
Abstract
Objectives
The goal of this study was to document the natural history of celiac artery aneurysms (CAAs).
Background
Celiac artery aneurysms are rare. Existing literature is skewed towards outcomes after intervention of large, symptomatic aneurysms but the behavior of untreated CAAs is poorly understood.
Methods
This is a single institution, retrospective analysis of patients with CAA diagnosed by CT imaging (2015–2019) identified through an institutional radiology database. Radiologic, demographic, and follow-up data were analyzed. The primary endpoint was the mean growth rate of CAAs.
Results
Of the 76 patients included, 86.8% were men with a mean age at presentation of 69.8 years. The mean CAA diameter on index imaging was 15.4 +/− 3.8 mm (range, 7–30 mm). All were classified as true aneurysms and 76.3% were saccular. All patients had clinical follow-up with mean follow-up 31.2 months +/− 21.6 months. No patient developed symptoms or rupture. The mean radiological follow-up among 45 patients was 25.2 +/− 16.8 months. Over this period, 16 CAAs (35.6%) enlarged, while 29 (64.4%) remained stable. One patient (1.3%) underwent intervention for increasing size in the setting of a chronic dissection. On multivariate analysis, age <70 was significantly associated with increased risk of aneurysm growth.
Conclusions
In this institutional review of patients with CAAs, the majority of aneurysms remained stable in size, with no patients developing symptoms or rupture over clinical follow-up. Given the observed benign behavior of these aneurysms, guidelines that suggest conservative management of CAAs less than 2 cm seems appropriate.
Introduction
Celiac artery aneurysms (CAAs) are rare, accounting for only 3–4% of all visceral artery aneurysms, fourth in incidence behind splenic, hepatic, and superior mesenteric artery aneurysms, respectively.1–3 With the wider availability and utilization of computed tomography (CT) scans 4 ; however, CAAs are being more frequently detected in asymptomatic individuals. 2 Despite this, our understanding of the natural history of these aneurysms, in particular the risk of growth and rupture, remains poor.
Historically, rupture rates were thought to be as high as 72% as the majority of patients presented symptomatically and CAAs were thought to be infectious in etiology. 1 Although the modern rate of rupture is lower, between 6-13%, data on mortality after rupture is scarce and ranges widely depending on the source, particularly since a significant number of patients will not make it to the hospital.1,2 Given the concern of this dreaded complication, elective repair is advocated by the Society for Vascular Surgery in patients with asymptomatic aneurysms >2 cm, symptomatic aneurysms regardless of size and pseudoaneurysms, while surveillance is recommended for aneurysms <2 cm in asymptomatic patients. 5 Although these guidelines have provided an important framework for optimal management of CAAs, there is still limited data to support them. Considering the increasing incidence of CAAs in an aging population, a contemporary analysis of the behavior of CAAs is paramount. As such, the present study aims to document the natural history of CAAs managed at a single institution with a particular interest in recording the mean growth rate of CAA and identifying factors associated with aneurysm growth.
Methods
Patient cohort
This is a single institution, retrospective analysis of patients with CAA diagnosed by CT imaging between January 2015 and December 2019. The New York University Langone (NYU) Radiology Database was searched for terms including “celiac artery aneurysm” and “visceral artery aneurysm” to identify potential candidates. The studies captured in this search were individually assessed by a radiologist to confirm the presence of a celiac artery aneurysm (i.e., there was a visible and measurable difference in the caliber of the artery throughout its course). Aneurysms were measured in the axial dimension at the greatest diameter of the vessel on Visage 7 Imaging Platform (Visage Imaging, Inc., San Diego, California).
Patients aged 18 years or older with confirmed diagnosis of CAA on abdominal CT scan were included. Patients without clinical or radiological follow-up were included in the original study cohort but were excluded from follow-up analysis. Additionally, patients with a diagnosis of median arcuate ligament syndrome were excluded. As a retrospective chart review, the study was exempt from review by the NYU Institutional Review Board and the use of deidentified data allowed for waiving of individual patient consent.
Imaging data collection and follow-up
Data collected from the CT scans included maximum diameter at diagnosis (outer wall to outer wall) and aneurysm characteristics (including true vs pseudoaneurysm; fusiform vs saccular morphology; presence of thrombosis, dissection, or rupture) as identified through retrospective chart review. Associated imaging findings including abdominal aortic aneurysm, atherosclerosis of the abdominal aorta, additional visceral aneurysms, or anomalies were also recorded. Referral to vascular surgery was additionally captured.
Follow-up was classified as either clinical or radiologic. Clinical follow-up was calculated as the time between initial scan and the patient’s most recent inpatient or outpatient visit to any NYU associated physician. Radiological follow-up was recorded as the time between the patient’s original scan to the most recent abdominal CT scan, irrespective of indication for imaging. Indications for imaging and intervention were deduced through chart review of associated clinical encounters. Basic demographic information, including medical comorbidities, was collected for patients who met imaging inclusion criteria.
Objectives
The primary aim of this study was to report the mean growth rate of CAA with a secondary objective to identify factors associated with aneurysm growth.
Statistical analysis
Continuous data are reported as mean value +/− standard deviation, and categorical variables are presented as absolute numbers with population percentages. Mean growth rate was calculated by dividing growth (mm) by time (years) between initial and follow-up scans for each patient. Univariate comparison of categorical data was performed to identify variables associated with aneurysm growth. Variables with a p value <.1 on univariate analysis were included in multivariate logistic regression to evaluate the independent effects of patient comorbidities and aneurysm characteristics on growth. Results are reported as odds ratios with corresponding 95% confidence intervals.
Results
Patient demographics
Demographics of patients with celiac artery aneurysm (CAA).

Imaging and CAA characteristics
The most common indication for imaging was follow-up of a pathology unrelated to CAA (48.7%). Other indications included abdominal pain (22.4%), follow-up of a known CAA (21.1%), and other/unknown (6.8%). Of note, no patients underwent imaging for hemodynamic instability, defined as hypotension or tachycardia, for presumed rupture.
Celiac artery aneurysm characteristics and associated imaging findings.
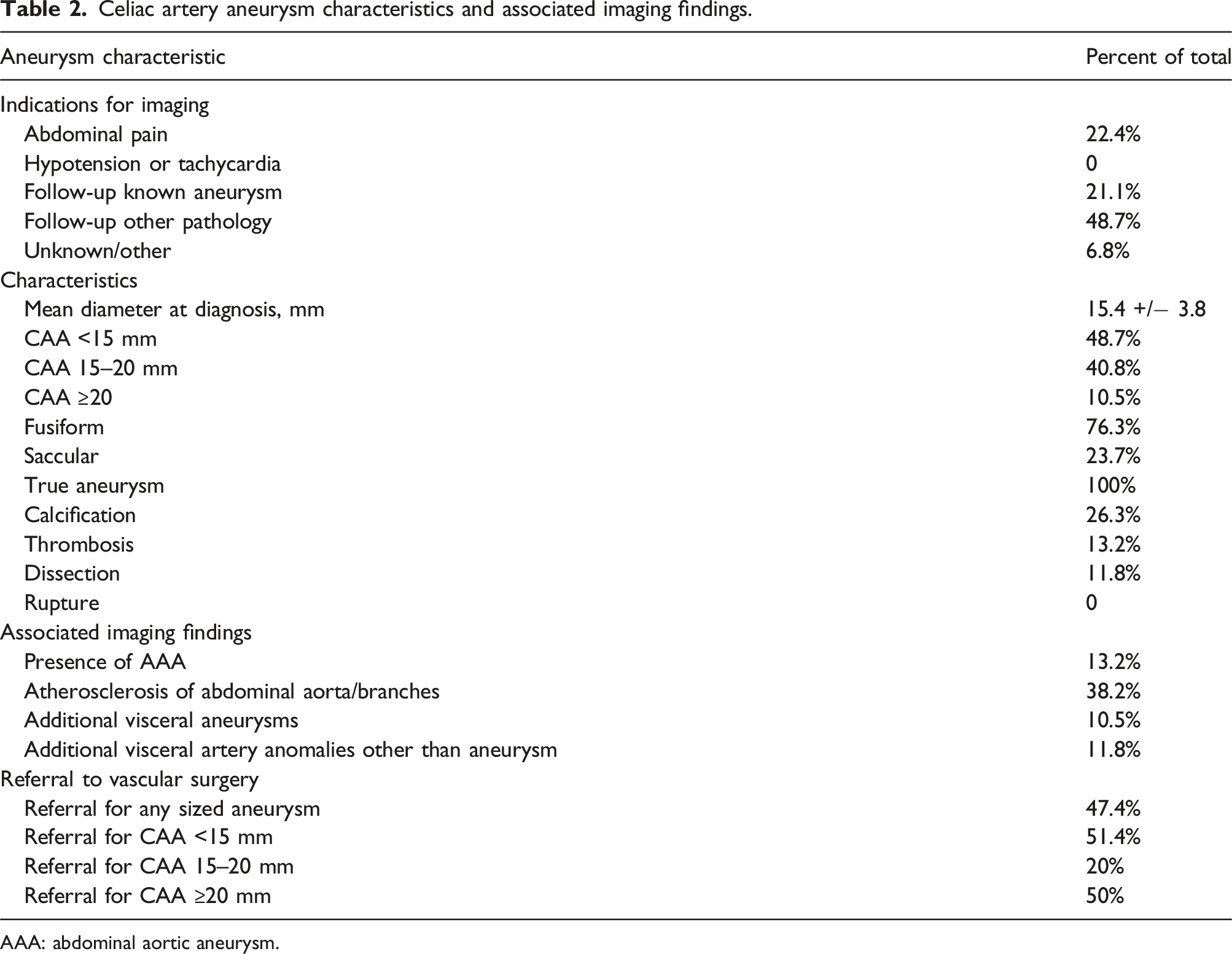
AAA: abdominal aortic aneurysm.
Clinical and radiological follow-up
All 76 of the patients originally identified had documented clinical follow-up with mean time to follow-up of 31.2 +/− 21.6 months. At follow-up, no patients were symptomatic (defined as abdominal pain, back pain, nausea, vomiting, anorexia, or any symptom concerning for mesenteric ischemia). During this time frame, there were no documented ruptures. One patient underwent intervention for interval enlargement of the aneurysm in the setting of a chronic dissection. The patient had a history of a rupture of an inferior pancreaticoduodenal artery aneurysm which was coiled. At that time, he was noted to have aneurysmal degeneration of the celiac artery with focal dissection. The aneurysm was followed with serial CT scans until it reached 20 mm. The patient was taken for endovascular repair with placement of a covered stent in the celiac artery. No perioperative morbidity or mortality was recorded, and the patient has not required further intervention.
A total of 45 patients (59.2%) had documented radiological follow-up with mean time to follow-up of 25.2 +/− 16.8 months. Over this time, 16 (35.6%) patients had documented interval enlargement of the aneurysm with a mean growth rate of 1.09 +/− 0.79 mm/year. The remaining 29 patients (64.4%) had a stable aneurysm. Follow-up data are depicted in Figure 1. Flow chart depicting clinical and radiological follow-up for patients with celiac artery aneurysms. CT: computed tomography.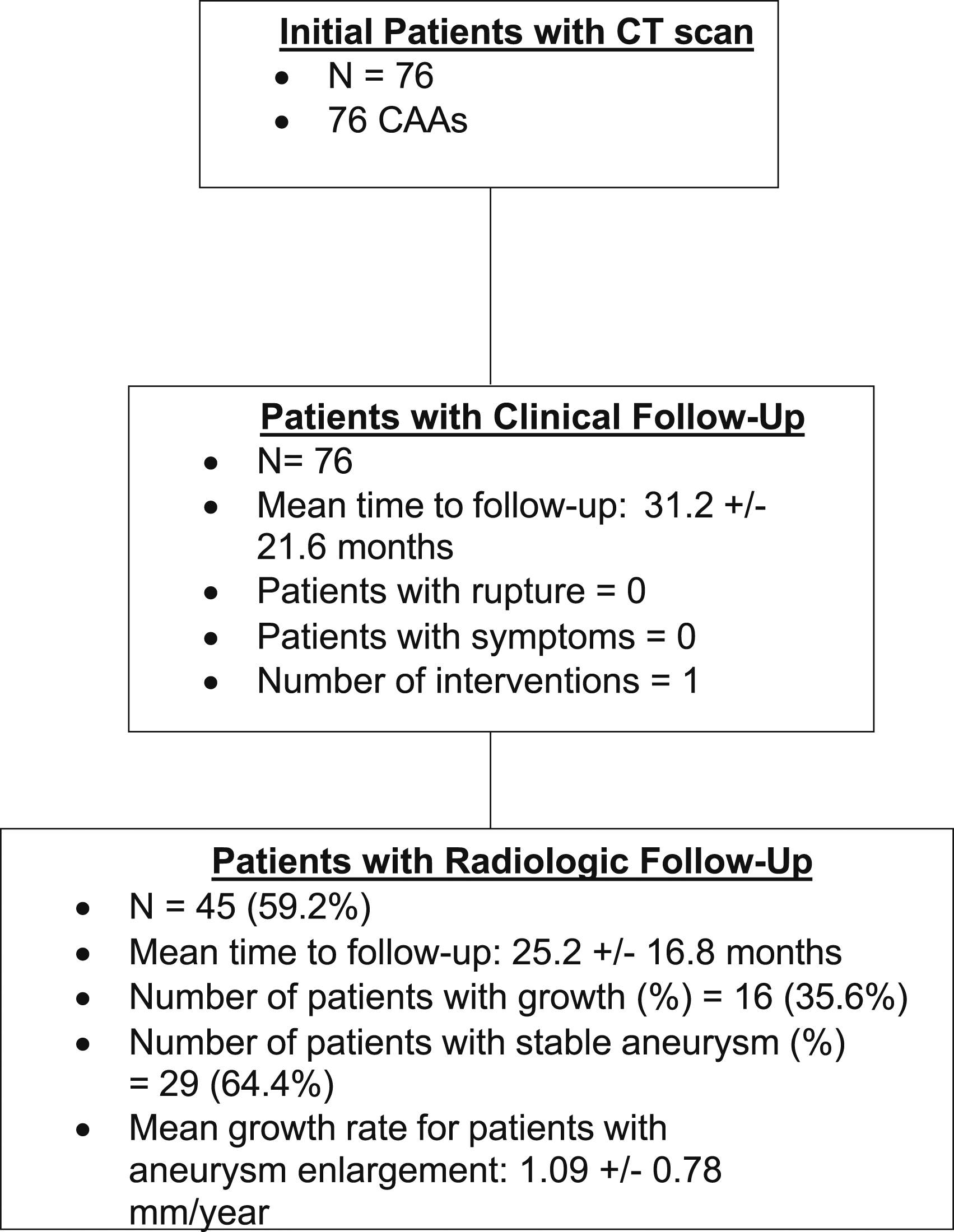
Univariate comparison and multivariate regression
Univariate analysis of patient and aneurysm characteristics on CAA growth.
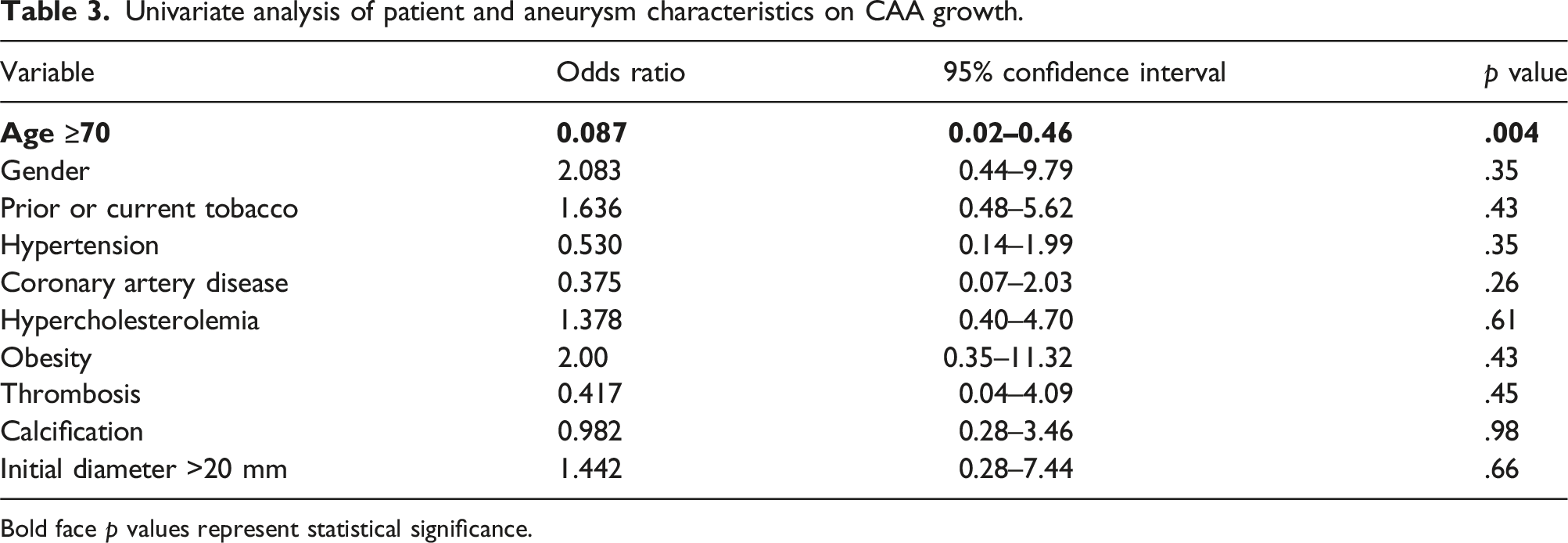
Bold face p values represent statistical significance.
Multivariate regression analysis of patient and aneurysm characteristics on CAA growth.
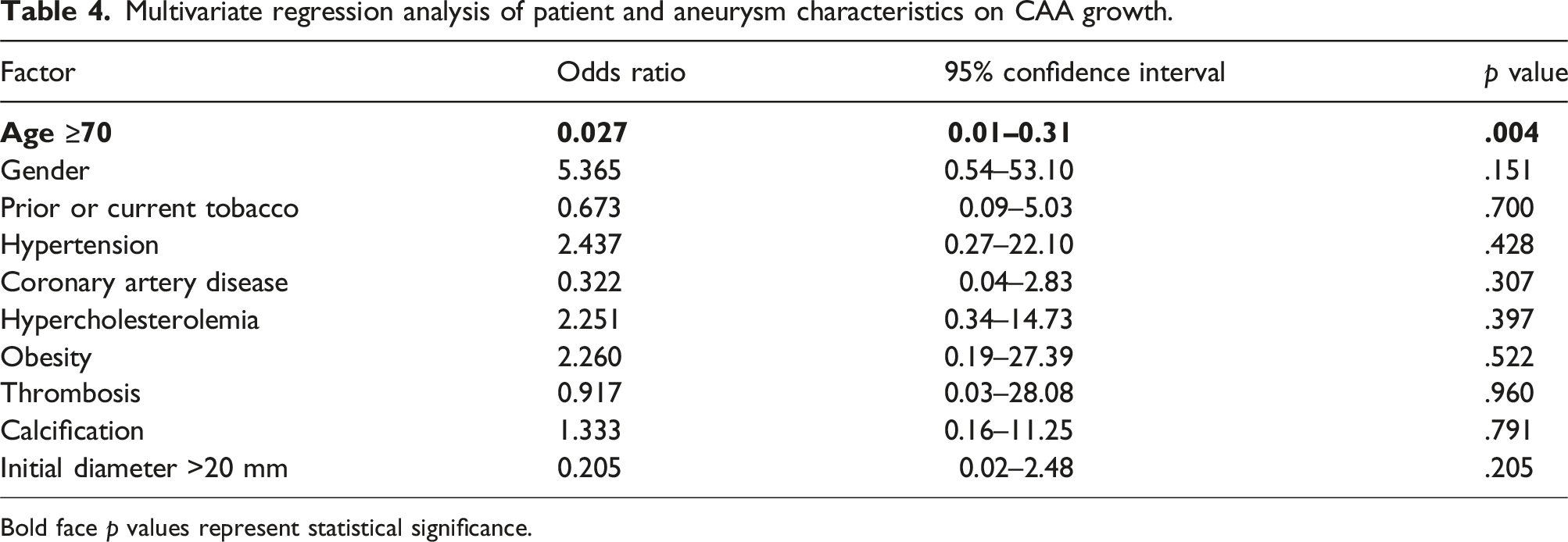
Bold face p values represent statistical significance.
Discussion
The Society for Vascular Surgery Guidelines for the management of visceral artery aneurysms published in 2020 recommends treatment of asymptomatic non-ruptured true celiac artery aneurysms measuring >2 cm. Despite being a grade 1 (strong) recommendation, the supporting evidence is deemed low quality. 5 As such, we performed a single institution, retrospective analysis of patients with untreated CAAs to further define the natural history of these entities. Our study found aneurysmal enlargement in slightly over one-third of patients with radiological follow-up with a mean growth rate of only 1.09 mm/year within this cohort. Moreover, there were no documented cases of rupture or symptomatic disease at mean clinical follow-up of 31.2 months. Our findings are consistent with prior reports suggesting that CAAs are insidious, slow-growing lesions with low risk of rupture and provide further evidence to support the current guidelines.
Given the rarity of CAAs, it is no surprise that the current literature consists mainly of case reports and small retrospective series. The largest of these contemporary studies focused solely on CAAs analyzed a total of 18 patients, of which there was a single initial presentation of a ruptured aneurysm (6%). Within this initial cohort, 8 patients were managed non-operatively. Mean aneurysm size within this group was 2.1 cm and no aneurysm was observed to significantly enlarge over follow-up. There was a single late rupture (6%) in a patient with a 2.5 cm aneurysm who had previously declined repair. 2 It is difficult to draw comparisons between our study and this previously published report for many reasons, the most obvious being the small overall number of patients who were surveilled in the original report. It is unclear how many of these asymptomatic patients are referred to or followed by a vascular specialist, but of the 8 patients in this study with CAA >2.0 cm, half were not seen by a vascular surgeon and the remainder were managed expectantly for a variety of reasons, including high risk medical comorbidities.
Retrospective single center studies analyzing the behavior of splanchnic artery aneurysms (SAA; i.e., arising from the celiac, superior mesenteric or inferior mesenteric arteries) provide complementary yet limited data on CAAs. A study published by Batagini et al. 6 evaluating 74 patients with 87 SAAs with at least two subsequent CT scans reported a median growth of 0.63 mm/year for all aneurysms. More specifically, 20 patients were noted to have a CAA with mean diameter at presentation of 15 mm and a reported growth rate of −0.1 mm/year (+/− 1.4 mm). Within a follow-up period of 57.3 months, there were no reported ruptures. Other studies have additionally confirmed the indolent nature of SAAs and CAAs amongst patients demonstrating aneurysmal enlargement. In 2017, Erben et al. 7 reported a mean growth rate of 0.64 mm/year amongst 122 patients with 138 SAAs. Of the 63 CAAs identified, mean initial size was found to be 14.6 mm. Growth rate stratified by aneurysm location was not provided, but of note, there were no ruptures within the CAA cohort.
The study population included in this report tended to be older men which is consistent with the existing literature,2,8 but stands in contrast to patients with splenic and renal artery aneurysms, who are often be female.8,9 The relationship between gender and CAAs has yet to be fully elucidated but the male predominance appears to date back to historic reports published prior to the 1950s. 1 Interestingly, up to 18% of CAAs are associated with abdominal aortic aneurysms, 1 a disease primarily affecting men. 10
The data is even more sparse in identifying risk factors for CAA aneurysm growth and rupture. In their presentation of 18 patients, Stone et al. 2 were unable to identify any comorbid conditions or aneurysm characteristics associated with risk of rupture, which they attributed to being underpowered for such analysis. In their study of SAAs, Erben et al. 7 found that female sex was associated with faster annual aneurysm growth rate, while smoking was associated with a slower growth rate. However, a similar analysis of SAAs by Batagini et al. 6 identified only portal hypertension as a risk factor for faster SAA enlargement. Regardless, it is unclear how applicable these findings are to patients with CAAs given the diversity of SAAs.
Our study found on both univariate and multivariate analysis that age >70 was protective against aneurysm growth. The mean age of patients who were found to have aneurysmal growth at follow-up was 62.3 years, while the mean age of patients who demonstrated aneurysm stability was 74.3 years. This finding has important implications for future surveillance protocols. Currently, the SVS guidelines suggest annual surveillance scans of patients with CAAs who are being observed, which they list as grade 2 (weak) evidence. 5 Given our findings, future studies should be undertaken to determine whether the screening interval can be increased in patients over 70 years old in an effort to spare them from unnecessary radiation and preserve hospital resources. Identifying which patients warrant annual screening is particularly important as the use of CT scans continues to increase annually, 11 leading to more patients being diagnosed incidentally.
As incidental diagnoses become increasingly common, guidelines will need to be updated to better reflect these trends. Currently, none of the major society guidelines,5,12 put forth specific recommendations on when patients with asymptomatic splanchnic artery aneurysms, including CAA, should be referred to a vascular specialist. Given this lack of clarity, it is not surprising that within our own health system only 47.4% of patients with CAA were referred to a vascular surgeon. At our own institution, guidelines are being addressed to encourage referral at time of diagnosis.
There is a wide variety of treatment options available today for patients with larger aneurysms indicated for repair. Previously, celiac artery aneurysms were managed with open ligation, excision, or bypass—procedures associated with higher morbidity and mortality particularly in the face of rupture. However, management options have expanded with the development of coil embolization and endovascular stenting. A comparison of open and endovascular management of celiac and superior mesenteric artery aneurysms performed by Sachdev et al. 13 found that the technical success rate for endovascular treatment approached 90% and was safe even amongst hemodynamically unstable patients presenting with rupture.
There are several limitations to this study. Although it is larger than previously published reports on the subject, the overall numbers are still small and data collection was performed retrospectively. Additionally, clinical follow-up time was relatively short at 31.2 months and only 45 patients (59.2%) had radiological follow-up. To better quantify the risk of growth and rupture, longer and more consistent follow-up will be needed. Symptoms at follow-up were identified through chart review of encounters often unrelated to the pathology at question, which created the potential for incomplete assessment. For example, it was not always possible to identify the exact etiology of the patient’s abdominal pain after aneurysm related issues were excluded. It is additionally worth mentioning the limitations of CT scanning, which although currently is the gold standard for diagnosis, cannot fully characterize CAAs or reliably distinguish between true and false aneurysms. Furthermore, while we did not collect information on whether all patients were seen by a vascular surgeon, our intervention rate is potentially explained by the fact that many of our subjects were not assessed by a vascular specialist or other provider, such as an interventional radiologist, who manages this disease. Lastly, but perhaps most importantly, there were no documented ruptures so analysis of risk factors for this event could not be performed. Despite these limitations, we believe this is the most comprehensive contemporary review of the natural history of celiac artery aneurysms to date.
Conclusions
This single institution study of patients undergoing observation of CAAs found that the majority of CAAs remained stable in size over a mean follow-up 31.2 months with only one patient undergoing intervention and no documented ruptures. Given the benign nature and indolent growth of these lesions, particularly of those <2 cm, our findings support the current SVS recommendations.
Footnotes
Authors’ note
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.