
Abstract
Objectives
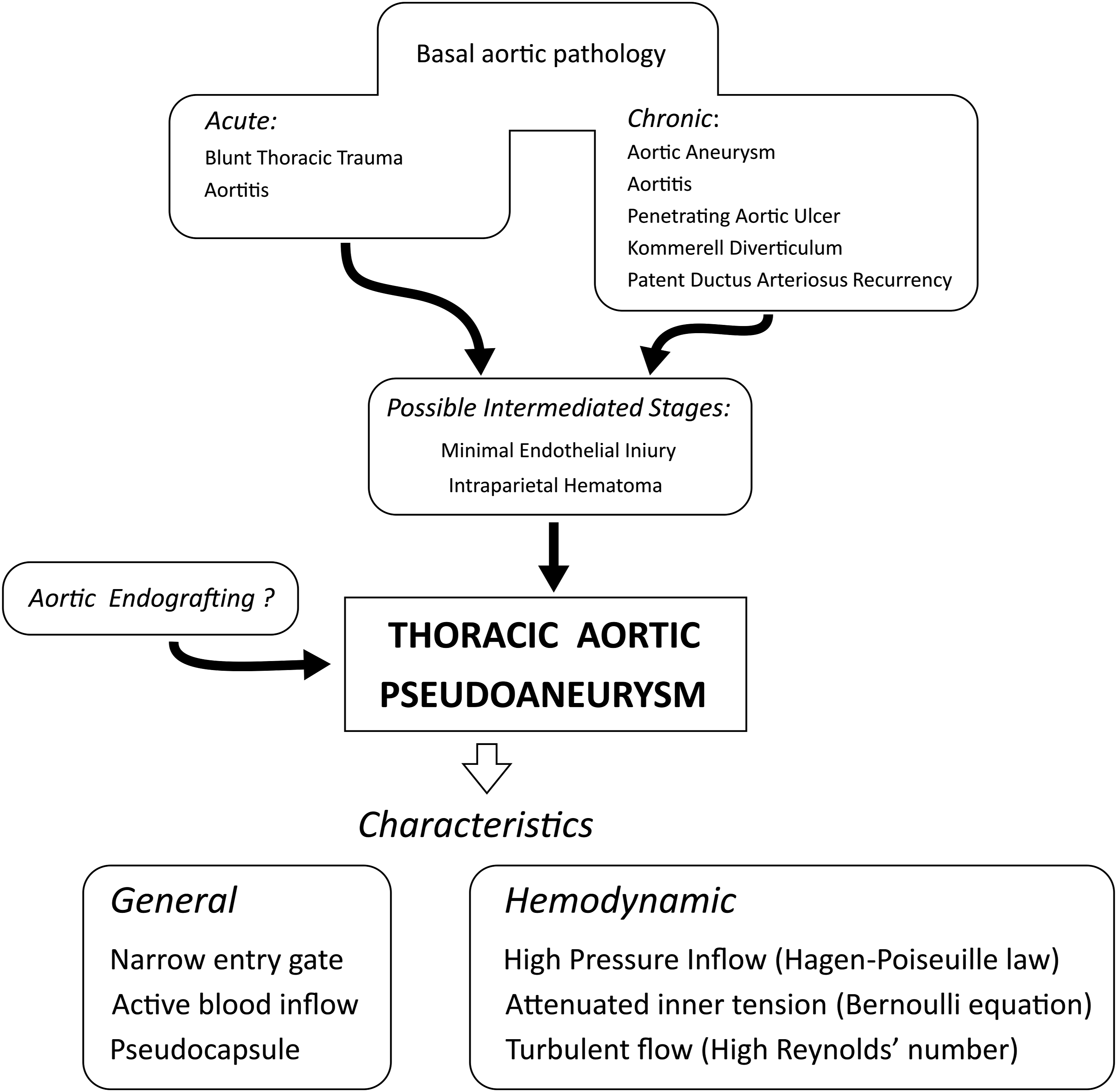
Our aim was to investigate pathophysiology of pseudoaneurysm of the thoracic aorta, an acute or chronic pathology, respectively, secondary to blunt thoracic trauma and aortitis, or complicating a deep penetrating aortic ulcer, intraparietal hematoma, aortic aneurysm, and even aortic graft, often with atherosclerosis as a common background.
Methods
Given the relative rarity of this disease, an “inductive” retrospective method made it possible to retrieve clinical, radiological, and histopathological elements, which were mutually compared and validated through a “deductive” process of reinterpretation.
Results
We have identified three main structural constituents of this disease: a cavity, a single blood entry port, communicating with the aortic lumen, and a pseudocapsule. It is often caused by a chronic degenerative pathology of the intima and medial layers of the aorta, typically involving elastic fibers and smooth muscle cells, with possible intermediate stages of deep aortic ulcer or intraparietal hematoma. Otherwise, the acute onset may be secondary to acute aortitis or aortic injury.
Conclusions
Today, thanks to the current angiographic tools represented by 3-D high resolution multidetector CT and MRI angiography, the diagnosis of thoracic aortic pseudoaneurysm is easier, as well as its surgical indications.
Keywords
Introduction
Today, the pseudoaneurysm of the thoracic aorta (TAP), or “false aneurysm,” can no longer be considered, despite its sporadic incidence, a “niche topic,” given the frequent predisposing pathologies, current sophisticated imaging, and the importance of a timely therapeutic choice, ranging from urgent treatment to careful follow-up. We consider its pathophysiological approach as an appropriate method of studying and learning. From the point of view of its architecture, a TAP has three main structural components: a cavity, typically spherical, an external fibrous pseudocapsule, and an entrance port located in the aortic wall. Its origin may be secondary to an acute aortic pathology, such as aortitis or aortic tear, or a pre-existing chronic disease, corresponding to a deep, penetrating aortic ulcer or an intraparietal hematoma, related to atherosclerosis.1–3
Patients’ recruitment and study methods
Our research was essentially observational and retrospective, including 20 cases observed between 2011 and 2021, all with a precise diagnosis supported by CT angiographic and histopathological data, retrieved from our archives and reviewed by two vascular radiologists and two pathologists. Five cases were post-traumatic, following blunt chest trauma, and 15 were correlated with atherosclerosis. All patients underwent successful surgical treatment, open in 3 and endovascular in 17. We solved the problem of the small number of cases, insufficient for a precise statistical analysis, by integrating two methods of study: an “inductive” one, consisting in the selection of the most relevant clinical, radiological, and histopathological elements, and a “deductive” one, consisting in their critical deepening and mutual correlation. This strategy made it possible to clarify several pathophysiological features of this disease.
Results
Our series of cases, consisting of 20 male patients aged between 22 and 70 years, provided sufficient elements to study a rare disease; the results enabled to obtain data about general pathology and hemodynamics of this disease.
TAP general pathology
In case of TAP development from a chronic or sub-chronic pathology, typically correlated with a deep penetrating aortic ulcer, intraparietal hematoma, or even aortic aneurysm, some specific factors can be further differentiated. In the aortic intima, a limited zone of dis-endothealization or rupture of an atherosclerotic plaque can create an intimal flap, which damages the aortic medial layer mechanically, through the strong kinetic energy of the inflowing blood stream, and chemically by contact with plasma components: together can promote the necroptosis of its smooth muscle cells and elastic fibers, and the lysis of its extracellular matrix substance, mainly through metalloproteinases. All this, in a vicious circle increases the release of inflammatory mediators, typically cytokines.4–6 In parallel, in the tunica adventitia, some clones of connective stem cells, thanks to their innate plasticity and sensitivity to the Fibroblast Growth Factor, translate into fibroblasts, generating a fibrous pseudocapsule (Figure 1).7–11 This process is favored by patent vasa vasorum and lymphatic vessels and immune-inflammatory cells released by the peri-aortic tertiary lymphatic structures, activated by atherosclerosis or recent deposits of hemosiderin.12,13 The preserved nerve fibers make the transmission of painful stimuli possible (Figure 2). Similarly an acute TAP, with an inflammatory origin, can have an equivalent development, with a greater inflammatory impact secondary to a contiguous aortitis or a septic embolus, which promote, respectively from outside or inside the aortic lumen, a more rapid cascade of events similar to that observed in the cases of a chronic pathology.14–18 Otherwise an acute TAP can follow a thoracic trauma, where an aortic parietal tear typically affects the aortic isthmus, which may luckily evolve through the intermediates stages of intraparietal and then peri-aortic hematoma. This event is favored by aortic walls elasticity, normal blood coagulability (Figure 3).
19
An equivalent chain of events can follow an aortic iatrogenic injury during an endovascular procedure. Differently, a full thickness aortic wound rapidly causes a severe hemorrhage, which rarely subsides or stops during the period of arterial hypotension. Two possible pathways leading to a thoracic aortic pseudoaneurysm. [1] Progressive evolution (A) a minimal aortic lesion corresponding to a small area of endothelial rupture, covered by a thrombus; (B) intraparietal hematoma, developed within the tunica media and protruding from the aortic contour; (C) a true aortic pseudoaneurysm surrounded by a pseudocapsule. [2] Acute evolution (D) aortic wall laceration, involving tunica intima and media and (E) acute intraparietal hematoma, altering the profile of the aortic wall. Histopathological features of a ruptured thoracic aorta pseudoaneurysm, and its components (hematoxylin-eosin staining). (A) Panoramic view of the adjacent aortic wall with tunica intima, extensively disrupted, media devoid of elastic fibers and smooth muscle cells, and adventitia infiltrated by a large hematoma (40×). (B) A segment of the pseudocapsule surrounding a thoracic aortic pseudoaneurysm with permeable vasa vasorum (100×). (C) A segment of ruptured/delaminated pseudocapsule with blood infiltrations (100×). (D) Peri-pseudocapsular lymph node with hemosiderin deposits and chronic lympho-macrophagic inflammatory reaction (100×). (E) A well preserved nervous fiber in the ruptured pseudocapsule (100×). Flowchart: from different aortic pathologies to thoracic aortic pseudoaneurysms.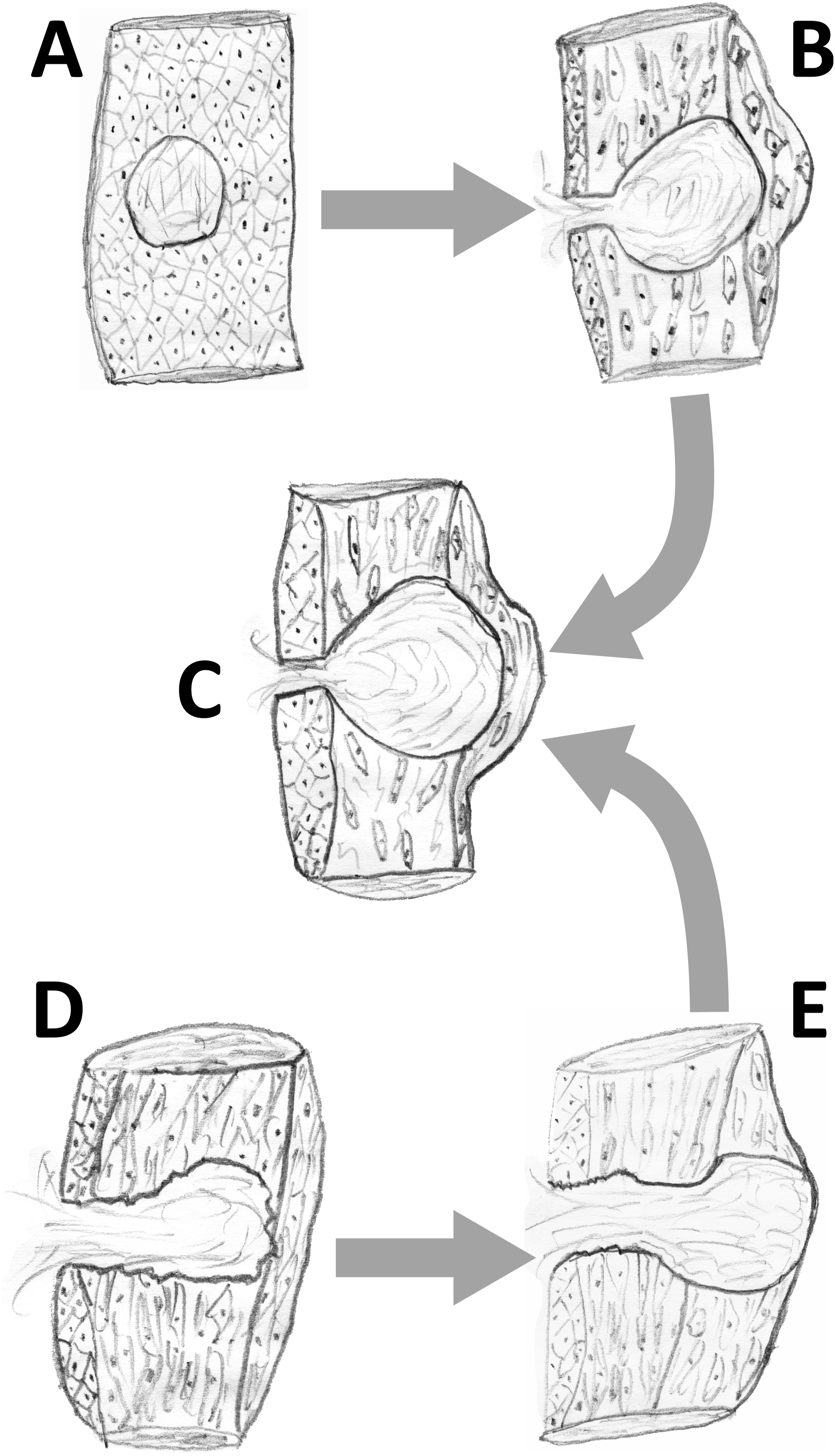

TAP rheological characteristics
From a hemodynamic point of view, a TAP can be regarded as an incompletely closed vascular structure, often saccular, with an entry port directly inscribed in the aortic wall and a “to-and-fro” waveform blood stream, namely with a systolic inflow and a diastolic outflow. This particular hemodynamics entails: (1) in the case of brady-arrhythmia, and subsequent recurrent periods of decreased blood inflow, the possible onset of an intraluminal thrombus, which mechanically and biologically increases the TAP inner tension and parietal weakness, in absence of any protective cushioning effect
20
; (2) because of Hagen-Poiseuille law, a decrease in the blood inflow total kinetic energy, inversely proportional to its entry port diameter, notwithstanding its paradoxically higher velocity, in agreement with the Bernoulli’s equation; and (3) in this inelastic semi-closed system, subdivision of the blood inflow vector in multiple sub-segments, colliding against the TAP wall, and promoting an increased walls stress and inner tension.21,22 This detailed cascade of rheological factors correlates with the chronic, but not the acute development of a TAP, unpredictable in its progression and unsuitable to a strict monitoring. In addition, the hemodynamics of this pathology cannot be considered the only factor of a TAP development, which also depends to a large extent on other pathobiological elements (Figure 4). It results that the TAP changes over time cannot be defined precisely, given the variable incidence of other pathobiological factors, and the clinical contraindication to radiological controls, excessively frequent. Computed tomography angiographic images of thoracic aorta pseudoaneurysm. (A) Saccular pseudoaneurysm originating in the inner part of the aortic arch, complicating a blunt thoracic trauma (arrow). (B) Within the descending thoracic aorta, large intimal flap (arrow) indicating an aortic psuedoaneurysm in progression. (C) Long hematoma within the aortic wall (arrows), with swelling of its outer countour, simulating an aortic dissection, but more appropriately indicating an evolving pseudoaneurysm with a great risk of rupture. (D) Large saccular pseudoaneurysm developing within the aortic arch (asterisk), result of a balance between the kinetic energy of its blood inflow, and the resistance of the pseudocapsule.
Discussion
From a clinical point of view, we consider it more interesting to correlate our results with pre-existing aortic pathology and previous surgery, and consequently delineate a possible evolution and management of TAP.
Aortic pre-existing pathologies
It cannot be ruled out that an aortic aneurysm, atherosclerosis correlated, could complicate with a TAP, through a self-limited process of fissuring, instead of its frank rupture, leading to a peri-aortic hematoma, subsequently enveloped in a pseudocapsule. Differently, it is unlike that an aortic dissection may evolve into a TAP, instead of a true rupture, given its different pathological background, consisting of a severe and degenerative process mainly affecting the tunica media, which becomes unable to withstand the strong kinetic power of the aortic blood flow, and reduces its repairing power. 23 Conversely, some congenital aortic pathologies may predispose to a TAP, typically a Kommerell’s diverticulum, when its intima and media tunica deteriorate.24,25 On the other hand, a newly generated TAP can mimic an aortic diverticulum, an embryological vestige of a ductus arteriosus, however prone to develop into a true aneurysm for its weaker histological structure. Similarly, a “giant cell” or a Takayasu arteritis can complicate firstly with a true aneurysm, and later with a TAP. 14
Post-surgical TAP
Any open aortic surgery may be followed by a TAP in the short/medium term through the direct mechanism of a self-limited post-operative hemorrhage. This can happen after resection of a ductus arteriosus or aortic isthmic coarctation.26–28 However, in the first case it has to be excluded a post-operative true aneurysm involving the aortic distal aortic stump, because of its texture inadequate to withstand the aortic pressure: it affects the entire aortic circumference, and do not consist of a more limited bulging. Differently a TAP can directly complicate any procedure of open aortic grafting. With regard to aortic endovascular surgery, some endoleaks, often similar to those classified as type II of the abdominal aorta, can be considered TAP-like structures, when a bulge develops outside the aortic wall, without any communicating entry port, and a blood inflow, usually from an intercostal artery. Pathophysiological links with a proper TAP are represented by metalloproteinases and other enzymes released from peri-prosthetic thrombi, fibrin filaments, and destructed zones of the intimal layer, with a lithic action affecting also the aneurysm adventitia.29–31
TAP evolution
According to Laplace’s principle, the evolution of TAP relies on an often precarious balance between the internal parietal tension and the resistance of the pseudocapsule. 32 This explains the three main possible clinical scenarios. First, a “silent” one, which corresponds to the incidental discovery of a mediastinal mass on chest X-ray or a bulging in the aortic wall on Doppler echocardiography. Second, a TAP progressive increase in size may compress adjacent mediastinal organs, typically esophagus, left recurrent laryngeal nerve, or the surrounding lung parenchyma, respectively causing dysphagia, dysphonia, or a zone of atelectasis. Third, a TAP can rupture, generating an unexpected and severe hemorrhage, with the clinical signs of hematemesis, hemoptysis, hemopericardium, or hemothorax, according to the different organs or structures involved. Moreover, a TAP located in the ascending aorta may further complicate with an aortic fistula communicating with a cardiac chamber, usually the right ventricle. 33 Predisposing factors consist of a TAP asymmetrical shape, which associated with a relatively small entry port easily makes turbulent the blood inflow, increasing the inner tension. In these cases, a 4-D MRI angiography can demonstrate areas of higher shear stress.34–36 The other prognostic element, represented by the mechanical resistance of the TAP pseudocapsule, difficultly can be assessed, except in the case of its evident low thickness or inflammatory state, today demonstrated at Positron emission/CT as a thickened area of contrast hyper-enhancement. 37 Today, this difficult problem expects to be faced by methods of radiomics and artificial intelligence.38–40
Possible treatment options
Instead of precise and validated guidelines, we can indicate only general principles of treatment, which will be further specified, on the base of larger multicentre studies. Today, deep penetrating aortic ulcer, or an intraparietal hematoma, mainly if rapidly expanding, can be considered predisposing factors to a TAP and other aortic pathologies, such as aneurysm and dissection, and require a surgical treatment, even urgent, and preferably endovascular, given the current consolidated experience gained in this technology.23,41–43 Differently, small intra-parietal and unchanged over time hematomas can be submitted to a strict and careful follow-up, before a surgical decision. In fact, the general guidelines followed in case of abdominal aortic aneurysms, fundamentally consisting in a diameter threshold of 5/5.5 cm and year increase ≥1 cm, cannot be directly translated to the TAPs treatment.37,44 This correlates with their histological architecture, which is properly non-vascular and lacks of smooth muscle cells elastic and other elastic-muscular components, and is provided of an external layer consisting of a connective capsule, with unpredictable resistance and possible latent inflammatory signs. All this considered, alerting signs of a possible rupture are a rapid volumetric increase, greater than 1 cm/year, a non-spheric feature, and a turbulent blood inflow. 45 In addition three clinical conditions have to be considered. Firstly, a TAP that originates from a pre-existing aneurysm is at greater risk of rupture, since its underlying pathology demonstrates a rapidly evolution. Secondly, in the cases of polytrauma, the priority in treatment is for the associated aortic lesion, given the imminent risk of sudden and unexpected circulatory destabilization.46–48 This policy may require a direct shift from a radiological diagnostic to an interventional procedure, often endovascular, which is today facilitated by the sophisticated technology of cone CT and hybrid operating room. Thirdly, a TAP, as a structure with a potential increase in volume, when proximal to an implantation site of a free coronary grafts, requires a careful follow-up, given the danger of its stretching, narrowing or partial occlusion, in which cases a prompt surgical treatment, usually open, becomes indicated. 49
Conclusion
TAP is a rare disease with different clinical, radiological, and histopathological features, which merit to be deepened in their pathophysiology. Vascular surgeons have to be learned about this disease, whose diagnosis can be promoted by a simple clinical suspicion, and possible severe complications may require a prompt surgical decision. In perspective, TAP, given its multifactorial origin and different clinical, histological, and pathophysiologic elements, may become a topic of further studies using methods of artificial intelligence and machine learning algorithms.38–40
Footnotes
Acknowledgments
The authors are grateful to Dr Massimo Borri for his active and valuable collaboration.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.