and October 2019 were identified according to the inclusion criteria. The SCSO group consisted of 116 patients (18.8%), whereas the non-SCSO group included 501 patients (81.2%). During the study period, staged bilateral CEAs were performed on 97 patients, but only the first CEA surgery was included in our analysis. We excluded 25 patients with atrial fibrillation, 28 patients who died before the procedure, 57 patients with insufficient information, and 46 patients who were lost to follow-up. This left us with 617 cases which represented our study cohort (Figure 1).

Patient flow chart.
Baseline characteristics before and after propensity score matching
Patients’ baseline characteristics before and after matching are shown in Table 1. In the overall study population, mean age was 68.5 ± 9.2 years old. In most instances, patients who underwent CEA were more likely to be male (86.1%) and smoke (69%). Simultaneously, they were found to have a higher burden of hypertension (75.9%). Before propensity score matching, between groups analysis showed that patients in the SCSO group were slightly older (70.7 ± 8.9 vs. 68.0 ± 9.1, p = 0.005), drinkers (197 (39.3%) vs. 60 (51.7%), p = 0.015), had a worse neurological deficit (23 (4.6%) vs. 15 (12.9%), p = 0.002), and presented a significantly higher incidence of CAD (84 (16.8%) vs. 32 (27.6%), p = 0.007) than patients in the non-SCSO group. There were no significant differences in other characteristics including sex, diabetes, hypertension, smoking, preoperative symptoms, shunt implantation, or IOM. By propensity score matching, 114 patients in SCSO group were matched with 228 patients in non-SCSO group. After matching, the baseline characteristics were not statistically different. Standardized differences varied between 0.00 and 0.11 for all variables, indicating small differences between the two groups (p > 0.05) (Table 1).
Univariate analysis
Univariate analysis (Table S1) revealed an increased 30-day MAEs risks for CEA in the SCSO group (OR, 6.46 [95% CI, 2.54–16.44], p = 0.002). Furthermore, patients with a more severe neurological deficit (mRS ≥ 3 vs. mRS < 3) had an elevated risk of perioperative MAEs (OR, 6.11 [95% CI, 2.08–18.00], p = 0.004). Patients with CAD also had a higher risk of MAEs after CEA (OR, 3.30 [95% CI, 1.30–8.40], p = 0.012).
Clinical outcome
Among the 617 cases, the MAEs endpoint occurred in 19 cases. Sixteen cases had 30-day stroke, all occurring within the first week after surgery, including 14 cases of cerebral ischemia, and two of cerebral hemorrhage. One case of death occurred 30 days after surgery due to cardiac arrest. Two cases had myocardial infarction, amounting to an overall 2.5% MAEs rate (Table 2). Primary outcome 30-day rates in the SCSO and non-SCSO groups were 9.5% and 1.6%, respectively. This difference was statistically significant (p < 0.001). After matching, this difference was still relevant (p = 0.012). Secondary outcomes occurred in 27 cases, of which 4 had TIA, 10 cranial nerve injury, 12 ecchymoma, and 1 poor wound healing within 30 days after surgery. Postoperative TIA incidence rate was statistically different between groups (SCSO group vs. non-SCSO group; 0.2% vs. 2.6%; p = 0.022), but there was no statistical difference on secondary outcomes between the two groups (SCSO vs. non-SCSO).
Periprocedural complications (no. of events within 30 days) before and after propensity-score matching.
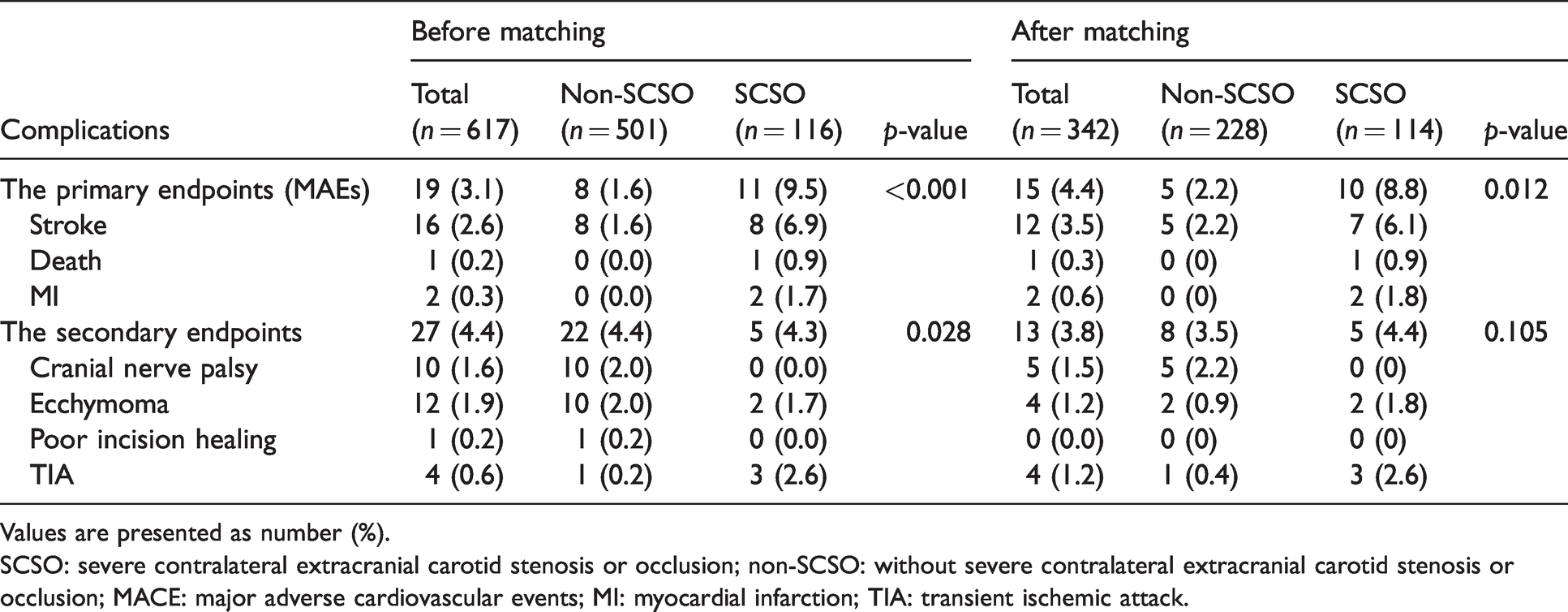
Values are presented as number (%).
SCSO: severe contralateral extracranial carotid stenosis or occlusion; non-SCSO: without severe contralateral extracranial carotid stenosis or occlusion; MACE: major adverse cardiovascular events; MI: myocardial infarction; TIA: transient ischemic attack.
SCSO effect on 30-day MAEs after CEA
Kaplan–Meier analysis showed that the MAEs-free survival rate within 30 days among patients with SCSO was significantly (p = 0.0002) lower than in those without SCSO (Figure 2). Multivariable logistic regression analysis revealed that SCSO patients (crude OR, 6.46 [95% CI, 2.54–16.44]) had higher MAEs rates. After adjusting for confounding variables, 30-day MAEs risk was decreased in SCSO subjects (aOR, 5.08 [95% CI, 1.78–14.55]). This effect was similar among patients in the propensity score-matched cohort (Table 3). The multivariable logistic regression analysis of the propensity score-matched cohort demonstrated that patients with SCSO had an increased 30-day MAEs rate in comparison to those without (crude OR, 4.66 [95% CI, 1.45–14.98]). After adjusting for propensity scores, 30-day MAEs risk was decreased in subjects with SCSO (aOR, 3.78 [95% CI, 1.13–12.64]). The interaction analysis revealed no interactive role in the association between SCSO and 30-day risk of MAEs (Table 4).
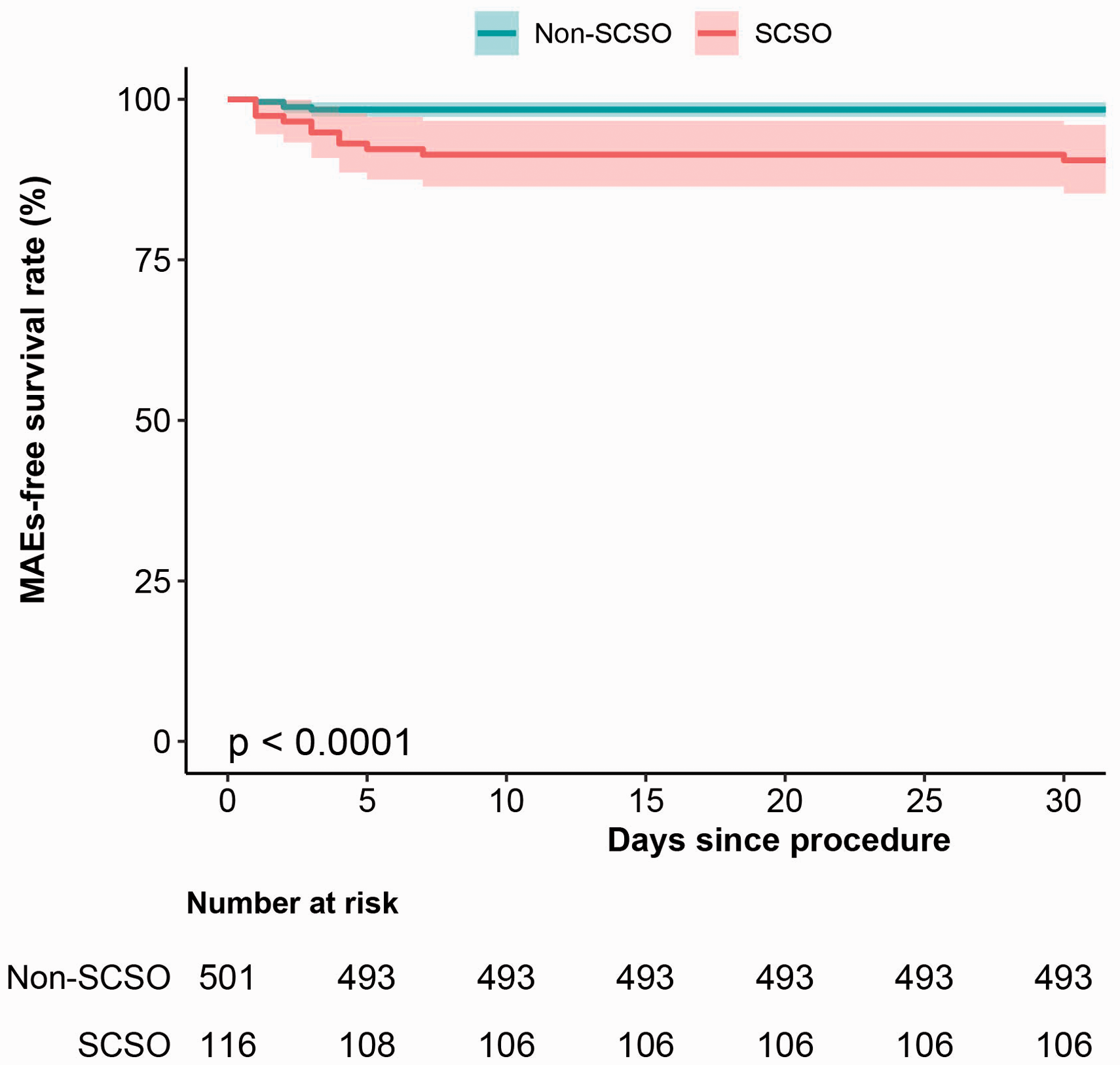
Kaplan–Meier analyses of cumulative MACE-free rates in the SCSO group and non-SCSO group within 30 days after CEA surgery.
Multivariable logistic regression models evaluating the effect of SCSO on the primary outcomes before and after propensity score matching.

SCSO: severe contralateral extracranial carotid stenosis or occlusion; non-SCSO: without severe contralateral extracranial carotid stenosis or occlusion; OR: odds ratio; CI: confidence interval.
aMutually adjusted for age, sex, hypertension, diabetes, coronary artery disease, smoking, drinking, surgical side, ipsilateral degree of stenosis, neurological deficit, preoperative symptoms, surgical technique, shunt implantation, and intraoperative monitoring.
Effect of age, sex, hypertension, diabetes, preoperative symptoms and shunt implantation on the association between the presence of SCSO and MAEs.

aEach stratification adjusted for all the factors (age, sex, hypertension, diabetes, coronary artery disease, smoking, drinking, surgical side, ipsilateral degree of stenosis, neurological deficit, preoperative symptoms, surgical technique, shunt implantation, and intraoperative monitoring) except the stratification factor itself.
Discussion
In this retrospective cohort study, SCSO was significantly associated with 30-day MAEs risk. Subjects with SCSO had a 4.08-fold higher risk of MAEs rates within 30 days than those without. Although participants with SCSO were slightly older, drinkers, had a more severe neurological deficit, and presented a significantly higher incidence of CAD than controls, even after adjusting for these risk factors, the association remained significant. Moreover, after a propensity score-matched analysis, in the matched cohort of patients with similar baseline characteristics, patients with SCSO had a 2.78-fold higher MAEs risk within 30 days than those without SCSO after adjustment for a propensity score, which adds to the credibility of our findings. Meanwhile, we found no interactive role in the association and higher MAEs risk, suggesting that SCSO is associated with a worse perioperative prognosis and outcome independent of other vascular risk factors.
Many multicenter studies and systematic reviews have suggested that SCSO is associated with increased risk of adverse preoperative events.18–21 In a study on 3092 CEAs performed across 11 hospitals from 2003 to 2007, Goodney et al. 22 found that contralateral carotid occlusion was an independent predictor of perioperative stroke/death (OR, 2.8 [95% CI, 1.3–6.2]). Cheng et al. 21 revealed that patients with contralateral carotid occlusion had an increased risk of perioperative neurological complications, including stroke and TIA when compared to those without contralateral occlusion (OR, 1.20 [95%CI, 1.11–1.31]), which is consistent with our results. However, the controversy about increased perioperative and early postoperative risk in patients undergoing CEA with SCSO is still present. Several single-center studies reported no statistically significant difference in the perioperative prognosis of patients with contralateral carotid artery disease after CEA.8,23 A French study 8 showed that the presence of contralateral carotid stenosis was not predictive of postoperative events, and an Italian one 24 reported that concomitant occlusion of the contralateral carotid artery was not associated with an increased risk of perioperative cardiological or neurological adverse events. However, these study cohorts were small, with groups with contralateral carotid artery disease making only 6–13% of the entire cohort, potentially resulting in a type II error. Moreover, none of the above studies adjusted for confounding factors, and there may also be ethnic differences in environmental and genetic factors. The World Health Organization’s Department of Measurement and Health Information claims that there is a significant difference in MAEs risk between different ethnic groups, with Asian populations having higher stroke incidence than MI incidence in comparison to Western populations.25,26
During carotid clamping, cerebral perfusion is maintained from the contralateral internal carotid artery or the vertebrobasilar system via the circle of Willis. 20 In SCSO patients, both impaired cerebrovascular reactivity and limited functional reserve likely contribute to increased risk for cross-clamp related cerebral ischemia and potential infarction. Sam et al. 27 have reported that unilateral carotid stenosis affects the vascular reserve of both brain sides not only the hemisphere ipsilateral to the occlusion but also the contralateral. Bilateral severe carotid stenosis leads to a further decrease in bilateral cerebral function reserves and intolerance to ischemia. Oka et al. 28 demonstrated that cerebral blood flow and cerebrovascular reactivity increased in both hemispheres three to six months after carotid stenosis treatment, which further supports the theory of hemodynamic impairment in SCSO patients. Consistent with the literature,29,30 unstable perfusion created an increased demand for shunt implantation as a cerebral protection method during CEA in SCSO patients.
There is controversy concerning the need for shunt implantation in SCSO patients during CEA. Strategies currently including routine shunting, 31 selective shunting, 32 and no shunting 33 have been adopted. Goodney et al. 34 have reported that shunt use for patients with contralateral carotid artery occlusion is associated with fewer complications, but only if the surgeon used a shunt as part of his or her CEA routine practice. In our center, the surgeon performed selective shunting based on intraoperative cerebral perfusion monitoring including TCD, SEP, SP, EEG, and/or multimodal monitoring modalities avoiding arterial dissection, distal embolization, and acute occlusion. The surgeon in our department had ample experience in selective shunting. In our study, shunting rates were 10.2% in the non-SCSO and 10.3% in the SCSO group, respectively, and not statistically different.
Surprisingly, we did not find hypertension to be associated with increased 30-day MAEs risk; in fact, it even seemed protective in univariate analysis after adjusting for confounding factors (OR, 0.18 [95%CI, 0.06–0.59], p = 0.004). Stratified analysis also demonstrated that patients without a history of hypertension had a higher risk of MAEs events, when compared with those with a history of hypertension, despite most studies reporting a higher risk of stroke in the hypertension population in CEA.35–37 Bond et al. 36 have reported systolic hypertension predicted the operative risk of stroke and death (HR = 1.01/10 mmHg, 95% CI [1.00–1.02], p = 0.030), while Caridad et al. 38 demonstrated patients with poorly controlled hypertension had a greater incidence of transient neurologic deficit than patients with controlled hypertension and normotension. However, this finding could be an artifact. Additionally, the decreased sample size after stratification may also have resulted in biases.
Another study showed that patients with preoperative mRS > 2 had the greatest risk for perioperative deterioration of neurological symptoms after CEA. 39 Similarly, our study also found a worse neurological deficit (mRS ≥ 3) associated with higher perioperative MAEs risk (aOR, 7.49 [95% CI, 1.90–29.49]), which was consistent with previous research. 7
In conclusion, our research and the previous literature have shown that patients with SCSO have worse outcomes after CEA. This can be partly caused by diminished cerebral perfusion resulting from the lack of collateral circulation. Carotid artery stenting (CAS) had been increasingly evaluated as a minimally invasive alternative to CEA. Several randomized controlled trials (RCTs)40,41 have showed that CAS had a higher 30-day risk of stroke or death in patients with symptomatic and asymptomatic stenosis than CEA. However, the periprocedural risks of stenting and endarterectomy vary according to patient characteristics. Outcomes might differ between the two procedures in specific groups of patients, especially in patients with increased surgical risk. According to the guidelines of the American Heart/Stroke Association, 42 CAS can been offered to those patients considered high risk for open endarterectomy, including those with contralateral carotid occlusion (CCO). Mericle et al. 43 found a seemingly lower 30-day stroke and death rate for stent placement than that for CEA in patients with CCO, while Mehta et al. 44 suggested that CAS was comparatively safe in patients with or without CCO. More RCTs and prospective cohort studies are needed to further elucidate the ideal approach for this patient subgroup.
Limitations
There are several limitations of our study. First, it was a single-center retrospective and nonrandomized study, and there were differences in baseline characteristics of traditional risk factors for carotid stenosis; however, we performed propensity-score matching to minimize selection bias. Second, information on intraoperative cross-clamp time was lacking; therefore, we did not evaluate the role of intraoperative cross-clamp time in the risk of perioperative complications after CEA with selective shunting. Third, we are aware that it is not possible to assess whether high risk patients with SCSO derive benefit or harm from surgery without a non-surgical control group. Last, the results of this study only apply to Chinese patients who underwent CEA.
Conclusions
SCSO is an independent predictor of 30-day major adverse events in the Chinese population. Whether these patients with SCSO are suitable for carotid endarterectomy should be carefully considered. Considering the limitations of our study, a prospective and randomized clinical trial to evaluate SCSO impact on perioperative complications in the Chinese population is warranted.
Supplemental Material
sj-pdf-1-vas-10.1177_1708538121993619 - Supplemental material for Severe contralateral carotid stenosis or occlusion drive 30-day risk after carotid endarterectomy
Supplemental material, sj-pdf-1-vas-10.1177_1708538121993619 for Severe contralateral carotid stenosis or occlusion drive 30-day risk after carotid endarterectomy by Wenyan Zhao, Faliang Gao, Cheng Wu, Deqing Peng, Xiao Jin, Lin Lou and Weijun Sun in Vascular
Footnotes
Acknowledgements
We gratefully thank Dr Jie Liu of Department of Vascular and Endovascular Surgery, Chinese PLA General Hospital for his contribution to the statistical support, study design consultations, and comments regarding the manuscript.
Ethics approval and consent to participate
The present study was approved by the Institutional Review Board of Zhejiang Provincial People’s Hospital, Hangzhou Medical University, and was exempted from written informed consent due to retrospective analysis based on medical records by Institutional Review Board.
Competing interests
The authors declare that they have no competing interests.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Natural Science Foundation of Zhejiang Province (grant no. LY19H160035) and Zhejiang Province Public Welfare Technology Application Research Project (grant no. LGF20G030011).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.