
Abstract
Background
Isolated iliac artery aneurysm (IIAA) is an uncommon finding. It, accounts for 0.03% of all patients and 2% of all abdominal aneurysm. Endovascular approach represents the treatment of choice for most patients with IIAA. We reported our experience on iliac aneurysm with no proximal landing zone by simultaneous aortoiliac kissing endovascular (S.A.K.E.) covered stenting.
Methods
This is a retrospective analysis of nine consecutive patients with IIAA with no proximal landing zone, who underwent endovascular kissing covered stenting (Gore®Viabahn®VBX) The median aneurysm diameter was 4.1 cm, with a median 3-mm proximal neck length. In 3/9 aneurysms involving the internal iliac arteries the origin of the internal iliac artery was covered after its embolization and a stent graft extending to the external iliac artery (EIA) was placed. All stents were flared with semi-compliant balloon.
Results
Iliac aneurysm exclusion was obtained in all cases (100%), no graft migration or endo-leak were recorded. The median operative time was 28 min; the median fluoroscopy time was 9 min and a median 70 mL of contrast was used. At a median 24-month follow-up, all patients are alive, and no endo-leak or migration, infection, distal embolization, limb loss were observed. Moderate buttock claudication was experienced in 1/9 patients with internal iliac artery embolization. In 6/9 patients a shrinkage of the aneurysmal sac was recorded after 1 year.
Discussion
Endovascular management of IIAAs cases has been reported in literature and it was confirmed to be safe and successful. The IAA usually progresses into expansion which eventually leads into rupture. Adequate long proximal and distal landing zones were the most important feature related to better outcomes. Short proximal neck (˂10 mm) represents a real challenge for iliac aneurysm treatment and, nowadays, a classical bifurcated aortoiliac endograft deployment represents the treatment of choice. Endovascular repair of isolated CIA aneurysms with no proximal neck is safe and successful using the SAKE stenting technique with VBX adequately flared and it represents effective and minimally invasive alternative to aortobiliac endograft implantation in the treatment of these aneurysms. To the best of our knowledge, this is the first report which describes this approach in the treatment of IIAA with no adequate proximal landing zone. Our approach overcomes the need to aortic bifurcation graft implantation and reduces procedure time, contrast dose and radiation exposure. It also preserves relevant collaterals vessels thanks to inferior mesenteric artery and lumbar arteries sparing. A proximal aortic bifurcation endograft allows proximal sealing to be regained. Large population study with longer follow-up are needed to establish this approach as a new standard.
Introduction
Isolated iliac artery aneurysm (IIAA) is an uncommon finding. It accounts for 0.03% of all patients and 2% of all 1 abdominal aneurysms.2,3 Endovascular approach represents the treatment of choice for most patients with IIAA. These aneurysms are associated with a high risk of rupture and related death.4,5 IIAAs are defined as any dilatation of the iliac arteries >1.5 cm in diameter with an aortic diameter ≤3.5 cm. They are characterised by slow expansion rate and their rupture ranges from 15 to 70% in larger aneurysms. 3 IIAA repair is recommended when the diameter reaches 3–4 cm. 6
Endoluminal exclusion of iliac aneurysms is both feasible and effective when the proximal and distal aneurysm necks are adequate for graft fixation. It is generally contraindicated for those aneurysm with short or absent proximal landing zone.7–10 This suggested a proximal extension approach using a standard aortic bifurcated stent graft. However, some patients could possibly be over-treated, especially when the abdominal aorta is small.
We reported our experience in treating iliac aneurysm with no proximal landing zone by simultaneous aortoiliac kissing endovascular (S.A.K.E.) covered stenting (Gore®Viabahn® VBX).
Methods
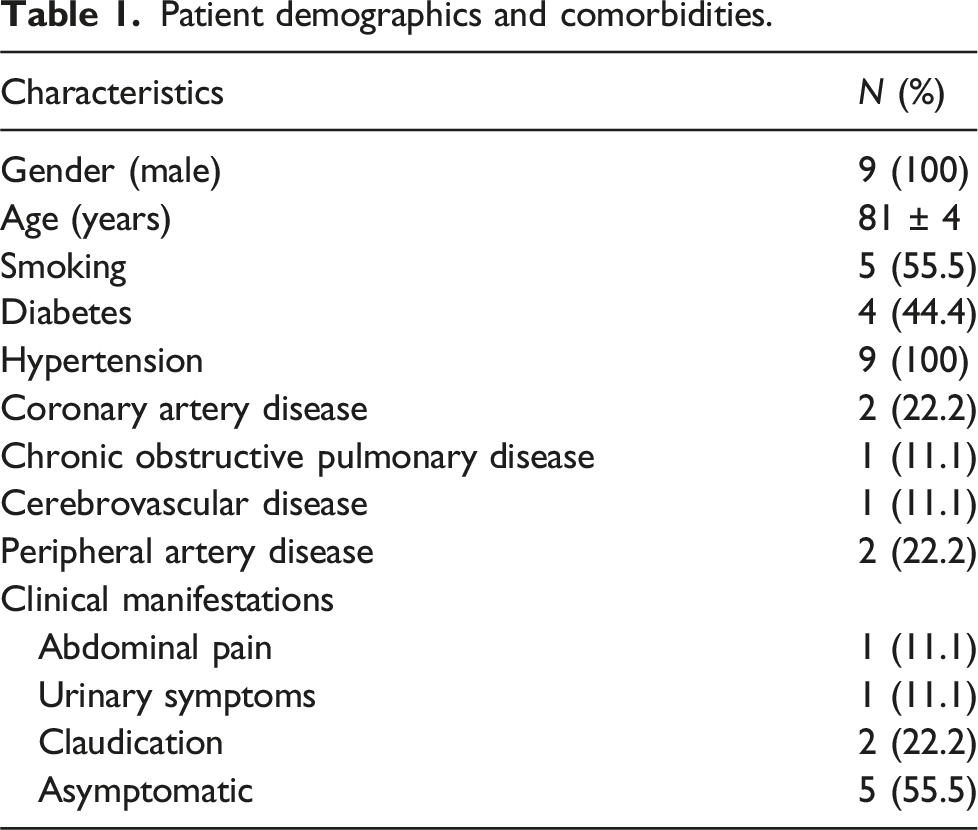
Patient demographics and comorbidities.
The anatomic features of the isolated IAAs.
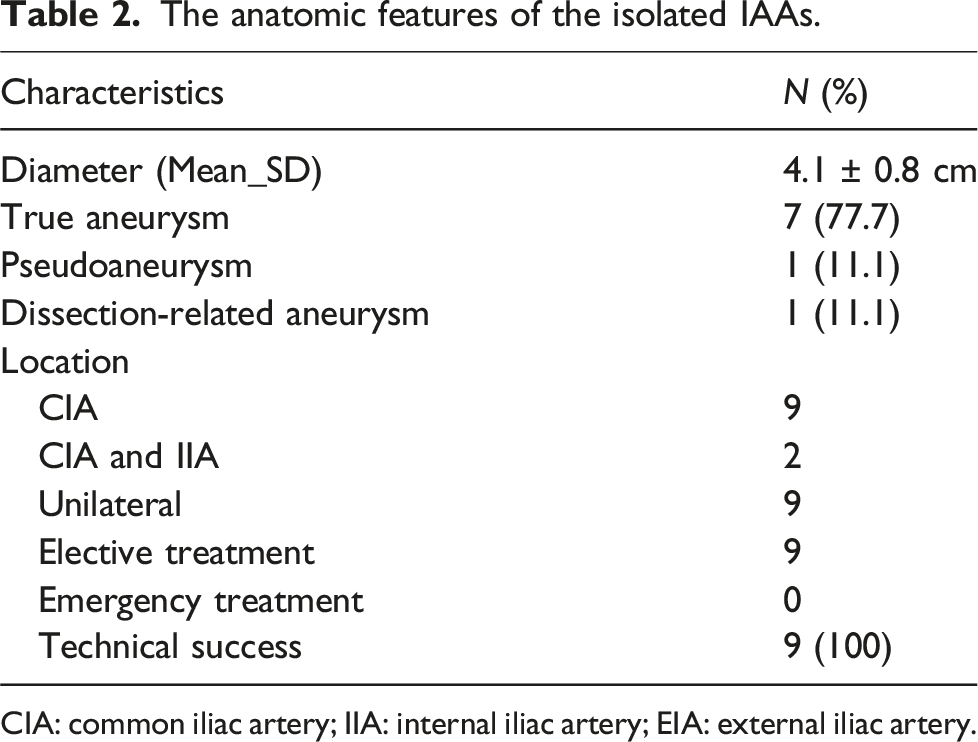
CIA: common iliac artery; IIA: internal iliac artery; EIA: external iliac artery.
The treatment was indicated for IAAs greater than 3.0 cm in diameter, or rapid enlarging (>5 mm in the last 6 months or 10 mm in 1 year). All aneurysms were assessed using computed tomography angiography (CTA). None of the aneurysm involved the aorta. All interventions were performed in local anaesthesia. Femoral access was obtained by bilateral percutaneous approach.
In this group, the median aneurysm diameter was 4.1 cm (range 3.2–4.9), with a median 3-mm proximal neck length (range 1–4). The median diameters of the proximal and distal necks, were 13 mm (range 12–15) and 9 mm (range 8–14), respectively. The median diameter of distal aorta was 20 mm (range 19–24).
A standard kissing aortoiliac covered stent was placed with or without occlusion of the ipsilateral internal iliac artery origin. For 3 aneurysms involving the internal iliac arteries, the arterial branches distal to the aneurysms were embolised with coils and the origin of the internal iliac artery was covered by a stent graft extending to the EIA. Gore®Viabahn®VBX in simultaneous kissing fashion was used in all patients. The stent diameter was 11 mm for all procedures, while the stent’s length ranged from 59 to 79 in contralateral side and 79 mm (minimum) In case the external iliac artery was beyond the landing zone other overlapped stent, ranged 59 to 79 mm were placed. All stents were flared with a semi-compliant balloon (16 mm in diameter). In all patients, 8-F introducer sheath was removed and the femoral artery was repaired by Femoseal closure device.
Anticoagulation therapy was initiated with heparin (5000 IU) administered intravenous once the bilateral femoral introducer deployment was obtained. No anticoagulation therapy was administered after the procedure, and oral double antiplatelet therapy with acetylsalicylic acid (100 mg per day indefinitely) and clopidogrel (75 mg per day for 1 month) was started in all patients. All the patients were discharged on the second postoperative day. Duplex ultrasound was performed at 3, 6, and 18 months after discharge and annually, thereafter during the follow-up period, CTA was performed at 1 and 12 months after procedure and annually, thereafter. The stent-related complications, including migration, fracture and thrombosis, and the shrinkage of the aneurysms were analysed.
The primary objectives of this analysis was to identify the technical success of the VBX stent reconstruction by SAKE technique. The related primary end point was the rate of uncomplicated exclusion of IIAAs from circulation, with restoration of normal blood flow.
The secondary objectives of the study were to identify long term outcomes and safety findings. The related end-points were endoleak and stent migration-rate.
Results
Iliac aneurysm exclusion was obtained in all cases (100% success rate) and no graft migration or endo-leak were recorded. In 3/9 patients, a second stent-graft was deployed to achieve a complete cover of the length and guarantee definitive aneurysm exclusion. The ipsilateral internal iliac artery was occluded in 3 cases due to the orifice involvement in the aneurysm and the graft terminated distal to the EIA (Figure 1). The median operative time was 28 min (range 23–47); the median fluoroscopy time was 9 min (7–17), during which a median 70 mL (range 40–110) of contrast medium was used. The median hospital stay was 3 days for all patients (including pre-surgery assessment). None of the patients was admitted to the intensive care unit. The median serum creatinine levels were stable, postoperatively. the image shows a CT scan preoperative, at 12 and 30 months follow-up with shrinkage of the aneurysmal sac after 12 months.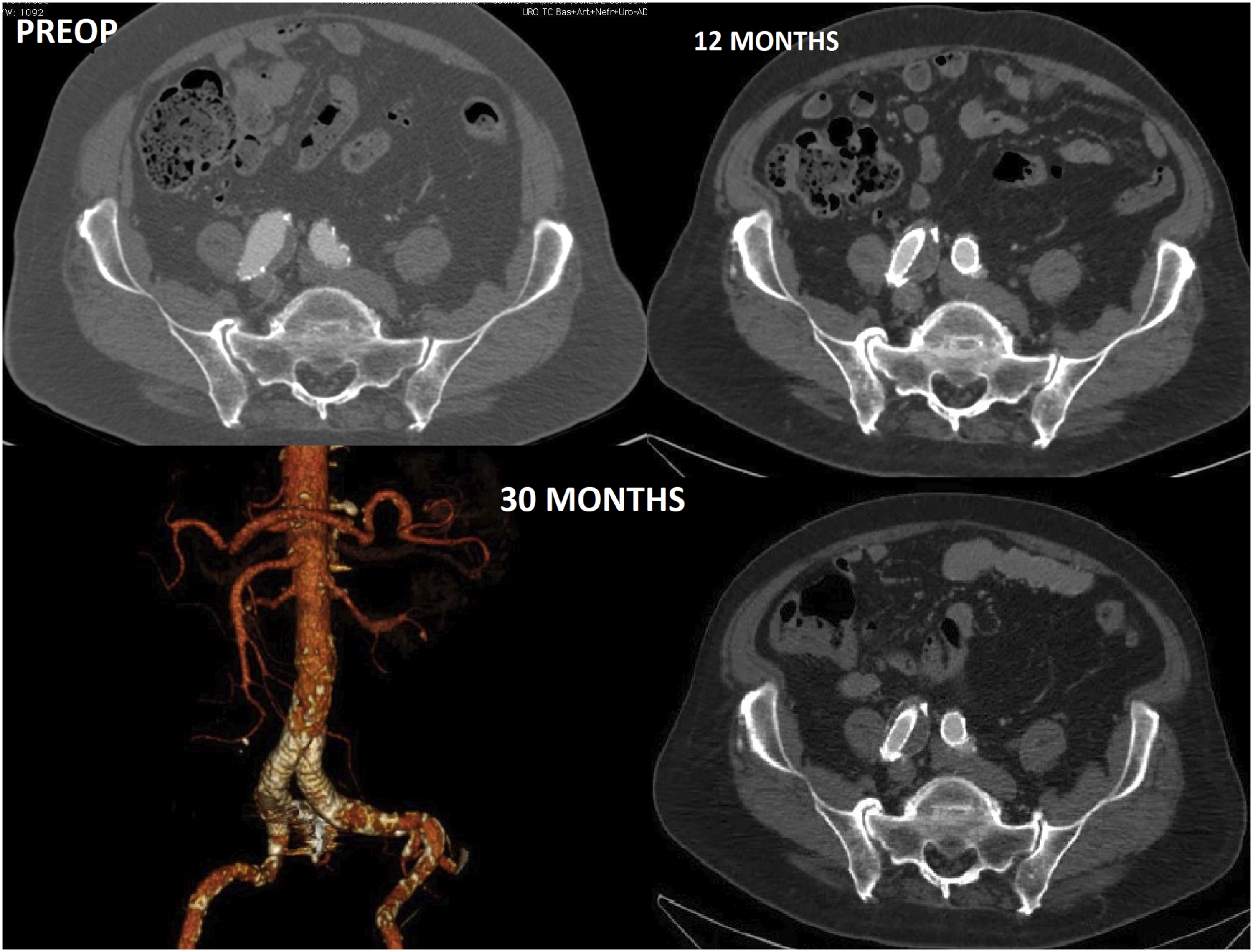
During a median 24-month follow-up (range 12–38), all patients are alive, and no endo-leak or migration has been observed. We observed neither CIA ruptures during follow-up checks, nor any serious complication (infection, distal embolization, limb loss). Moderate buttock claudication was experienced in 1 patient with internal iliac artery embolization. During the follow-up time none of the patients developed aneurysm in different anatomical sites.
The aneurysm diameter did not increase in any subject, while in 6/9 patients a shrinkage of the aneurysmal sac was recorded after 1 year (Figure 1, Video 1), according to the follow-up CT findings. The patency of the contralateral iliac arteries has not been affected.
Discussion
Endovascular management of IIAAs cases has been reported and appeared to be safe and successful.11–13 Data from literature suggest that iliac aneurysms should be treated at smaller diameters. 4
In our study, the good outcomes (100% exclusion rate) and the short length of hospital stay is consistent with previous reports and it supports the efficacy of this procedure. 4
Adequate long proximal and distal landing zones were the most important condition to guarantee a good outcome. In case of short distal landing zone, a more distal landing in the EIA with occlusion of hypogastric artery should be considered. Short proximal neck (˂10 mm) represents the limitation of our proposal. Under this condition, the literature suggests a classical bifurcated aortoiliac endograft deployment. This is associated with higher number of complication and it requires more time, increased the need of contrast dose and radiation. 14
Some authors proposed the specific endograft with the proximal bare stent placed in the aortic bifurcation. 15 Related outcomes are good.
Recent studies showed that iliac side–branched devices produce equal mid-term results to those of the IIA with EIA extension. The use of iliac branched devices showed a lower buttock claudication rate, impotence, and type II endoleak. The iliac side–branched devices should be implanted only with bifurcated aortoiliac endograft. We are currently evaluating the possibility to adapt iliac side–branched endograft to S.A.K.E. technique. This will improve the ability to spare ipogastric artery as well as lumbar and inferior mesenteric arteries.
While open surgery is still a good option for low-risk patients it can be complicated by injury to the adjacent structures such as the ureter, colon, or iliac veins, which can cause sudden, massive bleeding.16–18 Buttock necrosis, spinal cord ischaemia, erectile dysfunction, and ischaemic colitis can be related both to surgical and endovascular treatment of IAA with an associated mortality rate greater than 70%. This suggests that, while the open treatment is still the treatment of choice, there are valid reasons to consider endovascular treatment in those patients with severe comorbidities and poor general conditions.19,20
Endovascular repair of isolated CIA aneurysms with no proximal neck is safe and successful when using the simultaneous aortoiliac kissing endovascular (S.A.K.E.) VBX stenting and adequately flaring. It provides an effective and minimally invasive alternative to the aortobiliac endograft implantation in the treatment of such aneurysms. 21
To the best of our knowledge this is the first case series report which describes this approach in the treatment of IIAA with no adequate proximal landing zone. Our approach overcomes the need to aortic bifurcation graft implantation and it reduces the procedure time, contrast dose, and radiation, furthermore, preserves relevant collaterals thanks to the sparing of inferior mesenteric artery and lumbar arteries. A proximal aortic bifurcation endograft allows proximal sealing to be regained, where needed. The properties of flexibility and radial force varying among different types of Balloon-expandable covered stents (BESGs). The unique mechanical construction of the Viabahn-VBX and its antithrombogenic properties may provide an advantage for sealing in short landing zone. VBX has better outcomes in terms of adaptability within the target vessel. This could be related to the intrinsic nature and material of the device. The shape index is more constant along the stent without localised kinking zones, but the total length and geometry of target vessels must be carefully evaluated. It has been shown that the VBX underwent a greater shortening inside the vessel that pays to maintain its circularity.
In general, the balloon dilation tends to let the stent assume a straight configuration, which is then changed to curved configuration once the balloon is deflated and subsequent flared. Those stent that are more flexible will tend to better adapt to curved anatomy and kissing conformation. The effects of radial force on proximal seal or progressive dilation of the native target vessel have not yet been determined. There are no existing clinical data to confirm long term durability, and future studies should focus on describing the results in a critical manner.
We believe that to obtain a good fixing zone there should be at least 15 mm from the aortic bifurcation, leaving at least 8 cm of free infrarenal aorta; this allows a modular bifurcated stent graft implantation. The flaring VBX stent graft, through a simultaneous proximal balloon over-dilatation allows a good sealing and the reduction of gutter while maintaining the long-term stability of the implant. Moreover, the size of the stent-implants will allow introducers and aortic-endoprosthesis safe placement in case of aortic aneurysm development. Notwithstanding the limitations of this study which includes retrospective single cohort database analysis on a limited number of cases, our results suggest that the new generation of Balloon-expandable covered stents can successfully adapt to aortic bifurcation anatomies. Some technical precautions must be taken when considering the final outcome improvement and the possibility to re-operate during the follow-up. Preliminary data suggests that the VBX offers a better adaptability to several anatomies. The adequate overlap in distal aorta has to be carefully evaluated.
Multicenter series with large population and longer follow-up are required to confirm our encouraging preliminary results.
Supplemental Material
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.