
Abstract
Objectives
This systematic review was performed to examine all published practice Guidelines and Consensus Statements (together: GCS) on heparin dosing and monitoring during non-cardiac arterial procedures (NCAP). The objective was to scrutinize the recommendations and advice outlined within these GCS documents and to evaluate the supporting evidence for these recommendations. Additionally, the use of the activated clotting time (ACT) and target ACT values were explored.
Methods
This systematic review was performed in accordance with the PRISMA Guidelines. Medline and Embase databases were searched to identify all GCSs in the English language on NCAP. The final literature search was performed in January 2023. This search was supplemented by searching websites of relevant professional vascular surgical organizations for GCSs. Titles and abstracts were assessed by two independent reviewers.
Results
Of 9716 titles identified, 27 GCSs met the predefined inclusion criteria: six GCSs regarding carotid intervention, seven regarding procedures for aneurysmal disease of the abdominal aorta and iliac arteries, 12 regarding interventions for acute and chronic peripheral arterial occlusive disease and two regarding open and endovascular interventions of thoraco-abdominal aortic aneurysms. Administration of heparin is advised for al NCAP. There was high variability concerning heparin dose: both standard dose as weight based dosing (30-150 IU/kg) was advised. Recommendations on repeated doses, ACT monitoring and heparin reversal using protamine also varied widely. In none of the GCSs, the type of the ACT measuring device or used cartridges were specified.
Conclusions
Large variability was found between the included GCSs with regard to the recommendations on heparin dose and target ACT values during NCAP. Advice and recommendations in GCSs were based on low-quality studies or without providing any reference at all. The described variability in recommendations emphasizes the need for large prospective (randomized) studies or the incorporation of data on heparin and the use of ACT monitoring into verified vascular surgery registries, to develop evidence-based, practical and uniform applicable recommendations.
Introduction
Throughout the years, outcomes of non-cardiac arterial procedures (NCAP) have improved significantly.1,2 Yet, perioperative and postoperative arterial thromboembolic complications (ATECs) are still common.3,4 Therefore, an adequate anticoagulation has to be reached during the full duration of interrupted blood flow to maximally prevent ATECs. On the other hand, reduced coagulation may cause increased blood loss, which subsequently can cause a higher risk of re-operation for bleeding, need for a blood transfusion and eventually death. Hence, the outcomes after NCAP depend on a delicate balance between coagulation and anticoagulation.
To prevent ATEC, unfractionated heparin (heparin) has been used for more than 70 years during non-cardiac arterial procedures (NCAP). 5 The use of heparin is embedded in daily practice by all vascular specialists worldwide and is one of the foundations of the treatment of arterial pathology. However, previous research showed that heparin inherently possesses a non-linear dose response and elimination curve, inducing an unpredictable effect in the individual patient.6,7 To monitor the periprocedural anticoagulant effect of heparin, the activated clotting time (ACT) can be measured, which can be performed as a point-of-care test. It is quite astonishing, but despite heparin is used for years during NCAP, a recent systematic review showed that there are no high quality comparative studies to guide practice concerning heparin dosing protocols and target ACT values during NCAP. 8
This lack of data emphasizes the need for good quality studies to provide clear, comprehensive and evidence-based recommendations on the use of heparin. Until these are available, clinical practice guidelines and/or clinical consensus statements (together: GCSs) on heparin dosing and target ACT values in NCAP might aid in the development of a local heparinization protocol. Therefore, the current systematic review was performed to examine all published GCSs on heparin dosing protocols and target ACT values during NCAP and evaluate the supporting evidence for these recommendations.
Methods
This systematic review was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 9 Importantly, the aim of this systematic review was not to evaluate the quality and/or methodology of GCS but to investigate possible recommendations and statements from guidelines on heparin and protamine dosing and anticoagulation level monitoring.
Search strategy
A systematic literature search was performed, with the help of a librarian, to identify GCSs published in Medline (1946-2023) and Embase (1966-2023) on NCAP. The last search was performed on 27 January 2023. This search was supplemented by searching websites of relevant professional vascular organizations for GCSs. Index terms for search strategy are depicted in supplemental digital content I.
Study selection
Two reviewers (L.R. and O.D.) independently screened all articles by title and abstract for eligibility. Duplicates were excluded during the screening process for title and abstract. Full-text analysis of the remaining articles was performed, and relevant GCSs were selected using predefined inclusion criteria. Disagreements were discussed and resolved between the two reviewers and, if necessary, two additional researchers (A.W. and V.J.).
Eligibility criteria
Eligibility criteria were predefined. GCSs were included if they: (1) were labelled as: guideline, or recommendation, or consensus, or position paper/stand; (2) provide a recommendation on heparin/protamine dosing or a target ACT; (3) involve non-cardiac arterial procedures (e.a carotid endarterectomy (CEA) or carotid stenting (CAS), open or endovascular treatment of aortic aneurysms or dissections, surgical bypass or endovascular treatment for peripheral occlusive disease; (4) used English as the reporting language and (5) in case of multiple versions, the most recently published GCS was included.
Data extraction
Two independent authors (L.R. and O.D.) extracted all the relevant features from each GCSs. The following data were extracted from all included GCSs: year of publication, guideline group, type of procedure, statements on the use of periprocedural heparin, recommendations/suggestions about the heparin dose, recommendations/suggestions on periprocedural heparin monitoring (using the ACT), measurement device used, recommendations/suggestions on target ACT values, recommendations/suggestions on the use and dosage of periprocedural protamine, classification of recommendations as found in the document (supplemental digital content II) and literature used to form the recommendation or statement. The name of the document was used: consensus document (CD), clinical practice guideline (CPG) or reporting standards (RS). Recommendations, statements or suggestions were extracted from full texts, including text, figures and tables.
Statistical analysis
No analyses were performed.
Results
Search and guideline characteristics
The search strategy in Medline and Embase resulted in a total of 14,311 publications. This number included several identical studies published in different international medical journals. Duplicates were excluded, and 9716 articles were screened and reviewed. Twenty-seven GCSs were included. Figure 1 shows the PRISMA flow chart.
9
Selected GCSs contained carotid pathology including endarterectomy and stenting (n = 6), open and endovascular repair of iliac and abdominal aortic aneurysms (n = 7), open and endovascular treatment of peripheral occlusive disease (n = 12) and open and endovascular repair of thoracic or thoraco-abdominal aortic aneurysms (n = 2). Search strategy and selection progress.
Carotid angioplasty, stenting and endarterectomy.

CD, consensus document; CPG, clinical practice guidelines; RS, reporting standards; CAS, carotid angioplasty and stenting; CEA, carotid endarterectomy; ASITN, American Society of Interventional and Therapeutic Neuroradiology; SIR, Society of Interventional Radiology; ACCF, American College of Cardiology Foundation; SVN, Society for Vascular Nursing; KSIN, Korean Society of Interventional Neuroradiology; ESVS, European Society for Vascular Surgery.
aHeparin is recommended; however, no statements were made about a specific dose regimen.
bHeparinization is generally allowed to taper physiologically rather than reverse using protamine sulphate. Alternatively, the femoral sheath may be removed immediately after the procedure without the need for heparin reversal using percutaneous closure devices.
cAfter the start of bolus based on the body weight, a maintenance dose of 1000-unit/hour is administered with control of ACT between 250 and 300 s.
Open and endovascular repair of iliac and abdominal aortic aneurysms.

CPG, clinical practice guidelines; CD, consensus document; EVAR, endovascular abdominal aneurysm repair; IIAA, isolated iliac artery aneurysm; OSR, open surgical repair; SIR, Society of Interventional Radiology; CIRSE, Cardiovascular and Interventional Radiological Society of Europe; ESC, European Society of Cardiology; SVS, Society for Vascular Surgery; ESVS, European Society for Vascular Surgery; SVN, Society for Vascular Nursing; SICVE, Italian Society of Vascular and Endovascular Surgery.
aHeparin is recommended; however, no statements were made about a specific dose regimen.
bACT measurements are recommended; however, no statements were made about a target ACT value.
cThe administration of a weight-optimized dose of heparin is suggested.
Open and endovascular treatment of peripheral arterial occlusive disease.
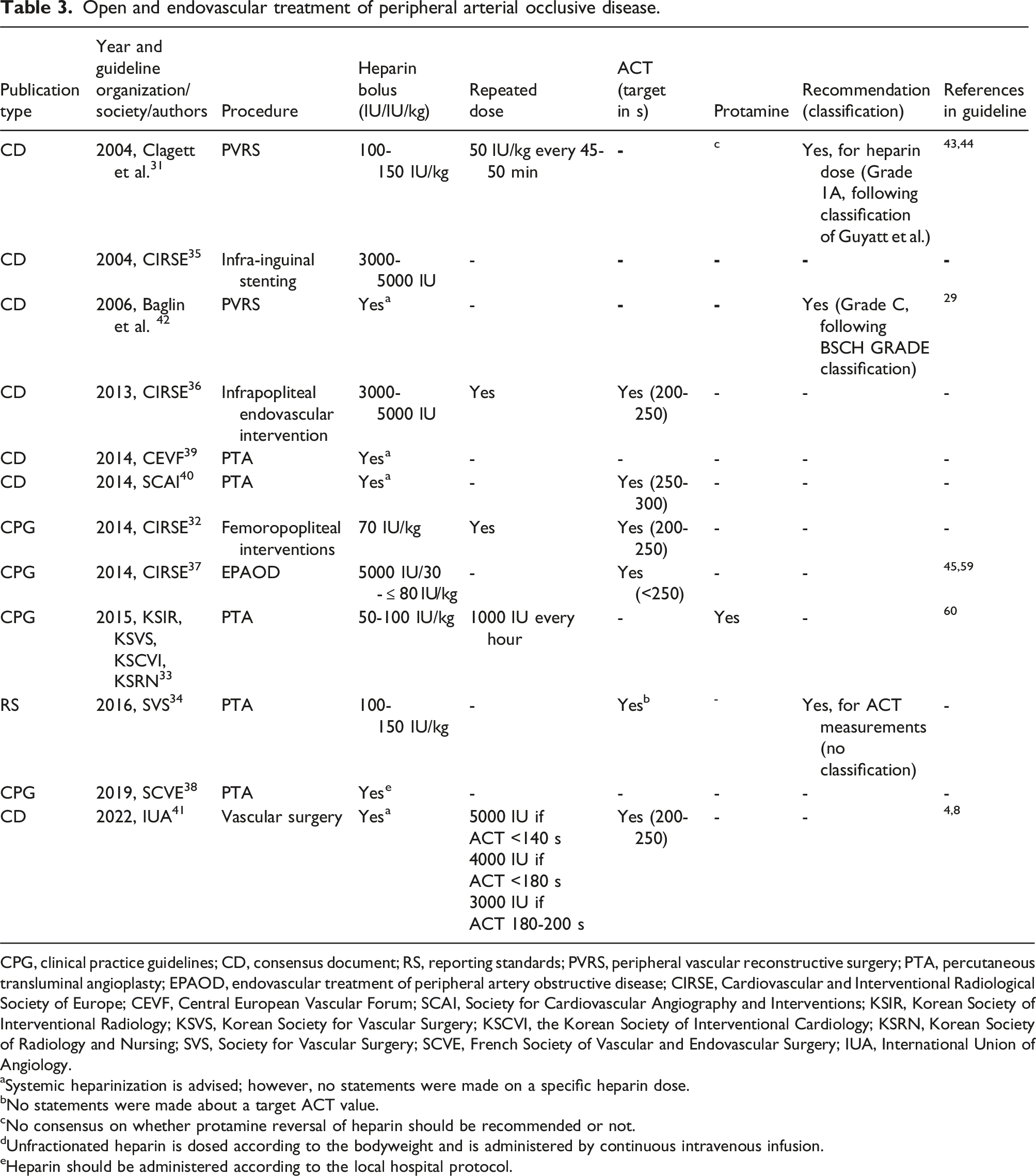
CPG, clinical practice guidelines; CD, consensus document; RS, reporting standards; PVRS, peripheral vascular reconstructive surgery; PTA, percutaneous transluminal angioplasty; EPAOD, endovascular treatment of peripheral artery obstructive disease; CIRSE, Cardiovascular and Interventional Radiological Society of Europe; CEVF, Central European Vascular Forum; SCAI, Society for Cardiovascular Angiography and Interventions; KSIR, Korean Society of Interventional Radiology; KSVS, Korean Society for Vascular Surgery; KSCVI, the Korean Society of Interventional Cardiology; KSRN, Korean Society of Radiology and Nursing; SVS, Society for Vascular Surgery; SCVE, French Society of Vascular and Endovascular Surgery; IUA, International Union of Angiology.
aSystemic heparinization is advised; however, no statements were made on a specific heparin dose.
bNo statements were made about a target ACT value.
cNo consensus on whether protamine reversal of heparin should be recommended or not.
dUnfractionated heparin is dosed according to the bodyweight and is administered by continuous intravenous infusion.
eHeparin should be administered according to the local hospital protocol.
Open and endovascular repair of thoracic or thoraco-abdominal aortic aneurysm.
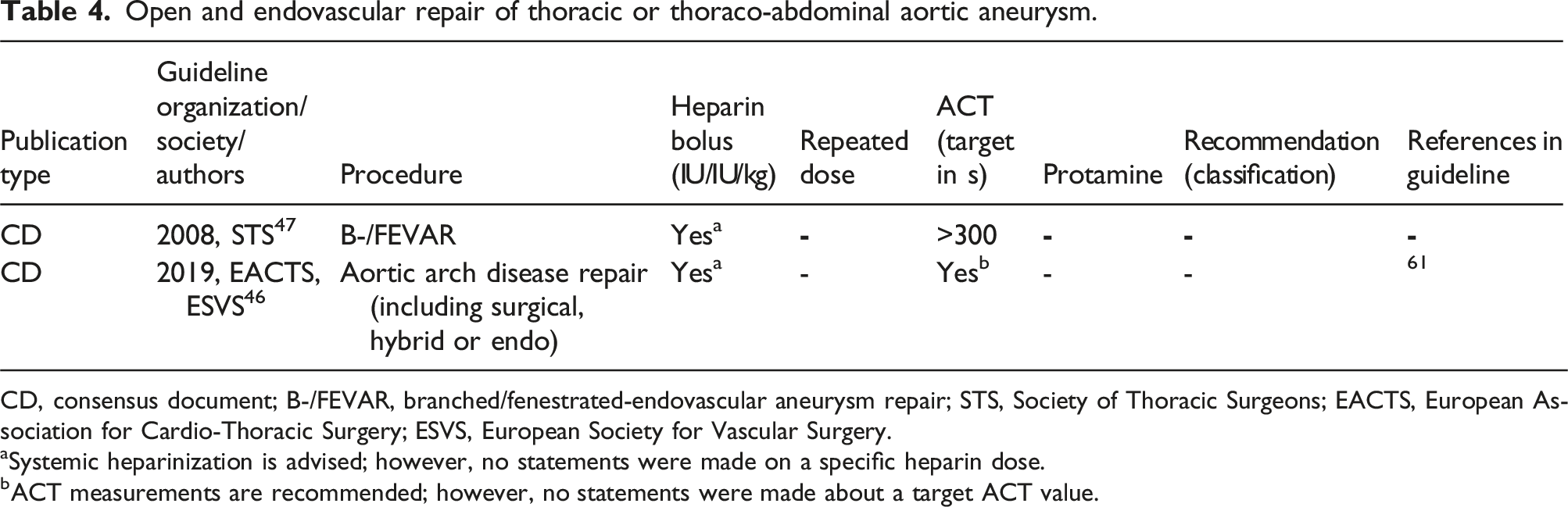
CD, consensus document; B-/FEVAR, branched/fenestrated-endovascular aneurysm repair; STS, Society of Thoracic Surgeons; EACTS, European Association for Cardio-Thoracic Surgery; ESVS, European Society for Vascular Surgery.
aSystemic heparinization is advised; however, no statements were made on a specific heparin dose.
bACT measurements are recommended; however, no statements were made about a target ACT value.
Heparin specification and ACT measurement device
In none of the GCSs, the type of the ACT measuring device or used cartridges were specified. In addition, the manufacturer of heparin was not specified in any of the included GCSs.
Carotid
Heparin dose protocol
Six GCSs on carotid intervention could be included, of which four on CAS, one on CEA and one on CAS and CEA (Table 1). The GCSs were published between 2004 and 2023. In one GCS on CAS and in one on CEA, a bodyweight-based heparin protocol of 50-100 IU/kg was recommended.10,11 A bolus of 2000-4000 IU with in addition a continuous infusion of 1000 IU/hour was advised in one CAS GCS. 12 The other three GCSs did not provide a recommendation on heparin dosing protocol.13–15
Target ACT
Three GCSs provided a target ACT for CAS of 250-300 s10,12,13 One GCS recommended a target ACT of 200-250 s for CEA. 11 The remaining two GCS did not specify a target ACT.14,15
Protamine
Three GCSs contained a recommendation on the use of protamine.11,14,15 For CAS, one stated that heparin should not be reversed. 14 In one GCS on CEA, it was stated that protamine should be administered at surgeon’s discretion, depending on patient comorbidities. 11 One GCS on CAS and CEA recommended that protamine reversal of heparin should be considered. 15 The other three GCS did not include any recommendations regarding protamine dosing.10,12,13
Recommendation classification and references in GCS
Out of six GCSs reviewed for CAS and CEA, three provided a recommendation. Of these three recommendations, the level of evidence was classified for two. One recommendation was classified as Class II following the SVN classification, and the other as Class IIA level B following ESVS classification (supplemental digital content II).
In four of the GCSs, one or more references were included to support the provided advice or recommendation. Reference was made to a retrospective study involving 605 CAS patients, which reported an optimal target ACT value of 250-299 s during CAS. 16 Additionally, GCSs referred to two registry studies, one observational study and one meta-analysis on protamine, which showed that the use of protamine could be considered.17–20 All other references did not refer to articles containing evidence on heparin dosing, heparin monitoring using ACT or the use of protamine.
Iliac and abdominal aortic aneurysms
Heparin dose protocol
In total, seven GCSs were included regarding interventions in the iliac arteries and the abdominal aorta for aneurysmal disease (Table 2). The selected GCSs were published between 2010 and 2022. One GCS on the interventional management of isolated iliac artery aneurysms advised a standardized heparin bolus of 3000-5000 IU. 21 Four GCSs on endovascular aneurysm repair (EVAR) advised the use of heparin, of which two recommended a weight based heparin dose between 50 and 100 IU/kg.22,23 A heparin dose between 50 and 100 IU/kg was also recommended in two GCSs on open surgical repair (OSR).22,23
Target ACT
In two GCSs, a recommendation was made regarding the target ACT.22,24 One GCS on OSR and EVAR advised monitoring the effect of heparin using ACT without mentioning a target ACT. One GCS on EVAR recommended a target ACT of ≥300 s. 22 The remaining five GCS did not provide a target ACT.21,25–28
Protamine
The use of protamine was mentioned in one GCS on OSR and EVAR. It was stated that the use of protamine should be considered. 23 The other six guidelines did not provide any recommendation regarding protamine.
Recommendation classification and references in GCS
Out of the seven GCSs on OSR and EVAR, three provided a recommendation, and one of them classified the level of evidence: Class 1 level C following ESVS classification (supplemental digital content II). Two provided one or more references. Reference was made to a prospective study from 1996, which showed a lower incidence of myocardial infarctions in patients who received heparin during elective open AAA surgery. 29 No optimal heparin dosing protocol was mentioned in this article. Another article which was referred to was a systematic review that advised the use of heparin based on the aforementioned prospective study from 1996. 30 The remaining references mentioned in the GCSs did not refer to articles containing evidence on heparin dosing, monitoring using ACT or the use of protamine.
Peripheral arterial occlusive disease (PAD)
Heparin dose protocol
Twelve GCSs concerning interventions for acute and chronic peripheral arterial occlusive disease, published between 2004 and 2022, were included (Table 3). Periprocedural use of heparin was advised in all GCSs, with bodyweight-based dosing (30-150 IU/kg) in four GCSs and a fixed bolus of heparin (3000-5000 IU) in three GCSs.31–37 One GCS mentioned that heparin should be administered according to the local hospital protocol. 38 An initial heparin dose of 100-150 IU/kg, and additional heparin doses of 50 IU/kg, every 45-50 min until the cross clamps were removed, was recommended by one GCS. 31 In another, an additional bolus of 1000 IU every hour was advised after administration of an initial heparin dose of 50-100 IU/kg. 33 The remaining two GCSs did not provide an advice on heparin dosing.39,40
Target ACT
In six of the 12 GCSs, it was advised to monitor the effect of heparin using the ACT. Three GCSs advised a target ACT of 200-250 s, one a target ACT <250 s and one a target ACT of 250-300 s.32,36,37,40,41 One GCS provided a protocol for additional heparin doses based on ACT values measured. 41
The other six GCSs did not specify a target ACT.
Protamine
In one GCS, the use of protamine was advised without mentioning the dose of protamine to be administered. 33 Another GCS described that reversal or non-reversal of heparin using protamine has not been established. 31 No advice on protamine administration was not provided in the remaining GCSs.
Recommendation classification and references in GCS
Out of 11 GCSs on PAD, three provided a recommendation, and two of them had classified the level of evidence.31,42 One recommendation was classified as Class 1A following the classification of Guyatt et al., and the other as Grade C following BSCH Grade classification (supplemental digital content II). Five GCSs cited references to support their advice or recommendations. Reference was made to two randomized trials from 1995 to 1997 on the use of protamine during PAD procedures.43,44 In addition, reference was made to a registry study on PAD procedures that showed a lower incidence of bleeding complications in patients with an periprocedural ACT <250 s. 45 Another study demonstrated the lowest incidence of ATEC in patients with an ACT between 200 and 250 s, treated for all types of NCAP. 4 Lastly, reference was made to a systematic review, which concluded that there is no concluding evidence available on optimal target ACT during NCAP. 8 Other references mentioned in the GCSs did not refer to articles containing evidence on heparin dosing, monitoring using ACT or the use of protamine during PAD.
Open and endovascular repair of thoracic or thoraco-abdominal aortic aneurysm
Heparin dose protocol
In total, two GCSs were included regarding OSR and EVAR for thoracic or thoraco-abdominal aortic aneurysms. The selected GCSs were published in 2008 and 2019. Systemic heparinization was advised in both; however, no statements were made on a specific heparin dose (Table 4). 46
Target ACT
In one GCS, a target ACT of >300 s was recommended. 47 The other GCS stated that the ACT was indicated as a minimum requirement during surgical, hybrid or endovascular aortic arch repair. It was mentioned that the ACT is not highly specific for heparin activity, and that the use of quantitative monitoring of circulating heparin concentrations should be considered, rather than simple serial ACT measurement during arch surgery with prolonged cardiopulmonary bypass and hypothermic circulatory arrest. 46
Protamine
None of the GCSs included the use of protamine to reverse the effect of heparin.
Recommendation classification and references in GCS
None of the GCSs provided a recommendation. One referred to a guideline on cardiac surgery, which contains advice based solely on cardiac surgical research.
Discussion
This systematic review provides a comprehensive overview of advice and recommendations from international GCSs on heparin dosing and monitoring during NCAP. Large variability was found in advice and recommendations regarding heparin dosing protocols and possible target ACT values. Since only limited research has been conducted on heparin dosing and target ACTs during NCAP, advice and recommendations in GCSs were based on low-quality studies or without providing any reference at all.
All included GCSs recommended systematic heparinization, 52% (14/27) provided a specific initial heparin dose or dose regimen and 41% (11/27) mentioned target ACT values.
Several findings in this systematic review are remarkable at least. First of all, some GCSs for PAD suggested a single heparin dose of only 3000 IU, while others suggested a heparin bolus of 100-150 IU/kg.31,34–36 Interestingly, sometimes the same heparin dose was advised to reach different ACT values; for example, the SVN GCS on CEA advices 70-100 IU/kg to reach an ACT of 200-250 s, while 50-100 IU/kg is advised to reach an ACT of 250-300 s in the SVN CAS GCS.
In addition, some GCSs advised an initial heparin dose of 50-100 IU/kg, which is a wide range, as twice as much heparin is administered at 100 IU/kg compared to 50 IU/kg. It is possible that GCSs are providing a wide range to accommodate for individual patient differences, such as sex, as previous research showed that females have higher ACT values after a same dose of heparin compared to males. 48
In other fields, there is more overlap. When a target ACT is mentioned, it is foremost 200-250 s or 250-300 s. Still, this is a wide range. It could very well be that the optimal ACT with the lowest ATEC and bleeding complications is within a much smaller range. However, the absence of clear evidence supporting a specific heparin dose may have contributed to the wide range provided.
A relatively high target ACT of >300 s was recommended in the SVS guideline for EVAR. 22 It is possible that this target ACT was adapted from cardiac surgery where higher ACT values are commonly targeted; however, no reference was provided to support this, possibly harmful, recommendation. In fact, previous research showed that bleeding complications were significantly more present in patients with ACT values >250 s. 45
Since heparin has a short half-life time, timely procedures may necessitate additional heparin administration to ensure sufficient anticoagulation. 49 This has been recently shown in a study in which a significant number of patients had insufficient anticoagulation just 30 min after the initial heparin dose. 48 In several included GCS for open and endovascular treatment of peripheral arterial occlusive disease, administration of repeated heparin doses with varying dosages was mentioned. However, in the GCS for other (lengthy) procedures as EVAR or OSR, no advice was provided regarding the administration of additional heparin doses.
Remarkably, none of the included GCSs mentioned the type of ACT measurement device or other details of ACT measurements, while previous research has shown that ACT measurements vary substantially depending on the measurement devices and cartridges used.50–54 Consequently, it is ineffective and possibly dangerous to present universal target ACT values.
Lastly, all recommendations from the included GCSs were integrated in this systematic review without modification, preserving the original wording used in the GCSs, even if they are incomplete, lacking in evidence-based support or if they do not align with our own perspectives. The limited available evidence prohibits the provision of clear recommendations regarding an optimal dosing protocol for heparin and corresponding target ACT in this systematic review.
A strength of this systematic review is that it provides a comprehensive overview of GCSs on heparin dosing and monitoring during NCAP. The review searched for all available GCSs on this topic, ensuring a complete representation of current recommendations worldwide. In addition, a comprehensive assessment was carried out on all the included GCSs, to confirm the presence of references that substantiate their recommendations. Another strength is that all GCSs were independently screened for eligibility by two reviewers.
Besides these strengths, there are several limitations that could have biased the findings. GCSs were only included if their full text was available in English, which is likely to have resulted in a bias in the regions included, and impacted the number of guidelines included in this review. Another limitation is that no instrument could be used to assess the methodological quality and the scientific validity of the GCSs. This was beyond the scope defined for this review. Nonetheless, this systematic review emphasizes that sound scientific evidence is needed to provide clear recommendations in GCSs on an optimal dosing protocol for heparin and corresponding target ACT.
Conclusions
Large variability was found between the included international GCSs with regard to the recommendations on heparin dosing and target ACT values during NCAP. No clear evidence, based on high quality comparative studies, is present for any heparin regimen or target ACT values mentioned in the recommendations in GCSs on NCAP. The identified variability and lack of literature on one of the foundations of vascular interventions (heparin use) may even be harmful for individual patient safety as it may increase thromboembolic and bleeding complications when too low or too high levels of anticoagulation are caused by insufficient heparin dosing. This emphasizes the urgent need for large prospective (randomized) studies, or the incorporation of data on heparin and the use of ACT monitoring into verified vascular surgery registries, to develop evidence-based, practical and uniform applicable recommendations.
Supplemental Material
Supplemental Material - Systematic review of clinical guidelines and consensus statements concerning heparin and protamine dosing and monitoring of anticoagulation levels for non-cardiac arterial procedures
Supplemental Material for Systematic review of clinical guidelines and consensus statements concerning heparin and protamine dosing and monitoring of anticoagulation levels for non-cardiac arterial procedures by Liliane C Roosendaal, Orkun Doganer, Arno M Wiersema, Jan D Blankensteijn and Vincent Jongkind in Vascular.
Supplemental Material
Supplemental Material - Systematic review of clinical guidelines and consensus statements concerning heparin and protamine dosing and monitoring of anticoagulation levels for non-cardiac arterial procedures
Supplemental Material for Systematic review of clinical guidelines and consensus statements concerning heparin and protamine dosing and monitoring of anticoagulation levels for non-cardiac arterial procedures by Liliane C Roosendaal, Orkun Doganer, Arno M Wiersema, Jan D Blankensteijn and Vincent Jongkind in Vascular.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.