
Abstract
Objective
Transcarotid revascularization (TCAR) is a minimally invasive hybrid surgical carotid stenting technique which utilizes cerebral flow reversal as embolic protection during carotid lesion manipulation. This investigation was performed to define the perioperative risks associated with this operation in the obese patient.
Methods
A retrospective review of tandem carotid revascularization databases maintained at two high-volume health systems was performed to capture all TCARs performed between 2015 and 2022. A threshold of body mass index of 35 kg/m2 defined the “obese” patient. Demographics, intraoperative, perioperative, and follow-up characteristics were compared using univariate analysis.
Results
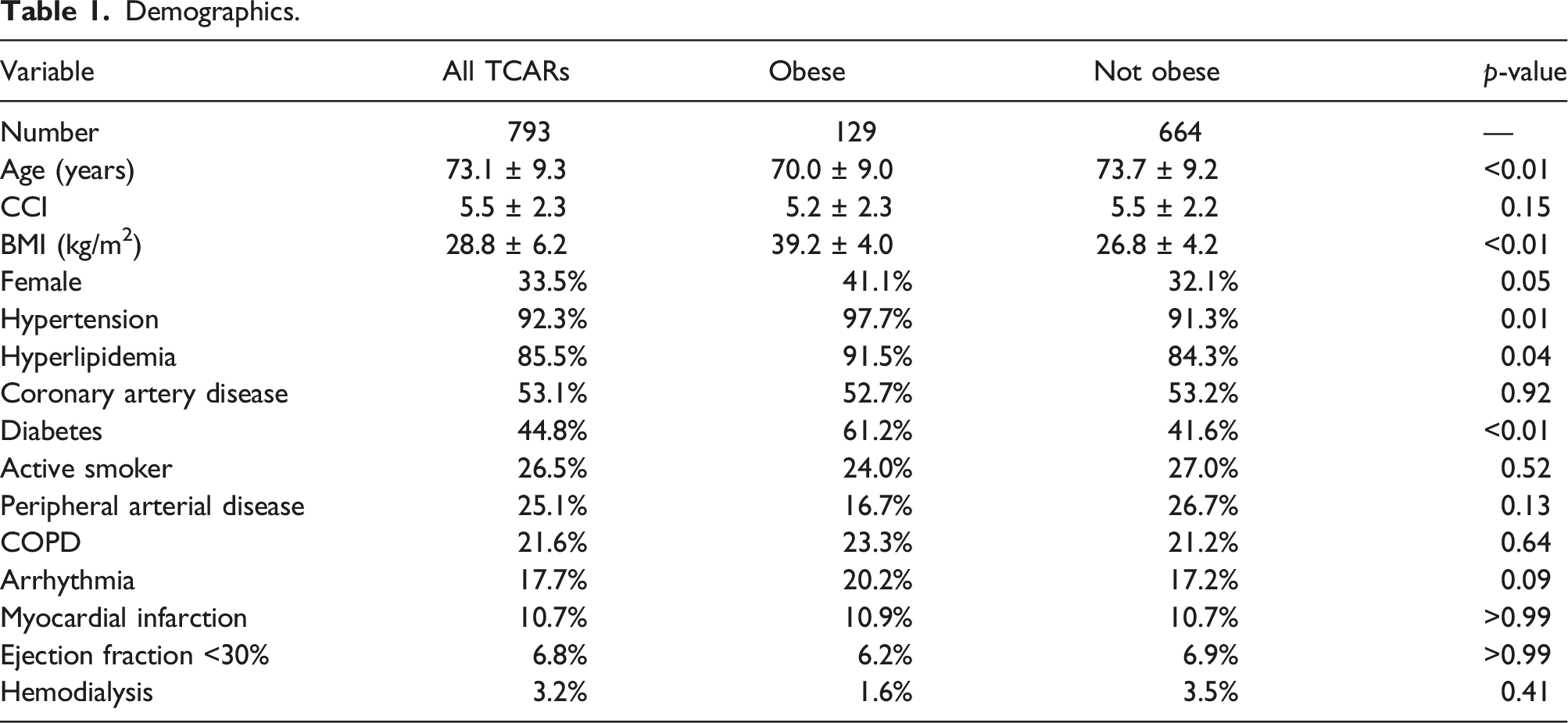
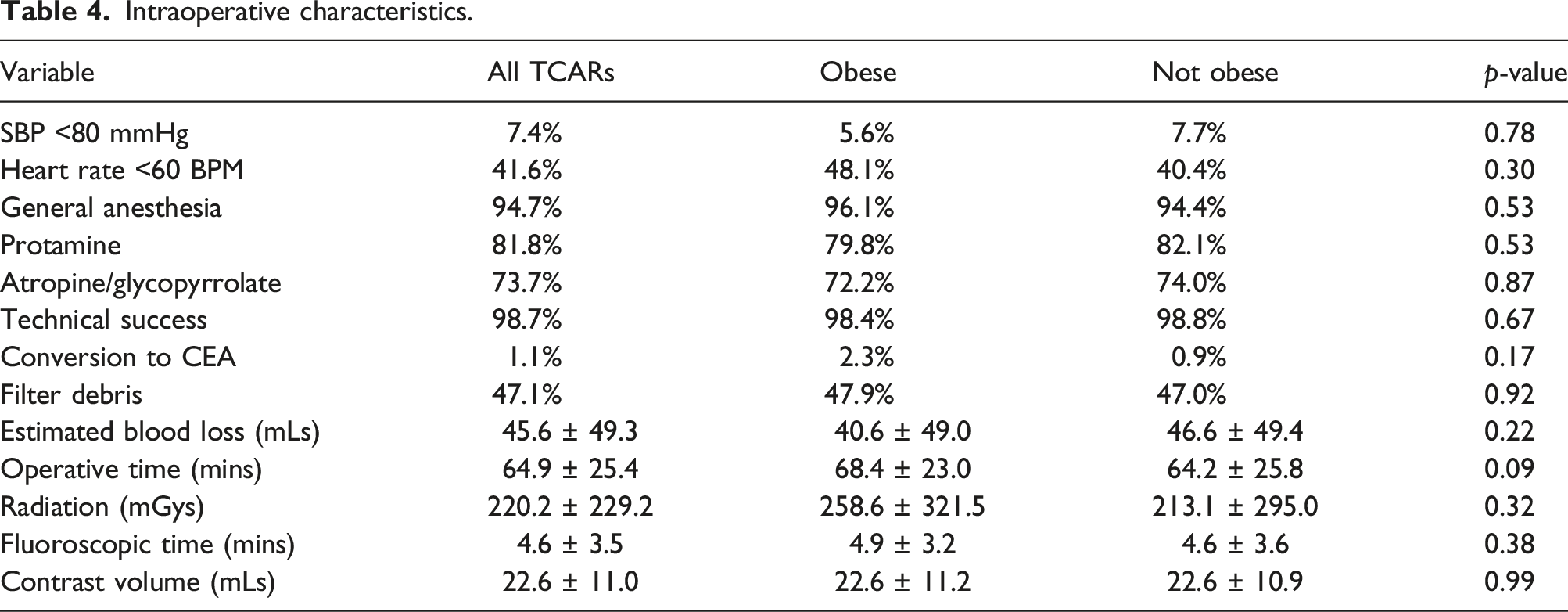
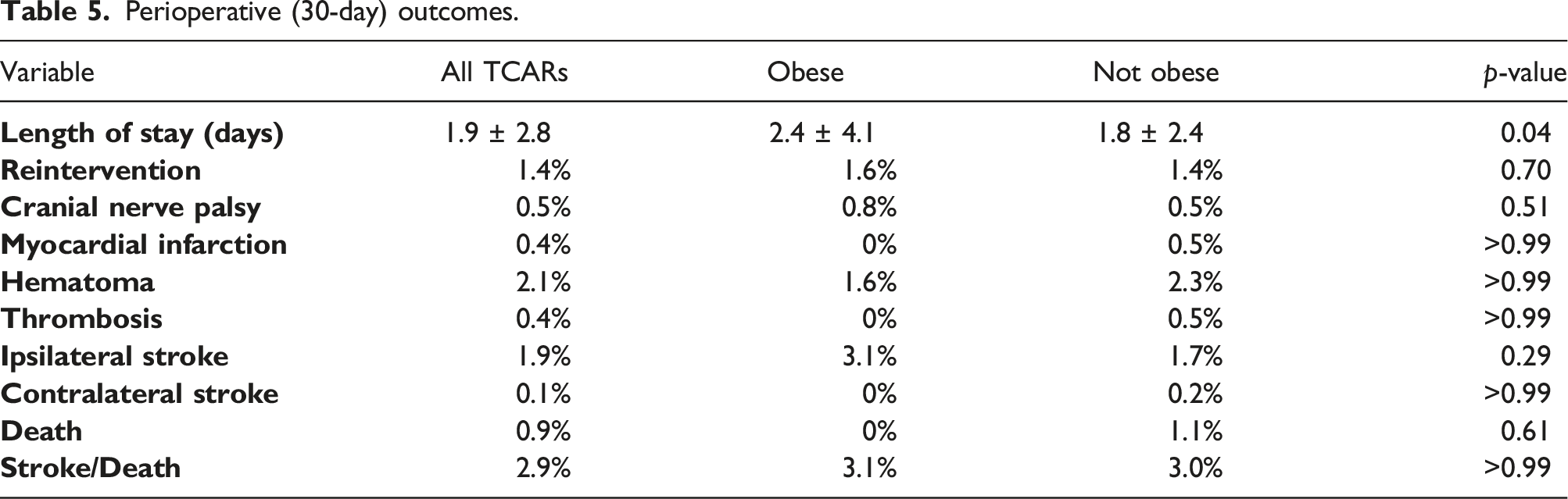
We performed 793 TCAR procedures that qualified for study inclusion within the prespecified time. After applying our obesity definition, 129 patients qualified as obese and were compared to the remainder. There were no significant differences in baseline demographics as comparable Charlson Comorbidity Indices were noted between groups; however, obese patients had a significantly higher prevalence of hypertension, hyperlipidemia, and diabetes. Intraoperative, case complexity in the obese patients did not seem to be increased, as measured by operative time (68.4 ± 23.0 vs 64.2 ± 25.8 min, p = 0.09), fluoroscopic time (4.9 ± 3.2 vs 4.6 ± 3.6 min, p = 0.38), and estimated blood loss (40.6 ± 49.0 vs 46.6 ± 49.4 min, p = 0.22). Similarly, no disparities were observed with respect to ipsilateral stroke (3.1 vs. 1.7%, p = 0.29), contralateral stroke (0 vs. 0.2%, p > 0.99), death (0 vs. 1.1%, p = 0.61), and stroke/death (3.1 vs. 3.0%, p > 0.99) in the 30-day perioperative period. Both cohorts were followed for approximately 1 year (12.0 ± 13.4 vs 11.6 ± 13.4 months, p = 0.76). During this period, rates of ipsilateral stroke (3.1% vs. 2.7%, p > 0.99), contralateral stroke (1.1 vs. 0.8%, p > 0.99), and death (4.7 vs. 6.2%, p = 0.68) were similar.
Conclusions
TCAR performed in the obese population was not more challenging by intraoperative characteristics and did not result in a statistically higher incidence of adverse events in the perioperative phase.
Background
Transcarotid revascularization (TCAR) is a stenting technique utilizing cerebral flow reversal as embolic protection and is increasingly offered by surgeons since the initiation of commercial availability in the mid-2010s 1 Although no randomized controlled trials have established superiority of TCAR over other more established interventions, large registry studies have demonstrated noninferiority of TCAR compared to traditional carotid surgical techniques.2,3 The Society for Vascular Surgery (SVS) extracranial carotid practice guidelines published in 2022 recommends TCAR as the preferred surgical technique in patients with high physiologic or anatomic risk, as defined by the Centers for Medicare and Medicaid Services (CMS). 4
The influence of obesity on carotid revascularization is unclear as studies describing both an increase in adverse events and a non-effect are present.5-8 However, the majority of these investigations focus on the open surgical technique of carotid endarterectomy (CEA). Very little is published regarding the role of obesity on transfemoral carotid stenting (TF-CAS), a percutaneous, minimally invasive technique. 8 Similarly, there does not appear to be any studies evaluating the impact of obesity on the successful application of TCAR and influence on perioperative results. Therefore, this investigation was performed to bridge this gap in knowledge.
Methods
The investigational methods described herein was reviewed and approved by the respective institutional review boards at the Indiana University School of Medicine (IU; #1606299805) and the McGovern Medical School at The University of Texas Health Science Center at Houston (UTHealth) and the affiliated Memorial Hermann Health System (MHHS; HSC-MS-21–0772). Because this was a retrospective review with no direct patient contact, the need for informed consent was waived by both research governing bodies. A retrospective review was performed of prospectively maintained parallel TCAR databases at both institutions. Procedure capture, database population, and auditing were all performed by vascular surgery trainees and faculty independent of the Vascular Quality Initiative TCAR Surveillance Project.
Two cohorts were created based on body mass index (BMI) at a cutoff of 35 kg/m2. We selected this BMI because patients with a weight-related comorbidity and BMI >35 kg/m2 are considered to be obesity class III by the American Society for Metabolic and Bariatric Surgery and therefore qualify for weight reduction surgery. 9 We captured demographics, intraoperative, perioperative, and follow-up courses for these patients and compared our groups with Fisher’s exact and Student’s T tests in JMP software version 16 (SAS Institute Inc., Cary, NC) for categorical and continuous variables, respectively, at an α of 0.05. Mean and standard deviations were reported for continuous variables.
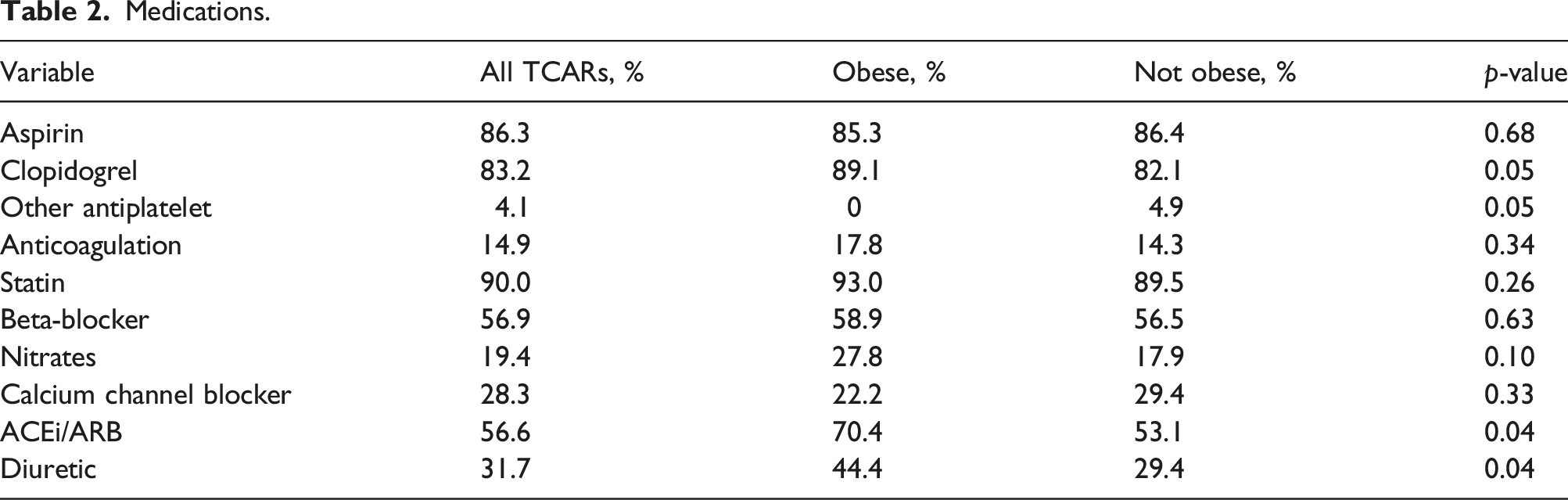
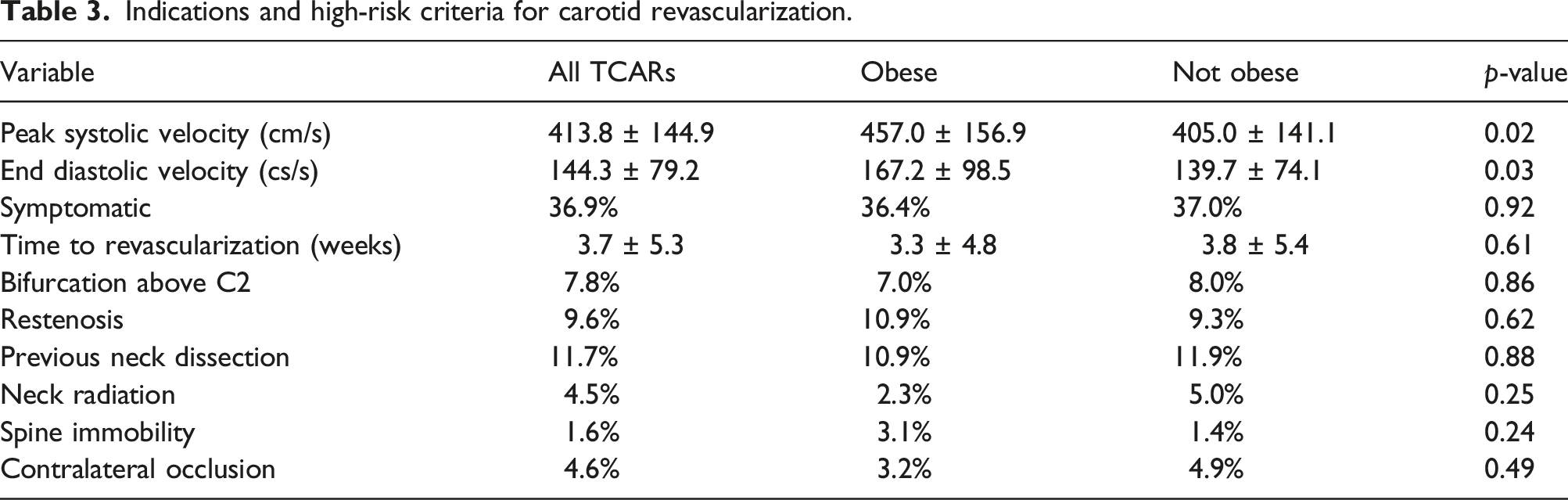
This was a heterogeneous experience and, therefore, the procedure-related decision making was performed independently of institutionally established protocols. However, all patients treated presented with, at minimum, asymptomatic >70% carotid stenosis or symptomatic carotid stenosis >50%, per the latest SVS carotid practice guidelines. 4 IU utilized a more stringent cutoff of 80% stenosis for asymptomatic patients, given continued advances in stroke prevention related to best medical therapy. 10 Although medication management was individualized, in general, we attempted to place all patients undergoing TCAR on dual antiplatelets consisting of aspirin and clopidogrel. If the patient was previously on anticoagulation, then clopidogrel was the preferred antiplatelet to avoid the initiation of “triple therapy.” Unless an absolute contraindication was present, a statin was continued for life postprocedure.
We considered the perioperative period to start the day of the procedure until 30 days after. A postoperative stroke was defined as any new transient or permanent neurologic deficit with evidence of acute ischemia on brain imaging. A myocardial infarction (MI) was any chest pain in the presence of elevated cardiac enzymes more than demand ischemia as adjudicated by our cardiology colleagues. Cardiac enzymes were not routinely screened for after carotid revascularization procedures. 11
Results
Between December 2015 and January 2022, 22 cardiac and vascular surgeons operating at 10 distinct academic and community facilities performed 800 TCAR procedures. The BMI was not available for seven of these patients and, thus, they were excluded from further analysis, leaving a population of 793 patients. (Figure 1) After applying BMI cutoff, we were left with 129 obese patients who underwent TCAR and 664 patients who did not exceed a BMI of 35 kg/m2. Chart shows combined the results of the 793-patient study after applying BMI cutoff.
Demographics, Medications, and Indications
Demographics.
Medications.
Indications and high-risk criteria for carotid revascularization.
Intraoperative
Intraoperative characteristics.
Perioperative (30-Day)
Perioperative (30-day) outcomes.
Follow-Up
The mean follow-up between our cohorts were comparable at 12.0 ± 13.4 vs 11.6 ± 13.4 months (p = 0.76). In the obese patients, we failed to capture a postoperative visit in 27.6% of these patients, while 43.3% completed a minimum of 1 year follow-up surveillance. In the non-obese patients, we did not capture a post-op visit in 22.7%, while 40.5% completed 1 year surveillance follow-up. During this phase, we observed no differences with respect to in-stent stenosis >50% (0.8 vs. 1.1%, p>0.99), stent thrombosis (0.8 vs. 0.8%, p > 0.99), and need for reintervention (2.3 vs. 0.6%, p = 0.09). Last, we observed no variation with respect to ipsilateral stroke (3.1 vs. 2.7%, p > 0.99), contralateral stroke (1.1 vs. 0.8%, p > 0.99), and death (4.7 vs. 6.2%, p = 0.68).
Discussion
As TCAR continues to gain acceptance, largely due to analysis of the TCAR Surveillance Project, we believe it is important to continue to critique and validate these results using alternative datasets. In this institutional study, obesity, defined as exceeding 35 kg/m2, was not associated with statistically increased perioperative stroke or death after TCAR, which seems to persist at 1-year postprocedure. Postprocedural hematoma, cranial nerve injury, and need for reintervention were also comparable between our groups. Last, intraoperative characteristics did not indicate an increased level of case complexity in these large necks.
The effect of BMI on perioperative results after TF-CAS and CEA are not well understood. The literature is populated with conflicting results, both indicating an increase and decrease in perioperative stroke/death.14-16 With respect to CEA, Jackson et al. reported increased perioperative cardiac complications and death in 3645 CEAs derived from the Veteran’s Affairs Surgical Quality Improvement Program in patients with BMI >35 kg/m2. 6 However, a similar study by Volkers et al. utilizing datasets derived from three randomized controlled trials failed to show the same result in symptomatic patients with a BMI >30 kg/m2. 8 The authors also failed to find any effect of obesity on cardiovascular results after TF-CAS. 8 These findings in TF-CAS seem to be corroborated in the perioperative period. 14 However, long-term mortality results in obese patients may be less favorable after carotid stenting. 14 We observed an increased length-of-stay in obese patients after TCAR, which present in the CEA population as well, according to the literature.5,7
An often-debated peculiarity in the literature is whether the so called “obesity paradox” exists with regard to surgical intervention of carotid artery stenosis. 17 This is a condition proposed by some that obesity may be protective against mortality in certain cardiovascular procedures.14,18 Jackson et al. evaluated the results of CEA within the National Surgical Quality Improvement Program, capturing 23,652 cases. 15 In this population, class I obesity was associated with a protective effect against perioperative death (OR, 0.52; 95% CI, 0.26–1.08; p = 0.08). 15 If this effect is real, it could be explained by BMI being a poor approximator of body fat distribution, as abdominal obesity carries a worse prognosis. 19 Alternatively, perhaps a higher BMI in an elderly patient has a better health prognosis compared to geriatric cachexia. 20 Not all studies confirm the existence of this “obesity paradox” and it continues to be debated.6,16 For example, Rovella et al. demonstrated increased plaque instability by histology in patients undergoing CEA, which was independently associated with obesity, putting these patients at higher risk of embolic stroke. 21
Limitations
There are several limitations to this investigation which should be considered when examining the generalizability of the results. This is a retrospective analysis of tandem prospectively maintained institutional databases. As such, variables may be missing or incomplete, leaving the potential for misinterpretation and investigator bias. Next, patients undergoing TCAR at MHHS were captured in separate EMRs for inpatient and outpatient encounters depending on the nature of the practice of the operating surgeon. The authors did not have access to several of the proprietary outpatient medical records, which affected the ability to capture long-term follow-up. Also, we did not have anatomic measurements of CCA depth compared to truncal obesity; BMI can be a crude approximator of neck obesity by itself. Last, the population of the obese patients was small compared to the relatively rare incidence of the adverse events of interest. Therefore, this investigation may not be adequately powered to detect incremental differences.
Conclusion
TCAR in the obese patient can be safely performed with minimal, if any, increased intraoperative complexity by our definitions or a statistically significant elevation in perioperative risk compared to less obese patients. Therefore, indicated carotid revascularization using this minimally invasive technique should not be deferred based on body mass index alone.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclosures
RM is the national principal investigator for the Silk Road Medical-sponsored DW-MRI TCAR study but does not receive any personal remuneration. Silk Road Medical was not involved in the decision to prepare or submit this manuscript in any form and no funding was required for the completion of this study.