
Abstract
Objective
Even low quantities of iodine contrast media (ICM) could be responsible for exacerbation of a chronic kidney disease (CKD). Aim of this study was to determine whether it is more reasonable to perform endovascular aneurysm repair (EVAR) procedures in patients with initial CKD using CO2 rather than ICM to prevent further kidney deterioration.
Methods
A retrospective analysis was performed at our institution to identify patients with preoperative CKD at initial stage (class G3a-G3b according to KDOQI-KDIGO classification) who underwent either CO2-EVAR or ICM-EVAR. Primary endpoint was renal function evaluation; secondary endpoints were technical success, perioperative complications, hospital stay, and reinterventions and overall mortality at follow-up.
Results
Both CO2-EVAR and ICM-EVAR groups were composed of 21 patients. There were no differences in demographics, anatomy, and comorbidities, apart from worse ASA score in CO2-EVAR group (100% vs 57.1%, p = .001). Preoperative serum creatinine and glomerular filtration rates (GFR) were comparable (1.73 vs 1.6 mg/dl, p = .082 and 39.71 vs 43.04 mL/min/1.73 m2, p = .935). At follow-up (16.7 ± 18.1 months), CO2-EVAR was not associated with significant changes in creatinine and GFR, whereas ICM-EVAR determined a significant increase in creatinine (1.6 mg/dl vs 1.91 mg/dl, p = .04) and decrease in GFR values (43 vs 37.9 mL/min/1.73 m2, p = .04), determining the need for dialysis in one patient.
Conclusions
ICM seems to be a determining factor in worsening renal function; therefore, an effort should be made to standardize the use of CO2 as the contrast medium of choice in patients with initial renal insufficiency undergoing EVAR.
Introduction
Chronic kidney disease (CKD) affects about 10% of the entire world population, with an estimation of about 2 million people on dialytic therapy. 1 The dysfunction of the components of the extracellular matrix (in which metalloproteases play a key role) is a common physiopathogenetic event in vascular and renal damage; this is reflected in the observation that patient population affected by CKD is more at risk of developing vascular diseases, including infrarenal abdominal aortic aneurysm, and its complications. 2 Evidence suggests that the prevalence of CKD is more than 30% among individuals with abdominal aortic aneurysm (AAA) disease compared with the general population. 3 In a recent large observational study, a GFR < 75 mL/min/1.73 m2 was an independent risk factor for AAA over a median follow-up of 13.9 years. 2 CKD also affects outcomes after surgery for AAA: several observational studies have demonstrated that preoperative CKD (glomerular filtration rate (GFR) < 60 mL/min/1.73 m2) is associated with a greater postoperative GFR decline, as well as a higher incidence of GFR reduction (>20%) during long-term follow-up.4–6 Similarly, CKD has been associated with a higher perioperative mortality rate, higher risk of cardiovascular events, and longer hospital stays.7,8
The endovascular aortic aneurysm exclusion procedure (EVAR) has become the most widely used technique worldwide and the first treatment of choice for AAA in those patients with a compatible anatomy, especially if elderly and/or with multiple comorbidities.9–13 This procedure involves the use of iodinated contrast medium (ICM) to enable digital subtraction angiography (DSA), but the risks of nephrotoxicity and allergic reactions may contraindicate its administration. Although technological advances and the use of lower osmolarity ICMs have improved the renal safety profile of EVAR, deterioration of renal function remains the major complication of the procedure with estimated rates ranging from 2%–16% and with an average reduction in creatinine clearance by about 10% in the first year. 14 Therefore, considering that for mild-moderate CKD in patients with aortic aneurysmal disease reported incidence rates are up to 34%,15–17 and knowing that mortality in patients with acute kidney injury (AKI) after EVAR can reach 30%–50%, 18 it is extremely useful to perform the procedure with an alternative contrast medium, such as CO2, which allows to avoid or reduce the amount of ICM administered especially in patients at high risk of developing an AKI or a deterioration in kidney function over time.
The aim of our study is to assess the effects of CO2-assisted EVAR procedures on patients experiencing initial renal function deterioration (stages G3a-G3b CKD), comparing them with a control group characterized by a similar level of renal function impairment but subjected to EVAR using conventional contrast medium.
Materials and methods
Study design, inclusion criteria and endpoints
An automated CO2 injection system (Angiodroid SRL, San Lazzaro, Bologna, Italy) was introduced at our academic Institution in July 2019. From that date to December 2022, 230 consecutive standard EVAR were performed at our center, and the use of the automated CO2 injection system was reserved for patients with CKD or iodine material allergies. Patients were treated for aortic or aorto-iliac aneurysms, anastomotic pseudoaneurysm in previous AAA open surgery, aneurysmatic evolution of previous aortic dissections. Demographic and anatomical characteristics, comorbidities, graft design, procedural, and follow-up data were prospectively collected on a dedicated database.
A retrospective analysis of the database was performed to identify all patients with CKD (defined as a GFR < 60 mL/min/1.73 m2) who underwent EVAR with CO2 as contrast media of choice. Of these, we selected patients at stage G3a (mildly to moderately decreased GFR) and G3b (moderately to severely decreased GFR) according to the KDOQI (Kidney Disease Outcomes Quality Initiative) and KDIGO (Kidney Disease Improving Global Outcome Organization) classification of GFR stages, 19 which were defined as being at “initial” CKD, and constituted the CO2-EVAR study group.
The latter group was compared with an historic cohort of consecutive patients with the same characteristics (stages G3a-G3b CKD) who underwent standard EVAR with ICM (ICM-EVAR group) at our Institution before and during the CO2-EVAR group study period (October 2016 to December 2022), with the aim of conducting a 1:1 comparison between the two groups. GFRs were calculated applying the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) formula. AKI definition followed the Acute Kidney Injury Network (AKIN) criteria. 20
Informed consent was obtained from all patients for the inclusion of their data in our records and for the retrospective analysis of the results. In agreement with national law, owing to the retrospective nature of the present study based on anonymized data, approval of the local Ethical Committee was not mandatory.
Primary endpoint was the decline in renal function at discharge and follow-up compared to the preoperative period. Secondary endpoints were technical success according to reporting standards for EVAR, 21 perioperative complications, hospital stay, and reinterventions and overall mortality at follow-up.
Preoperative workup
Preoperative diagnosis consisted of plain computed tomography (pCT) and Doppler ultrasound (DUS) in the CO2-EVAR group and of a computed tomography angiography (CTA) in the ICM-EVAR group. A preoperative DUS without contrast was utilized to evaluate the patency of aortic collateral vessels (hypogastric and renal arteries) and to measure the extent of thrombus at predetermined landing zones, as this could not be achieved with pCT.
ICM-EVAR group patients underwent day-hospital admission about 10 days before surgery, if foreseen and following nephrological advice, to carry out a functional hydration protocol for the execution of the preoperative CTA.
Preoperative pCT or CTA images reconstructions and planning were performed with a dedicated 3D workstation (TeraRecon Inc., San Mateo, CA, US).
All patients received contrast-induced nephropathy (CIN) prophylaxis before and after EVAR procedure; our center protocol provides, in patients affected by CKD or with risk factors for CIN, hydration with intravenous crystalloids during the 24 h before and 24 h after surgery, with infusion rate correction in elderly patient and patients with heart failure. The protocol is summarized in Figure 1. Institutional hydration protocol for contrast-induced nephropathy (CIN) prevention before and after iodine contrast media (ICM) injection in patients at risk.
Additionally, patients undergoing CO2-EVAR were subministered antispastic drugs (Hyoscine butylbromide, 20 mg) intravenously half an hour before the procedure to reduce gastrointestinal motility and guarantee better visualization of intraoperative CO2 angiographies.
According to Literature, angiotensin-converting enzyme (ACE) inhibitors and angiotensin II receptor blockers were suspended the day of surgery, since the association with the drugs used for induction of anesthesia exposes to intraoperative hypotension potentially deleterious for renal function. 22
All the procedures were executed in an hybrid operating room equipped with a Philips Allura angiography system (Philips Healthcare, Best, The Netherlands). Starting from January 2018, all patients have undergone preoperative cone-beam CT (XperCT) to enhance 3D collimation accuracy with the preoperative pCT using dedicated fusion imaging software. This strategy is implemented to reduce intraoperative fluoroscopy time and the requirement for digital subtraction angiographies.
Postoperative controls
Follow-up consisted of pCT (CO2-EVAR group) or CTA (ICM-EVAR group) at 1 month from surgery and DUS at three and 6 months, annually thereafter.
The laboratory surveillance program of renal function instead, involved serum creatinine measurements at one to 3 months from discharge, and at 12 to 18 months from intervention; measurements taken at 12 to 18 months from the interventions were utilized to assess the primary endpoint at follow-up.
Statistics
The statistical analysis was performed with the “SPSS v. 25 statistical software” (IBM Corporation, Armonk, NY, USA). Quantitative variables were compared through Student t-test and qualitative variables through Pearson χ2 test. Statistical significance was considered for p < .05. Data are presented as n (%) and standard deviation (SD) unless otherwise stated.
Results
Study group
Of the 230 consecutive standard EVAR performed from July 2019 to December 2022, 34 (14.8%) were performed with the aid of the automated CO2 injector, of which 21 (9.1% of the total) met the inclusion criteria (patients with CKD at stage G3a-G3b according to the KDOQI-KDIGO classification, operated on with CO2 as contrast media) and constituted the CO2-EVAR group. We date back to October 2016 to obtain a group of 21 patients with the same renal function characteristics operated on with ICM, which constituted the ICM-EVAR group (total of 42 patients at preoperative stage G3a-G3b CKD out of 460 consecutive standard EVAR procedures performed from October 2016 to December 2022).
Of the 42 standard EVAR included in the study, 39 (92.9%) were performed for aortic or aorto-iliac aneurysms, 2 (4.8%) for an anastomotic pseudoaneurysm in a previous infrarenal AAA open surgery (one in the CO2-EVAR and one in ICM-EVAR group), and 1 (2.4%) for an aneurysmatic evolution of a previous aortic dissection limited to the infrarenal aorta (CO2-EVAR group).
Demographics, clinical, and anatomical characteristics
Preoperative characteristics (demographics, comorbidities, and anatomy).
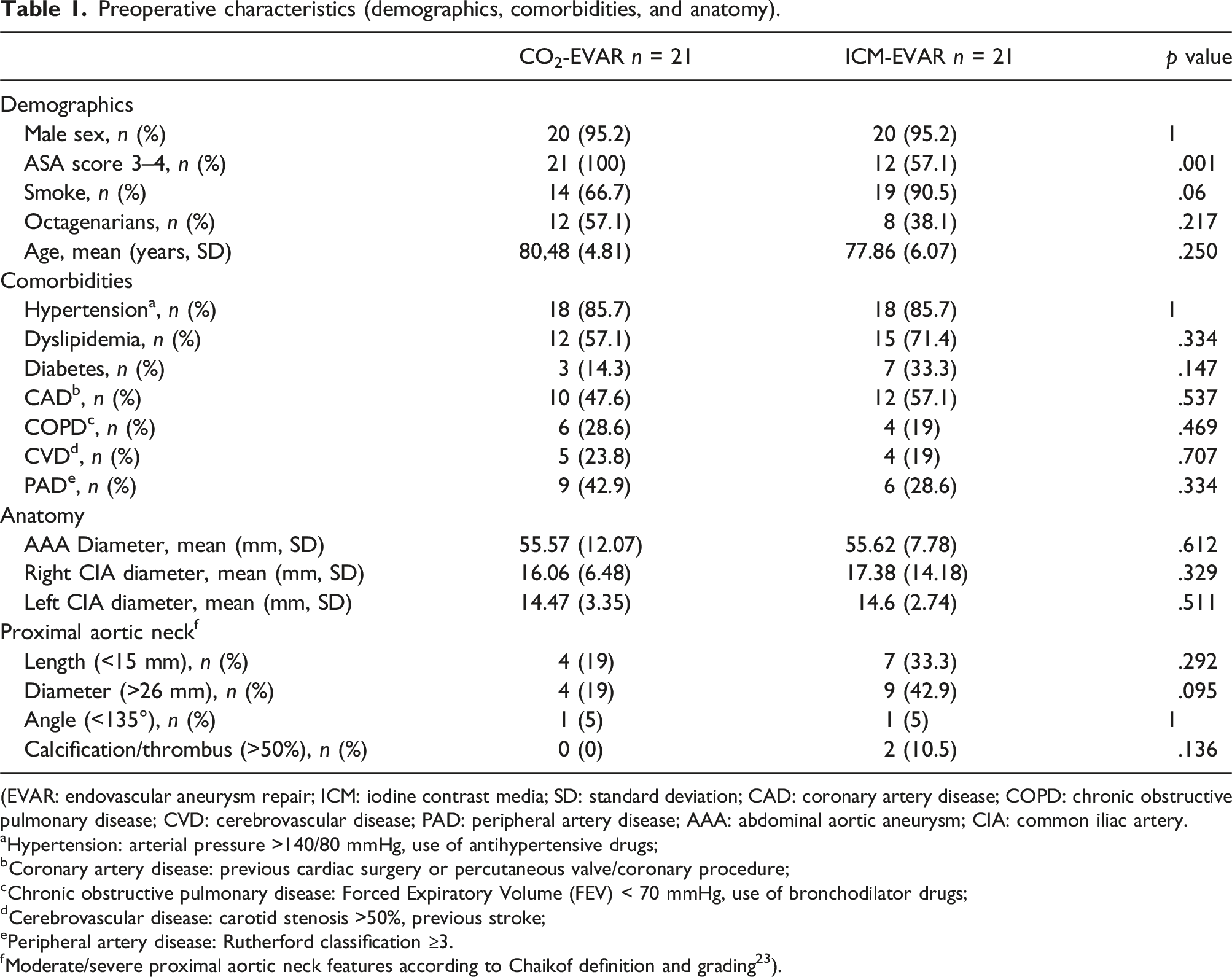
(EVAR: endovascular aneurysm repair; ICM: iodine contrast media; SD: standard deviation; CAD: coronary artery disease; COPD: chronic obstructive pulmonary disease; CVD: cerebrovascular disease; PAD: peripheral artery disease; AAA: abdominal aortic aneurysm; CIA: common iliac artery.
Hypertension: arterial pressure >140/80 mmHg, use of antihypertensive drugs;
bCoronary artery disease: previous cardiac surgery or percutaneous valve/coronary procedure;
cChronic obstructive pulmonary disease: Forced Expiratory Volume (FEV) < 70 mmHg, use of bronchodilator drugs;
dCerebrovascular disease: carotid stenosis >50%, previous stroke;
ePeripheral artery disease: Rutherford classification ≥3.
fModerate/severe proximal aortic neck features according to Chaikof definition and grading 23 ).
Globally, almost all of the cohort were represented by male patients (95.2%), with an average age of 80 (70–87, SD 4.81) years in the CO2-EVAR group and 78 (66–92, SD 6.07) years in the ICM-EVAR group.
As concerning anatomical characteristics, the two groups had comparable aortic neck features judged moderate/severe according to Chaikof definition and grading, 23 in terms of length, diameter, angle, and presence of calcification/thrombus; in particular, only two patients in the ICM-EVAR group (0% vs 10.5%, p = .136) had a thrombus involving >50% of the aortic neck circumference (Table 1).
Renal function in the pre-, peri-, and postoperative period.
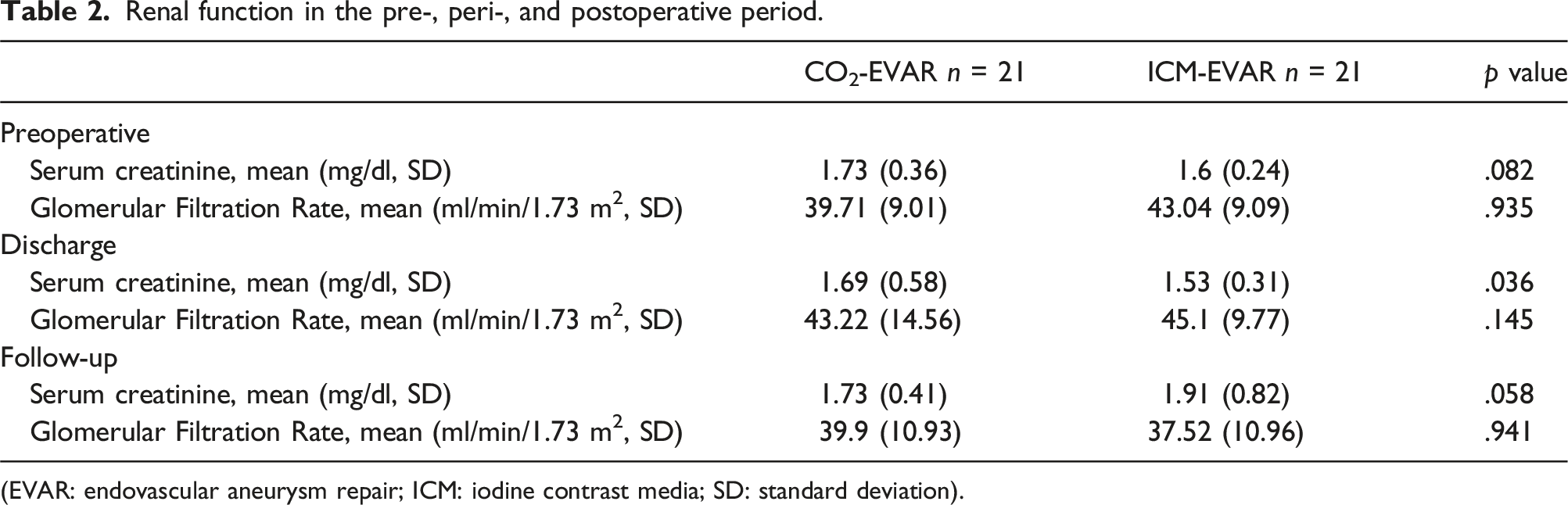
(EVAR: endovascular aneurysm repair; ICM: iodine contrast media; SD: standard deviation).
Intraoperative details
Overall, only one procedure (2.4%), in the ICM-EVAR group, was performed in an urgent setting for the imminent risk of rupture of a fissurated AAA. The absolute majority of patients in the entire sample were operated on under loco-regional anesthesia and through percutaneous accesses.
Multiple consecutive injections of CO2 were either avoided or administered with a minimum waiting time of 30 seconds between each. The CO2-EVAR group did not register any cases of vomiting or hypotension; patients who received high volumes of CO2 injections experienced low-lasting abdominal pain, though without clinically significant consequences.
Supra-renal fixation prostheses were used in 60% of patients in the CO2-EVAR group and in 71.4% of patients in the ICM-EVAR one (p = .440).
Fluoroscopy time was shorter in the ICM-EVAR group, but not statistically significant (19.3 vs 23.4 min, p = .887). In the CO2-EVAR group the average volume of CO2 contrast used was 870 (SD 227.88) ml, while in the ICM-EVAR group the average volume of iodinated contrast was 68.57 (SD 29.54) ml. In the CO2-EVAR group, ICM was used in 5 cases (23.8%) to solve diagnostic doubts arising from the completion CO2 digital subtraction angiography (CO2-DSA), limiting its use to an extremely low dose of 7.67 mL on average. Diagnostic doubts consisted in the operator’s inability to properly visualize the ostium of renal arteries during the proximal deployment of the endoprosthesis, attributable to the presence of air in the transverse colon area or patient’s high BMI, for which a low quantity of ICM was injected to overcome the issue. Completion angiography revealed 7 type II endoleaks in the CO2-EVAR group and 6 type II endoleaks in the ICM-EVAR group (p = .577), with no other types of endoleak detection. There were no access-related complications.
Performed adjunctive procedures were similar between the two groups (p = .747). Bail-out procedures were performed in 2 cases, 1 for each group (4.8% each) and consisted of a hypogastic artery stenting for its unintentional partial coverage (CO2-EVAR group) and an additional iliac limb stenting for prosthetic limb infolding (ICM-EVAR group). No surgical conversions were recorded and the technical success was 100% in both groups; when CTA was not feasible, the EVAR planning protocol consisting of pCT and DUS demonstrated 100% accuracy in defining the proximal and distal landing zones of the graft (Figure 2). EVAR planning on plain computed tomography (pCT) scans reconstruction.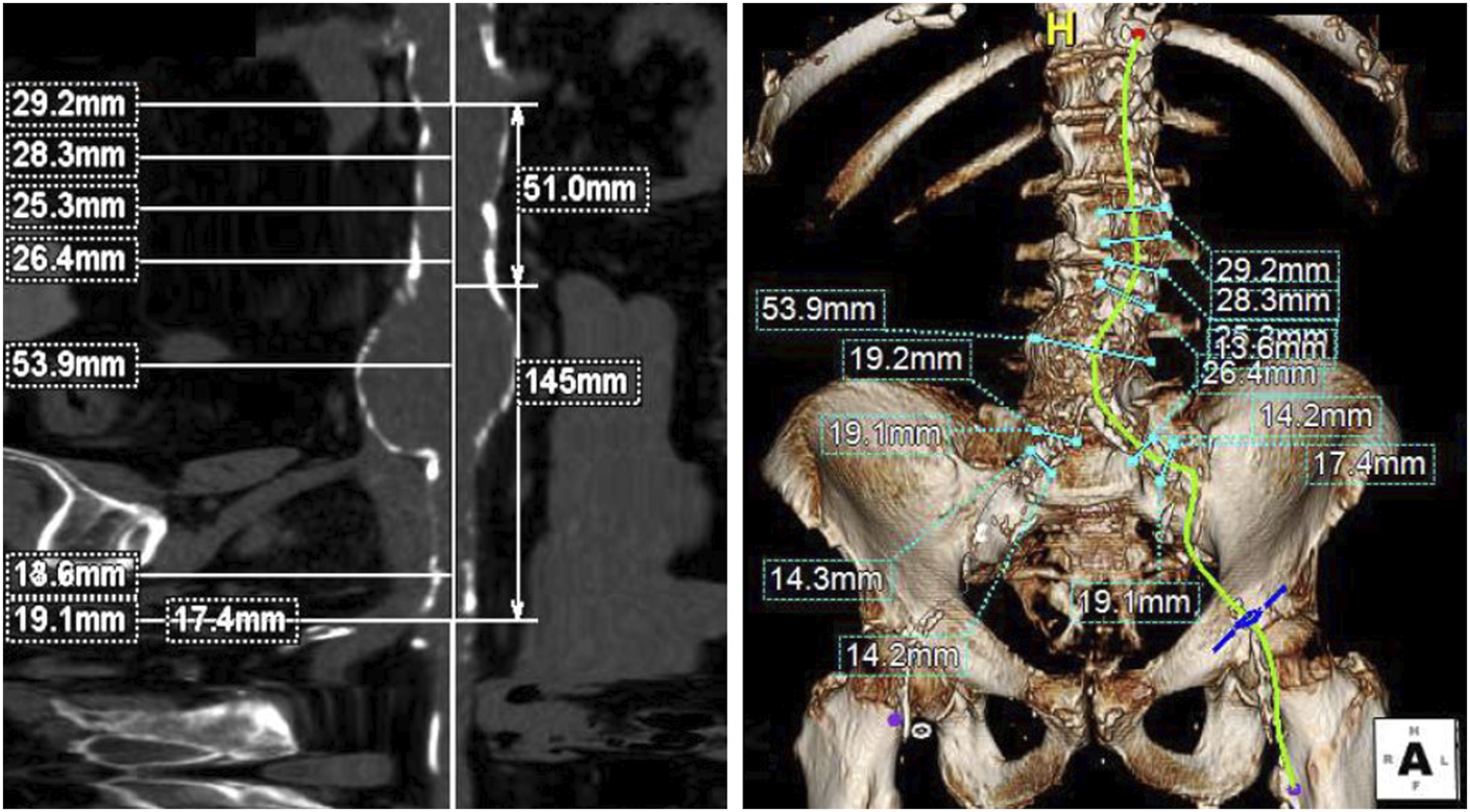
Intra- and perioperative details.
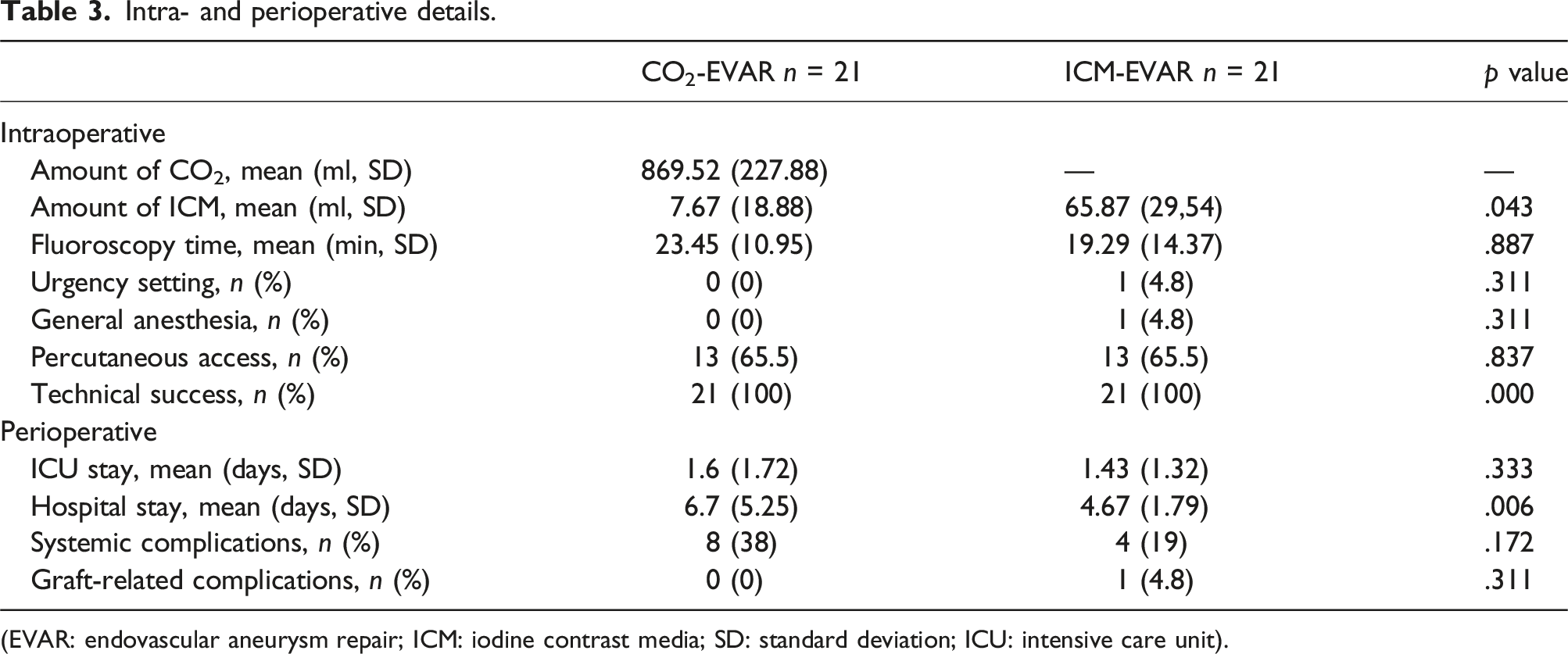
(EVAR: endovascular aneurysm repair; ICM: iodine contrast media; SD: standard deviation; ICU: intensive care unit).
Early outcomes
In the perioperative period (<30 days) we recorded one reintervention on a patient from the ICM-EVAR group who presented with iliac limb thrombosis and was treated with thromboendarterectomy of the femoral bifurcation and iliac thrombectomy through a Fogarty catheter. No perioperative deaths occurred.
Patients in the CO2-EVAR group had longer hospital stays (6.7 days vs 4.6 days, p = .006), however without statistically significant differences in terms of mean length of stay in the intensive care unit (1.6 vs 1.4 days, p = .333). Patients in the CO2-EVAR group experienced more systemic postoperative complications when compared to the ICM-EVAR one, even if not statistically significant (38% vs 19%, p = .172). Details are listed in Table 3.
Renal function variations according to time period (preoperative vs perioperative phase, and preoperative vs follow-up phase).
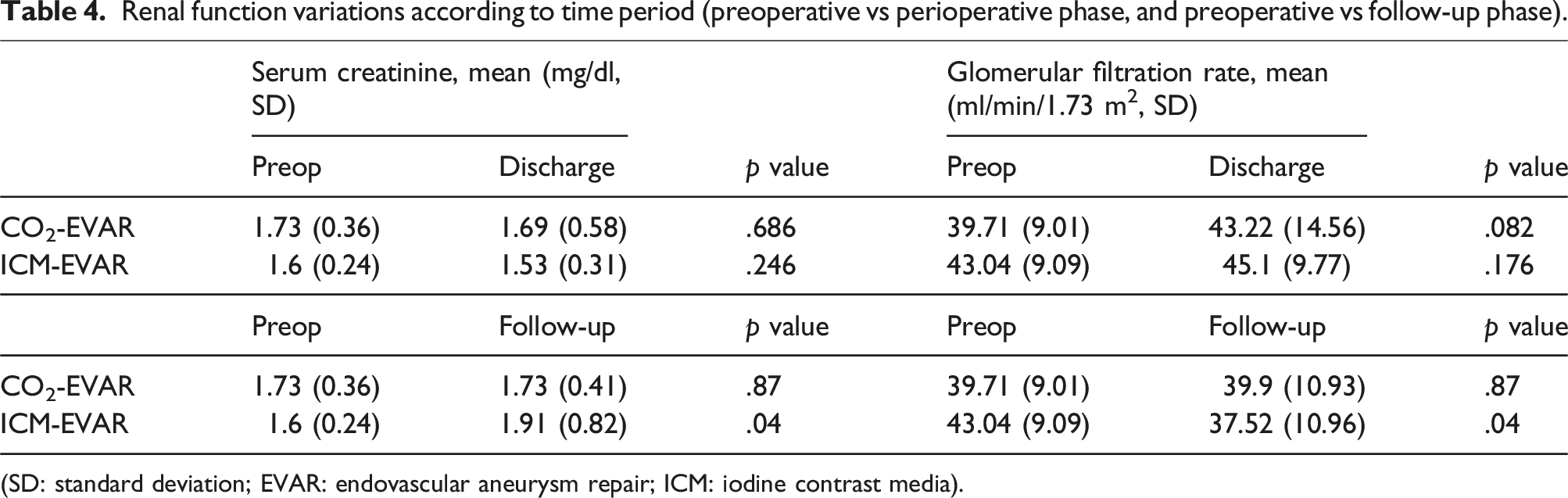
(SD: standard deviation; EVAR: endovascular aneurysm repair; ICM: iodine contrast media).
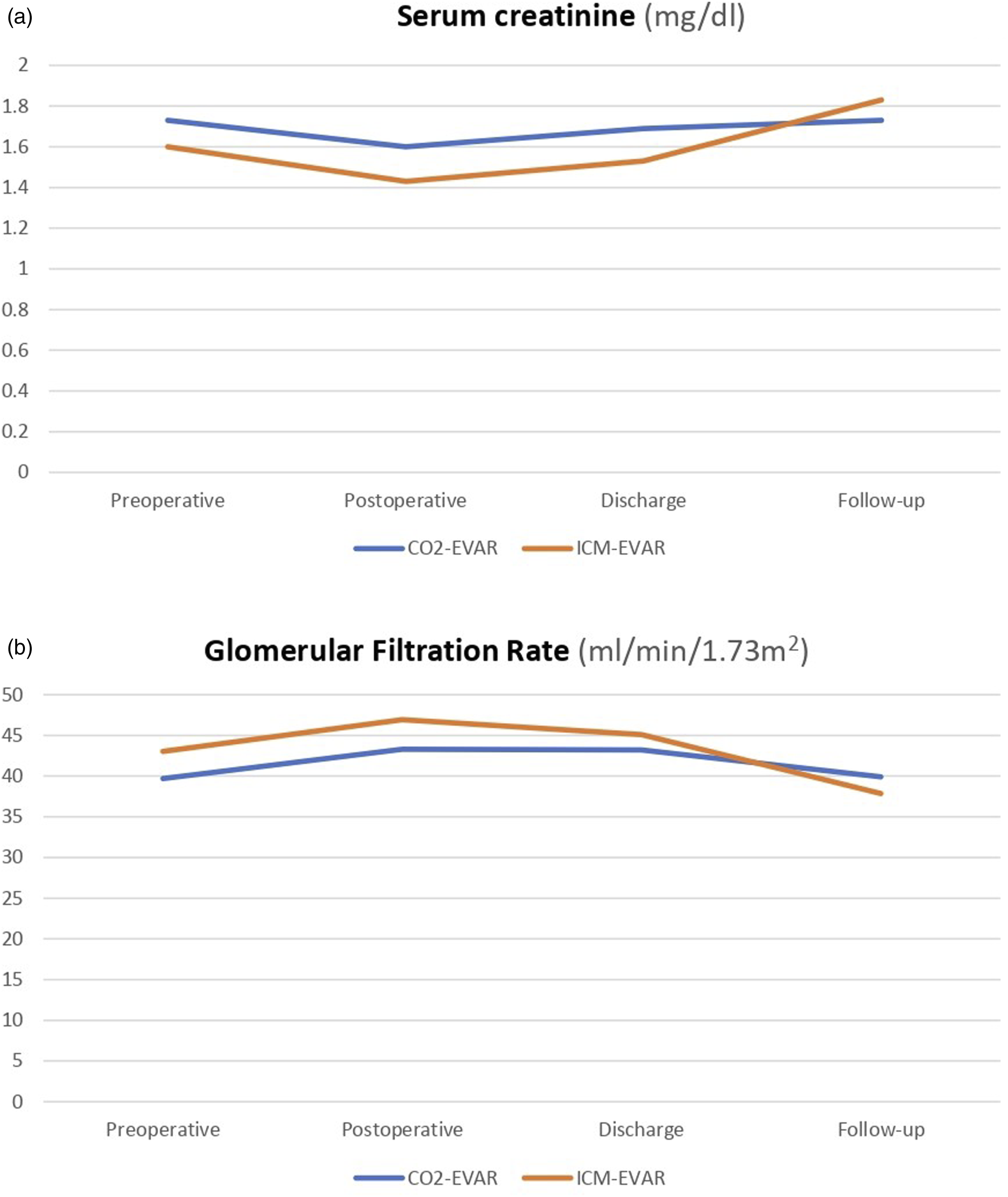
Graphical representation of renal function temporal flow (A: serum creatinine and B: glomerular filtration rate).
One-year follow-up
Mean instrumental follow-up time was 12.8 (SD 14.8) months, while mean laboratoristic follow-up time was 16.7 (SD 18.1) months. One patient in the CO2-EVAR group did not adhere to the follow-up programme.
There were no cases of thrombosis, migration and/or surgical conversion. Type II endoleak rate was 11.8% in the CO2-EVAR group and 28.6% in the ICM-EVAR group, with no statistically significant difference between the two samples (p = .206). One reintervention was recorded in the ICM-EVAR group, for a type IA endoleak treated with an off-the-shelf thoraco-abdominal stent graft implantation, which did not determine significant renal function worsening. In addition, there was a single case of aneurysm-related death due to presumed rupture of a patient from the CO2-EVAR group, which occurred 2 months after surgery. This patient had a fusiform aneurysm with a preoperative maximum diameter of 97 mm, and a type II endoleak from lumbar arteries was evident at the final completion angiography. Overall mortality was higher in the ICM-EVAR group (28.6% vs 14.3%), but the difference was not statistically significant (p = .259).
In the CO2-EVAR group, serum creatinine at one-year follow-up returned to values comparable to preoperative ones (1.73 mg/dl vs 1.73 mg/dl, p = .87), while in the ICM-EVAR group it statistically worsened (1.6 mg/dl vs 1.91 mg/dl, p = .04). As concerning GFRs, values were similar in the CO2-EVAR group (39.7 mL/min/1.73 m2 vs 39.9 mL/min/1.73 m2, p = .87), while there was a worsening in the ICM-EVAR group (43.04 mL/min/1.73 m2 vs 37.52 mL/min/1.73 m2, p = .04). Renal function variations between preoperative period and follow-up are presented in Table 4 and Figure 3.
One patient in the ICM-EVAR group (4.8%) progressed to end-stage CKD during follow-up, therefore requiring dialytic therapy. The latter patient did not have a preoperatively fissured AAA and did not require any reinterventions during follow-up.
Discussion
The progression of renal dysfunction after EVAR seems to be related to multiple factors, such as embolizations from aortic endoluminal maneuvers or the use of ICM in the peri- and postoperative period. While it is not entirely possible to eliminate the potential for embolizations, even with meticulous patient selection and careful procedure execution, avoiding the administration of ICM to patients undergoing EVAR is arguably the sole contributing factor to renal dysfunction that could be entirely prevented.
Vascular surgeons have traditionally been trained exclusively on the use of ICM for endovascular procedures and very few are familiar with the use of alternative contrast agents. Recently, the validation of performing EVAR with the aid of CO2 has been supported by an increasing number of significant studies. These papers consistently report positive outcomes associated with this procedure and offer guidance on optimal operative protocols to minimize CO2-related complications and enhance image quality, even in the urgent setting.24–27
In our initial experience with the use of CO2 as a contrast agent for EVAR, we did not highlight any statistically significant differences with the group of patients who underwent ICM-EVAR in terms of intraoperative mortality, adjunctive procedures, surgical conversions, unidentified type 1 or type 3 endoleaks, and number of reinterventions immediately and during follow-up. The shorter operative time in terms of fluoroscopy for ICM-EVAR compared to CO2-EVAR, even if not statistically significant (19.3 vs 23.4 min, p = .887), reflects a reasonable increased familiarity with the traditional technique, which for the CO2 procedure required a learning curve to fulfill the time gap.
Patients in the ICM group had a shorter mean hospital stay than the CO2 group (4.7 vs 6.7 days, p = .006) and this difference reflects a greater global clinical impairment of patients selected for EVAR-CO2, as expressed by the ASA score of these patients which was higher on average (ASA score 3–4: CO2-EVAR 100% vs ICM-EVAR 57.1%, p = .001). This finding is likely an expression of the tendency of our center to reserve, at least initially in our experience, the CO2 angiography technique only for patients for whom it was strictly necessary by virtue of a greater impairment of renal function, on the basis of a lower absolute value of glomerular filtration, although all patients of both groups were selected for being at the same CKD stage (stage G3a-G3b).
On the other hand, from the comparison of anamnestic data there were no statistically significant differences between the two groups in terms of individual comorbidities and, although more complex from an anesthesiological point of view, we did not detect a statistically significant difference in terms of average length of stay in the intensive care unit (1.4 vs 1.6 days, p = .333), and instead the overall mortality was even slightly better (28.6% in the ICM-EVAR group vs 14.3% in the CO2-EVAR group), although not reaching statistical significance.
CO2 provides all the information necessary to complete an EVAR procedure, with the advantages of not causing known renal or systemic toxicity, not being allergenic, being widely available in hospitals at extremely low cost and, when used with the proper knowledge, it is an extremely safe negative contrast medium. 28 The technical suitability of CO2 angiography for EVAR and its beneficial effect on the preservation of renal function have been suggested during the last decade in several publications;29–31 nevertheless, it still constitutes a non-standardized technique for patients with CKD, although a growing number of studies is demonstrating its advantages in maintaining renal condition.32–34
In patients with pre-existing renal insufficiency or severe iodine contrast allergy, it is advisable, if not mandatory, to use alternative, non-nephrotoxic or hypoallergenic diagnostic methods during EVAR. As such, intravascular ultrasound (IVUS) and transabdominal ultrasound were technically successful and suggested to reduce the amount of ICM used during EVAR.35,36 Nonetheless, IVUS has failed to gain popularity perhaps due to its technical complexity, cost, and limited availability in many surgical centers.
The degree and rate of renal function deterioration after EVAR remain poorly defined. As previously mentioned, a large EVAR study showed an average decrease of approximately 10% in creatinine clearance during the first year after surgery. 14 However, another study revealed a slight recovery of renal function during the second year after surgery, but with no return to preoperative levels. 37 A recent retrospective analysis of EVAR I and II trials suggests that the rate of GFR decrease after EVAR is slow and that the increased rate of renal function deterioration after EVAR is associated with stent graft complications. 38 A plausible explanation for this association may be the administration of ICM required for additional imaging studies during follow-up as well as endovascular procedures required to manage any post-implantation complications, so this could be another valid reason to avoid ICM in EVAR patients. Interestingly, the latter cited studies suggest that the presence of renal insufficiency prior to EVAR is not associated with an increased risk of long-term renal dysfunction. This finding is counterintuitive, since pre-existing renal insufficiency is an important predictor of postoperative renal insufficiency in patients undergoing EVAR, and renal insufficiency itself is associated with a significant increase in hospital mortality.39,40
Our data suggest that CO2-EVAR in patients with pre-existing moderate renal dysfunction (KDIGO class G3a and G3b) was not associated with significant changes in mean GFR over time (39.7 vs 39.9 mL/min/1.73 m2, p = .87), whereas among ICM-EVAR patients, one suffered of a postoperative AKI episode and GFR generally worsened at follow-up (43 vs 37.9 mL/min/1.73 m2, p = .04), determinig the need for hemodialityc therapy in one case. This is an observation compatible with Literature experiences, among which that of Criado et al. that suggests an important role for CO2 in the reduction of ICM-associated nephrotoxicity in patients undergoing EVAR, recently confirmed by Busutti et al. who showed a significant worsening of renal function in patients treated with standard dose of ICM, even at 1 year of follow-up.41,42 Contrary to the aforementioned papers, we took a different approach in our study by categorizing patients based on the preoperative presence and degree of CKD. We accomplished this by matching patients with similar preoperative renal conditions, aiming to ensure a fair comparison of the results. Our aim was to discern the specific advantages of avoiding ICM in patients already experiencing initial CKD, with the goal of preventing further deterioration of kidney function. This approach points at directing CO2-EVAR specifically to patients who might genuinely benefit from ICM avoidance, which might be the case of patients with an already impaired kidney function. 43
Unfortunately, the long-term nephroprotective effects related to the non-use of ICM during EVAR cannot be reduced to the procedural time alone, but should be extended to the follow-up as well, relying on the use of ICM-free instrumental surveillance methods, such as contrast-enhanced US (CEUS), magnetic resonance imaging (MRI), and pCT.
Study limitations
The present study has several limitations. First, it is a single center retrospective experience, with a limitation in patient sample size, which on the other hand is the direct consequence of limiting the study population to that of patients with “initial” CKD (stages G3a and G3b), thus excluding all the other CKD patients presenting with different renal conditions (stages G1, G2, G4, and G5); follow-up time is limited because of the recent introduction of automated CO2 injection systems in our center.
It was essential to include patients operated on before the introduction of CO2 in our practice (July 2019) to facilitate a 1:1 matched comparison of ICM-EVAR with CO2-EVAR. This necessity might have impacted the results due to potential minimal variations in surgical practices and endovascular materials during the study period.
A significant limitation arises from the possibility that pre- and postoperative CTAs performed in the ICM-EVAR group might have substantially contributed to renal function deterioration, even if carried out under an hydration protocol. Consequently, assessing the true positive effect of CO2-EVAR on renal function preservation is challenging, given the potential influence of ICM during preoperative CTA and postoperative controls in the ICM-EVAR group. Unfortunately, we could not exclude or evaluate this impact due to the retrospective nature of the study and the unavailability of this data.
Likewise, the pre-, intra-, and postoperative administration of liquids performed to satisfy institutional hydration protocols might have altered creatinine and GFR values, which could explain the slight postoperative kidney function amelioration registered in both groups after surgery.
Another relative limitation is the selection defect of patients undergoing CO2-EVAR, on average more compromised from a global clinical level; however, this bias did not particularly affect the purpose of the study, since patients undergoing ICM-EVAR, although less compromised according to the ASA scores, had the same preoperative renal function performances, and presented a significantly worse decline in renal function over time anyway.
Conclusions
Renal failure is a major predictor of mortality after endovascular repair for AAA. According to our findings, patients undergoing ICM-EVAR had renal complications in both postoperative and follow-up periods, with a significant deterioration in renal function in the long-term, which could have played a role in determining a slightly higher mortality rate in comparison to patients who underwent a CO2-EVAR. In conclusion, ICM seems to be a determining factor in worsening an already compromised renal function; therefore, CO2 should be standardized as the contrast medium of choice in patients with initial renal insufficiency, for whom an ICM-free “pathway” from diagnosis to postoperative surveillance would be desirable. 44
Footnotes
Author contributions
Authors FV and DE have given substantial and equal contributions to the conception and the design of the manuscript and have shared first authorship; authors ATF, WD, RF, SDB, MC, and NB contributed to acquisition, analysis and interpretation of the data. All authors have participated to drafting the manuscript, authors ATF and RP revised it critically. All authors read and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.