
Abstract
Objective
Acute aortic occlusion (AAO), though rare, carries a high morbidity and mortality risk. Rapid recognition and revascularization are crucial for limb and life preservation. We present a case of a hybrid approach using open thrombectomy and endovascular arterial stent grafts in lieu of an open bypass for management of AAO.
Methods
This case describes a 77-year-old man who presented with new-onset lower extremity pain with associated sensory deficits and was found to have acute infrarenal aortic occlusion. Open femoral cutdown for open thrombectomy and distal embolic protection with endovascular balloon occlusion was combined with aortic and bilateral iliac artery stenting.
Results
The patient was discharged home on post-operative day 3 with resolution of his presenting symptoms and remains asymptomatic at 1-month follow-up.
Conclusion
This technique of aorto-iliac reconstruction using stent grafts has previously been described in the setting of chronic aorto-iliac occlusive disease; however, its use has not been previously documented in the setting of acute aortic occlusion. This case illustrates the safety and feasibility of a hybrid approach to AAO, particularly in patients who are physiologically unfit for open revascularization.
Keywords
Case Report
The patient provided written informed consent for the report of their case details and imaging studies; therefore, no additional institutional review board (IRB) approval was required. A 77-year-old male non-smoker with a history of hypertension and hyperlipidemia presented to the emergency department with acute onset of left gluteal and ipsilateral lower extremity pain for several days. He also reported numbness over the dorsal aspect of the left foot. He endorsed no prior history of claudication nor vascular procedures/interventions. Interestingly, the patient reported to emergency department 1 day prior to the index presentation with complaints of left leg and foot numbness. He underwent neurologic work-up for presumed acute neurologic event. Imaging studies, including a computed tomography scan and magnetic resonance imaging of the head, were negative for acute intracranial pathology. He was then discharged home.
On index presentation, the physical exam was significant for absent femoral pulses with monophasic pedal signals bilaterally. He had sensory deficits to the left midfoot with motor weakness of the left foot. His laboratory values were significant for leukocytosis of 11.3 (1000/μL) and elevated creatinine kinase of 1399 (U/L). Acute left lower extremity arterial ischemia was suspected (Rutherford 2b classification) and further evaluated with computed tomography angiography (CTA) of the aorta with lower extremity runoff. This demonstrated extensive occlusive thrombus within the infrarenal abdominal aorta extending into bilateral distal common iliac arteries. Bilateral external iliac arteries were patent with patent femoro-popliteal segments and 2-vessel runoff bilaterally. There was no evidence of aortic dissection nor intramural hematoma.
A heparin infusion was initiated, and the patient was taken emergently to the operating room for lower extremity revascularization. The right common femoral artery (CFA) was exposed via vertical groin incision, and circumferential control of the CFA, superficial femoral artery (SFA), and profunda femoris artery was obtained. Concurrently, ultrasound-guided access of the left CFA was obtained. A stiff 0.035″ wire was gently advanced into the infrarenal aorta. Aorto-iliac angiogram confirmed an occluded aorta with reconstitution of bilateral external iliac arteries (Figure 1). A 6 × 40 mm occlusion balloon was placed in the proximal left external iliac artery to protect from distal embolization during contralateral thrombectomy (Figure 2). The patient was maintained on full anticoagulation and activated clotting times (ACTs) were maintained in therapeutic range throughout the procedure. Aorto-iliac angiogram demonstrating aortic occlusion 3–4 cm below renal arteries (yellow arrow). Occlusion balloon (yellow arrow) placed in the proximal left external iliac artery to protect from distal embolization during open thrombectomy on the right side.

The right SFA and profunda femoris were clamped, and embolectomy of the right iliac and abdominal aorta was performed through transverse arteriotomy of the right CFA. A small amount of thrombus was returned, which appeared to be acute in nature. The remainder of thrombus was chronic and adherent to the arterial wall. Through the existing arteriotomy in the right CFA, wire and sheath access were established. A 0.035″ intravascular ultrasound catheter (Phillips Volcano, San Diego, CA) was advanced into the aorta and confirmed presence of non-diseased, thrombus-free aorta 2 cm below the renal arteries. The aorta measured 12–14 mm in diameter by IVUS at that level. A covered, balloon-expandable stent (11 × 79 mm VBX stent graft, Gore Medical, Flagstaff, AZ) was deployed in the infrarenal aorta. The wire was withdrawn from the aorta into the left common iliac artery. The left CFA was exposed via transverse groin incision. Circumferential control of the left SFA and profunda femoris was obtained to prevent distal embolization. The aortic stent graft was re-cannulated using a 0.035″ Glidewire (Terumo Medical, Somerset, NJ). IVUS evaluation confirmed bilateral intra-aortic wire placement. The aortic stent graft was carefully dilated with an Atlas 14 × 40 mm balloon to achieve full wall apposition.
An 8 × 59 mm VBX balloon-expandable stent graft was advanced into each iliac artery. These were simultaneously inflated with 1 cm overlap into the previously placed aortic stent graft. Fogarty balloon thrombectomy was then performed again on each side to retrieve residual loose thrombus from the iliac arteries. There was a small amount of embolization to the left internal iliac artery; however, the right internal iliac artery was widely patent on completion angiogram (Figure 3). A total of 43 mL of iodixanol contrast and 6.6 min of fluoroscopy time was required for the procedure. Estimated blood loss for the procedure was 200 mL, and operative time was 2 h and 20 min. Completion angiograms demonstrating patent infrarenal aortic stent and bilateral iliac artery stents. Left internal iliac artery with embolization (3a); however, the right internal iliac artery remains patent (3b).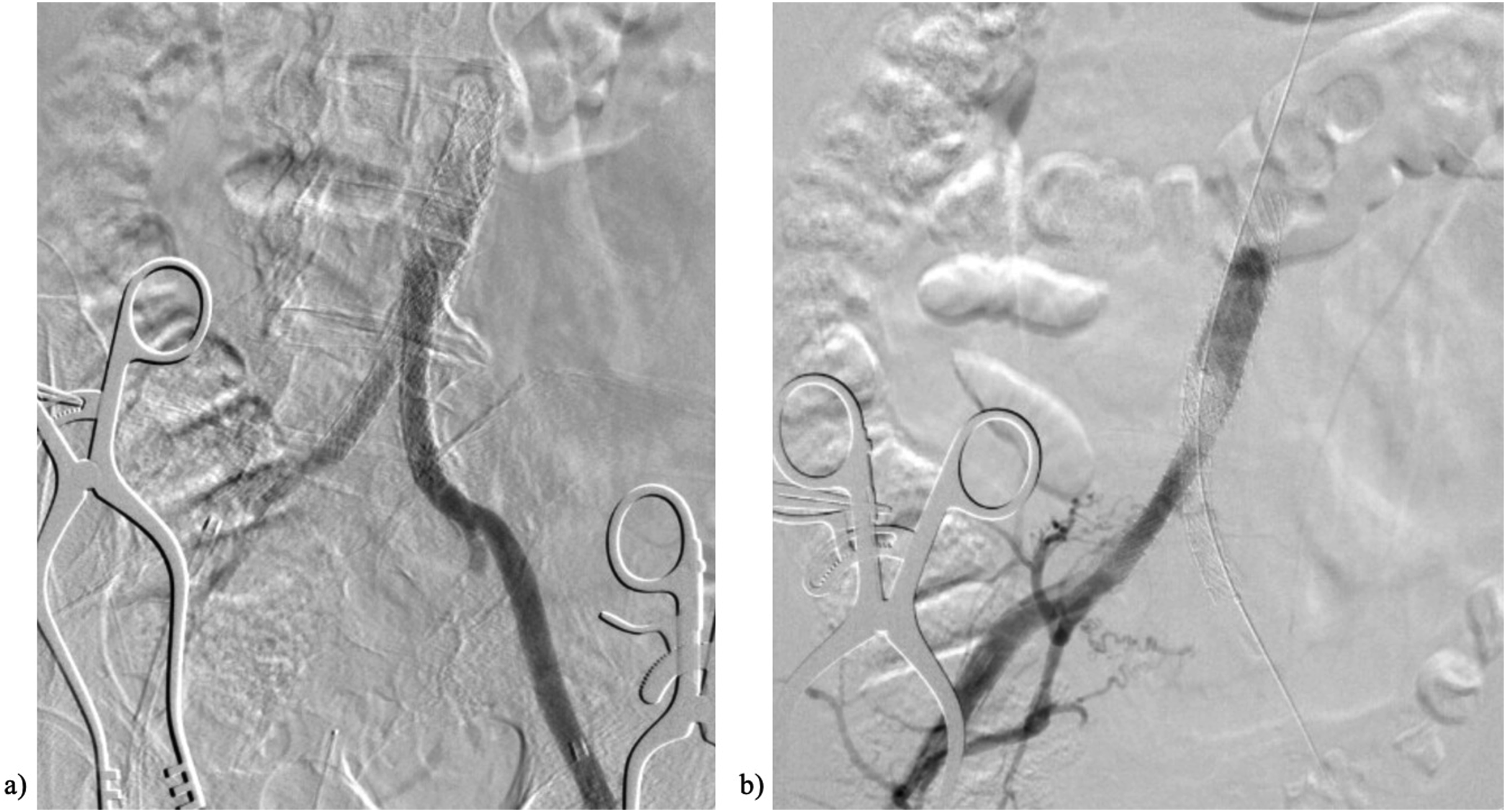
At the completion of the procedure, the patient had bilateral palpable femoral and dorsal pedal pulses. Fasciotomies were not performed at the discretion of the operating surgeon. Close monitoring for evidence of lower extremity compartment syndrome was instituted. The laboratory values, including creatinine kinase level, normalized post-operatively. The patient recovered well after revascularization and was discharged home on post-operative day 3 without motor or sensory deficits. Of note, additional embolic work-up was performed. Transthoracic echocardiogram was negative for intracardiac abnormalities with preserved ejection fraction. CTA of the chest demonstrated no evidence of aortic thrombus or aneurysm.
At 1-month follow-up, patient maintained full ambulatory status with stable bilateral lower extremity perfusion. He denied buttock or leg claudication. He was maintained on Eliquis, aspirin, and high-intensity statin daily regimen.
Discussion
Acute aortic occlusion is associated with high morbidity and mortality and therefore must be recognized and addressed emergently. In some cases, spinal or cerebrovascular etiologies are investigated as neurologic deficits of the lower extremities, thus delaying the diagnosis. 1 Despite treatment, 30-day mortality is estimated to be near 30%, 2 with even higher mortality rates for patients with severe motor or sensory deficits at the time of presentation.2–4 In this case, sensory deficits were initially incorrectly attributed to a central nervous system issue. The case highlights that patients who present with neurologic deficits should undergo pulse examination and further vascular evaluation so as not to delay the diagnosis of AAO.
For patients with AAO without renal artery involvement, revascularization strategies usually include transfemoral embolectomy in the setting of embolization, and in-line revascularization with aortobifemoral bypass or extra-anatomic axillobifemoral bypass for restoration of flow.5,6 Patients deemed higher risk for major vascular procedures more likely will undergo axillobifemoral bypass as they may not tolerate aortic cross clamping or laparotomy. 2 These open revascularization techniques for AAO are well-described with more recent studies reporting pharmacomechanical thrombectomy as an additional adjunct.2–4,7,8
We present a hybrid approach using bilateral open thrombectomy followed by covered aorto-bi-iliac stent grafts. The technique of covered aorto-bi-iliac stent grafts, known as covered endovascular reconstruction of the aortic bifurcation (CERAB), is commonly used for patients with aorto-iliac occlusive disease and has had good outcomes in terms of symptom improvement limb salvage rates and patency. 9 We present a case in which the same stent graft configuration was applied in the acute setting with the addition of open thrombectomy.
This technique eliminates the need for laparotomy or axillary dissection for patients with higher surgical risk. At the same time, it allows for in-line reconstruction with potential for shorter operative time compared to a bypass. The in-line reconstruction may also offer better long-term patency and leaves an option for future extra-anatomic bypass. Adjunctive techniques such as occlusion balloon for distal embolic protection during thrombectomy and intravascular ultrasound for appropriate sizing, thrombus location, and wire position should be considered to aid in the conduct of this hybrid procedure. In-situ thrombosis, saddle embolus, occluded prior graft/stents, hypercoagulable states, and low-flow states due to cardiac etiologies have been implicated as etiologies of AAO.4,10 The most likely etiology of AAO for this patient was in-situ thrombosis of underlying aorto-iliac disease, which was made evident by intraoperative IVUS evaluation.
Conclusions
Acute aortic occlusion is a rare but life- and limb-threatening diagnosis. For patients who carry higher risk for an open revascularization, a hybrid approach including open retrograde thrombectomy and aorto-iliac stent graft placement can be considered as a safe alternative. Intraoperative adjunctive tools such as intravascular ultrasound could be paramount in sizing and planning of operative intervention.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.