
Abstract
Background
Extracranial internal carotid artery aneurysms are rare entities that arise within the carotid triangle. Although rare, they are clinically significant due to the risk of neurologic thromboembolic events, compression of cranial nerves and vasculature, rupture, and ischemia.
Objective
Surgery is the gold-standard treatment for symptomatic patients of all ages with extracranial internal carotid artery aneurysm.
Method
A 26-year-old female patient was admitted to our institution with complaints of left auricular pain, hoarseness, and uncontrollable hypertension. She had a pulsatile mass located at the left cervical region. After diagnosing the extracranial internal carotid artery aneurysm, it was decided that surgery was necessary to relieve the patient’s discomfort and prevent possible complications from the aneurysm in the left carotid artery.
Result
In the operation, the aneurysmatic segment was resected and sent for histopathological evaluation. Saphenous vein graft was interposed as end to end anastomosis to the proximal and distal healthy segments of the internal carotid artery.
Conclusion
This case report highlights the surgical management of a 26-year-old female patient who presented to our institution with complaints of left auricular pain, hoarseness, uncontrolled hypertension, and a pulsatile mass localized at the left cervical region and diagnosed extracranial internal carotid artery aneurysm.
Introduction
Extracranial internal carotid artery aneurysms are rare entities, comprising less than <1% of all arterial aneurysms. 1 They arise within the carotid triangle, with localization to the carotid bifurcation or distal portion of the internal carotid artery. 2 Most cases of extracranial internal carotid artery aneurysms are asymptomatic and are diagnosed incidentally. However, when enlarged, they may present as a pulsatile mass with symptoms of dysphagia, hoarseness, auricular pain, compression-related cranial nerve deficits, rupture, and hemorrhage and most importantly as cerebral ischemia, transient ischemic attacks, and strokes due to thromboembolism. 3
The natural course of extracranial internal carotid artery aneurysms is poor, with a risk of stroke in up to 50% of patients. 4 Although clinical treatment and follow-up of asymptomatic extracranial internal carotid artery aneurysms have been suggested, the mainstay of treatment is surgical intervention due to the risk of adverse events. The current gold-standard approach is surgical management performed with resection of the aneurysm followed by arterial reconstruction.5,6
In this report, we present the surgical management of a 26-year-old female patient with the diagnosis of extracranial internal carotid artery aneurysm.
Case report
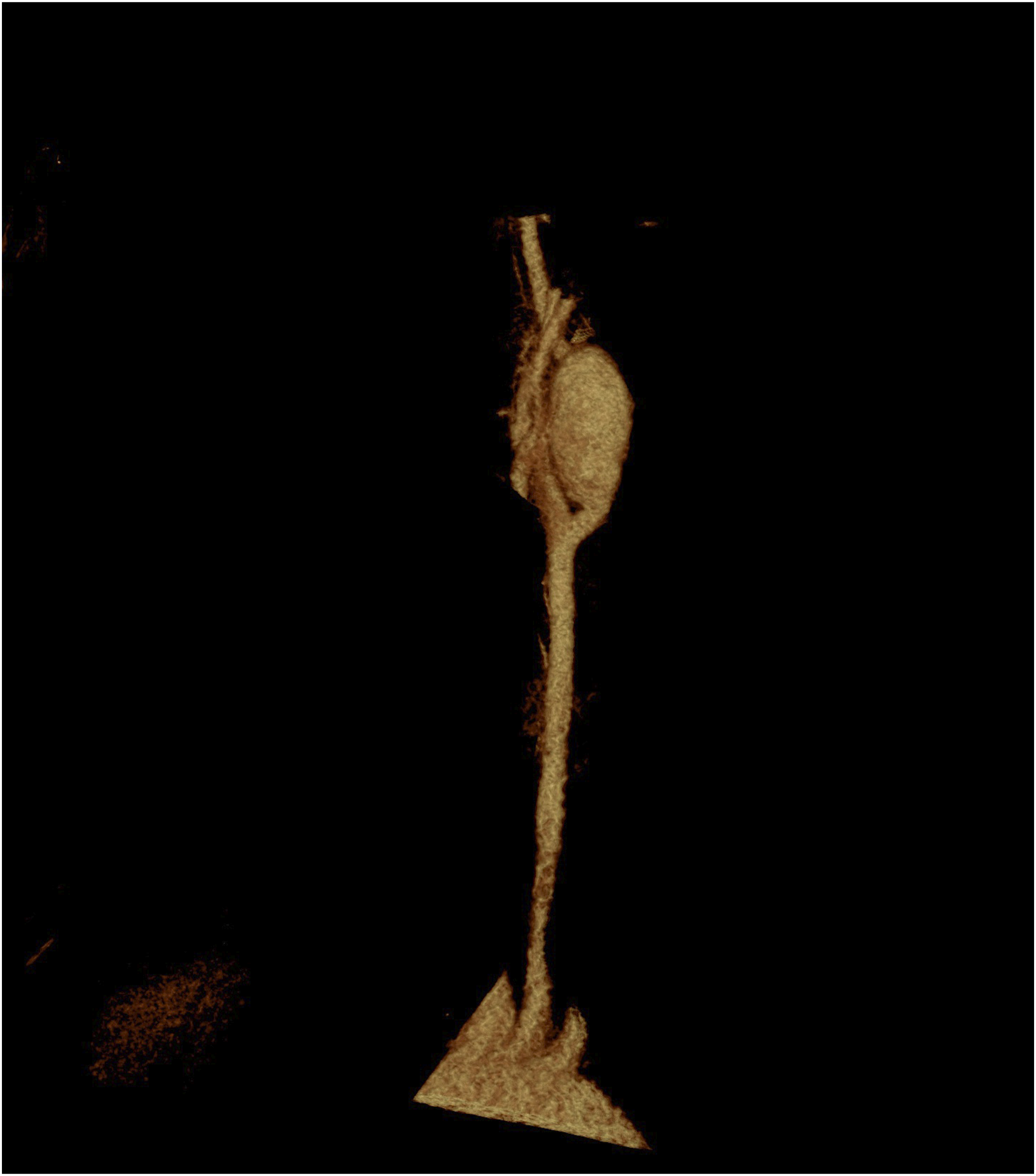
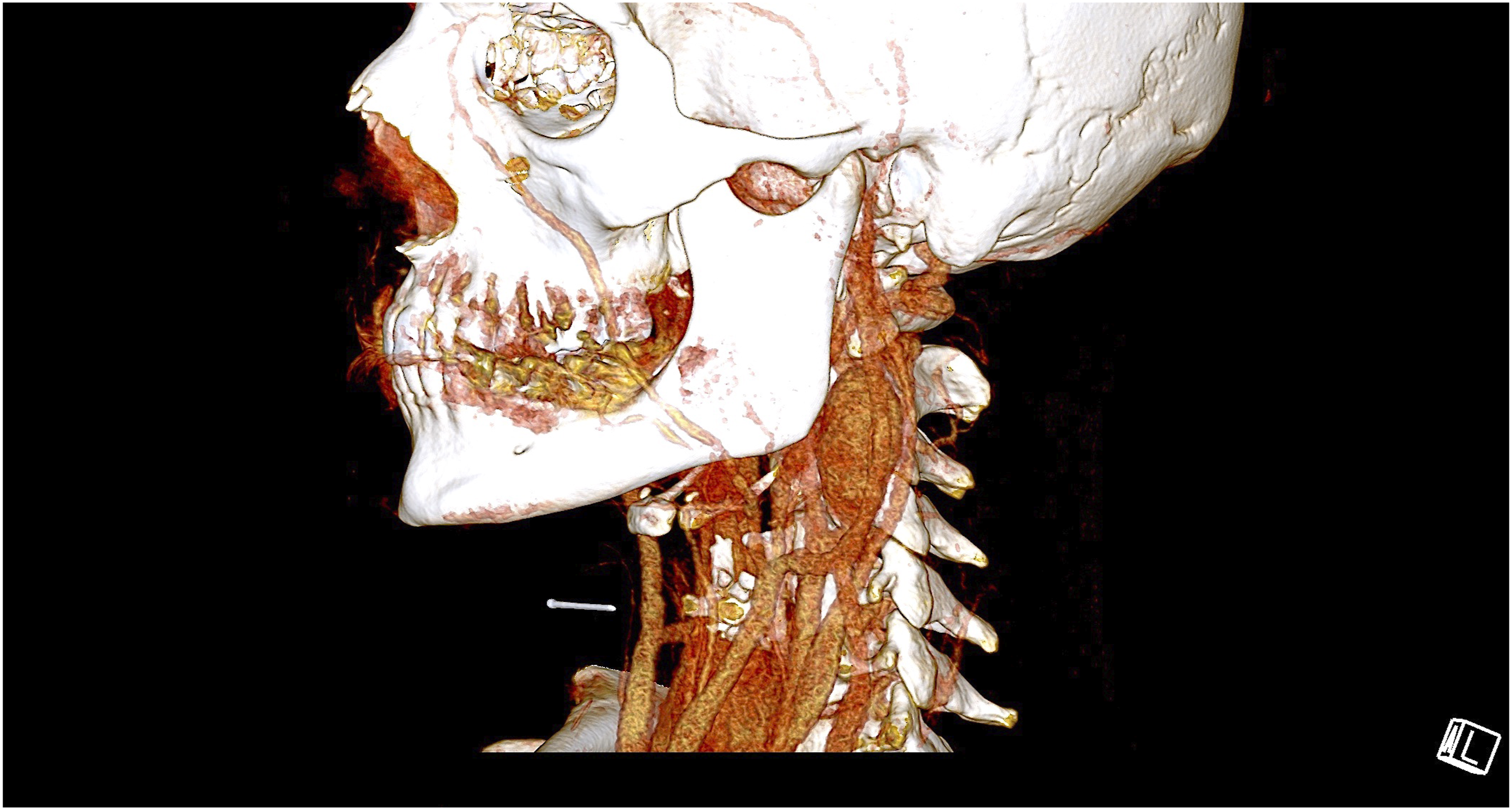
A 26-year-old female patient was admitted to our institution with complaints of left auricular pain, hoarseness, and uncontrollable hypertension. She had a pulsatile mass located at the left cervical region. Doppler ultrasonography indicated extracranial carotid artery aneurysm which was confirmed with computerized tomography angiography revealing a fusiform internal carotid artery aneurysm within the carotid triangle originating proximal to the carotid artery bifurcation and extending distally with a maximum diameter of 1.76 cm (Figures 1–3). Preoperative computed tomography angiography. Preoperative computed tomography angiography. Preoperative computed tomography angiography.
Upon diagnosing the pathology, the need for surgical intervention was determined to alleviate the patient’s discomfort and mitigate potential complications related to the left extracranial internal carotid artery aneurysm. The patient was provided with comprehensive information regarding the risks and benefits of the treatment, and following consent, the surgery was scheduled.
Surgical management
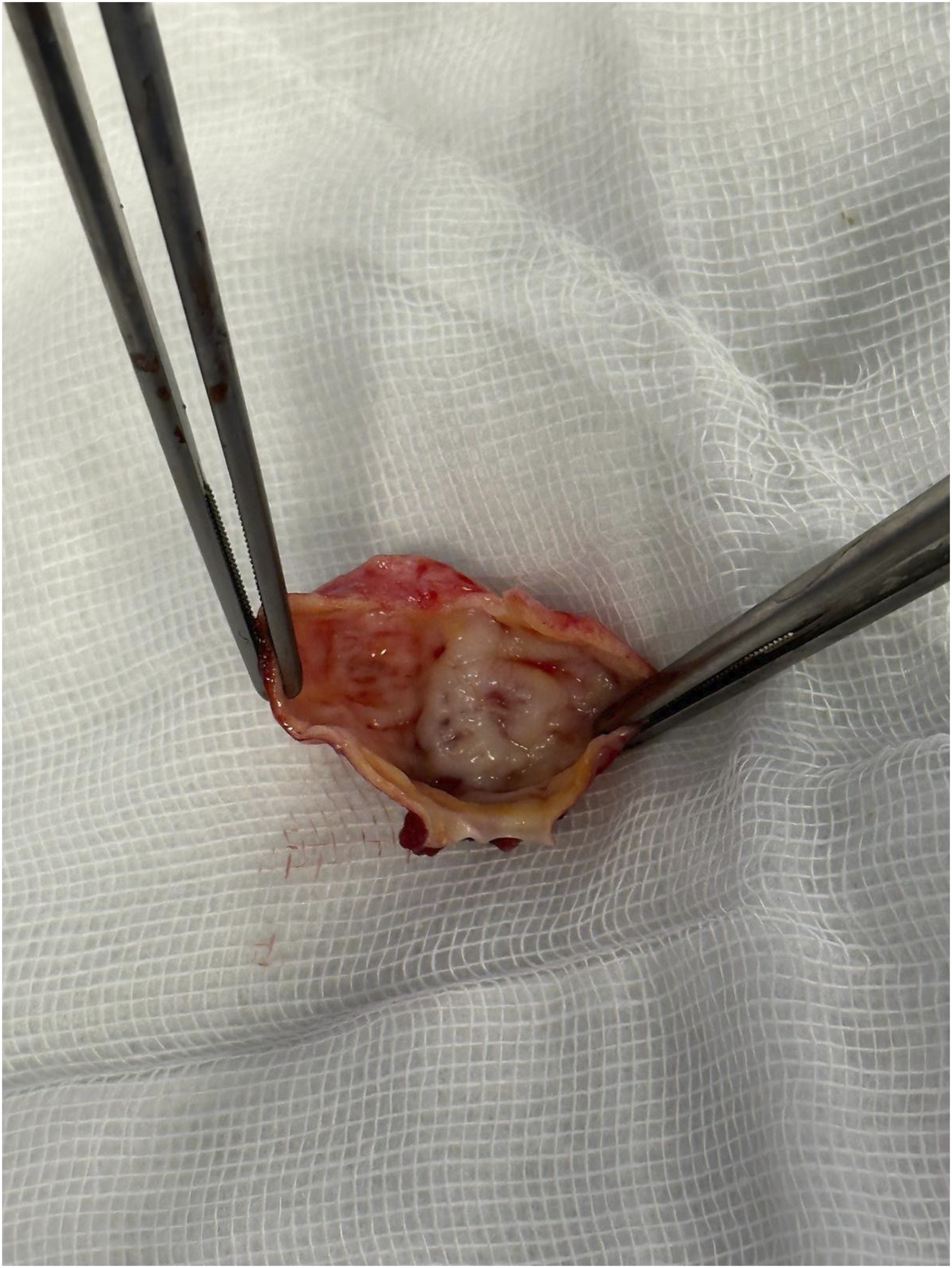
Under general anesthesia, the operation was initiated with a linear incision to the left cervical region anterior to the sternocleidomastoid muscle. The left common carotid, internal carotid, and external carotid arteries and the aneurysmatic segment of the internal carotid artery were explored. The left internal carotid artery was extremely aneurysmatic beginning about 0.5 cm from the point of bifurcation extending distally for a length of about 3.5 cm and reaching a maximum diameter of about 2 cm (Figures 4 and 5, Supplementary 1). The right saphenous vein graft was harvested from the proximal right lower extremity for autologous grafting. The carotid bulbus was locally anesthetized. Following heparin administration, the proximal and distal disease-free segments of the internal carotid artery were clamped. The external carotid artery was not needed to be clamped, and the flow through external carotid artery was not interrupted. The aneurysmatic segment was resected and sent for histopathological evaluation. Saphenous vein graft was interposed as end to end anastomosis to the proximal and distal healthy segments of the internal carotid artery (Figure 6, Supplementary 2). Following careful de-aeration, the clamps were released and operation was finalized. Postoperative course was uneventful, and the patient was discharged on the 3rd postoperative day without complications. Perioperative image of the carotid artery aneurysm. The inner wall of the carotid artery aneurysm. The saphenous vein graft was interposed as end to end anastomosis to the internal carotid artery.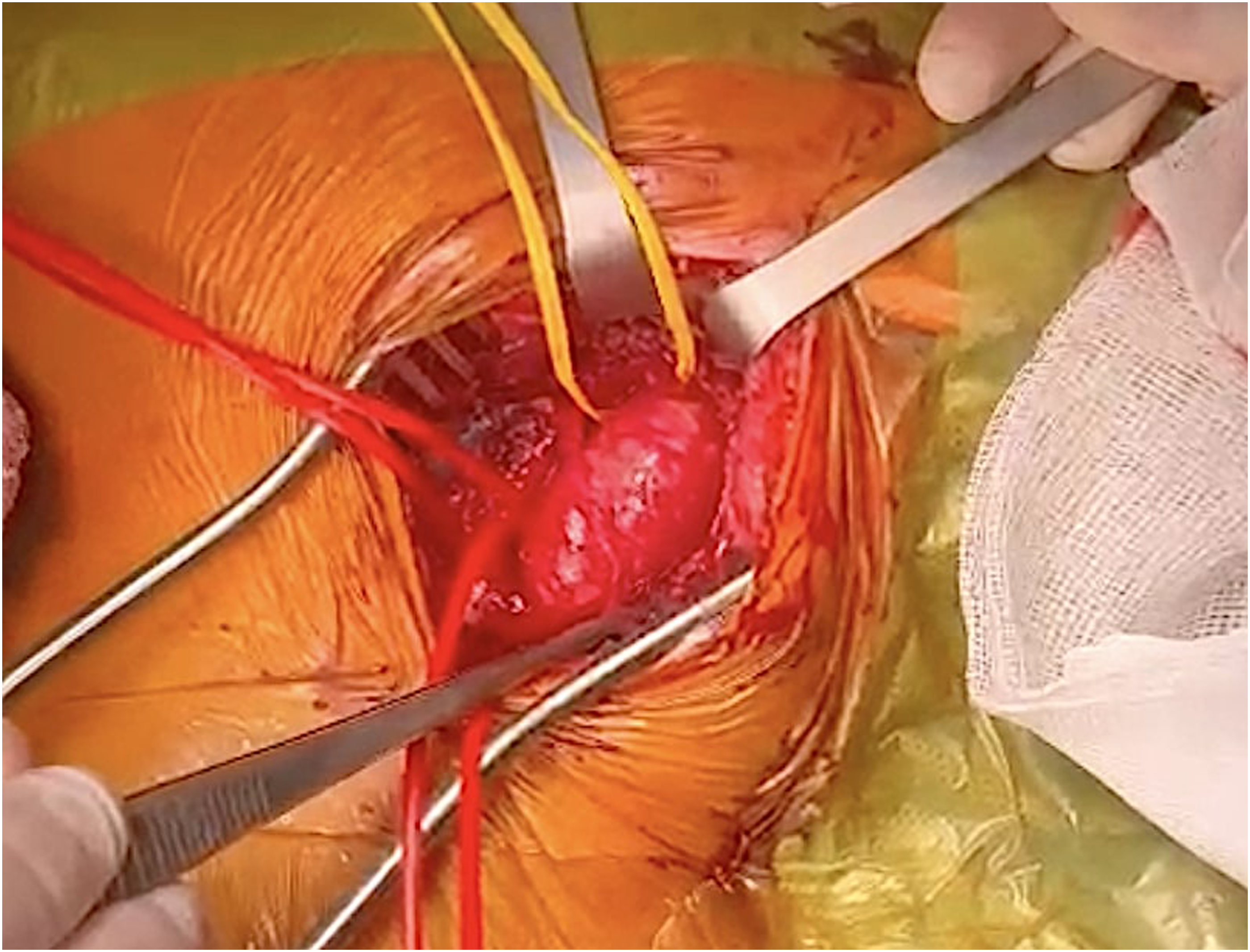

Pathological examination
The histopathologic examination of the excised material was completely sampled with parallel sections and full-thickness. On hematoxylin and eosin–stained sections, the endothelium was identified. The lesion wall under the endothelium had a partially degenerate appearance. Loss and atrophy were observed in the muscular layer, varying from area to area. Regular elastic lamina was not identified. Active or chronic inflammation (lymphocyte and macrophage) was not observed. Histological changes related to atherosclerosis (lipid deposits, cholesterol clefts, foamy histiocytes, and calcification) were not detected (Figure 7). All were suggestive of a degenerative disease. Patient is currently back to daily activities and followed asymptomatic for more than 1 year. Pathological examination of carotid artery aneurysm. (a) Under the surface endothelial layer, aneurysm wall with degeneration, partially loss of the muscle layer, which is different from the normal vessel structure (HEx100). (b) Vasculitis or atherosclerotic changes were not observed in the thinned aneurysm wall and surrounding vessels (HEx200). (c) Disorganized and fragmented elastic fibers (EVGx100). (d) Muscle bundles with variable thickness from area to area (Masson’s trichrome ×100).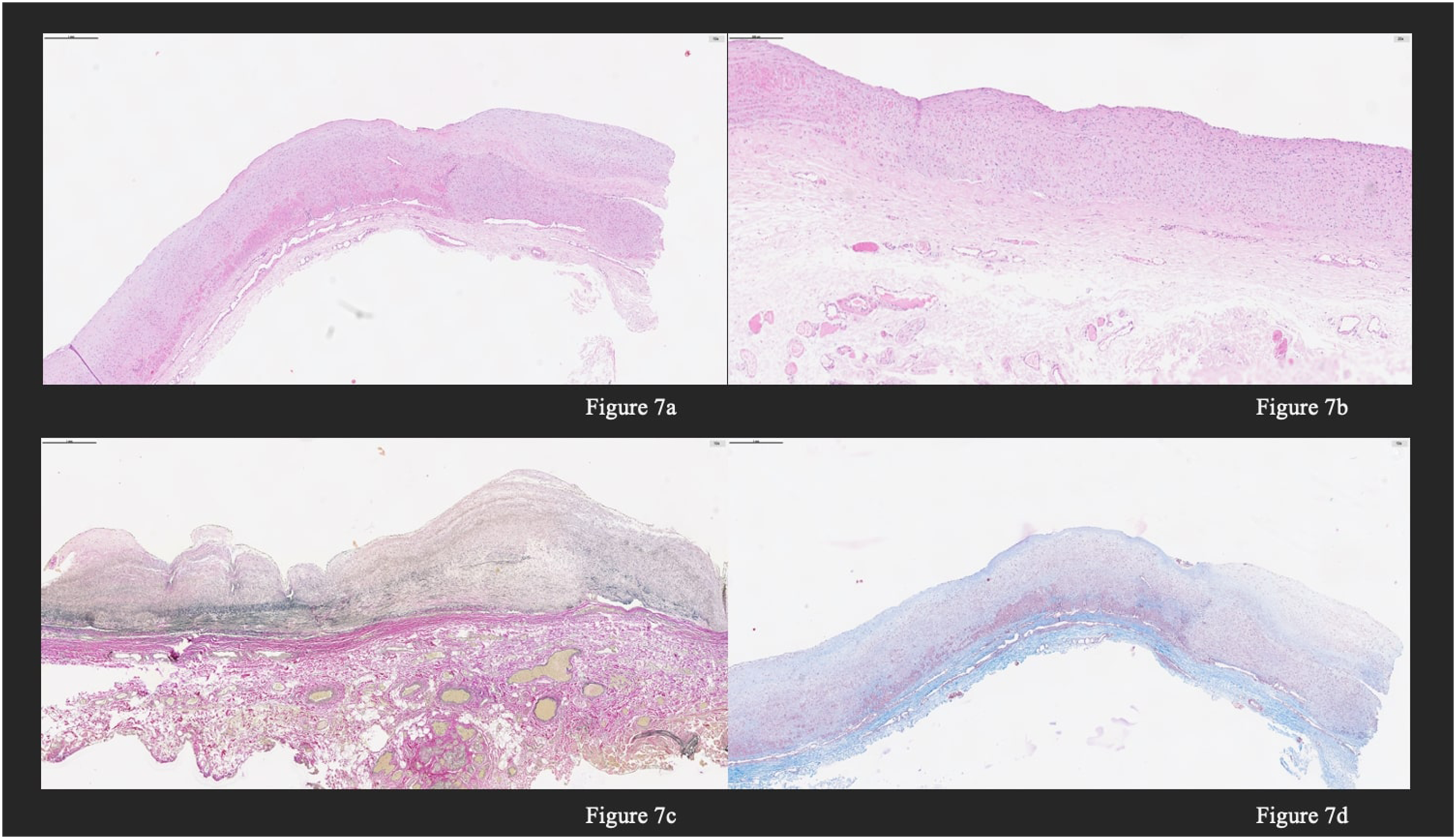
Discussion
Extracranial internal carotid artery aneurysms are rare, requiring for only 0.1% to 2% of all carotid artery–related interventions and account less than 1% of all peripheral artery aneurysms. Atherosclerosis stands as the primary etiology for the pathology, followed by trauma. 7 Infectious etiologies are more prevalent in younger populations. Autoimmune diseases, such as Behcet’s disease, Takayasu’s arteritis, and Cogan syndrome also play a role in the pathogenesis. Additionally, genetic predispositions including fibromuscular dysplasia, Marfan syndrome, Ehler-Danlos syndrome, osteogenesis imperfecta, and pseudoxanthoma elasticum can lead to such aneurysms. 8
Most cases of extracranial carotid artery aneurysms are incidentally detected in asymptomatic patients. However, clinical presentation can be highly variable and overlap with other conditions affecting the neck and cerebral circulation. In symptomatic individuals, the presentation depends on the underlying etiology, location, and size of the aneurysm. Common symptoms observed include pain, the presence of palpable masses, sensation of thrills, and nerve palsies resulting from compression by the carotid artery aneurysm. Less frequently, patients present with neurological manifestations such as cerebral ischemia, transient ischemic attack (TIA), or stroke. These symptoms arise from embolization of thrombi or plaque from the aneurysm into the cerebral circulation. Additionally, in some cases, the aneurysm may exert pressure on adjacent structures, causing symptoms of dysphagia (difficulty swallowing) or hoarseness due to compression of the esophagus or laryngeal nerves, respectively. 9 Diagnostic imaging with CT angiography is the gold-standard diagnostic tool and is critical for assessment of the aneurysm and planning for the most appropriate treatment approach whether it be surgical or endovascular. 10
Intervention is necessary to avoid adverse events of thromboembolism. Although the use of flow diverter stents in the endovascular treatment of extracranial carotid artery aneurysms has significantly increased in the past decade, surgery remains as the gold-standard approach. 11
Surgical management of extracranial carotid artery aneurysms includes clipping, excision with primary anastomosis, excision with interposition graft, extracranial–intracranial bypass, and carotid ligation. 12 Surgical management of the patient in our case was performed with resection of the aneurysmatic portion of the carotid artery followed by interposition of an autologous great saphenous vein graft. The choice of graft is mainly determined by etiology, size, and location of the aneurysm. While saccular aneurysms require partial aneurysmectomy of the carotid artery and angioplasty with Dacron, PTFE graft, or facial vein, fusiform aneurysms require total aneurysmectomy and arterial reconstruction with polytetrafluoroethylene, Dacron graft, the great saphenous vein, or cervical vein. 13
Endovascular approach to extracranial carotid artery aneurysms is on the rise as a novel treatment modality. Currently used stenting techniques include covered stenting, bare metal stenting, stent-assisted coil embolization, flow diverter stenting, and ligation. 14 The data is limited on the early and 5-year outcomes of stenting given its novelty; however, outcomes in a recent article by Schurman et al. demonstrated patients who underwent the endovascular approach had a higher proportion of postoperative stroke rates. 15 Another single institutional study found open repair was associated with greater risk for cranial nerve injury; meanwhile, the endovascular approach was more appropriate in cases requiring extensive dissection or with distal aneurysms but was consistent with higher postoperative stroke rates. 16
Endovascular strategies may be considered in patients with distal internal carotid artery aneurysms or contraindications to surgery. However, surgical therapy remains the gold standard in the treatment of extracranial carotid artery aneurysms, as we performed in our patient.
Supplemental Material
Supplemental Material
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.