
Abstract
Objectives
This study aimed to evaluate the outcomes and anatomical predictors of the complications of flared limb (FL) use for ectatic common iliac arteries accompanied by abdominal aortic aneurysm treated with endovascular aneurysm repair (EVAR).
Methods
In this single-center retrospective study, we reviewed data from 391 patients (638 limbs) treated between 2005 and 2020. The cohort was divided into two groups. The standard limbs (SLs, n = 403) included stent graft (SG) of <20 mm in diameter and the FLs (n = 235) included stent graft of ≥20 mm in diameter. Complications within 30 days were investigated as the short-term outcome. Limb events during follow-up including type Ib endoleak (EL), type IIIa EL, and limb occlusion were compared between SLs and FLs using log-rank test.
Results
Early results indicated that the FL group had a significantly higher incidence of intraoperative type Ib EL at 5.1% (12), than 1.7% (7) in the SLs (p = .016). For 19 patients in whom intraoperative type Ib EL was discovered, SG extension alone or internal iliac artery embolization was all performed before completing the procedure. Overall, we noted one case of type Ib EL and two cases of limb events in each group at 30 days. Over a median follow-up of 39 months, 31 (4.9%) events (17 type Ib EL, 2 type IIIa EL, and 12 limb events), 13 (5.5%) in FLs and 18 (4.5%) in SLs (p = .984), were observed. The FLs had significantly higher rates of aortic sac enlargement, with 46 (19.6%) cases for FLs and 36 (8.9%) for SLs (p < .001). The Kaplan–Meier analysis revealed significant differences at 5 years in SLs versus FLs for freedom from type Ib EL (96.6% vs 82.4%, respectively; p < .001) and no difference in freedom from limb events (94.7% vs 84.5%, respectively; p = .519). Furthermore, no difference was observed for overall survival and aneurysm-related mortality.
Conclusions
Although an FL for EVAR is used to treat dilated iliac arteries, there is an increased risk of intraoperative and late type Ib EL and aortic sac enlargement. Long-term close follow-up is mandatory, especially in the patients who undergo EVAR using FLs.
Introduction
The probability of abdominal aortic aneurysm (AAA) with coexisting aneurysm or enlarged common iliac artery (CIA) is currently reported to be 20% to 40%. 1 In such cases, it is important to secure a distal landing zone on the side where the ectatic or aneurysmal CIA is located when planning treatment with endovascular aneurysm repair (EVAR). Currently, several endovascular techniques are available to treat aorto-iliac aneurysms. One of these methods involves the use of the external iliac artery (EIA) as a landing zone after embolization of the internal iliac artery (IIA), the second uses a flared iliac limb up to 25 mm in diameter for CIA bifurcation, and the third uses a branched iliac stent graft with a snorkel and sandwich technique.2,3 Compared with other techniques, the flared limb (FL) method, which can preserve the IIA, is the simplest and has the advantage of a short surgical time.4,5 However, if EVAR is performed using an FL, dilatation of the CIA may continue to progress during the follow-up period. This has the disadvantage of a high possibility of type Ib endoleak (EL) and reintervention. 6 Ballotta et al. 7 reported that aneurysmal or ectatic CIAs were twice as likely to become enlarged than non-aneurysmal CIAs.
Clear evidence on the long-term outcomes of treatment with FL and predictors of efficacy during the follow-up period are lacking. As such, the use of FLs in EVAR remains controversial. To address this knowledge gap, the present study aimed to evaluate the outcomes and anatomical predictors of the complications of FL use for ectatic common iliac arteries accompanied with AAA treated with EVAR.
Methods
Data from 640 patients, treated with standard EVAR at our center between August 2005 and June 2020, was retrospectively reviewed. The exclusion criteria were (1) preprocedural planned EIA extension; (2) isolated iliac artery aneurysm; (3) use of AFX2 (Endologix Inc, Irvine, CA); (4) use of aorto-uniiliac devices; (5) ruptured AAA; (6) emergent EVAR; (7) use of iliac branch device; (8) mycotic AAA; (9) other (AEF, follicular lymphoma, PAU, Lt limb converter, status per AAA repair, CIA dissection, failed EVAR, and no preoperative computed tomography (CT) image). Eventually, 638 limbs from 319 patients with AAA who underwent EVAR were included in the analysis. Figure 1 presents a flow chart of patient enrollment/exclusion process. Flow diagram of the patient enrollment and exclusion process.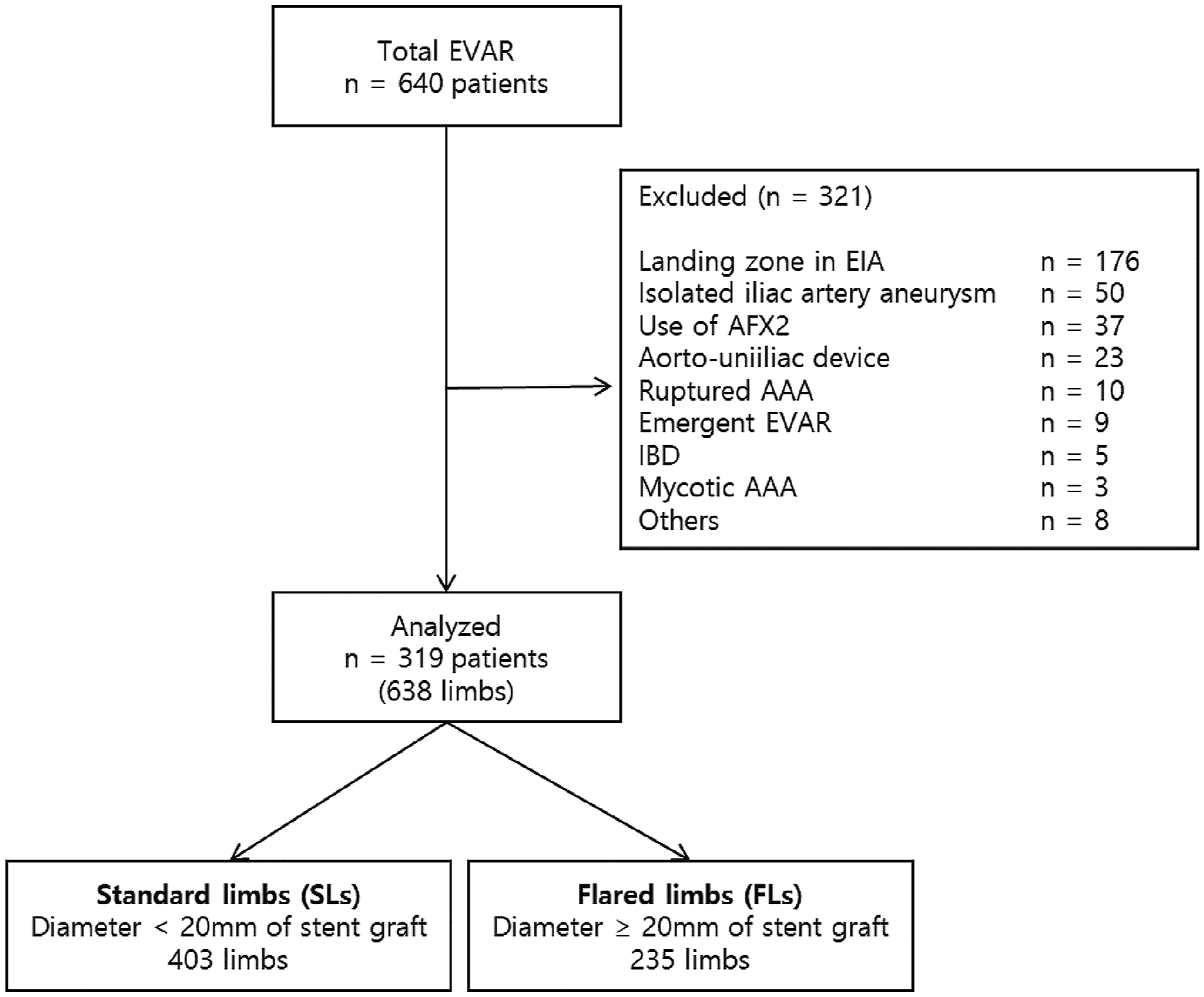
Three vascular surgeons and two cardiologists developed a plan for EVAR and determined the size of the stent graft based on preoperative computed tomography angiography. As a rule, the diameter of the iliac limb was selected to be 15% to 25% oversized. Aortic stent grafts were purchased from four manufacturers: Zenith (Cook Medical, Bloomington, IN), Endurant (Medtronic vascular, Santa Rosa, CA, USA), Excluder (W. L. Gore & Associates, Flagstaff, AZ), and INCRAFT (Cordis, Bridgewater, NJ, USA).
Contrast CT was performed within 7 days after EVAR. Subsequently, the imaging was repeated at 6 and 12 months and annually thereafter during the follow-up period to monitor patient progress. For patients in whom contrast medium could not be used, a non-contrast CT was performed, and if a leakage was suspected, vascular ultrasound was performed.
Patient baseline and demographic characteristics.
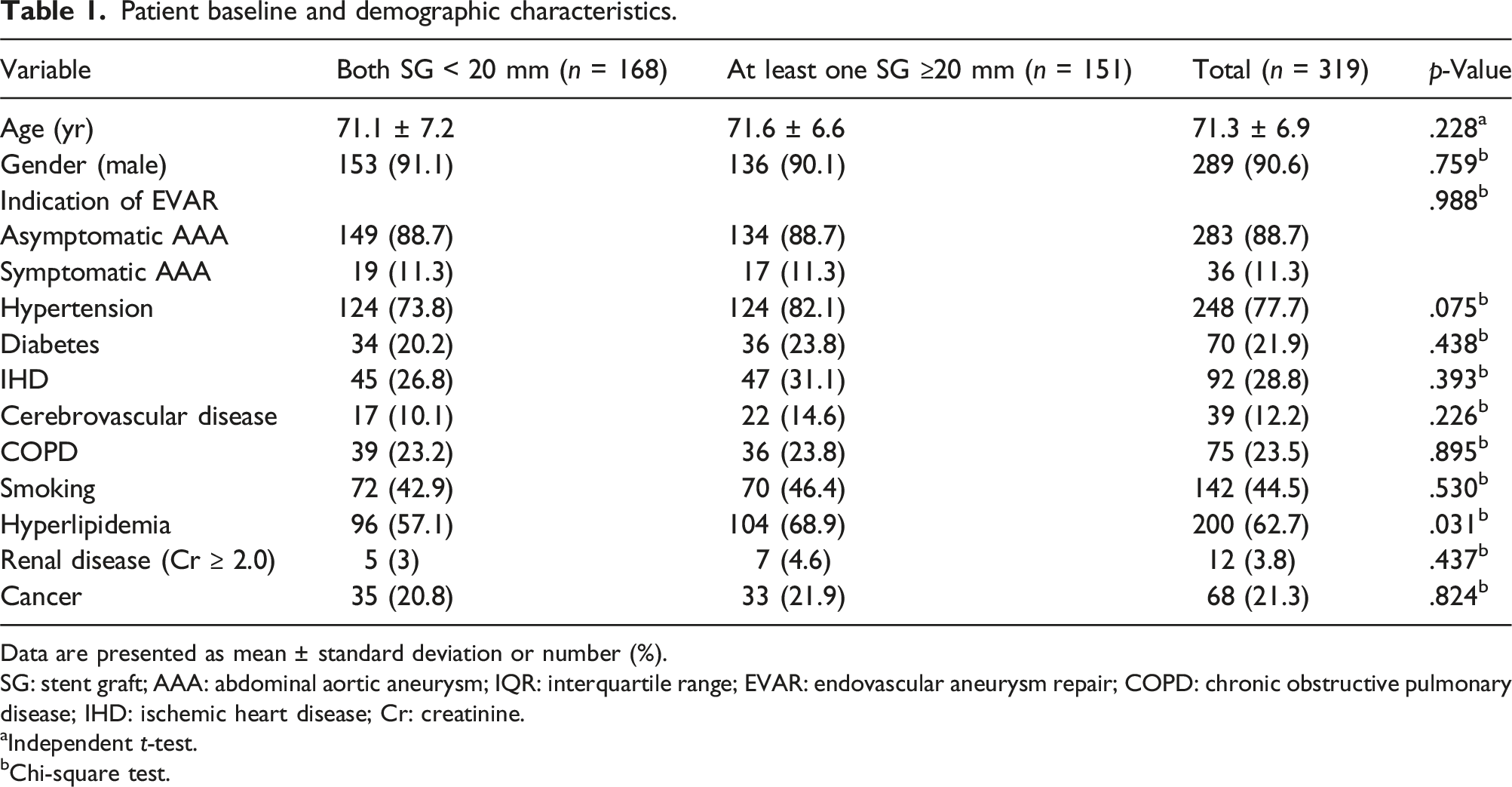
Data are presented as mean ± standard deviation or number (%).
SG: stent graft; AAA: abdominal aortic aneurysm; IQR: interquartile range; EVAR: endovascular aneurysm repair; COPD: chronic obstructive pulmonary disease; IHD: ischemic heart disease; Cr: creatinine.
aIndependent t-test.
bChi-square test.
Anatomical factors between the SL group and FL group.

SL: standard limb; FL: flared limb; SG, stent graft; SD: standard deviation; AAA: abdominal aortic aneurysm; IQR: interquartile range; CIA: common iliac artery.
aMann–Whitney test.
bChi-square test.
Complications within 30 days, including intraoperative type Ib EL, type Ib EL, limb occlusion or stenosis of >50%, and death rate, were examined during the follow-up period.
All statistical analyses were performed using IBM SPSS ver. 26.0 (IBM Corp., Armonk, NY, USA). Continuous variables are denoted as median with mean ± standard deviation or interquartile range. Categorical variables are expressed in terms of frequency and percentage, and the two groups were compared using the chi-square test and Fisher exact test. During the follow-up period, the incidence of limb events was analyzed using the Kaplan–Meier method, and the comparison between the two groups was performed using the log-rank test. Statistical significance was set at values of p < .05.
This study was registered with the Samsung Medical Center institute review board (IRB). And it was approved by the same organization. Informed consent was obtained from all patients.
Results
Early and late outcomes in the SL and FL groups.

SL: standard limb; FL: flared limb; IQR: interquartile range.
Description of early and late causes and procedures of reintervention during the follow-up.

SL: standard limb; FL: flared limb; EL: endoleak; EIA: external iliac artery; IIA: internal iliac artery; FF bypass: femoro-femoral bypass.
The incidence of aortic sac enlargement was significantly higher in the FL group than in the SL group (p < .001). Three aneurysm-related mortalities (ARMs) were noted, with an overall mortality rate of 9.6% (Table 3). The 5-year Kaplan–Meier analysis, derived including intraoperative type Ib EL, showed a statistically significant difference in the freedom event rate from type Ib EL between the two groups (SLs vs FLs, 96.6% vs 82.4%, respectively; p < .001) (Figure 2). However, no difference was observed at 5 years in terms of freedom from limb occlusion (SLs vs FLs, 96.4% vs 97.1%, respectively; p = .117) or total limb event (SLs vs FLs, 94.7% vs 84.5%, respectively; p = .519). Separate comparisons of type Ib endoleak between the standard limbs (SLs) and flared limb (FLs) groups during the follow-up.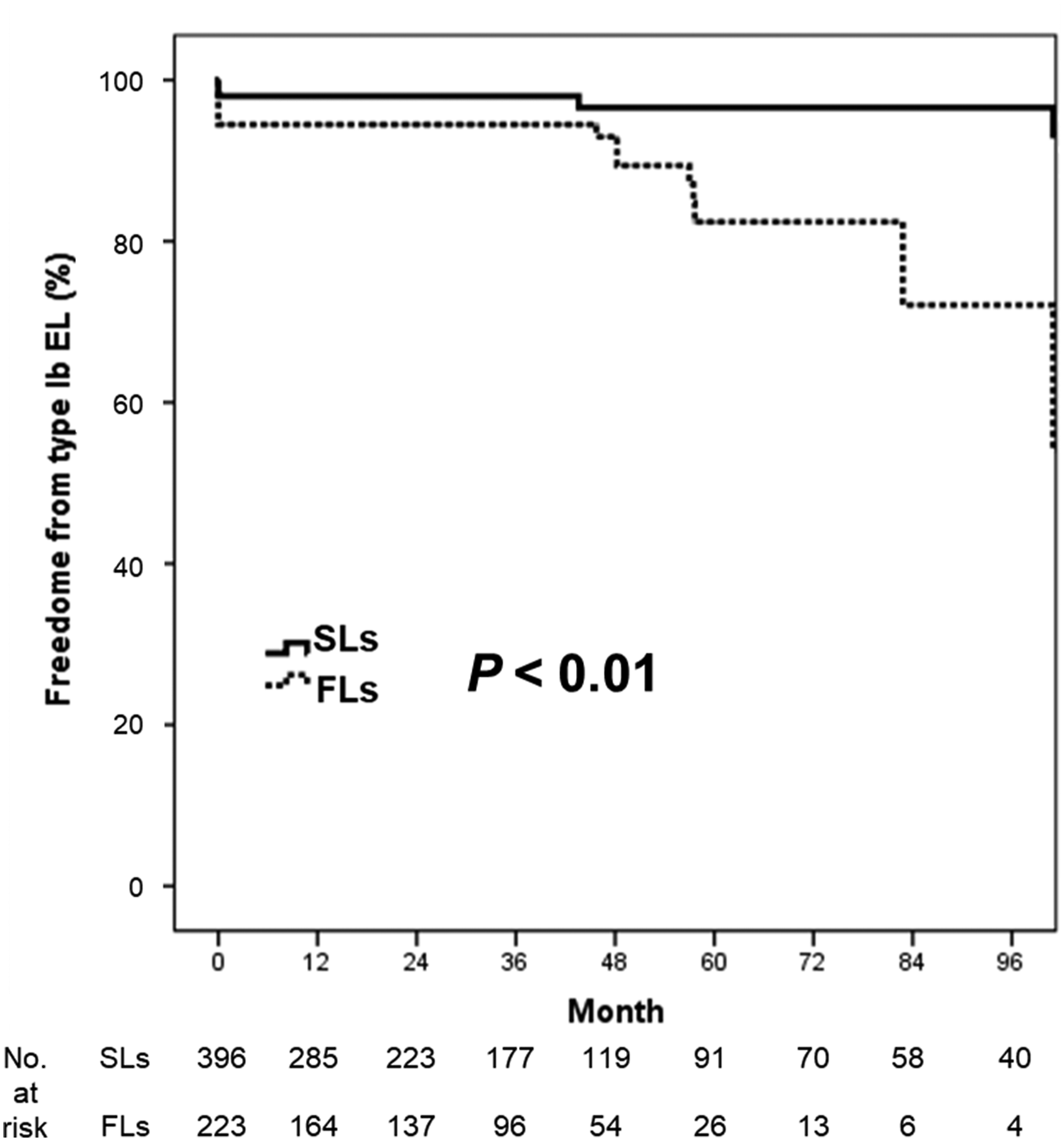
No difference was found for overall survival and ARMs in patients with SLs and FLs (77.5% vs 72.1%, p = .154, and 100% vs 98.6%, p = .168, respectively).
Discussion
The FL was used to preserve the internal iliac artery. Embolization of the IIA into a coil is a common method to prevent blood flow to the aortic aneurysm through the IIA when the landing zone is determined for use as an EIA.8,9 However, embolization of the IIA can cause side effects, such as erectile dysfunction and severe buttock pain, and in some cases, obstruction of blood flow in the lower intestinal tract, resulting in bowel necrosis or sepsis. 10 With the development of the flared type stent graft, comprising an enlarged distal part, the procedure can be performed without embolization of the IIA. However, studies on FL stability and long-term outcome are scarce.5,11
Our study findings might raise questions as the mean maximum diameter of AAA was 53.5 mm, which is below the 55 mm treatment threshold outlined in the guidelines. 12 This discrepancy is because, in Korea, the insurance standard for an indication for the EVAR procedure for an AAA is when the AAA has a diameter of 50 mm or more.
Apart from proximal SG, there is no consensus for oversizing of distal SG, but usually around 10%–15% oversizing would be acceptable. However, in ectatic cases, we have experienced >15% oversizing would be safe to prevent type 1b EL. In the cases of a narrow proximal but large distal or vice versa, we usually have a focus on the iliac landing zone with a larger diameter, when the length of the iliac landing zone should be considered to prevent SG compression or occlusion at the narrowest portion as well as type 1b EL, simultaneously. As a result, our data showed that the degree of oversizing was significantly more than an SL group.
According to a recent report by Gray, 13 the risk of type Ib EL was significantly higher in the group treated with FL after a follow-up period of at least 3 years, even when no type Ib EL was present initially. In this study, the 5-year Kaplan–Meier analysis revealed a statistically significant difference in the freedom event rate of type Ib EL between the two groups. Conversely, in 2019, Pini et al. 14 reported no difference in freedom from free limb occlusion or type Ib EL in the 5-year Kaplan–Meier analysis between SLs (CIAs <16 mm) versus FLs (CIAs ≥16 mm). In addition, the 5-year iliac complication rates were similar between the two groups. In this study, no significant difference in freedom from limb occlusion at 5 years was observed between the two groups (p = .054).
In a study by Bonardelli et al. in 2022, 15 freedoms from ARMs and iliac-related reintervention were analyzed in 995 FLs in 795 patients over a median follow-up duration of 52 months. The estimated freedom from ARM was 99% and that from iliac-related reintervention was 95% at 5 years. The authors concluded that the use of FLs in EVAR resulted in a higher rate of freedom from ARM and lower reintervention rate. In the present study, the estimated freedom from ARM in a group of patients with at least one FL was 100% at 5 years. Additionally, no difference in overall survival was observed in patients with at least one FL and those without FL (78.1% vs 79.3%, respectively, p = .154).
The current study 16 evaluated three limb strategies—bell bottom (BB), iliac branch endoprosthesis (IBE), and coil and cover (CC)—for treating iliac artery aneurysms, using data from the GORE registry with 924 patients over 5 years. Findings revealed no significant differences in EL rates, stent migration, or aneurysm outcomes across methods. Notably, IBE required more reinterventions for additional grafts (8.6%) than BB (2.2%) and CC (1.3%). Conclusively, all strategies effectively manage iliac aneurysm, with the choice of strategy depending on specific patient needs and physician judgment.
The limitations of this study include the retrospective, single-center design, which may have introduced bias. Furthermore, we were unable to analyze all factors that can influence treatment decisions for AAA with ectatic CIA. Additionally, the SL group was larger than the FL group, which may have introduced a selection bias when comparing the two groups. Finally, the mean follow-up period was relatively short (median, 39 months; IQR 18.1–61.1 months); therefore, analysis over a longer follow-up period may be necessary to ensure the validity of FLs.
Conclusion
Although an FL for EVAR is commonly used to treat dilated iliac arteries, this technique is associated with an increased risk of intraoperative and late type Ib EL and aortic sac enlargement. Long-term close follow-up is, therefore, mandatory in patients who undergo EVAR using FLs.
Footnotes
Author contributions
Research: Choshin Kim, Yang-Jin Park, Joon-Kee Park, Young-Wook Kim, Dong-Ik Kim, Shin-Seok Yang, Taek Kyu Park, and Seung-Hyuk Choi. Manuscript: Choshin Kim, Yang-Jin Park, and Joon-Kee Park. Approval: Choshin Kim, Yang-Jin Park, Joon-Kee Park, Young-Wook Kim, Dong-Ik Kim, Shin-Seok Yang, Taek Kyu Park, and Seung-Hyuk Choi. Accountability: Choshin Kim, Yang-Jin Park, Joon-Kee Park, Young-Wook Kim, Dong-Ik Kim, Shin-Seok Yang, Taek Kyu Park, and Seung-Hyuk Choi.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.