
Abstract
Introduction
Intermittent claudication includes a wide spectrum of peripheral artery disease ranging from asymptomatic with reduced perfusion to lifestyle-limiting atherosclerotic disease. The purpose of this study was to evaluate the management of claudicants with a low toe-brachial index (TBI).
Methods
This study was a retrospective review of consecutive patients that presented in 2015 with claudication and a low TBI (<0.6) monitored over 5 years. The patient demographics, co-morbidities, and vascular-related characteristics (ankle-brachial index, TBI, calcified vessels, and wounds) were collected. The patients were separated into two cohorts: diabetics and non-diabetics. The outcomes included progression to chronic limb threatening ischemia (CLTI), interventions (endovascular or open), minor amputations, major amputations, and mortality.
Results
A total of 184 patients with 356 limbs were identified as claudicants with a low TBI, and there were 103 diabetics with 81 non-diabetics. The ABI and TBI were similar between the diabetics and non-diabetics, but the diabetics had a significantly higher number of calcified vessels (p < .001) and progression to CLTI (p < .001). The time to revascularization and number of patients that had a revascularization procedure were similar between the two groups, and nearly half of the revascularization procedures were performed within the first 6 months. The major amputation rate trended higher in the diabetic population, and there was a statistically significantly higher rate of minor amputations in the diabetics over the 5 years (Log-rank, p < .001). There was no difference in 5-year survival between diabetics and non-diabetics, and the overall 5-year mortality was 34%.
Conclusion
Patients presenting with claudication and low TBI, especially with diabetes, are at a higher risk to develop chronic limb threatening ischemia. Claudicants with a low TBI should have closer follow-up and more aggressive risk factor modification to reduce long-term mortality.
Introduction
Peripheral artery disease (PAD) affects 8–9 million people in the United States, and the prevalence of PAD in the elderly population is 10%–15%.1–3 Symptomatic PAD is characterized by intermittent claudication, or asymptomatic PAD can be defined by an ankle-brachial index (ABI) of less than 0.9.4,5 Peripheral artery disease is objectively diagnosed by ankle-brachial index.4,6 However, ABI may be limited by severe arterial calcification that results in incompressibility associated with diabetes mellitus and chronic kidney disease. 7 In addition to ABI, toe-brachial index (TBI) and toe pressures are obtained during a routine ABI because digital arteries are more resistant to arterial calcification.5,7 Individuals with symptomatic or asymptomatic PAD have a threefold risk of death and an increased risk of other cardiovascular events, including progression to amputation.8,9
The natural history of intermittent claudication is a slowly progressive atherosclerotic disease with an emphasis on risk factor modification and medical management. The risk of major amputation in claudication is relatively low (<5% over 5 years), so the importance of risk factor modification is to reduce the risk of a fatal cardiac or cerebrovascular event.5,6 Persistent smoking and uncontrolled diabetes mellitus are the risk factors most associated with progressive peripheral artery disease to chronic limb threatening ischemia (CLTI).6,10 However, many patients with claudication are not compliant with medical therapy and develop lifestyle-limiting claudication. Fortunately, the current management of life-style limiting claudication is an endovascular-first approach that provides symptomatic relief. 11
There is evidence to suggest a higher-risk population within the claudication cohort is those patients with a decreased toe-brachial index (<0.6) or low toe pressures (<40 mm Hg). 12
Not only is this population more likely to have progression to critical limb threatening ischemia, but the claudication with a low TBI cohort also has an increased mortality rate.12,13 The best management strategy in the diabetic claudicants with low TBI has not been defined. Some studies have suggested close surveillance with shorter follow-up intervals and even a lower threshold for a diagnostic angiogram in less compliant patients. 12 However, there is a lack of data on minor and major amputation rates in the claudicants with a low TBI. Therefore, the objective of this study is to evaluate the management of claudicants with low TBI, including diabetic and non-diabetic cohorts.
Methods
Study patients
This was a single-institution, retrospective study at Audie L. Murphy Memorial Veterans Hospital (ALMMVH) in San Antonio, Texas. The study was approved by the Institutional Review Board at the ALMMVH in collaboration with University of Texas Health Science Center at San Antonio. The vascular lab software (VasculoPro, Richmond, British Columbia, Canada) was used to search consecutive patients with the following criteria: 0.4 > ABI < 0.9 or ABI > 1.3 (non-compressive) with biphasic or monophasic dorsalis pedis and posterior tibial signals and a low TBI <0.6. Patient charts from 2015 were reviewed to allow for 5 years of follow-up. The patient chart was reviewed to confirm a diagnosis of claudication, and patients were excluded with the following conditions: a known history of claudication and low TBI, prior documented peripheral neuropathy, previous amputation (minor or major), prior revascularization, open wounds (at the start of enrollment), rest pain, or lost to follow-up over the 5 years. A total of 184 patients were included in the study with 356 limbs, as many patients (not all) had two limbs that fit the study criteria. The demographic data, medications, procedure (surgical or endovascular), amputations (major and minor), and survival were collected over the 5 years.
Vascular laboratory
All non-invasive studies were performed by vascular technicians in the vascular surgery clinic. A Unitex (North Kingston, RI) photoplethysmography device was used for all measurements. Non-invasive studies were obtained with the patients in a supine position. Brachial and ankle digital cuffs were inflated until the plethysmography signal was zero or up to 250 mm Hg. Brachial, ankle, and toe pressures were determined as the pulsatile plethysmography signal returned as the cuff was deflated. The toe pressure was measures from the great toe. The interval for the vascular lab studies was up to the discretion of the vascular surgeon. The non-invasive studies with the ABI and TBI were recorded over the study period per limb for each patient.
Statistical analysis
The patient characteristics, vascular-related characteristics, and outcomes were reported as mean ± standard deviation for continuous variables (except time to revascularization was reported as mode with interquartile range) or as number and percentage for categorical data. A chi-squared statistical analysis was performed to determine significance for patient characteristics, vascular-related characteristics, and outcomes; except time to revascularization, a Mann–Whitney (non-parametric analysis) statistical analysis was performed. A univariable logistic regression analysis was used to obtain the odds ratio and 95% confidence interval for progression to CLTI and mortality. Kaplan–Meier curve with log-rank (Mantel–Cox) analysis was used to compare diabetics to non-diabetics for freedom from major amputation, freedom from minor amputation, and survival over 5 years. A Kaplan–Meier curve with log-rank (Mantel–Cox) analysis was also used to compare patient survival with and without intervention (either endovascular or open revascularization) over 5 years. The statistical analysis was completed using GraphPad Prism Software, version 9.0.0; a p-value of <0.05 was considered significant.
Results
Patient characteristics.

BMI, body mass index; HTN, hypertension; CAD, coronary artery disease; COPD, chronic obstructive pulmonary disease; CVA, cerebrovascular accident. Continuous data are presented as mean ± standard deviation, and categorical data are presented as number (%).
Vascular-related characteristics at the time of presentation by limb.
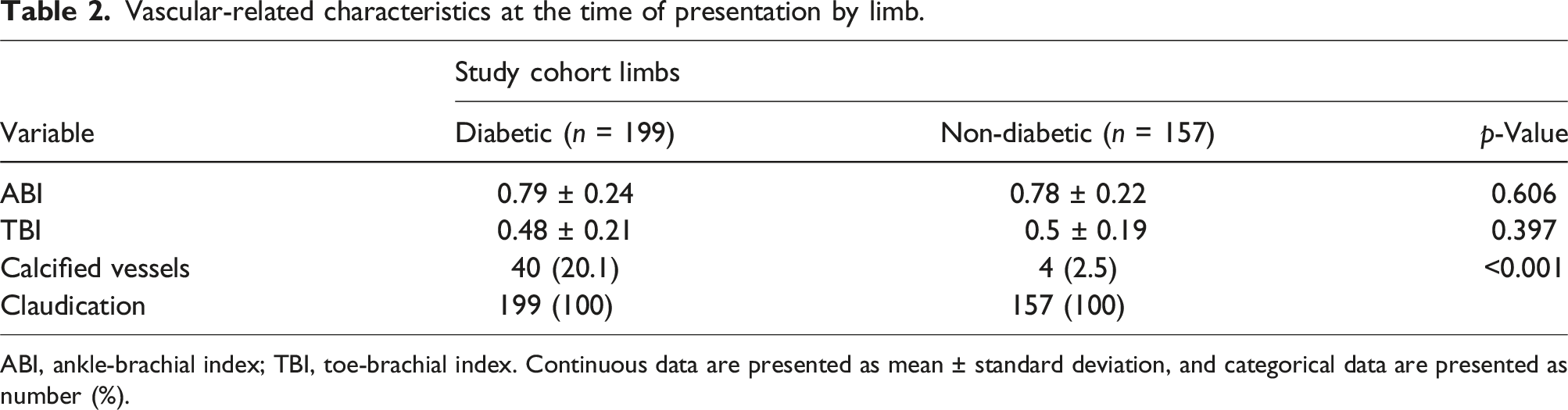
ABI, ankle-brachial index; TBI, toe-brachial index. Continuous data are presented as mean ± standard deviation, and categorical data are presented as number (%).
Outcomes over 5 year by limbs.

CLTI, chronic limb threatening ischemia. Continuous data are presented as mode and interquartile range (IQR), and categorical data are presented as number (%).
Univariable analysis of progression to CLTI by patient characteristics.

CLTI, chronic limb threatening ischemia; DM, diabetes mellitus; CAD, coronary artery disease; CVA, cerebrovascular accident; BMI, body mass index.
The Kaplan–Meier curves for freedom from major or minor amputation and survival comparing diabetics and non-diabetics are shown in Figure 1. Although there was no difference in freedom from major amputation between diabetics and non-diabetics (Figure 1(A)), there was a significant difference (Log-rank, p < .001) in freedom from minor amputation in patients without diabetes in comparison to patients with diabetes (Figure 1(B)). There was no difference in overall survival over the 5-year period in diabetic and non-diabetic patients (Figure 1(C)), but the survival rate was relatively low for both claudication groups (non-diabetics 72%; diabetics: 61%). In order to confirm that lack of association of diabetes to mortality, a univariate analysis was performed on the patient characteristics. Indeed, the odds ratio (1.6) and confidence interval (0.86–3.02) did not demonstrate a statistically significant association between mortality and diabetes. The two patient characteristics that were significantly associated with mortality were elevated creatinine (OR 2.6, CI 1.23–5.66) and stroke (OR 2.23, CI 1.03–4.87). A Kaplan–Meier survival curve is shown in Figure 1(D) for those patients that underwent an intervention for revascularization compared to those without an intervention. There was no difference in overall survival between the two groups; however, the Kaplan–Meier curve had a lower survival trend for the patients with no intervention. Kaplan–Meier Curves: (A) Freedom from major amputation, per limb; (B) freedom from minor amputation, per limb; (C) survival, per patient; (A–C): DM (diabetes mellitus), nDM (non-diabetes mellitus); (D) survival, per patient; Int (Intervention), no Int (no Intervention); Log-rank (Mantel–Cox) for statistical significance.
Discussion
Claudication is a mild to moderate spectrum of peripheral artery disease with a relatively low risk of major amputation or cardiovascular-related mortality.5,6 However, claudicants with a low TBI or toe pressures have been associated with higher cardiovascular morbidity and mortality. 13 This is a single institution study that evaluated the outcomes of claudicants with a low TBI over 5 years separated into diabetic and non-diabetic cohorts. The 5-year mortality in this patient population was higher than a standard population of patients with claudication regardless of their diabetic status, which is consistent with previous studies.6,13 However, we did find a higher incidence of progression to chronic limb threatening ischemia in the diabetic patients as well as increased number of minor toe amputations. These findings may have implications for management of claudicants with low TBI, especially diabetics.
TBI can be used as an adjunct to ABI to risk stratify the severity of the peripheral arterial disease for risk of progression to chronic limb threatening ischemia (CLTI) and amputation. 12 In most vascular labs, TBI and toe pressures are a standard part of non-invasive studies along with ankle-brachial index. The ABI may be falsely elevated (>1.3) in diabetics because of medial artery calcification. 7 In patients with PAD and diabetic foot ulcers, meta-analyses have reported a correlation with toe systolic blood pressures of greater than 30 mm Hg and wound healing.14,15 In the absence of ulcers or wounds, the role of TBI or toe pressures to identify a high-risk population of claudicants for limb loss remains less clear. In the only study that has directly evaluated claudicants with a low toe pressure (<40 mm Hg), Bowers et al demonstrated a low toe pressure is a risk factor for clinical deterioration. 12 Over the mean follow-up time of 31 months, there was an annual major amputation rate of 4% per year. In our study, the overall major amputation rate of the claudicants with low TBI was much closer to a typical claudication population at approximately 1% per year. 6 The major amputation rate trended higher in the diabetic population (1.63% per year) than in the non-diabetic population (0.74% per year), but there was no statistically significant difference over the 5 years (Figure 1(a)). The progression to CLTI and minor (toe) amputations was significantly higher in the diabetic population than in the non-diabetic population (Table 2 and Figure 1(b)). Similar to other studies of claudication with progression to CLTI, the univariate analysis in our study indicated diabetes (OR 4.75) and smoking (OR 4.74) were the risk factors most associated with CLTI.5,6 The healing potential of foot wounds is multi-factorial; hence, our institution manages CLTI patients with an interdisciplinary team that includes a vascular surgeon, podiatrist, primary care physician, and infectious disease specialist. The differences in major amputation rates between our study and Bowers et al may be due to the interdisciplinary team, inclusion of endovascular interventions, compliance with medical therapy, and better perfusion at the ankle level (0.78 vs 0.42). 12 Although diabetic claudicants with low TBI develop CLTI at a higher incidence than non-diabetics, often with revascularization this results in a minor amputation with prevention of major limb loss.
Peripheral artery disease is associated with increased cardiovascular events and mortality. Claudicants with a low TBI have been associated with a higher mortality rate than a standard intermittent claudication population.13,16 The incidence of cardiovascular events (myocardial infarct, stroke, or cardiovascular death) in patients with peripheral artery disease is approximately 25% over 5 years, and the mortality rate alone is 10%–15% over the same time period.6,17 In a study by Hyuan et al, they reported that the association of TBI with cardiovascular death was linear regardless of the diabetes status with the highest risk of death as the TBI category decreased. 13 Of note, the risk of cardiovascular death as determined by TBI was independent of ABI. 13 In this study, claudicants with a low TBI overall mortality was 34%, which is nearly three times higher than a standard claudication population. 6 Therefore, the adjunct of low TBI in claudicants can identify a high-risk population for increased all-cause mortality and morbidity.
There is not a defined management strategy for high-risk claudication populations, including claudicants with low TBI. The SVS has clinical practice guidelines for management of asymptomatic disease and claudication that recommends medical management with antiplatelets, smoking cessation, diabetes mellitus, dyslipidemia, hypertension, and exercise therapy. 18 The role of revascularization for intermittent claudication is recommended for patients with significant functional or lifestyle-limiting disability. An individualized patient-centered treatment plan is based on the functional impairment to improve quality of life rather than treatment of physiologic parameters such as ABI. 18 In claudicants with low TBI, this population often presents with more advanced peripheral artery disease and multiple co-morbidities with functional limitations related to chronic obstructive pulmonary disease, congestive heart failure, obesity, or osteoarthritis of the hips or knees. Clinical practice guidelines do not provide specific recommendations regarding non-invasive surveillance for claudication, although typical follow-up intervals are 6 to 12 months with an office visit and non-invasive studies. In our study, 65%–70% of the patients (both DM and non-DM) were stable over 5 years without intervention. The median time to revascularization was 6.3 months for non-diabetics and 7.23 months for diabetics, but nearly half of the revascularization interventions were done in the first 6 months of the study period. Based on this data, a potential treatment strategy for patients with new-onset claudication with low TBI would be close observation consisting of a vascular surgery office visit and a non-invasive study every 3–4 months at least for a year after the initial presentation. Additional care pathways include primary care physicians for compliance of medical therapy, podiatry for foot care (especially diabetics), referral to smoking cessation specialist, and a low threshold for referral to a cardiologist.
There are several limitations in this single-center retrospective study. Potential inherent biases include the relatively small sample size, all-male veteran population, and the possible institutional-specific confounders. In order to identify the claudication population, the vascular lab search criteria were reported as the baseline value by ABI (0.4 > ABI < 0.9 or ABI > 1.3) and a biphasic or monophasic DP or PT waveform rather than ABI alone. The patients in this study are considered new onset of claudication with low TBI, but prior to 2015 the reporting of non-invasive physiologic patient data was not standardized in the chart. The charts were searched for the inclusion and exclusion criteria; however, it is possible that not all the patients had new-onset claudication with low TBI. The ABI and TBI values were recorded throughout the study, but there was not a consistent interval to obtain follow-up ABI and TBI. The mortality rate was not reported as cardiovascular-related death because not all the causes of death were identified in the electronic medical record.
Conclusion
In the peripheral artery disease population, a low TBI can help to identify a higher-risk cohort of patients with claudication. This study is consistent with other studies demonstrating that claudicants with low TBI have a higher than expected 5-year mortality rate for both diabetics and non-diabetics.13,16 Although the low TBI does not increase the risk for major amputation, we did observe diabetics with a low TBI progressed to chronic limb threatening ischemia and minor toe amputations compared to non-diabetics with a low TBI. Claudicants with a low TBI, especially diabetics, should be considered for closer vascular surgery follow-up, aggressive management of cardiovascular risk factor modifications, and routine foot care by a podiatrist. Given the limitations of this study, additional future investigations with larger data sets are needed to validate the increased risk of claudicants with low TBI.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.