
Abstract
Objectives
The carotid web is a compelling potential mechanism of cryptogenic stroke. It is easy for it to escape diagnosis or be misdiagnosed, since it rarely causes hemodynamic stenosis. Currently, there is a lack of consensus on the prevalence, etiology, imaging evaluation, and treatment strategy of carotid artery. We aimed to present the multimodal imaging of carotid web and comprehensively review the characteristics of carotid web.
Methods
A 38 year-old man with carotid web, who presented with acute left hemispheric syndrome, was not identified by computed tomography angiography and high-resolution magnetic resonance imaging in the initial report, but were identified in retrospect and then confirmed by digital subtraction angiography and histopathology. A literature review of carotid web was performed to identify prevalence, nature history, imaging tools, and optimal management of carotid web.
Results
80 reports including 681 patients with carotid web were identified. The prevalence of symptomatic carotid web was 1.2% in patients with transient ischemic attack/stroke, 6.4% in patients with cryptogenic ischemic stroke, 1.1% in patients with large vessel occlusion stroke, and 4.4% in patients who operated on for carotid stenosis. A total of 23.0% patients had bilateral carotid web. In most patients, carotid web was located on the posterior wall (87.3%) of the carotid artery (98.7%). The mean length was 3.3 mm and mean stenosis rate was 20.9%. A total of 31.6% percent patients had thrombus trapped in carotid web and 75.9% patients had large vessel occlusion. Computed tomography angiography and digital subtraction angiography were favorable tools to detect carotid web. There were rare periprocedural complications and no recurrent strokes in carotid revascularization patients.
Conclusions
carotid web is an under-recognized cause of ischemic stroke. It is easy to be missed or misdiagnosed. Carotid revascularization can effectively prevent recurrent stroke for patients with symptomatic carotid web. Clinicians should strength their learning and understanding of carotid web.
Keywords
Introduction
Carotid web (CW) corresponds to a shelf-like fold of the vessel wall. It is a compelling potential mechanism of cryptogenic stroke due to large vessel occlusion (LVO), particularly in young and middle aged women without conventional stroke risk factors.1–3 Several studies suggest that patients with symptomatic CW have a high risk of recurrent stroke, even if they receive medical treatment.4–6 Carotid revascularization may be safe and effective in patients with CW.6, 7 However, many clinicians have insufficient understanding of CW. It is easy for it to escape diagnosis or be misdiagnosed, since it rarely causes hemodynamic stenosis. There is a lack of consensus on the best imaging tool for evaluation of CW and the morphological characteristics of CW. Besides, the natural history, etiology, and prevalence of CW are unclear. Hence, we present a case of a young man with CW who were not identified by computed tomography angiography (CTA) and high-resolution magnetic resonance imaging (HRMRI) in the initial report, but were identified on CTA and HRMRI in retrospect and then confirmed by digital subtraction angiography (DSA) and histopathology. A review of the literature was then performed to fully elucidate the prevalence, nature history, imaging tools, and optimal management of CW. Written informed consent for patient information and images to be published was obtained.
Case report
A 38 year-old Chinese man, who was a smoker, was admitted to emergency department with acute left hemispheric syndrome. One month ago, he suffered an episode of transient aphasia. He was under no medications and did not have any history of atrial fibrillation. Multimodal computed tomography imaging showed total occlusion of distal M1 segment of middle cerebral artery (MCA) and cerebral tissue hypoperfusion in left frontotemporal parietal lobe, radial crown and basal ganglion (Figure 1(a)). Additionally, carotid artery dissection was suspected in the initial CTA assessment. A subsequent DSA confirmed the finding of MCA occlusion and discovered a thin intraluminal filling defect along the posterior wall of the ipsilateral carotid bulb, compatible with CW (Figure 1(b)). It showed 3.1 mm long and approximately 10% stenosis according to the North American Symptomatic Carotid Endarterectomy Trial criteria. When retrospectively reviewing the CTA imaging, we found a shelf-like septum emanating from the posterior wall of the internal carotid bulb on a sagittal section and a corresponding axial section (Figure 1(c)). The patient accepted mechanical thrombectomy inside the therapeutic time window, with a good clinical and angiographic result. A red thrombus was retrieved with subsequent histological analysis by hematoxylin and eosin staining showing a mixed composition of fibrin/platelets and red blood cells, consisting of 50% fibrin/platelet ratio, 45% red blood cells, and 5% white blood cells (Figure 1(d)). On the third day, the patient with CW was considered normal by HRMRI in the initial report, but was identified in retrospect, which revealed protrusion with enhancement along the posterior wall of carotid bulb (Figure 1(e)). Because the complete reperfusion of left MCA was obtained, the patient was discharged with dual antiplatelet therapy and was recommended for endovascular or surgical treatment for CW. On the 36th day, CTA demonstrated an unchanged degree of stenosis of the left internal carotid bulb. The morphology of the intraluminal lesion was unchanged from 36 days prior. On the 56th day, he was transferred to neurosurgery department for surgery for CW. No recurrent stroke occurred during this period. Preoperative Doppler ultrasonography (DUS) revealed a hyperechogenic septum along the left carotid bulb associated with thrombus formation (Figure 1(f)). There was no new ischemic lesion on magnetic resonance imaging (MRI). Transthoracic echocardiography and transcranial Doppler with bubble test did not reveal any potential cardioembolic source of embolism. Transcranial Doppler study was negative for microembolic signals. He underwent carotid endarterectomy (CEA) to eliminate the web, with successful results and no complications. A thrombus was identified in the web pocket. Histology demonstrated smooth muscle cell–rich intima, increased elastic tissue, and myxoid degeneration in the resected shelf-like septum. The superimposed thrombus had a fewer fibrin/platelet ratio (20%), higher red blood cells (77%), and 3% white blood cells (Figure 1(g)). Postoperative CTA and DUS showed normal lumen without any flow or structural abnormalities (Figures 1(h) and (i)). After 11 months follow-up, the patient experienced no recurrent stroke/transient ischemic attack, and no restenosis was detected by DUS. Multimodality imaging of carotid web. (a) Cerebral computed tomography perfusion (CTP) showing delayed mean transit time (MTT) and time to peak (TTP), and decreased cerebral blood flow (CBF) and cerebral blood volume (CBV) in left frontotemporal parietal lobe, radial crown, and basal ganglion. (b) Digital subtraction angiography (DSA) showing total occlusion of left middle cerebral artery and a thin intraluminal filling defect along the posterior wall of the carotid bulb, compatible with carotid web (arrow). (c) Carotid web on computed tomography angiology (CTA), which shows a thin intraluminal filling defect along the posterior wall of the carotid bulb on a sagittal section and a corresponding axial section (arrow). (d) The thrombus retrieved during the mechanical thrombectomy and histological analysis by hematoxylin and eosin staining showing a mixed composition of fibrin/platelets and red blood cells. (e) High-resolution magnetic resonance imaging (HRMRI) showing the abnormal enhancement along the posterior wall of the left internal carotid bulb on a sagittal section and a corresponding axial section (arrow). (f) Doppler ultrasonography (DUS) showing a hyperechogenic septum along the left carotid bulb associated with thrombus formation (arrow). (g) The resected carotid web with the superimposed thrombus (arrow), and histology showing intimal fibrous thickening without atherosclerotic change. (h) CTA in sagittal and axial views showing a postoperative normal carotid lumen. (i) Postoperative DUS showing normal lumen without any structural abnormalities.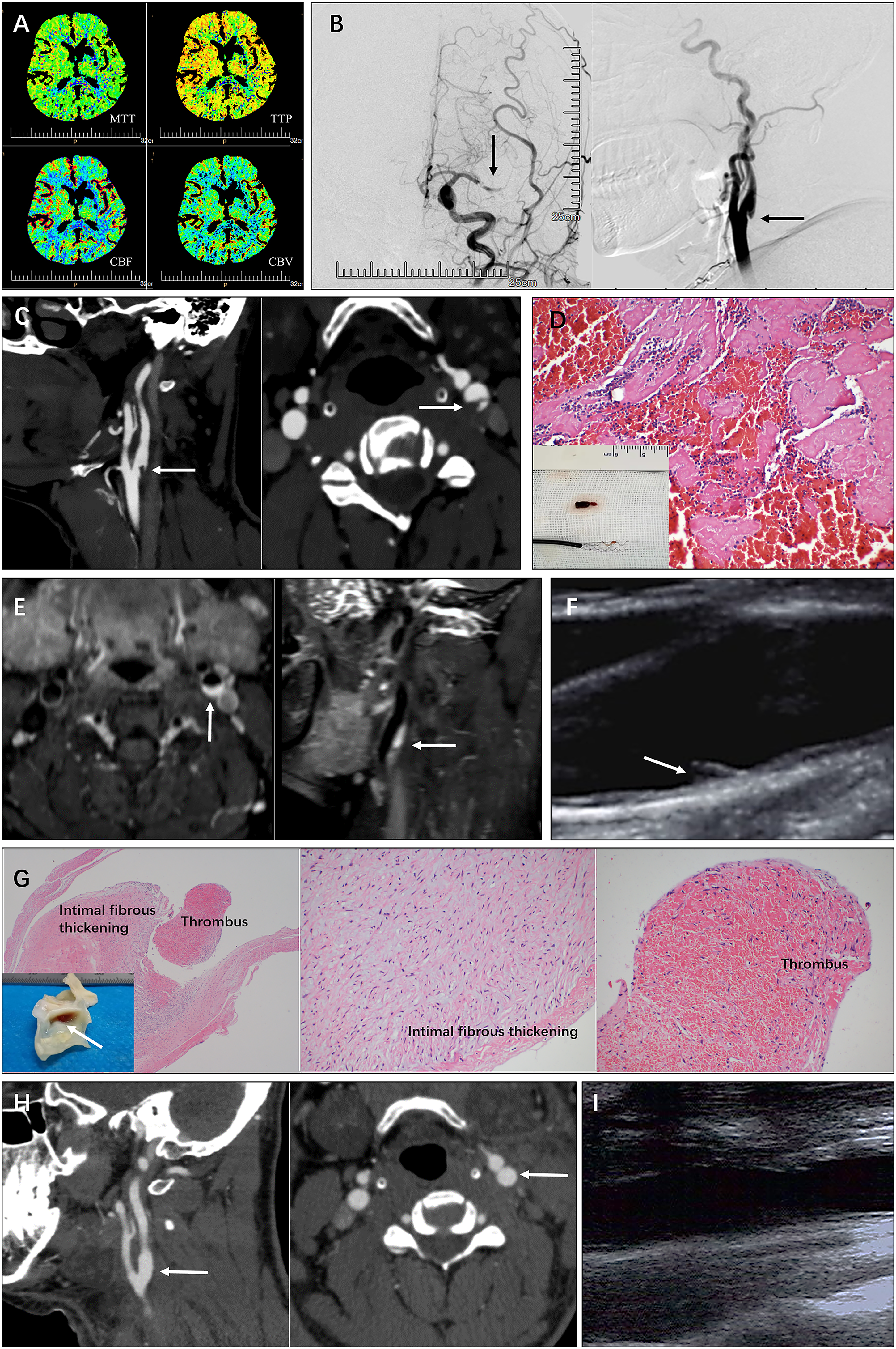
Literature review
Search strategy and article selection
This literature review was conducted and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement. We performed a detailed literature search using PubMed/MEDLINE databases. The search strategy consisted of using the following keywords/MESH terms for abstract and full text: “carotid web,” “intraluminal web,” “pseudovalvular fold,” and “intimal fibromuscular dysplasia.” The search included only articles in English published until November 2021 with no early date limit. Titles and abstracts of all articles were screened. Only articles were included if reports described cases of CW. If full text were unable to be reviewed, the articles were excluded. References from relevant reviews were hand-searched. Subsequently, relevant articles were retrieved and evaluated independently by two authors (J.Z., Y.Y.). A cross-reference check of the citations of each included relevant article was done to ensure that no relevant studies were missed by the computerized database search. Disagreements regarding inclusion of studies were resolved by discussion and consensus agreement.
Data extraction
First, we manually extracted patient-level data for all reported CW patients, including demographics, conventional stroke risk factors, symptomatic or asymptomatic, recurrent stroke, multimodality imaging, and treatment strategy. Conventional stroke risk factors included hypertension, dyslipidemia, atrial fibrillation, diabetes mellitus, coronary artery disease, smoking, patent foramen ovale, and oral contraceptive use. Symptomatic CW was defined as stroke or transient ischemic attack ipsilateral to the CW, and other possible causes of stroke or transient ischemic attack were excluded. Then, the CW-level data for all reported CWs was extracted, including location, length, and degree of stenosis. The reported degree of carotid stenosis in the original article was used, and it was classified as normal, 50–69%, 70–99%, and occlusion. Data abstraction was completed independently by two authors (J.Z., Y.Y.) and any discrepancies were resolved through review and consensus.
Results
Literature review
Flowchart of literature selection is reported in Figure 2. A total of 719 articles were identified. After reviewing the titles, abstracts, or full texts of each, we excluded articles in languages other than English, articles with unavailable full text, and irrelevant articles. The 80 remaining publications matched the inclusion criteria of our study (Supplemental Table 1). A total of 681 patients with CW were included; 680 from the 80 publications identified in our literature review and 1 case from our previous report. Four hundred and sixty-four (68.1%) patients were symptomatic, 39 (5.7%) were asymptomatic, and 178 (26.1%) could not be classified. Of these 80 publications, 64 (80.0%) were published after 2017, including 619 (90.9%) patients with CW and 415 (89.4%) patients with symptomatic CW. Literature review flowchart.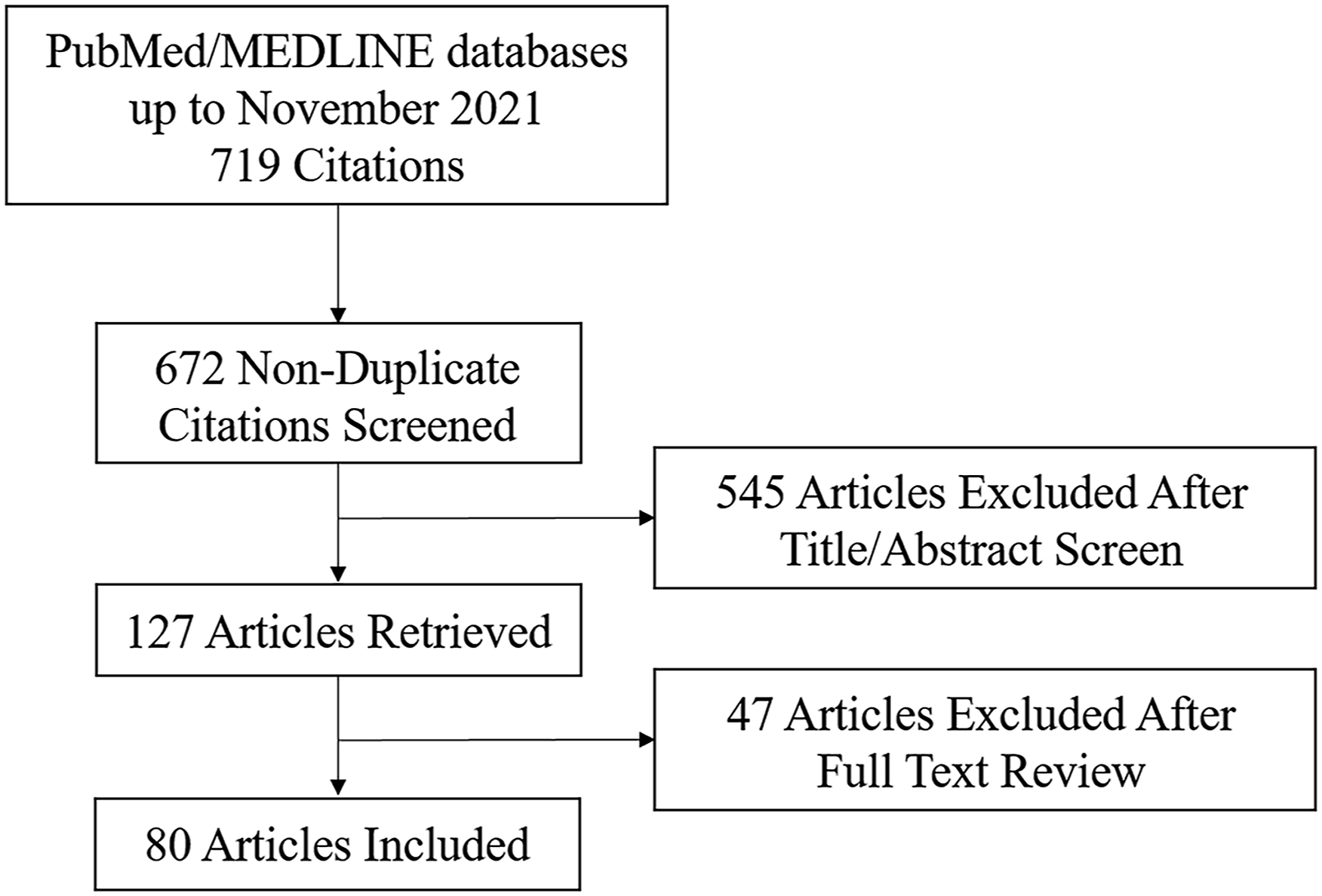
Prevalence
Three articles enrolled patients who underwent carotid CTA, and the overall prevalence of CW in these patients was 0.6% (65/10120). Five articles enrolled patients with transient ischemic attack (TIA)/stroke, and the overall prevalence of CW in these patients was 2.3% (109/4775) and that of symptomatic CW was 1.2% (36/3079). Seven articles enrolled patients with cryptogenic ischemic stroke, and the overall prevalence of CW in these patients was 6.4% (86/1342). Four articles enrolled patients with large vessel occlusion stroke, and the overall prevalence of ipsilateral CW in these patients was 1.1% (61/5778). Two articles enrolled patients who operated on for a carotid stenosis, and the overall prevalence of symptomatic CW in these patients was 4.4% (18/410).
Demographics of patients with carotid web and morphological characteristics of Carotid web
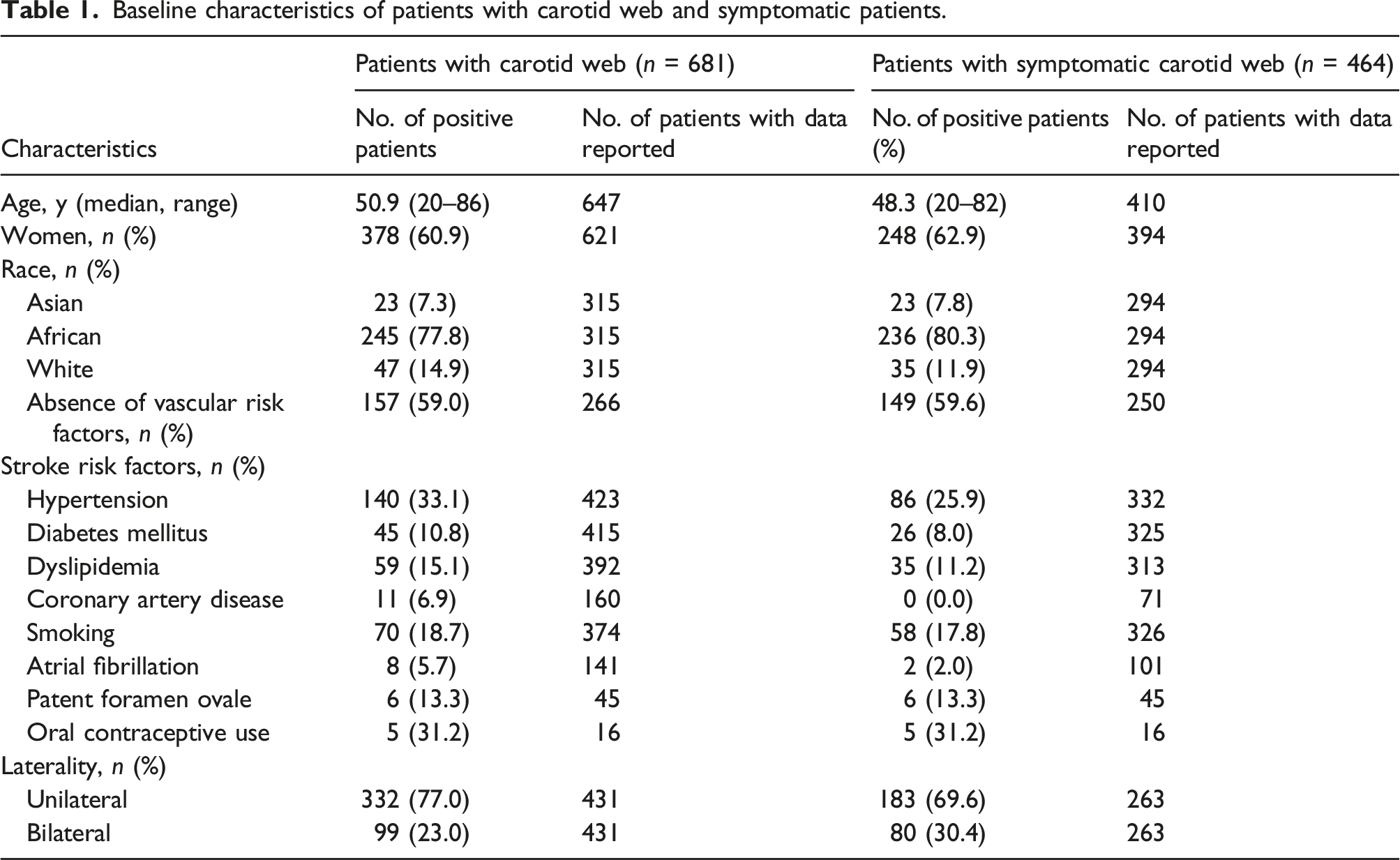
Baseline characteristics of patients with carotid web and symptomatic patients.
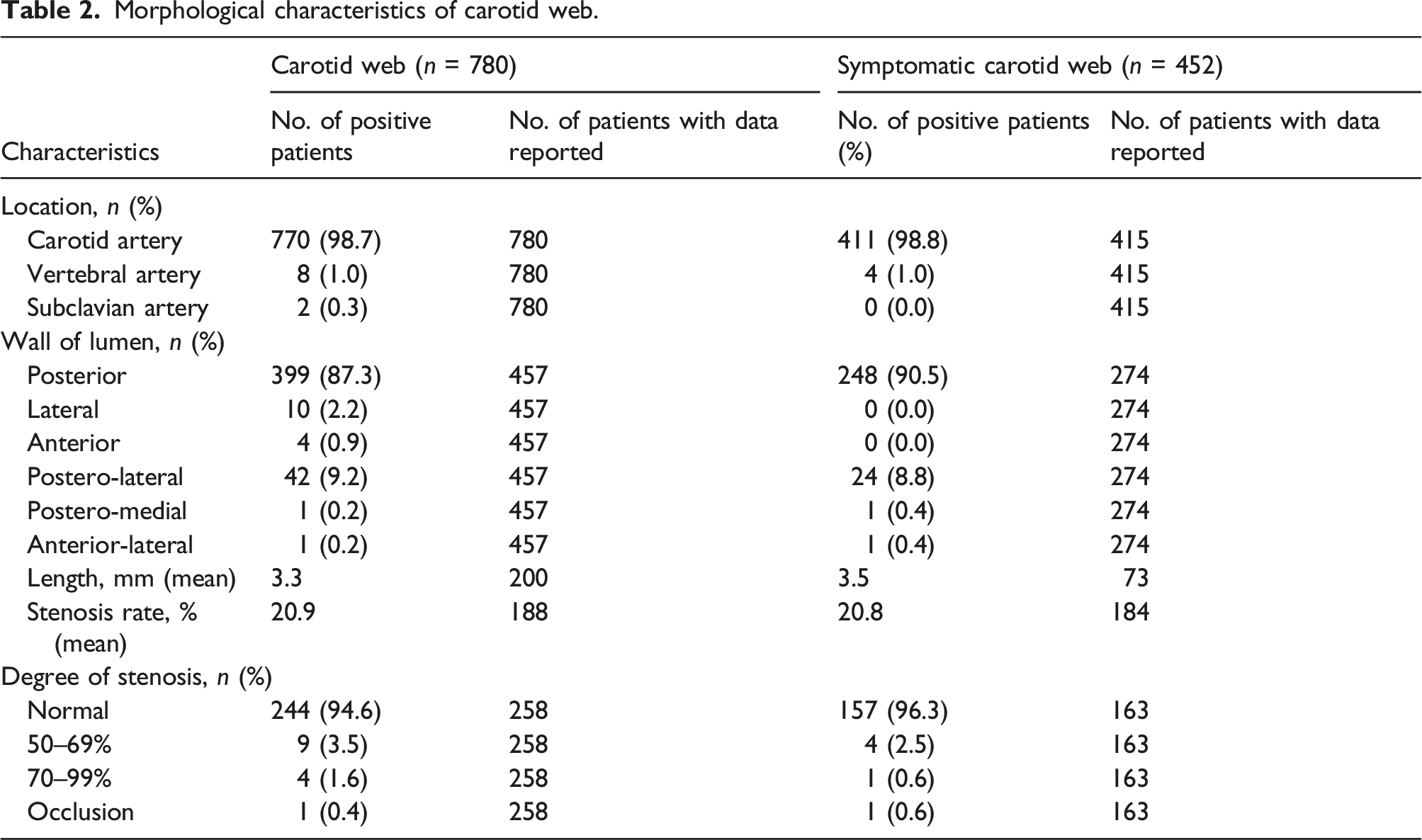
Morphological characteristics of carotid web.
Multimodality Imaging of carotid web
CW was detected in 136 patients by DUS, and 18 (13.2%) patients with CW confirmed by CTA were misdiagnosed as normal or atherosclerotic vessels. CW was detected in 551 patients by CTA, and 5 (0.9%) patients with CW confirmed by DSA were misdiagnosed as normal or stenotic vessels. CW was detected in 137 patients by DSA. One (0.7%) patient was considered as atherosclerotic lesion by DSA and then diagnosed as CW after evaluation of lesion etiology by CTA. CW was detected in 14 patients by magnetic resonance (MR), including six by HRMRI, one by 3.0 T magnetic resonance imaging (MRI), and seven by magnetic resonance angiography (MRA). Four CWs confirmed by DSA were not visible on MRA. Three patients with CW confirmed by DSA underwent intravascular ultrasound (IVUS), and CW was detected in 2 (66.7%) patients. Sixty-three patients were confirmed by histology, which demonstrates intimal fibrous proliferation without evidence of atheromatous deposits, consistent with a focal variant of intimal fibromuscular dysplasia. The presence or absence of superimposed thrombus was reported in 187 patients, of which 59 (31.6%) patients had thrombus trapped in CW detected by DUS, CTA, or DSA. The presence or absence of LVO was reported in 261 patients, of which 198 (75.9%) patients had LVO. The location of LVO was reported in 154 patients, including 140 (90.9%) in MCA (81 in M1 segment, 29 in M2 segment, 2 in M3 segment, and 28 unclassified), 3 (1.9%) in ACA, 1 (0.6%) in PCA, and 10 (6.5%) in ICA(8 in terminal ICA, 2 in supraclinoid ICA). Only two patients had histological analysis of thrombosis superimposed in CW and six patients of embolic thrombus in LVO. Among the 62 patients with CW extracted from articles published before 2017, 20 (32.3%) were detected by DUS, 42 (67.7%) by CTA, 22 (35.5%) by DSA, and none by MR. Among the 619 patients with CW extracted from articles published after 2017, 116 (18.7%) were detected by DUS, 509 (82.2%) by CTA, 115 (18.6%) by DSA, and 14 (2.3%) by MR.
Asymptomatic carotid web
A total of 119 patients with asymptomatic CW were reported. Of these asymptomatic CWs, 80 patients had contralateral symptomatic CW and 39 patients had unilateral asymptomatic CW. The patients with unilateral asymptomatic CW were 76.9% women with a median age of 54.1 years. Race was reported in five patients, and four were Africans. The presence or absence of conventional stroke risk factors was reported in seven patients, of whom 4 (57.1%) had one or more risk factors. The location of CW was reported in 62 patients, including 59 on carotid artery and 3 on vertebral artery. These CWs were all located on posterior wall of the lumen. The length of CW was reported in 14 patients, with a mean length of 2.6 mm. The stenosis rate of CW was reported in 43 patients, with a mean rate of 30.23%. The degree of stenosis was reported in 14 patients, and all CWs had normal lumen. Forty-three patients with asymptomatic CW were untreated. No ischemic events were associated with these asymptomatic CW, with a median follow-up time of 44.0 months. Six patients were treated with open surgery or stenting and one patient had available follow-up data. No ischemic event occurred, with 3 months follow-up.
Symptomatic carotid web and secondary stroke prevention
Secondary stroke prevention and stroke recurrence.

Discussion
CW is a proposed stroke mechanism that may underlie cryptogenic stroke, particularly in younger patients without vascular risk factors. The current literature review is the largest and most comprehensive collection of CW patients published to date.
The prevalence of CW in patients who undergo carotid CTA varies from 0.5 to 2.3%.8–10 The prevalence of CW in patients with ischemic stroke/TIA varies from 0.45 to 9.6%.11–15 The prevalence of symptomatic CW in patients with cryptogenic stroke varies from 1.6 to 21.2% and 4.5–23.1% in young patients with cryptogenic stroke.1, 2, 11–13, 16, 17 The prevalence of symptomatic CW in patients with large vessel occlusion stroke varies from 0.7 to 2.5%.3, 4, 16, 18 The prevalence of symptomatic CW in patients who were operated on for a carotid stenosis varies from 3.0 to 15.6%.7, 19 After our literature review, the prevalence of symptomatic CW was 1.2% in patients with transient ischemic attack/stroke, 6.4% in patients with cryptogenic ischemic stroke, 1.1% in patients with large vessel occlusion stroke, and 4.4% in patients who operated on for carotid stenosis.
Similar to the systematic review published by Zhang et al. in 2018, 20 our study found that patients with CW were relatively young, with a higher prevalence of women. The majority of these patients had few conventional stroke risk factors. The most commonly reported stroke risk factors were hypertension and oral contraceptive use. We also found that CW was most common among African population and rare in Asian population; however, there are several publications focused on CW in Asian population in recent years.8, 12, 14, 15, 21, 22 They were not included in the race data analysis of current literature review, since these studies did not explicitly state the race composition. In addition, we also updated some information about morphological features of CW. Bilateral CW was not uncommon, and 30.4% symptomatic CW had contralateral CW. CWs were located in carotid artery, vertebral artery, or subclavian artery, but it was most commonly located in the posterior wall of the carotid bulb. It may be partly due to the definition of CW. In most publications, CW was defined as a shelf-like septum in the posterior wall of the carotid bulb.1, 2, 4, 5, 7, 9-11, 13, 16–19, 23-28 On the other hand, the greater development and thickness of the intima and the greater amount of elastic fibers in carotid vessel are probably linked to the presence of a higher frequency of CW on the carotid artery. 29 The mean length of symptomatic CW was relatively longer than asymptomatic CW. CW could cause moderate stenosis, severe stenosis or even occlusion of vascular lumen, but most CW still did not cause obvious lumen stenosis.
There are several useful tools to identify carotid webs, including DUS, CTA, MR, and DSA. The finding of CW closely depends on the experience of radiologists. At present, there is no consensus on which imaging method is more suitable. DUS is a convenient and non-invasive method, but the diagnosis can be challenging because of thrombus inside CW, which mimics a classic hypoechoic non-calcified plaque. Ben et al. found that the rate of misdiagnosis and missed diagnosis was 30.43% in the first ultrasonography. 21 Hassani et al. attempted to evaluate the suspected CWs using IVUS. In two of the three cases, IVUS showed an isoechoic-to-hyperechoic focal eccentric area at the posterior carotid bulb, consistent with CW. But the endoluminal protrusion was inconspicuous on IVUS due to the low resolution of ultrasound not allowing a clear differentiation between fibrosis, thrombosis, and atherosclerosis. 30 CTA is the most widely used imaging tool for evaluation of CW. In the current review, only 0.9% patients with CW confirmed by DSA were misdiagnosed as normal or atherosclerotic vessels by CTA. Some scholars believed that the correlation between DUS and CTA showed a substantial agreement, but some believed not.31, 32 CTA and DSA shared very high strength of agreement. 31 DSA could show retrograde delayed filling of the carotid bulb web and stasis within the pouch. MR imaging enables an in-depth evaluation of patients with CWs: morphology (by MRA), composition (by multi-contrast FSE), and wall dynamics (by cineFSE). 27 In the current literature review, CW was detected in seven patients by MRA and four CWs confirmed by DSA were not visible on MRA. The missed diagnosis rate of CW by MRA was higher than that by other imaging tools. MRA maybe not a good modality to investigate for CW. However, the limitation of this study is the small sample size. The imaging diagnosis of CW needs more large sample size research. Histopathological analysis is the gold standard for the diagnosis of CW, which revealed that the etiology of CW was a nonatheromatous intimal fibromuscular dysplasia of the extracranial carotid artery. However, few patients had histological analysis of thrombus superimposed in CW and embolic thrombus in LVO, which may be of significance to clarify the pathogenesis of CW. In the present case we reported, we found that the histological analysis of LVO stroke embolized thrombus by CW was similar to that of other stroke etiologies, similar to previous studies.18, 33, 34 But the superimposed thrombus had a fewer fibrin/platelet ratio and a higher red blood cells than Gao et al. reported, which was the only previous study on histological diagnosis of thrombus superimposed in CW, to the best of our knowledge. 35
This literature review identified 43 patients with asymptomatic CW who did not take any treatment. No ischemic events were associated with these asymptomatic CW, with a median follow-up time of 44.0 months. Therefore, asymptomatic CW noted “on imaging only” is benign from a clinical perspective not requiring further treatment or surveillance. For patients with bilateral CWs, asymptomatic side also does not need intervention. Optimal management strategies for symptomatic CW include either medical treatment or carotid revascularization. Guglielmi et al. found that 1 of 6 patients with a symptomatic CW had a recurrent stroke within 2 years 4 Within the current review, we found that 36.4% untreated symptomatic CW patients had stroke recurrence, and more than a quarter of symptomatic CW patients treated with medical therapy alone had stroke recurrence with a median time to recurrent stroke of only 8.3 months. CW may be particularly amenable to revascularization, since these patients are relatively young and commonly lack of conventional stroke and cardiovascular risk factors. None of the patients treated with carotid revascularization had recurrent stroke, with a median follow-up of 24.9 months. Only 3.0% patients with periprocedural complications were reported, which is recovered in the first follow-up. The stroke recurrence rate in patients with CW who were treated with anticoagulant therapy (25.0%) was relatively lower than those in patients without any treatment (36.4%) or patients with antiplatelet therapy (30.9%). So anticoagulant therapy is recommended for those patients between diagnosis and definitive therapy. However, the stroke recurrence rate in patients with anticoagulant therapy is still higher than that in patients with carotid revascularization. Carotid revascularization is recommended for patients with symptomatic CW as early as possible. Besides, medication after carotid revascularization was reported in 63 patients. Some patients were treated with anticoagulant therapy, while others not. All the patients remained stroke free during follow-up. Therefore, postoperative anticoagulant therapy may not be necessary.
In the current literature review, most articles (80.0%) were published after 2017, which showed that both clinicians and radiologists had paid more and more attention to CW in recent years. After 2017, DSA (18.6%) was less used to detect CW, while non-invasive examination methods, such as CTA (82.2%), were more and more used to detect CW. However, only 34.9% patients with symptomatic CW extracted from articles published after 2017 were treated with carotid revascularization, which was relatively lower than that (46.9%) in symptomatic patients extracted from articles published before 2017. Clinicians should strength their learning and understanding of CW.
Conclusion
CW is an under-recognized cause of ischemic stroke, especially in young women without conventional stroke risk factors. It is easy for it to escape diagnosis or be misdiagnosed. Patients with symptomatic CW who are managed medically alone have a high stroke recurrence rate, and carotid revascularization can effectively prevent recurrent stroke. Clinicians should strength their learning and understanding of CW.
Supplemental Material
sj-pdf-1-vas-10.1177_17085381221084809 – Supplemental Material for Multimodality imaging of carotid web: A case report and literature review
Supplemental Material, sj-pdf-1-vas-10.1177_17085381221084809 for Multimodality imaging of carotid web: A case report and literature review by Jie Zhang, Yuzhu Yan, Weikai Yao, Jishuang Liu and Li Cui in Vascular
Footnotes
Acknowledgments
The authors acknowledge the patient for his participation in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.