
Abstract
Background
Intravascular lithotripsy has proven to be safe, less invasive, and effective for coronary and peripheral arteries, and the indication has been extended to the aortic district but there is still little evidence in the literature as only a few cases have been described so far.
Method
We report a case of intravascular lithotripsy of the infrarenal aorta due to coral reef, chronic occlusion using a single Shockwave M5 + balloon, followed by a covered stent deployment. The aortic bifurcation and common iliac arteries presented hemodynamic calcific lesions, which were prepared singularly with lithotripsy before aorto-iliac covered stenting in kissing configuration. The aortic length from which arises the inferior mesenteric and lumbar arteries was left uncovered preserving their patency.
Result
In this case, a single shockwave balloon was sufficient to treat successfully and safely the aortic occlusion by heavy calcific lesions. At 1 and 6 months follow-up, the patient had no clinical symptoms, and the ultrasound assessment showed a triphasic waveform at the common femoral arteries bilaterally and confirmed the patency of the stent grafts.
Conclusion
Selective assisted lithotripsy of heavy aortic and iliac vessels is possible, but definitive outcomes have yet to be supported by the literature.
Keywords
Introduction
Coral reef aorta and aorto-iliac heavy calcific lesions have been traditionally treated with endarterectomy or bypass grafting and have proved to be successful but with high mortality and morbidity rates. On the other hand, the endovascular approach with aorto-iliac kissing stents has provided similar outcomes to open surgery in terms of primary patency and limb salvage but with lower morbidity and mortality rates. 1 The technical success of the endovascular recanalizations can be significantly compromised in patients with complex and heavily calcified lesions at any anatomical segment either abdominal or lower limb arteries.2,3 For these selected patients, the vessel preparation with Intravascular Lithotripsy (IVL) may be advantageous and in some situations essential for the technical success of the endovascular procedure. IVL has proven to be a safe, less invasive, and effective procedure in coronary and peripheral arteries.4–6 However, in the recent literature, only few case reports have described its use for aortic lesions. We report a case of complete, severely calcified, 40 mm-long obstruction of the infrarenal aorta. Moreover, the aortic bifurcation presented with severe stenosis due to calcific lesions involving both the common iliac arteries (CIA). These lesions underwent selective IVL and covered stenting. Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Case presentation
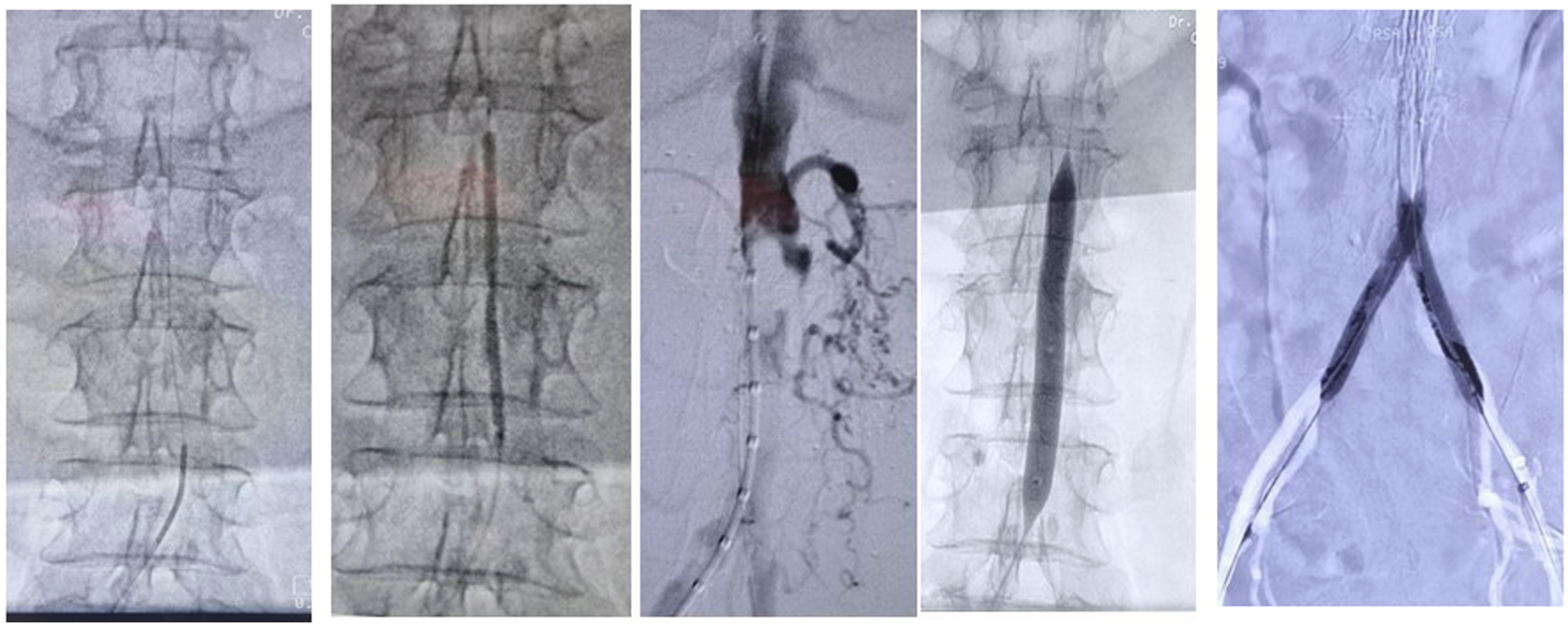
A 73-year-old female presented with bilateral peripheral artery disease of the lower limbs (Rutherford category 4 to the right, and 3 to the left). At physical examination, no femoral pulses were palpable, and at duplex ultrasound (DUS) examination, the flow at the common femoral arteries showed a monophasic waveform, ankle/brachial index (ABI): 0.4 left limb, 0.6 right limb. The preoperative computer tomography angiography (CTA) showed coral reef calcific lesions with total occlusion of the infrarenal aorta for a length of 40 mm and significant calcific stenosis of both common iliac arteries (CIA) extended to the aortic bifurcation, Figure 1. Notably, the aortic wall between the infrarenal obstruction and the bifurcation was free from disease, and the CTA scan demonstrated a patent inferior mesenteric artery (IMA) and two pairs of lumbar arteries originating from this free-from-disease aortic segment. Under general anesthesia and ultrasound guidance, a trans-femoral 8-Fr introducer sheath was percutaneously placed bilaterally (12 cm ULTIMUM™ EV INTRODUCER, Abbott, Plymouth, MN, USA). The patent aortic lumen, cranial to the obstruction was accessed intraluminally using a 0.014-inch hydrophilic guidewire (V-0.014, Boston Scientific, USA) with the aid of a 4-Fr catheter (VER Tempo-Aqua, Cordis, Miami Lake, FL, USA). A pre-dilation with a low-profile balloon 3 × 60 mm (Armada14, Abbott, Plymouth, MN, USA) was performed, to allow the progression of a 5-Fr Pig Tail catheter (Merit Medical, South Jordan, UT, USA). The intraoperative angiogram confirmed a complete 40 mm-long obstruction of the infrarenal abdominal aorta, Figure 2. A Shockwave M5 + balloon 8 × 60 mm (Shockwave Medical Inc., Santa Clara, CA, USA) was advanced and progressively inflated to 6 atm for one cycle of 30 pulses followed by two cycles of 30 pulses at 10 atm. Next, IVL was performed singularly for the preparation of each CIA. Finally, the procedure was completed by placement of a balloon-expandable covered stent (Advanta V12, 12 × 41 mm, GETINGE, La Ciotat, France) in the infrarenal aorta, sparing the origin of IMA and lumbar arteries, while two aorto-iliac balloon-expandable covered stents (Advanta V12, 8 × 59 mm) were positioned in kissing configuration, Figure 2. Angiogram confirmed patency of the stent grafts, IMA, and lumbar arteries arising from the distal abdominal aorta, Figure 3. The hemostasis was performed by percutaneous closure devices (ANGIO-SEAL VIP 8-Fr, Terumo Medical Corp., Somerset, USA). The in-hospital stay was uneventful and full recovery of the clinical symptoms (ABI: 1 left limb, 0.9 right limb). Dual antiplatelet therapy was set (aspirin 100 mg + clopidogrel 75 mg) daily for one month and then maintained on single antiplatelet therapy (aspirin 100 mg). At 1, 6, and 12 months follow-up, the patient had no clinical symptoms, and the DUS assessment at the CFA showed a triphasic waveform bilaterally and confirmed the patency of the stent grafts. Preoperative CTA showing: a coral reef chronic obstruction of the infrarenal aorta, associated to highly calcified stenosis of aortic bifurcation and both common iliac arteries. From the left position of the 0.014-inch wire in the aorta, pre dilatation with a 3 mm diameter balloon, intraoperative angiogram confirmed a complete 40 mm-long obstruction of the infrarenal abdominal aorta. Single Shockwave M5 + balloon 8 × 60-mm and single aortic covered stent and aorto—iliac kissing stenting. Completion angiogram and reconstruction imaging confirming the patency of the covered stents and patency of inferior mesenteric and lumbar arteries arising from the distal abdominal aorta.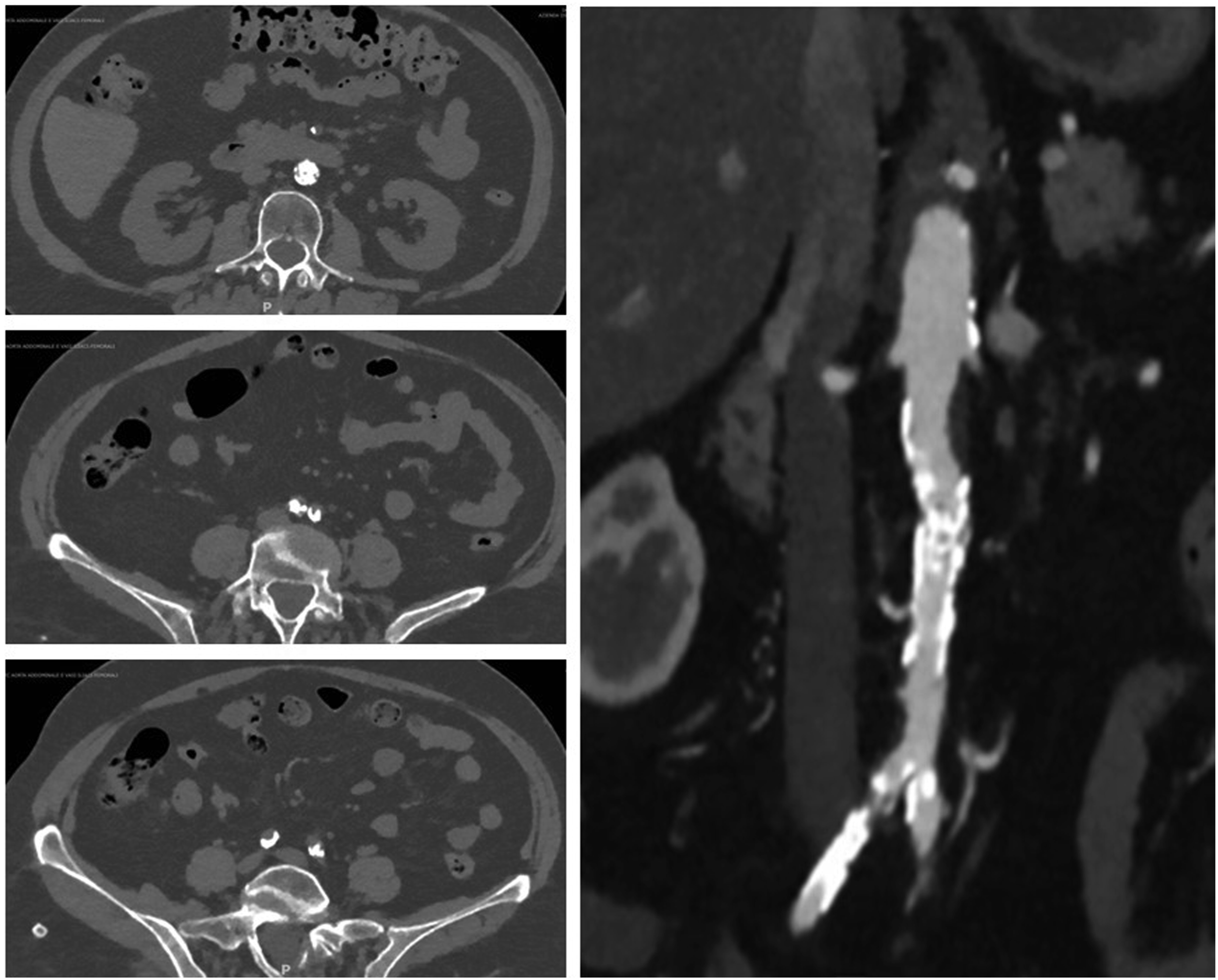

Discussion
The coral reef aorta and complex calcific aorto-iliac lesions have been treated by endarterectomy or bypass grafting with good long-term outcomes but with a high mortality and morbidity rates. The endovascular approach for the same lesion is a less invasive alternative and beneficial in elderly patients and with multiple comorbidities. However, the degree of calcium burden has been proven to be a predictor of technical failure in all arterial segments and thus the vessel preparation using lithotripsy could be beneficial in this aspect.4,5 IVL of intraabdominal arteries is performed mainly at iliac arteries and with the purpose of vessel preparation for facilitating large vascular devices during the endovascular treatment of abdominal aortic aneurisms.6,7 In the current literature, the data concerning IVL for coral reef aortic lesions are limited to seven papers. The Shockwave IVL device uses an angioplasty balloon catheter to deliver acoustic waves through the arterial wall and exerts its effect only on the calcium component creating microfractures in calcium structure and as a result, making the vessel more compliant to subsequent molding. The basic principle of IVL is to use a 1:1 ratio of the balloon to the artery diameter in order to have the complete balloon’s surface apposition to the vessel wall. Considering that the largest IVL Shockwave M5 balloon catheter has an 8 mm diameter, which is small for the aorta, it has been reported the double-balloon technique with two IVL Shockwave M5 balloons, each one attached to a dedicated generator and inflated simultaneously in a kissing fashion, to have an effective delivery of IVL.8,9 Furthermore, as described by authors, the apposition of the balloon to the juxta renal aortic segment can be achieved using the hugging balloons technique with a shockwave balloon catheter along with a plain balloon catheter for simultaneous parallel inflation and obtaining an effective diameter of the juxta renal aorta.10,11 Only three papers reported the use of a single shockwave balloon to perform the vessel preparation and then the lumen was molded at the desirable diameter with a huge plain balloon or with a stent.12–14
In our case, a single shockwave balloon was utilized to treat aortic occlusion, as the calcific distribution was concentric and equally distributed within the lumen. As a result, the calcium structure was altered, making the vessel more compliant and thus possible to mold it by positioning a single large balloon-expandable covered stent. The use of a double kissing shockwave balloon could have a role in this case but would have increased considerably the cost of the procedure. Finally, the need for stenting after lithotripsy remains unclear. In the current literature, there are no reported cases of rupture or dissection, and in some cases, the desirable aortic lumen diameter was achieved without stenting. To date, we cannot predict a future vessel dilation or stenosis after the lithotripsy in abdominal vessels as the current literature is scarce on the long-term outcome and in absence of evidence the stenting should be performed.
Conclusion
Selective IVL of multilevel calcific aorto-iliac lesions with a single shockwave device followed by selective stenting can be a valuable and cost-effective strategy to preserve aortic branches. It seems to be safe and with good outcomes in the short term, but more data are needed to confirm its safety and effectiveness.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.