
Abstract
Objectives
Revascularization according to the angiosome concept is of proven importance for limb salvage in chronic limb threatening ischaemia but it is not always practicable. Bifurcated bypasses could be considered as an option when an endovascular approach is not feasible or has already failed and a single bypass would not allow direct revascularization of the ischaemic area. Bifurcated bypasses are characterized by landing on two different arteries, the main artery (in direct continuity with the foot vessels) and the secondary one (perfusing the angiosome district). The aim of this study is to evaluate the safety and effectiveness of bifurcated bypass in chronic limb threatening ischaemia.
Methods
Thirty-five patients were consecutively treated with a bifurcated bypass for chronic limb threatening ischaemia from January 2014 to December 2019 in a single vascular surgery centre. Data from clinical records and operative registers were collected prospectively in an electronic database and retrospectively analysed. Primary and primary assisted bypass patency, amputation-free survival, morbidity and mortality rates at 12 and 24 months were analysed.
Results
Mean follow-up period was 25.1 months (range 2–72 months). Thirty-six bifurcated bypasses were performed on 35 patients (age 75.3 ± 7.2 years; 69.4% were male). According to Wound, Ischemia, foot Infection classification 22.2% belonged to stage 3 and 77.8% to stage 4 and the mean Rutherford’s class was 5.1 ± 0.7. Immediate technical success was 100%. Early mortality and morbidity rates were respectively 5.5%, and 33.3%; foot surgery was performed in 50% of cases with wound healing in all patients. Primary patency and primary assisted bypass patency were 96.7% and 100% at 6 months; 85.2% and 92% at 12 months, 59.9% and 73.4% at 24 months, respectively. Amputation-free survival at 12 and 24 months was, respectively, 95.6% and 78.8%. Overall survival rates at 12 and 24 months were respectively 94.4% and 91.6%.
Conclusions
Bifurcates bypass can provide good results in patients with chronic limb threatening ischaemia without endovascular option, especially in diabetic ones. Bifurcated bypass is a complex surgical solution, both to be planned and performed, and it is quite invasive for frail patients that should be accurately selected.
Keywords
Introduction
In the last decade, the angiosome concept has become a landmark amongst chronic limb threatening ischaemia (CLTI) revascularization.1–3 Non-angiosome targeted revascularizations (indirect revascularizations) could bear a greater risk of unsuccessful foot healing, and could be associated with a lower limb salvage rate. 3 , 4 Despite that, indirect revascularization is not infrequent because the target artery for the distal anastomosis (the vessel that is in direct continuity with the foot ensuring the better run off and therefore the best chance of primary bypass patency) often does not bring blood directly to the right angiosome. 3 , 5 , 6 Direct revascularization is preferable not only to improve the healing rate of ischaemic ulcers but even for allowing the healing of a minor non-disabling amputation in the forefoot for the presence of gangrene or osteomyelitis.3–5
Bifurcated bypasses (BBs) could be considered as an option when an endovascular approach, such as percutaneous transluminal angioplasty (PTA), is not feasible or has already failed and a single bypass would not allow direct revascularization of the ischaemic area. 6 , 7 BBs are characterized by landing on two different arteries, the main artery (in direct continuity with the foot vessels) and the secondary one (perfusing the angiosome district).
In the literature, the use of BB for CLTI has been published as anecdotal cases and never focused on angiosome concept. 8 , 9 Little is known concerning the safety and effectiveness of this approach in terms of mortality and morbidity rates, amputation-free survival (AFS), graft primary (PP) and primary assisted patency (PAP) at early and midterm follow-up.
The aim of this single centre study is to evaluate the outcomes of BB on a cohort of patients with CLTI.
Materials and methods
The medical records of all patients with CLTI consecutively admitted and operated in a single vascular surgery centre between January 2014 and December 2019 were reviewed.
Of all the patients, those who underwent BB were selected and their demographic, clinical characteristics, indication for revascularization, general condition on admission and comorbidities were recorded with their length of hospital stay and the immediate outcomes.
The experimental protocol and informed consent were approved by the Institutional Review Board and all subjects gave informed consent.
Preoperative planning
Selection criteria for BB were: - presence of CLTI, according GLOBAL Guidelines;
1
- patency of at least one leg or foot artery for primary bypass landing, providing the best possible outflow, but unable to perfuse directly the interested angiosome or to cover all angiosomes involved; - presence of another artery (or arterial segment) directed to the ischaemic areas but itself considered unable to ensure primary bypass patency; - availability of enough autologous vein length; - no PTA feasible (according to criteria already enunciated by TASC in 2007 and recently proposed by GLOBAL Guidelines) or PTA attempt already failed.
1
,
5
In the preoperative phase, duplex ultrasonography (DUS) is the principal tool for surgical planning, and all the planning and the surgery were performed by the same operator. 10 , 11
DUS assessment focused on: - proximal anastomotic artery (inflow, quality of the vessel in the selected anastomotic sites); - distal anastomotic site for the primary bypass: run off bed (end diastolic velocity and mean diastolic velocity estimation) and arterial features (diameter larger than 2 mm, atherosclerotic plaques and calcifications); - secondary landing artery identified in close correlation with the involved angiosomes; - vein features (diameter larger than 2 mm, absence of wall sclerosis, intraluminal thrombosis).
In case of uncertainty concerning the patency of leg or foot arteries, computed tomography angiography was performed. Patients with previous failed PTA attempt had a digital subtraction angiography (DSA) to integrate the missing information.
Surgical technique
The surgical technique for BB does not substantially differ from traditional ones, except that for the selection of the conduit, usually the saphenous vein, and for the selection of the primary and secondary artery for the distal anastomosis of the graft: the primary artery should guarantee above all the adequate run-off and the secondary artery should supply to the angiosome of the foot lesions. In some cases, the primary bypass landed on the angiosome related artery because those patients presented multiple ischaemic lesions in more than in one angiosome, and for that reason a BB was performed for a direct revascularization of more than one angiosome. Secondary bypass was angiosome targeted in all cases.
Proximal anastomotic sites were common femoral artery, superficial femoral artery and popliteal artery. Some adjunctive vascular procedures were needed to optimize the bypass inflow: iliac artery stenting and common femoral endarterectomies. Distal anastomotic sites were represented by the below-knee popliteal artery, the tibial arteries or the foot arteries (Figure 1).
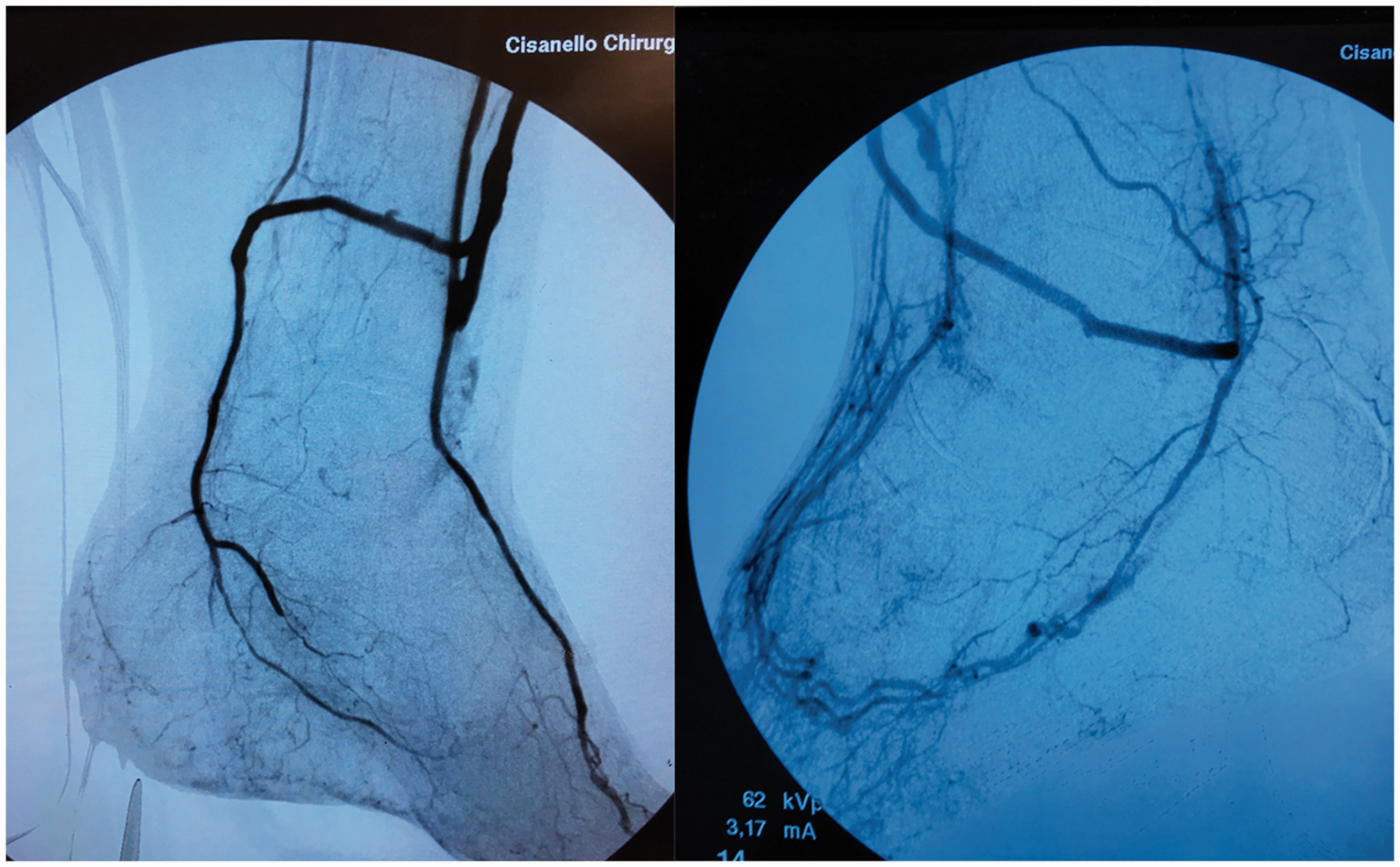
Digital subtraction angiography showing bifurcated bypasses landing to foot arteries.
The great saphenous vein was completely harvested by ‘bridged’ skin incisions along the length of the vein. All the bypasses were performed with ex-situ technique and the vein was tunnelled in a deep subfascial passage in order to spare vein length and, mostly, to prevent graft exposure in case of surgical wound dehiscence. The best venous trunk was used for the primary bypass, whilst secondary target artery was revascularized by a side branch. Whenever possible, a natural vein bifurcation was used. Otherwise, another vein segment was harvested and anastomosed in a termino-lateral fashion to the main saphenous trunk (Figure 2).
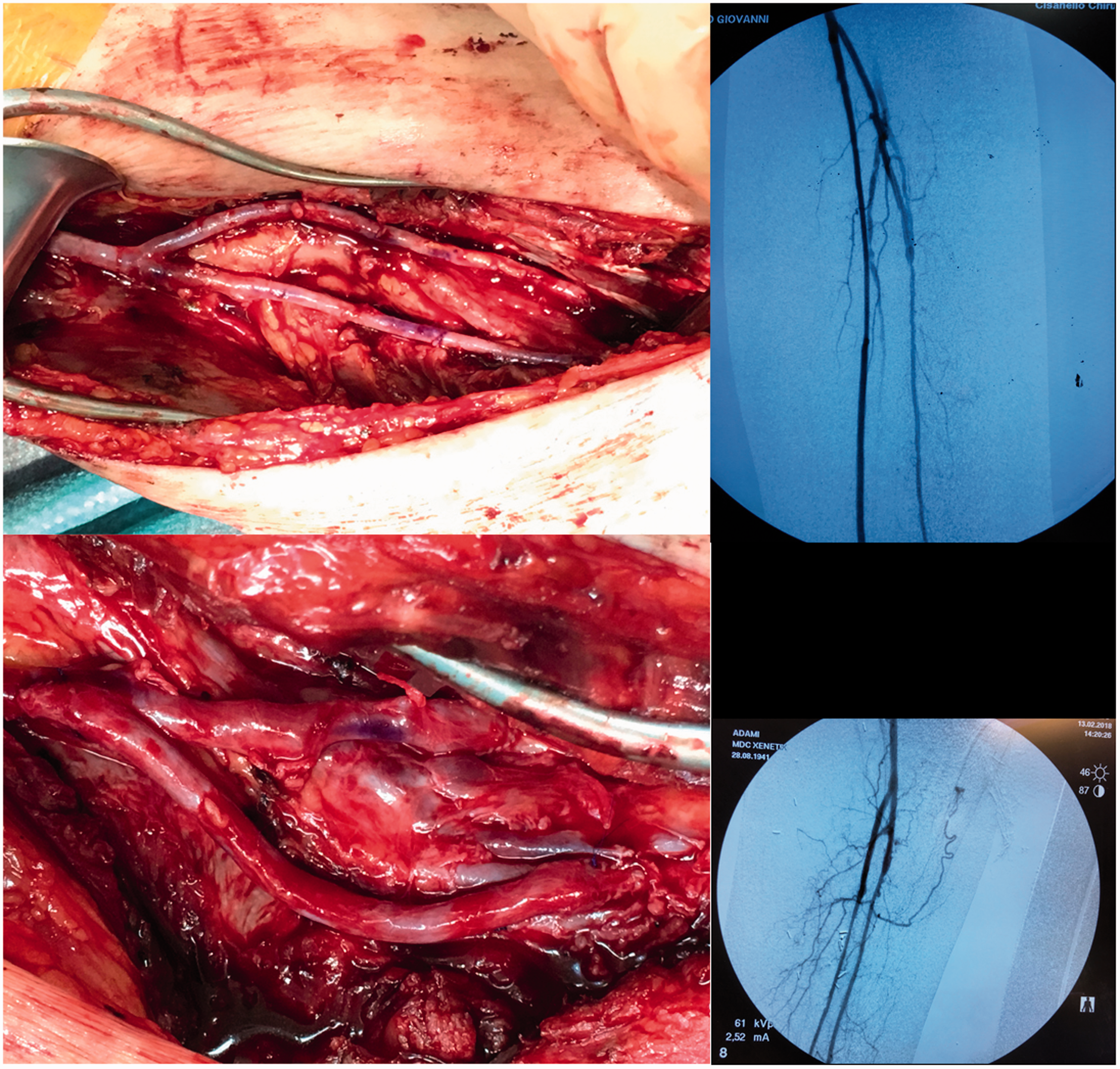
Intraoperative images of bifurcated bypass distal anastomosis for peroneal and posterior artery using a natural bifurcation and a side branch vein connection.
After performing the anastomoses, a DSA was done to evaluate whether PTA (usually on the second target artery) was required. PTA was performed on the outflow vessels when haemodynamic stenosis was present. DSA is helpful also to discover any technical pitfalls, for instance inadequate valve disruption, vein twisting, kinking or compression.
Patients were operated on single antiplatelet therapy whilst dual antiplatelet therapy was maintained only according to cardiac indications. Peripheral arterial diseases modifiable risk factors were treated intensively, and best medical treatment, such as statin therapy, was introduced in all patients. A 5000 UI of unfractioned heparin was administered during arterial clamping and thereafter 2500 UI hourly during surgery checking the activated clotting time. For thromboembolic prevention, prophylactic dosage of low molecular weight heparin was prescribed after surgery until recovery of the active mobility. After surgery if PTA was performed, dual antiplatelet therapy was introduced for 1 month.
All the procedures were performed under general anaesthesia.
All the patients, with or without diabetic foot (DF) syndrome, were followed by the DF specialists according to the Guidelines of the International Working Group on Diabetic Foot. 12 The DF specialists performed all the surgical procedures on the foot when required. The post-op foot wound care was performed in DF clinic. After minor amputation non-weight-bearing for three days was recommended in all the patients; afterwards, until recovery, touch-down weight-bearing was prescribed with footwear and orthotics.
Follow-up and statistical analysis
The patients were followed up with DUS in vascular clinic at 1, 3 and 6 months and thereafter every 6 months.
Mortality and morbidity rate and the perioperative complications for safety and AFS, graft primary (PP) and primary assisted patency (PAP) at early and midterm follow-up for effectiveness were evaluated.
All data were retrospectively revised using Excel Software (Microsoft Corp., Redmond, WA).
Data are expressed as a percentage in case of dichotomous variables and as mean and standard deviation in case of analogic ones. Cumulative graft patency and limb salvage were calculated as recommended by the reporting standards of the Committee of the Society of Vascular Surgery/North American Chapter of the International Society for Cardiovascular Surgery with the Kaplan-Meier method (SPSS 25, IBM Chicago, IL). 13
Results
Preoperative and intraoperative data
From January 2014 to December 2019, 675 patients with CLTI underwent treatment to 712 limbs with endovascular, hybrid and surgical revascularization. Amongst those 36 BB were carried out in 35 patients (18.3% of the total infrainguinal bypasses).
Indication for surgery was recurrent CLTI in 25 patients (69.5%), whilst in 11 patients (30.5%) CLTI was of new onset. Recurrent CLTI occurred mainly after previous endovascular procedures (24/25; 96%) and in these patients a further endovascular attempt was judged as not feasible. In all 11 new ischaemic cases the decision to perform a BB followed an earlier unsuccessful PTA attempt.
The clinical limb stage at the time of surgery was Rutherford ≥4 (average 5.1 ± 0.7) and the Wound, Ischemia, foot Infection (WIfI) score risk of major amputation was moderate in 22.2% and high in 77.8%.14–16 Foot lesions were present for an average of 1.8 ± 0.6 months prior to BB surgery.
The patient demographic and clinical characteristics are summarized in Table 1.
Demographic and clinical patient characteristics.
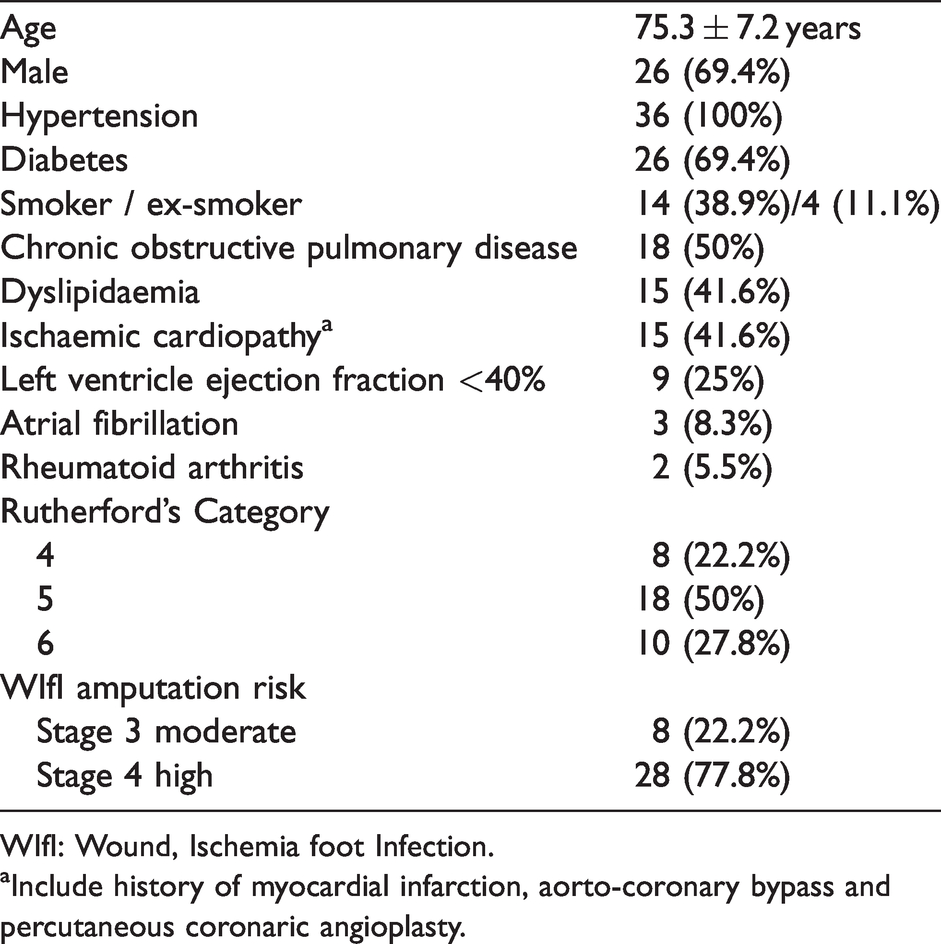
WIfI: Wound, Ischemia foot Infection.
aInclude history of myocardial infarction, aorto-coronary bypass and percutaneous coronaric angioplasty.
Proximal and distal anastomotic sites of the BB have been showed in Table 2. Primary bypass landed on the angiosome related artery only in 15 cases (41.6%).
Proximal and distal anastomotic sites of the bifurcated bypass.

In three patients an iliac artery stenting was performed simultaneously (8.3%), whilst in 10 (27.7%) a common femoral endarterectomy was needed. Adjunctive intraoperative PTA was performed below the distal anastomoses to improve bypass outflow and increase foot perfusion. PTA was mostly performed on the secondary target artery (23 cases: 63.9%) compared to the primary artery (12 cases: 33.3%; Figure 3). After ancillary endovascular procedure, a direct revascularization of the dorsal pedal artery was achieved in 31 cases (86.1%), of the plantar artery in 20 cases (55.5%) and in 15 cases (44.6%) of both. Overall average operative time was 358.9 ± 46 min.
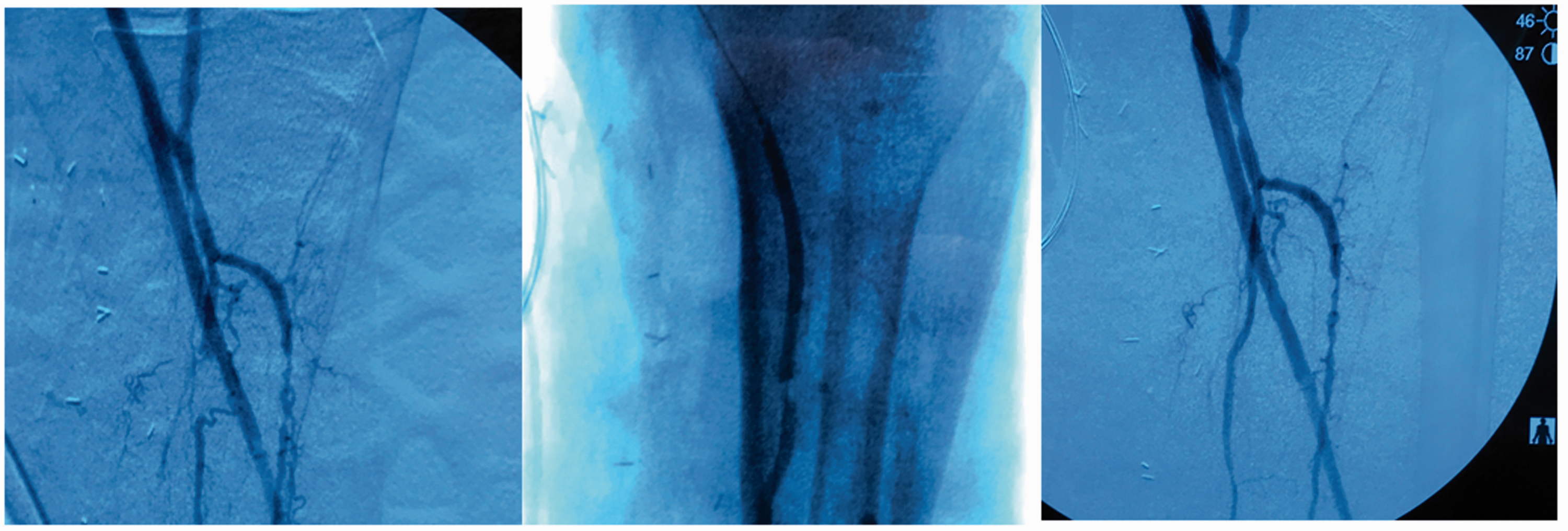
Angioplasty to restore peroneal direct inflow crossing peroneal trunk stenosis and peroneal origin occlusion.
Early results
The overall mean postoperative hospital stay was 8.3 ± 5 days.
Postoperative mortality rate (at 30 days) was 5.5%; both patients died after acute myocardial ischaemia (AMI). AMI occurred in four patients (11.1%).
Local complications were recorded in 10 cases (27.8%). In two cases (5.5%) it was related to bleeding which required reintervention. Surgical wound complications occurred in eight patients (22.2%), mostly skin necrosis but also infection and or dehiscence of the surgical wound without graft exposure and lymphorrhagia.
No major amputation was performed in the first 30 days. Delayed non-disabling amputations of the forefoot, both closed and open, were done in 18 cases (50%).
Late results
The median follow-up was 25.1 months (range 2–72).
The primary patency (PP) and primary assisted patency (PAP) were respectively 96.7% and 100% at 6 months, 85.2% and 92% at 12 months and 59.9% and 73.4% at 24 months (Figure 4).
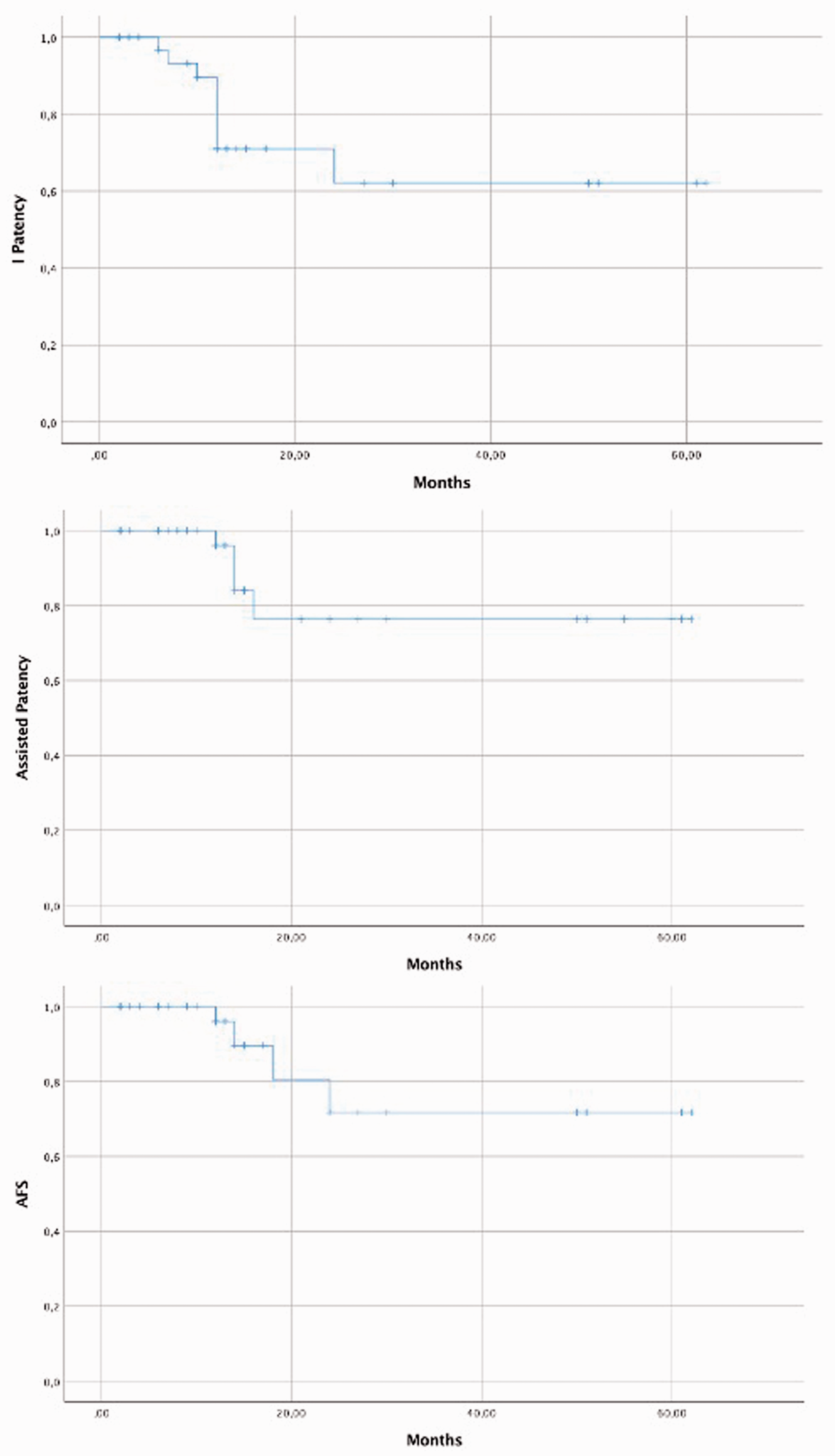
Kaplan–Meier analysis of primary patency (PP), primary assisted patency (PAP) and amputation-free survival rate.
PAP patency was achieved always by PTA in five cases (13.8%) at a mean follow-up of 6.2 months after surgery. PP and PAP are referred to the graft that is anastomosed to the best outflow vessel, even if in only three cases (8.3%) side branch occlusion occurred; the occlusion occurred after the complete lesion healing, but as the primary bypass remained patent, no clinical signs were noticed.
The global AFS was 86.1%; major above knee amputations were five (13.9%) in all case following late bypass occlusion (average occlusion time after surgery 28 ± 14 months).
AFS rates at 12 and 24 months were respectively 95.6% and 78.8% and the overall survival rates at 12 and 24 months were respectively 94.4% and 91.6%.
Discussion
BB has a long history of anecdotal and descriptive reports, but no studies have been carried out on its safety and effectiveness so far.
In 1999, Simms et al. suggested that sequential and BB lower limb bypass could improve leg and foot perfusion, but no data was reported. 17
Later Grus et al. reported a single centre analysis of 20 patients who underwent either simple (14 patients) or bifurcated (6 patients) bypass using reverse saphenous graft and allograft. The authors could not find any significant difference in primary or secondary patency rates, AFS, perioperative complications and overall survival, but they argued that the use of the vein instead of an allograft for the side branch could make the difference. 18
Several case reports on BB emphasize technical aspect without mid- or long-term results of patency and AFS rate.7–9
Spillerova et al. published a paper on angiosome revascularization and assessed that indirect revascularization leads to significantly worse wound healing rates compared with direct revascularization, although ‘in bypass surgery this concept is of less value and the artery with the best run off should be selected as the outflow artery’. The 1-year AFS rate achieved is only 18.0% for indirect revascularization bypass and 20.3% for direct ones. 4
The BB concept of a direct revascularization of all the ischaemic areas is the same used by cardiac surgeon for multiple aorto-coronary bypasses.19–21 The goal is to choose the distal target that provides the shortest bypass to re-establish inline flow, then extend the bypass to other arteries in order to bring blood for “myocardial”, and in our case “limb”, tissue salvage. 6 , 22 , 23 For this reason, the choice for primary bypass might not be strictly related to the angiosome theory, but mostly to allow the best run off vessel for the graft.
However, when the foot ischaemia is severe and/or in case of ischaemic ulcers, an “all angiosome-orientated” revascularization should be achieved. 3 , 6 , 7 Furthermore, data reveal that the foot ulcers can be found in different angiosomes in 38.3%, (41.6% in our findings). 4
The side branch of a BB represents the conduit to reach another angiosome target artery and, if necessary, as often happens (97.2% in our experience), to drive a balloon catheter to remodel the artery down to the foot. In our opinion this additional endovascular procedure had proven to be crucial in achieving satisfactory foot perfusion and probably bypass patency too.
Due to the high prevalence of diabetes in our programme (69.4%) combined with the severity of the arterial disease, as witnessed by the high Rutherford’s class and WIfI’s score, the BB technique with the help of adjunctive angioplasties could have improved limb salvage allowing only non-disabling minor amputations with subsequent healing. Moreover, it is reasonable to state that for all these CLTI patients with previous revascularization attempts this was the last chance before major amputation.
In a previously published article about diabetic patients with a newly onset CLTI, 200 patients were revascularized, mainly with PTA (94.5%). An AFS rate of 76% was achieved at 3-year follow-up. In this cohort, with 69.4% prevalence of diabetes but with much higher arterial impairment (since PTA had already failed or was not a feasible option), a global 83.3% AFS rate was reached at midterm. 24
Furthermore, all the major amputations occurred after bypass secondary failure, which indirectly reinforces the value of that bypass for limb salvaging. The most important role of the side branch was most likely not to improve the primary bypass patency, but rather to promote the healing of ischaemic lesions with the extensive use of downstream PTA distal to the anastomoses (particularly in the secondary target artery: 63.9%).
As seen from the literature, close US follow up allows for the discovery of signs of impending failure and consequently allowed secondary intervention, which increased the 2-year patency from 57.9% to 73.4% in those patients. 25 , 26
The retrospective nature of the study together with the rigorous control of patients with BB makes it difficult to compare our data with propensity matched control cases (like not-angiosome directed PTA or single vessel bypass cohort). However, comparing our early and midterm results to the objective performance goals (OPG) suggested for CLTI by the Society for Vascular Surgery 12 (Table 3), safety and effectiveness of the BB are confirmed despite the advanced CLTI stage and a relevant surgical trauma, which on the other hand might explain a relatively high peri-operative morbidity and mortality.
Comparison of the optimal performance goals (OPG) suggested for CLTI by the Society for Vascular Surgery and present series results.
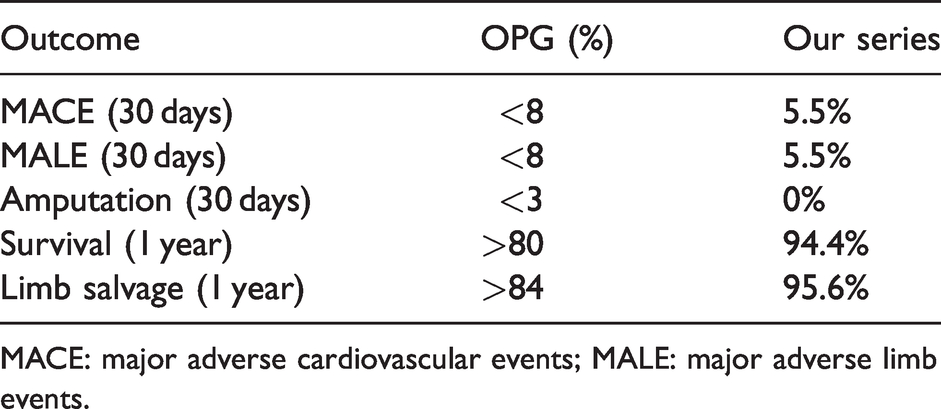
MACE: major adverse cardiovascular events; MALE: major adverse limb events.
For all these reasons, it is necessary to point out that careful patient selection before undergoing BB is mandatory to identify good candidates fit enough to overcome surgical trauma and to survive long enough to benefit from the procedure in the midterm.
In our experience the foot wound care was pivotal and, for that reason, all the patients, with or without DF syndrome, were followed by the DF specialists according to the Guidelines of the International Working Group on Diabetic Foot. 12 Adequate post-op foot wound care was performed in DF clinic for all CLTI patients in order to ensure the same standard of care.
The study presents some limitations, due to its retrospective nature, the limited number of patients and the absence of a control group. Those biases surely limit the validity of the conclusions but could hopefully add in the future to larger trials.
More prospective controlled studies are needed to evaluate the real impact of BB in CLTI treatment at 5 years and to compare them with already published long-term results concerning single tibial/foot artery bypass (Table 4).
Long-term tibial artery bypasses patency and limb salvage rate in literature.

Conclusions
BB can provide good results in patients with CLTI without endovascular option, especially in diabetic ones.
BB is a complex surgical solution both to be planned and performed, and proper patient selection is imperative.
Footnotes
Acknowledgments
This work has not been presented before.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.