
Abstract
Introduction
Patients with peripheral arterial disease (PAD) frequently require reinterventions after lower-extremity revascularization (LER) to maintain perfusion. Current Society for Vascular Surgery guidelines define reinterventions as major or minor based on the magnitude of the procedure. While prior studies have compared primary LER procedures of different magnitudes, similar studies for reinterventions have not been performed. The objective of this study is to compare perioperative outcomes associated with major and minor reinterventions.
Methods
Patients undergoing LER for PAD at a tertiary care center from 2013 to 2017 were included. A retrospective review of electronic medical records was performed, and reinterventions were categorized as major or minor based on the procedure magnitude. Minor reinterventions included endovascular procedures and open revision with patch angioplasty, while major reinterventions were characterized by open surgical or endovascular LER with catheter-directed thrombolysis (CDT). Perioperative outcomes following LER were captured and compared for major and minor reinterventions. An additional subgroup analysis was performed comparing outcomes associated with major reinterventions stratified into open major surgical reinterventions and CDT.
Results
This study included 713 patients over a mean follow-up of 2.5 years. A total of 291 patients underwent 696 ipsilateral reinterventions (range = 1–12 reinterventions). Most reinterventions were minor (72.1%, N = 502) and 27.9% (N = 194) were major. Patients receiving reinterventions had an average age of 67.2 ± 11.5 and most were white (73.5%) males (60.1%) initially treated for claudication (58.2%) and CLTI (41.8%). There was significantly higher post-operative bleeding (9.8% vs 3.4%, p = .001), arterial thrombosis (3.1% vs 1.0%, p = .047), and acute renal failure (6.2% vs 2.4%, p = .014) after major reinterventions than minor. Additionally, major reinterventions had significantly higher return to the OR (17.0% vs 11.3%, p = .046) and longer hospital stays (7.5 vs 4.3 days, p = <.0001). Overall, major reinterventions were associated with significantly increased perioperative morbidity (37.6% vs 19.7%, p ≤ .001) with no difference in perioperative mortality. In the subgroup analysis, open reinterventions resulted in significantly longer hospital stays (8.6 days vs 5.5 days, p ≤ .001) and more wound infections than CDT (11.0% vs 0%, p = .017). However, there was no other significant difference in morbidity or mortality following treatment with open surgical reinterventions or CDT.
Conclusions
In this study, major reinterventions after LER were associated with greater perioperative morbidity than minor reinterventions, with no difference in mortality. Major reinterventions performed via open surgery and CDT had similar morbidity and mortality.
Keywords
Introduction
Peripheral arterial disease (PAD) is characterized by a spectrum of clinical presentations that range from asymptomatic patients with abnormal ankle brachial indices to patients with intermittent claudication or chronic limb-threatening ischemia (CLTI). 1 While exercise programs, pharmacologic management, and risk factor modification are primary treatments for those with limited symptoms, open or endovascular lower-extremity revascularization (LER) is the standard of care for patients with more severe disease.1,2 Despite the initial effectiveness of LER, sustaining long-term patency remains a significant clinical challenge.3,4 As such, it is common for patients with PAD to require multiple LER procedures, or reinterventions, to preserve blood flow to the limb, provide sustained symptomatic relief, and prevent major amputation.4,5
The reintervention rate after LER has been reported between 24% and 58% after at least a 2-year follow-up period.4,6,7 More recently, the BEST-CLI randomized trial demonstrated an ipsilateral reintervention rate of 19.5% after open surgery and 28.4% after endovascular therapy. 8 Thus, it is important to assess outcomes associated with different types of repeat LER. The Society of Vascular Surgery (SVS) defines major reinterventions as an open surgical bypass, surgery with thrombectomy or thrombolysis, or the use of jump or interposition grafts for revision. In contrast, SVS characterizes minor reinterventions as endovascular balloon angioplasty, stenting, or open revision with patch angioplasty. 9 While previous studies have demonstrated variable morbidity and mortality when comparing open to endovascular techniques for initial LER, an analysis of perioperative outcomes following reinterventions of different magnitudes has not yet been explored.8,10,11 The aim of this study is to compare perioperative outcomes following major and minor reinterventions in patients with PAD and to assess the differences in the perioperative risk of catheter-directed thrombolysis (CDT) and open surgical reinterventions.
Methods
Study population
Through a retrospective review of electronic medical records (EMRs) at a tertiary care center, patients undergoing LER for PAD from 2013 to 2017 were identified. Only patients who were treated for PAD were included in this study. LER was performed by providers across different vascular specialties (vascular surgery, interventional radiology, and interventional cardiology). Patients who underwent a diagnostic angiogram without LER, or who were treated for other lower-extremity vascular conditions (e.g., aneurysms and trauma) were excluded. Patients with initial presentation of acute limb ischemia (ALI) were also excluded. Any LER procedure occurring after the initial intervention was defined as a reintervention, and each reintervention was documented separately in the database including its indication and perioperative 30-day outcomes. Reintervention magnitude was divided into major and minor as determined by SVS classification. 9 Major reinterventions included open surgeries and procedures involving CDT while minor reinterventions were endovascular and open revision with patch angioplasty. A separate subgroup analysis within the major reintervention group was also performed. Patients undergoing CDT for thrombus formation in an occluded vessel were compared to patients receiving open surgical reinterventions. The present study was approved by the Yale University Institutional Review Board, and the requirement for patient consent was waived.
Patient characteristics
Study data were collected and managed using REDCap (Research Electronic Data Capture) data capture tools hosted at Yale University.12,13 Patient demographics, comorbidities, and medications used prior to the initial intervention were documented. Recorded demographic factors included age, race, gender, and body mass index. Comorbidities included a history of hypertension, hyperlipidemia, diabetes mellitus, coronary artery disease (CAD), congestive heart failure, and stroke. Chronic renal insufficiency (defined by baseline serum Cr > 1.5 mg/dL), end-stage renal disease, cancer, smoking history (former or current), and hypercoagulable conditions were also documented. Prior lower-extremity interventions for PAD, including surgical bypass or endovascular therapy, occurring before the index procedure were noted. The use of medications of interest prior to the first procedure was captured including aspirin, statins, P2Y12 (ADP receptor) inhibitors, and anticoagulants including direct oral anticoagulants (DOACs). Our analysis was performed based on the reintervention type (major vs minor), and the procedural characteristics and perioperative outcomes were compared between the two groups. Thus, patients who received multiple reinterventions may be represented in both major and minor categories depending on the magnitude of their procedures.
Operative characteristics
LER procedures were categorized as open or endovascular. Hybrid procedures consisted of both open and endovascular components and were considered major procedures in the reintervention analysis. Open procedures were divided into endarterectomy and bypass, and the type of conduit used was noted. Supra-inguinal bypasses were defined as aortofemoral, iliofemoral, femoral–femoral, or axillofemoral procedures. Infra-inguinal bypasses were defined as bypasses originating at or below the common femoral artery connecting to distal arteries. Endovascular interventions were classified as balloon angioplasty, stenting, atherectomy, or atherectomy and stenting. The indications were divided into claudication and CLTI. Additional details included laterality of treated vessels and anatomical location of disease.
Perioperative outcomes
Perioperative complications (within 30 days) following each procedure were recorded. Operative site complications included hematoma, pseudoaneurysm, wound infection, and bleeding defined as any transfusion requirement or return to the operating room (OR) for bleeding. Pneumonia, urinary tract infection (UTI), arterial thrombosis in the bypass or revascularized vessel, deep venous thrombosis (DVT), pulmonary embolism (PE), stroke, acute renal failure (ARF) defined as creatinine rise ≥0.5, and new-onset hemodialysis after the procedure were also captured. Additionally, return to the OR, major limb loss (any above-the-ankle amputation), and mortality were documented.
Statistical analysis
Reintervention rate was calculated as the percentage of patients receiving ipsilateral reinterventions. Student t test for continuous variables and chi-square or Fisher test for categorical variables were used to identify statistical differences in perioperative outcomes. SAS 9.4 software was used for all analyses.
Results
Patient characteristics
Demographic characteristics of patients who underwent reinterventions.
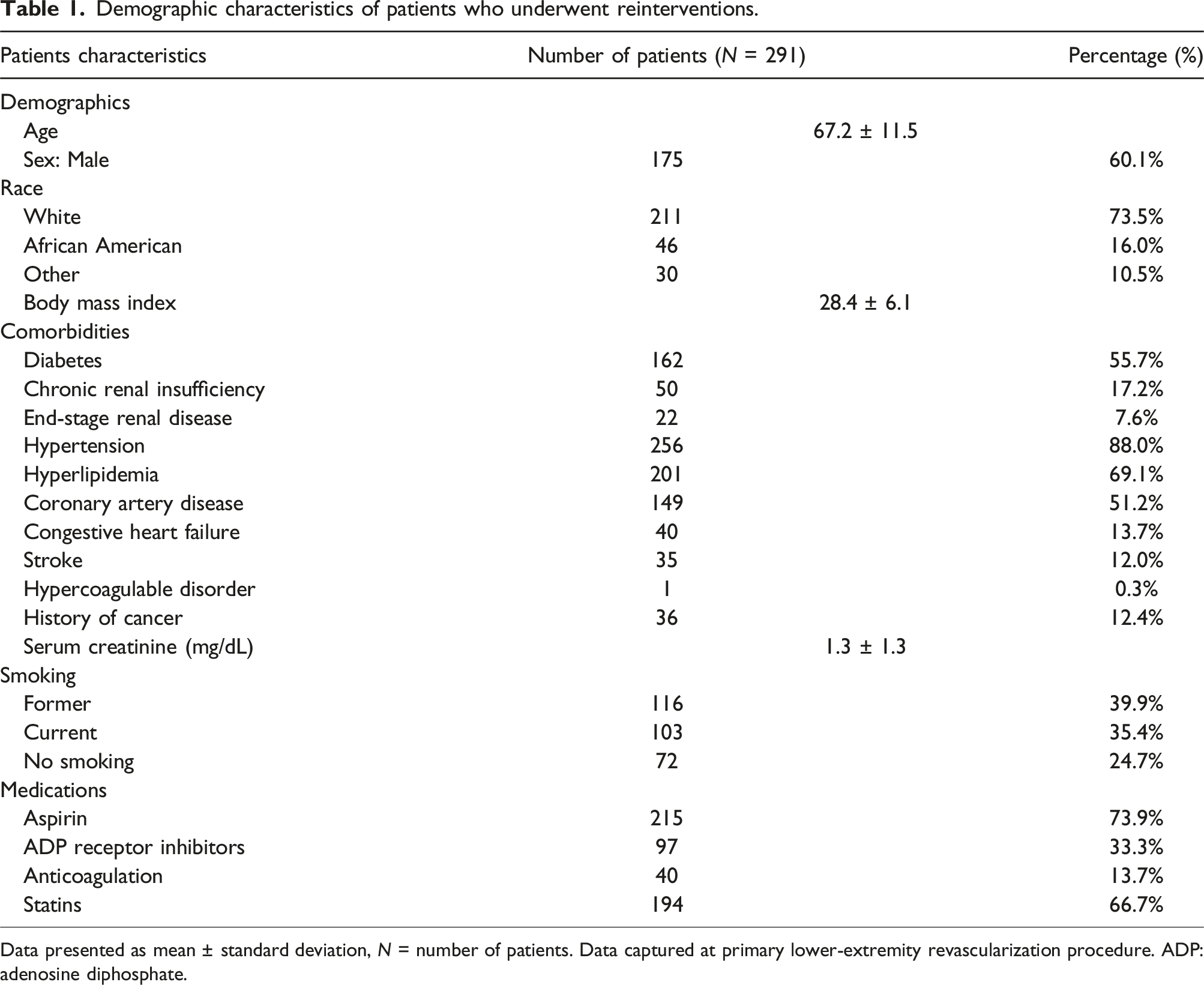
Data presented as mean ± standard deviation, N = number of patients. Data captured at primary lower-extremity revascularization procedure. ADP: adenosine diphosphate.
Procedural details for major and minor reinterventions.
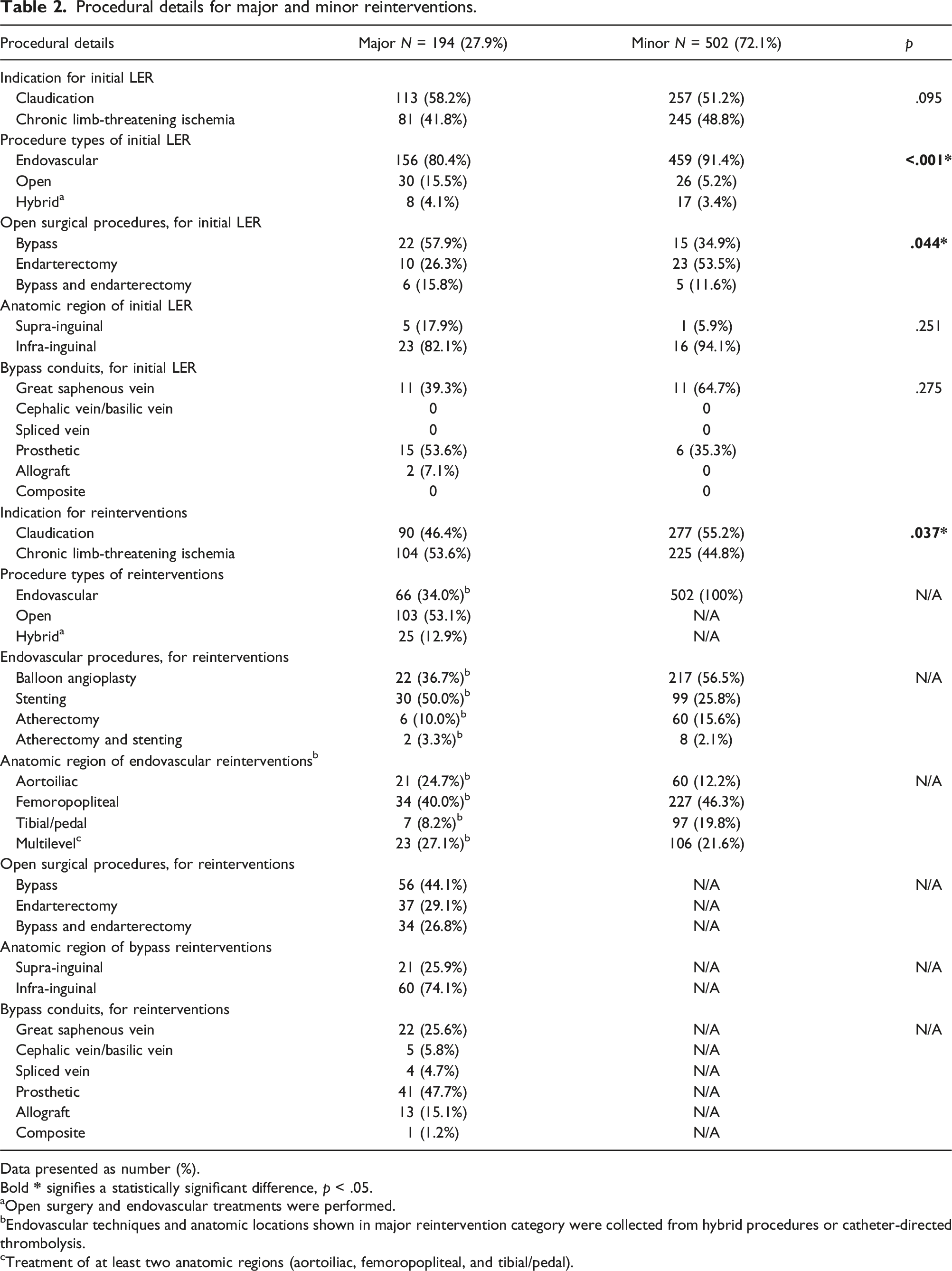
Data presented as number (%).
Bold
aOpen surgery and endovascular treatments were performed.
bEndovascular techniques and anatomic locations shown in major reintervention category were collected from hybrid procedures or catheter-directed thrombolysis.
cTreatment of at least two anatomic regions (aortoiliac, femoropopliteal, and tibial/pedal).
Major and minor reinterventions
During the study period, there were a total of 696 ipsilateral reinterventions performed (right = 336 left = 360). The range of reinterventions was 1 to 12 over a mean follow-up period of 2.5 years. The follow-up period ranged from a minimum of 30 days to a maximum time of 9.0 years. The average time to first reintervention was 254 days following the index procedure (supplemental table). The majority of reinterventions were minor (n = 502, 72.1%). While the indication for the initial LER was not significantly different between the two groups, major reinterventions were significantly more likely to be performed for CLTI than for minor reinterventions (53.6% v. 44.8%, p = .037). Further, major reinterventions also required longer hospital stays than minor reinterventions (7.5 days vs 4.3 days, p = <0.001) (Table 2).
Endovascular reinterventions
The majority of minor reinterventions were balloon angioplasty procedures (56.5%). Stenting was used in approximately a quarter of minor reinterventions (25.8%) and was the most common endovascular technique involved in major reinterventions (50.0%). Most endovascular treatments occurred in the femoropopliteal region for both minor (46.3%) and major (40.0%) reinterventions. Endovascular procedures in major reinterventions were either a component of a hybrid procedure or used concomitantly with catheter-directed thrombolysis (Table 2).
Open surgical reinterventions
Most open reinterventions were surgical bypasses (44.1%) or hybrid procedures with both bypass and endarterectomy (26.8%). The majority of bypass reinterventions were in the infra-inguinal region (74.9%). The most common conduits used in these procedures were prosthetic (47.7%) followed by great saphenous vein grafts (25.6%) (Table 2).
Subgroup analysis of major reinterventions
Procedural details for major reinterventions, open and CDT.
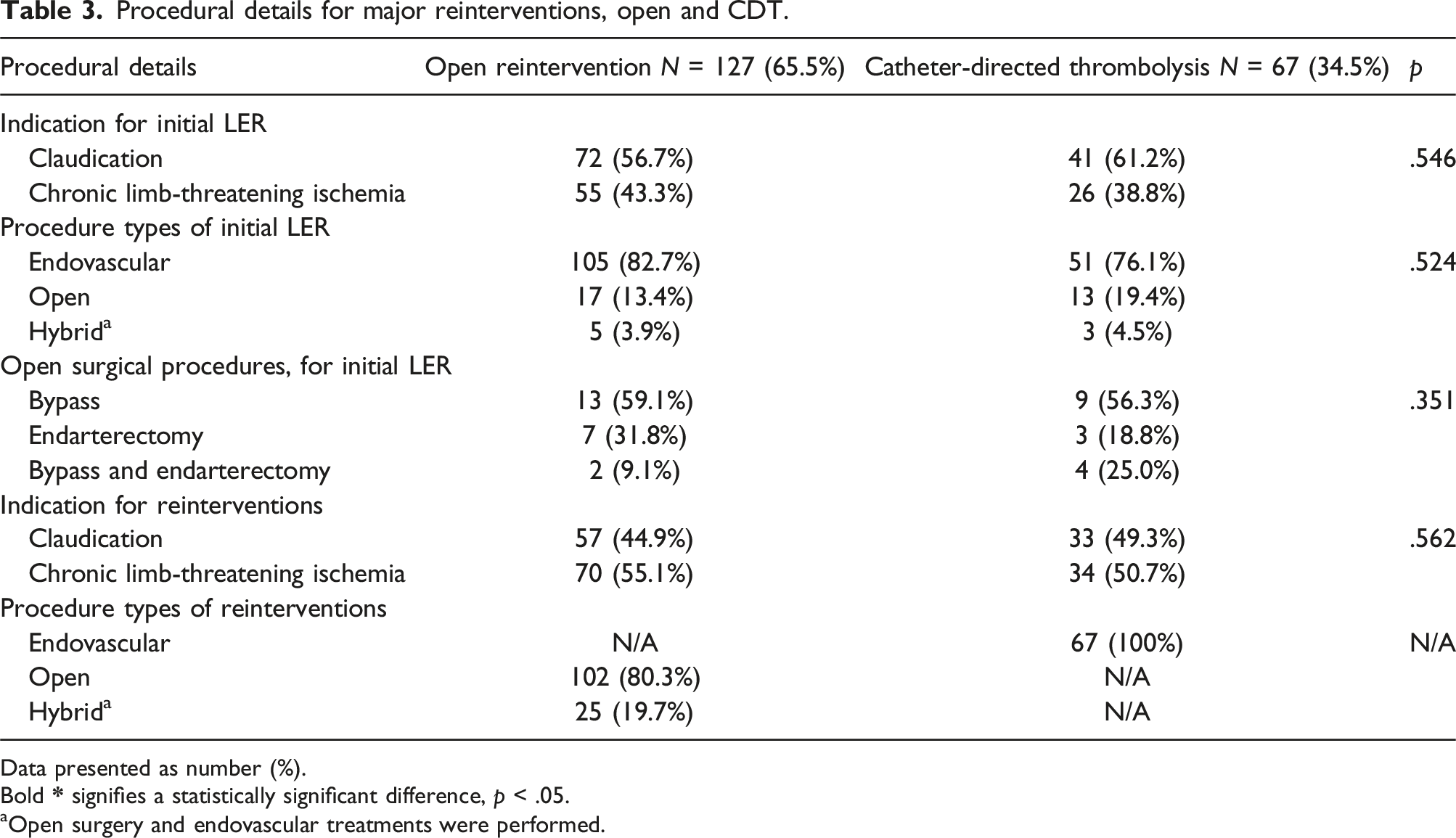
Data presented as number (%).
Bold
aOpen surgery and endovascular treatments were performed.
Perioperative outcomes
Perioperative outcomes following major and minor reinterventions.
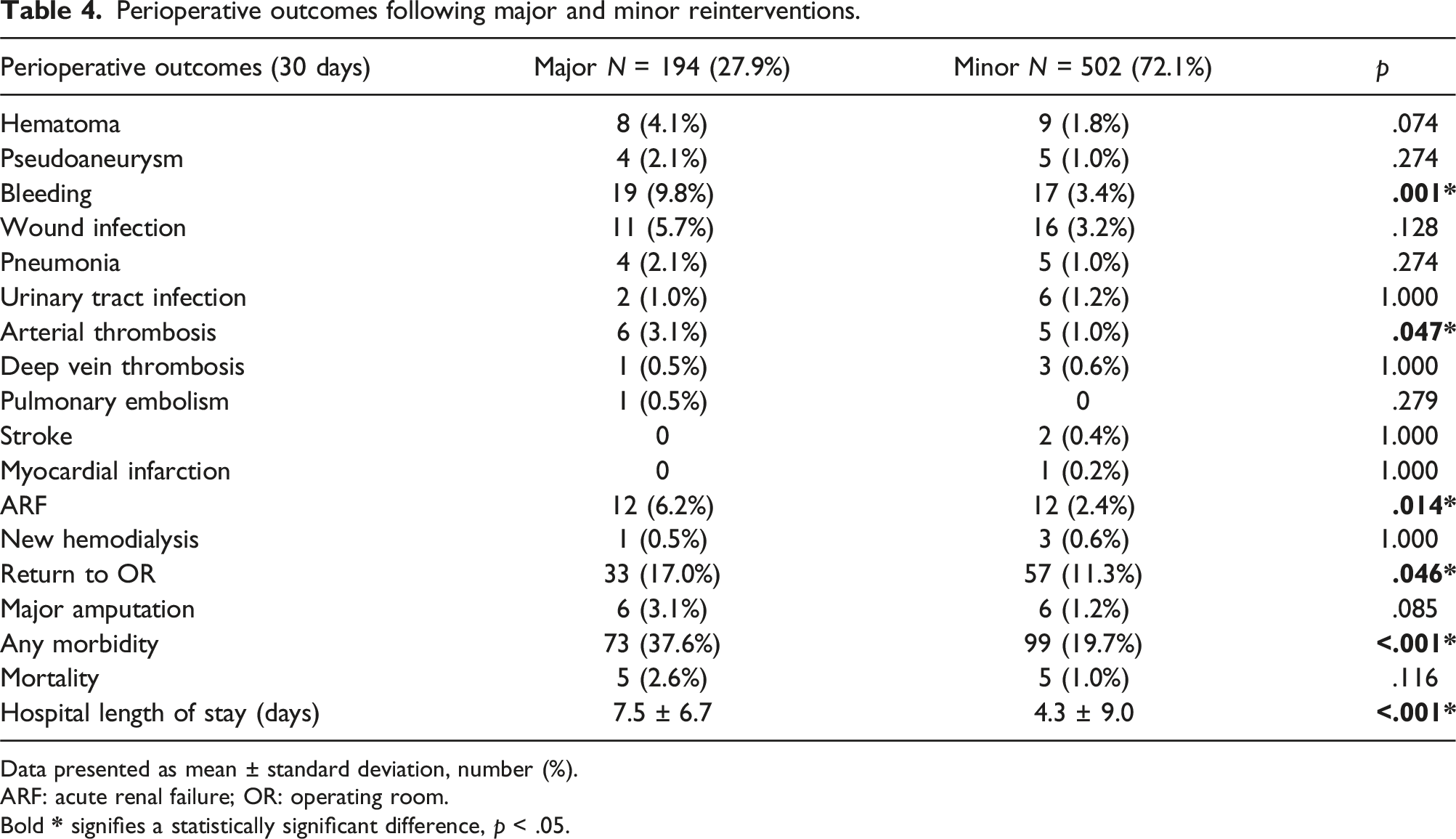
Data presented as mean ± standard deviation, number (%).
ARF: acute renal failure; OR: operating room.
Bold
Perioperative outcomes following open reinterventions and CDT.
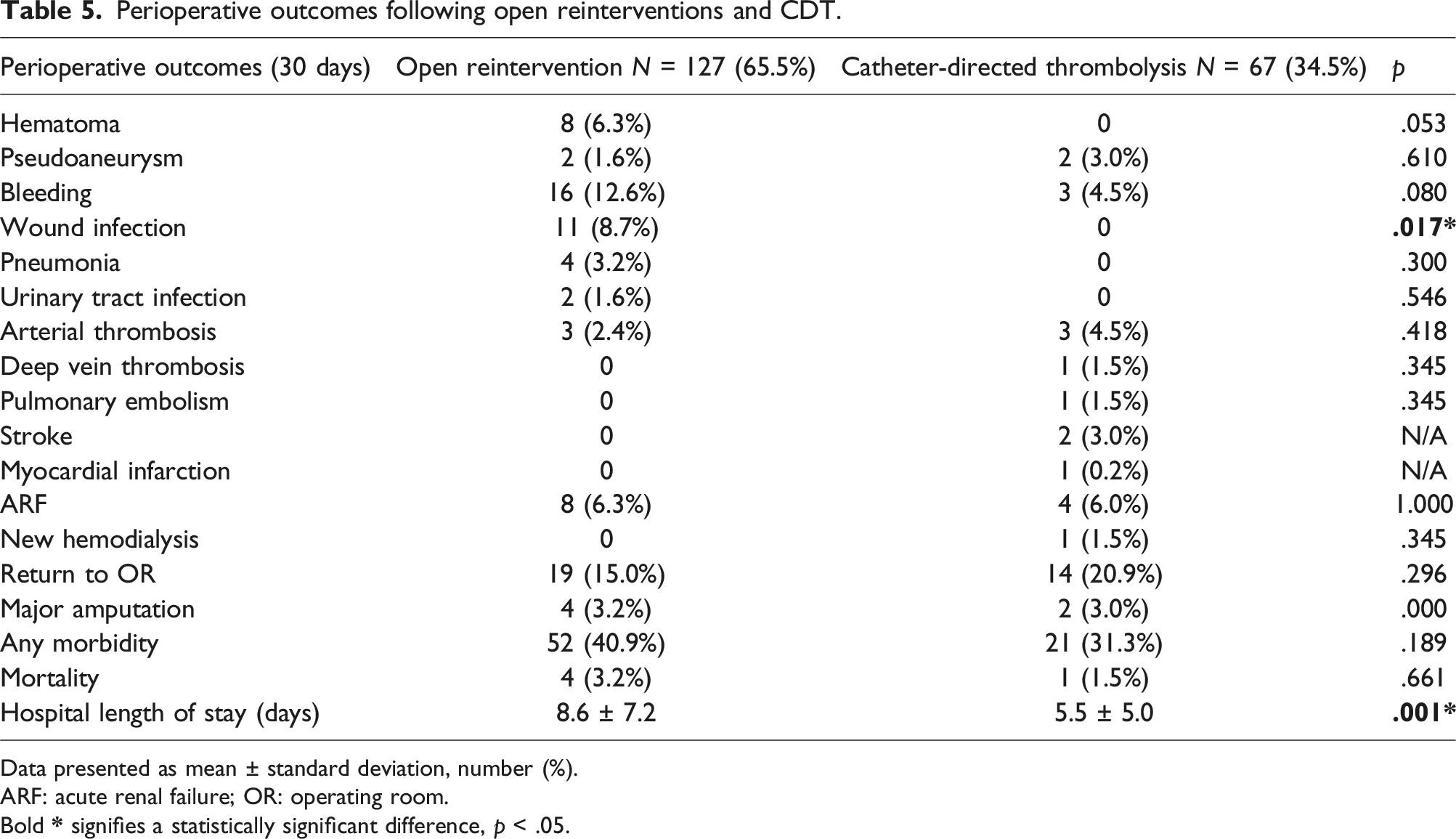
Data presented as mean ± standard deviation, number (%).
ARF: acute renal failure; OR: operating room.
Bold
Discussion
In this retrospective study of 713 patients undergoing LER for PAD at a tertiary care center, a total of 696 ipsilateral reinterventions were performed on 40.8% of patients, and perioperative outcomes associated with reinterventions of different magnitudes were evaluated. Although major reinterventions were associated with increased perioperative morbidity, including significantly higher rates of bleeding, thrombosis, acute renal failure, and return to the OR, there was no difference in mortality between the two types of reinterventions. When comparing perioperative complications associated with open reinterventions to those of CDT in the subgroup analysis, neither overall morbidity nor mortality was significantly different.
This study demonstrated a cumulative reintervention rate of more than 40%. Reintervention rates differ significantly depending on a variety of factors including smoking history, length of follow-up, disease progression, and operative or procedural history.14–17 In current literature, reintervention rates over at least 2 years of follow-up range from 24% to 58% for patients undergoing LER for CLTI.4,6,7,17 High rates of reinterventions and additional LER increases the cost of care of PAD and the risk of morbidity for patients. In fact, multiple reinterventions in claudicants have been associated with disease progression to CLTI and worse PAD outcomes. 18 Based on these results, it is important for operators to proceed with multiple LER only when completely necessary, and to select an optimal reintervention procedure that minimizes morbidity and provides adequate patency and sustainable relief of symptoms.
This analysis demonstrated that major reinterventions were associated with increased perioperative morbidity when compared to minor reinterventions. Current literature comparing reinterventions of different magnitudes is limited; however, open and endovascular primary LER has been thoroughly studied. In a recent analysis from the Vascular Quality Initiative database, treatment with open surgical bypass in patients with premature PAD was associated with increased perioperative morbidity, and similar rates of major amputation and mortality when compared to endovascular treatment. 19 Similarly, in a population of active smokers with PAD, open bypass was associated with higher rates of wound complications than endovascular therapy, and specifically for patients with intermittent claudication, an increased risk of MI or stroke within the perioperative period. 10 In contrast, the BEST-CLI trial demonstrated that patients with CLTI and adequate great saphenous vein have significantly fewer major adverse limb events (MALEs) or death when initially treated with surgical bypass than endovascular therapy, with similar incidences of major adverse cardiovascular events (MACEs). 8 Although our data is consistent with research reporting increased perioperative morbidity following open surgical interventions, major adverse limb and cardiovascular events occurring beyond 30 days after the procedure were not assessed. Therefore, while BEST-CLI provides strong evidence in support of open LER for primary procedures, additional analysis from the trial could shed light on the risks associated with minor and major reinterventions.
Major reinterventions had significantly higher incidence of ARF than minor reinterventions. ARF is a common complication associated with LER for PAD; however, its incidence varies based on procedure magnitude and indication. Following endovascular procedures for symptomatic femoropopliteal disease and CLTI, studies have reported respective rates of perioperative ARF as high as 11.7% and 10.4%, respectively, where ARF was also independently associated with post-intervention mortality.20,21 Conversely, after open bypass interventions, post-operative ARF rates as low as 4% have been described, and retrospective studies have proposed worse long-term renal outcomes after endovascular procedures when compared to open surgery.22,23 In contrast to the results just described, rates of ARF in our study were significantly higher for major (6.2%) than for minor reinterventions (2.4%). We speculate that the statistically significant difference between major and minor rates of ARF in our analysis could be related to variations in volume status with open procedures and fluctuations in blood pressure with the use of general anesthesia. Additional factors that could have contributed to this finding include the use of iodinated contrast in major reinterventions that were part of hybrid procedures, and the repeat use of contrast in CDT requiring multiple sessions. To better inform clinicians of the most appropriate management strategy for preserving renal function in patients requiring multiple LER for PAD, we suggest that future work investigating reinterventions should report comparative rates of ARF following procedures of different magnitudes.
In the subgroup analysis, there was no difference in perioperative morbidity or mortality between open surgery and CDT. Current literature comparing open reinterventions and CDT for claudication and CLTI is limited; however, a 2018 Cochrane meta-analysis compared surgery and thrombolysis as the initial intervention for ALI. This review concluded that perioperative limb salvage and mortality were similar for both treatments, and the investigators reported that there was insufficient evidence to endorse either procedure over the other. 24 Given this result and our comparable subgroup analysis outcomes for indications other than ALI (claudication and CLTI), it is reasonable to categorize both open surgery and CDT as the same magnitude of procedure. Additionally, the previously described meta-analysis reported that 30-day rates of major bleeding and distal embolization were greater for patients in the thrombolysis group. 24 Similarly, in several retrospective studies evaluating CDT and surgery for the treatment of ALI, rates of bleeding complications were either comparable between the two procedural groups or associated with CDT.25,26 While not significantly different in this analysis, our results are not consistent with these trends. In this study, open reinterventions resulted in higher rates of both hematoma (6.3% vs 0%) and bleeding (12.6% vs 4.5%) than CDT. One explanation for our discordant outcomes is that our study evaluates reinterventions while the other analyses focus on primary treatments for ALI. Since more than 17% of patients who underwent open surgical reinterventions already received some form of prior open revascularization, it is possible that their subsequent surgical procedures involved redo-dissections and reoperation in scarred fields which are known to cause additional bleeding. Therefore, CDT may help minimize bleeding in patients needing repeat revascularization in a limb that was previously treated with open surgery.
The results of the subgroup analysis also suggest that open surgical interventions contributed more than CDT to the differences in perioperative outcomes in the primary study. Open surgeries often requiring large incisions, tissue manipulation, and extensive dissection especially in those with a history of prior open LER explain the higher rates of wound complications and serious bleeding as compared to endovascular CDT technique. Since severe bleeding and wound infections represent more than 40% of overall morbidity after major reinterventions and occur after just 4.5% of CDT procedures, open surgery likely contributes more to the adverse outcome trends in the primary analysis than does CDT.
There were several limitations present in this study. Since this was a retrospective analysis, data that was not accessible via EMR was excluded. Missing information regarding previous operations, procedural complications, or follow-up data at other institutions could have potentially influenced the reported outcomes. Additionally, selection bias is present in the current study as different specialists have different thresholds for reintervention and for types of reinterventions offered. Since there is no standardized institutional protocol defining minimum requirements for intervention, the ability to stratify indication for procedure into distinct categories based on claudication severity is also limited in this study. As such, it was not possible to discern patients presenting with intermittent claudication from those with lifestyle-disabling claudication, which may have impacted the decision to proceed with reintervention. Further, since long-term outcomes were not analyzed in our study, comparative reintervention rates between the major and minor groups could not be derived; however, long-term survival and limb outcomes following reinterventions of different magnitudes are a topic of current research by our group. Finally, this study did not stratify magnitude of reintervention based on anatomical location of procedure. It is conceivable that the lesion location could disproportionately influence the perioperative outcomes for major or minor reinterventions, which may affect the generalizability of our results.
Conclusions
Major reinterventions after LER for PAD are associated with significantly higher morbidity than minor reinterventions with no difference in mortality. Approximately one-third of patients undergoing major reintervention in the form of open surgery or CDT develop perioperative complications. This study provides patient outcomes which can be used to discuss the risks associated with reinterventions of different magnitudes in patients with PAD.
Supplemental Material
Supplemental Material - Perioperative complications of minor and major reinterventions for peripheral arterial disease
Supplemental Material for Perioperative complications of minor and major reinterventions for peripheral arterial disease by Joshua J Huttler, Keyuree K Satam, Tanner I Kim, Haoran Zhuo, Yawei Zhang, Edouard Aboian, and Raul J Guzman in Vascular.
Footnotes
Author’s note
Conference Presentation: Poster presented virtually at Society for Clinical Vascular Surgery 48th Annual Symposium, Miami, Florida, USA, March 13–17, 2021 (“Perioperative Outcomes of Minor and Major Reinterventions For Peripheral Arterial Disease”).
Acknowledgments
We would like to thank the REDCap team at Yale University for their support in database setup and maintenance.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Joshua Huttler disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by National Heart, Lung, and Blood Institute of the National Institutes of Health. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Heart, Lung, and Blood Institute or the National Institutes of Health under Award Number T35HL007649.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.