
Abstract
Objectives
Post-reperfusion compartment syndrome is an emergency consequence following revascularization of acute limb ischemia. Fasciotomy is the gold standard treatment for acute compartment syndrome. Some surgeons perform prophylactic fasciotomy (PF) during the same operation; however, fasciotomy may lead to wound complications and an increased length of hospital stay. This study aims to evaluate the outcomes of prophylactic fasciotomy in our hospital.
Methods
This is a retrospective observational cohort study. We reviewed the data of acute limb ischemia patients at Maharaj Nakorn Chiangmai Hospital, who were diagnosed with non-traumatic acute limb ischemia and received revascularization between January 2006 and August 2022. The primary outcomes are 30-day amputation-free survival (AFS) and overall survival (OS). Propensity score weighting with confounder adjustment was used to balance peri-operative confounders.
Results
From our data, there were 56 patients in the PF group and 301 in the non-prophylactic fasciotomy (NPF) group. The 30-day amputation rates were 12.5% and 10% in the PF and NPF groups, respectively (p-value 0.895). The 30-day AFS was similar between the PF and NPF groups, with a hazard ratio (HR) of 0.93, 95% confidence interval (CI) 0.32-2.45, and a p-value of 0.882. The 30-day OS in the PF group was statistically lower than that in the NPF group, HR 4.09, 95% CI 1.55-10.77, and a p-value of 0.004. The 1-year and 5-year AFS were not significantly different between the PF and NPF groups. However, the 1-year and 5-year OS were lower in the PF group compared to the NPF group, with HR 3.44, 95% CI 1.37-8.65, and a p-value of 0.009, and HR 3.04, 95% CI 1.24-7.45, and a p-value of 0.015, respectively. Fasciotomy wound infection rates were higher in the PF group compared to the NPF group, 5.5% versus 1.7%, respectively, p-value 0.017. Other clinical outcomes did not show significant statistical differences.
Conclusions
Prophylactic fasciotomy may not improve amputation-free survival (AFS) but increases mortality, particularly within the first 30 days, even in some high-risk patients. The use of prophylactic fasciotomy should be limited to cases where it is clearly indicated.
Keywords
Introduction
Acute limb ischemia (ALI) is a condition characterized by a rapid decrease in blood flow to a limb due to acute occlusion of a peripheral artery or bypass graft. 1 Almost all cases of ALI require surgical revascularization to prevent the limb from becoming non-viable. However, following successful revascularization, the patient’s clinical condition can deteriorate. Ischemia-reperfusion injury (IRI) plays a major role during this period after revascularization and can manifest through either local or systemic effects. 2 Acute compartment syndrome (ACS) is the most common local effect of IRI. The clinical presentation of ACS includes severe extremity pain and massive tissue edema. An increase in intra-compartment pressure can decrease tissue perfusion and cause hypoxia. 3
The recommended treatment for ACS is emergency fasciotomy. Delaying fasciotomy can lead to further tissue necrosis, rhabdomyolysis, limb loss, and systemic organ failure. Some surgeons perform prophylactic fasciotomy during the same operation as revascularization to prevent post-reperfusion compartment syndrome in severe cases of ALI. 4 However, fasciotomy wounds may lead to complications such as nerve damage, wound infection, leg contracture, and prolonged hospital stays. 5 Until now, there is no consensus regarding early or prophylactic fasciotomy in cases of acute limb ischemia (ALI). This study aims to review the outcomes of prophylactic fasciotomy in our ALI case series to determine whether it provides clinical benefits.
Methods
This is a retrospective observational cohort study conducted at Maharaj Nakorn Chiangmai Hospital. The study included non-traumatic acute limb ischemia patients who underwent emergency revascularization between January 2006 and September 2022. Inclusion criteria comprised adult patients older than 18 years diagnosed with non-traumatic acute limb ischemia of Rutherford’s class I, IIa, or IIb. Each of these patients underwent revascularization through either open surgery or endovascular surgery. Patients diagnosed with acute limb ischemia of Rutherford’s class III requiring amputation were excluded. This study was reviewed and approved by the Research Ethics Committee, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand (No: SUR-2564-07995), with a waiver for written informed consent due to its retrospective nature. The objective of this study was to observe the therapeutic effects of prophylactic fasciotomy adjunct to revascularization in acute limb ischemia.
Definitions used in this study include the following: Acute limb ischemia refers to patients whose onset of symptoms is less than 2 weeks, with decreased arterial perfusion of the limb necessitating urgent evaluation and management. 6 Compartment syndrome is a condition that increases pressure within a closed compartment and compromises the circulation and function of tissue within that space. 7 Post-reperfusion compartment syndrome refers to patients diagnosed with acute limb ischemia who develop acute compartment syndrome following revascularization. The diagnosis of acute compartment syndrome is defined by clinical signs including a tense leg compartment, pain with passive motion of muscles traversing the same compartment, paresis or paresthesia referring to the same compartment, or an increase in intra-compartment pressure of the leg (where intra-compartment pressure minus mean arterial pressure is less than 40 mmHg, or intra-compartment pressure minus diastolic pressure is less than 10 mmHg). Emergency fasciotomy is indicated for every case of acute compartment syndrome.8,9 Prophylactic fasciotomy (PF) is performed concurrently with revascularization during the same operation. Prophylactic fasciotomy may be performed based on the surgeon’s opinion and is often indicated in cases with ischemic times exceeding 6 hours, Rutherford class IIB, younger age, and male patients. Therapeutic fasciotomy (TF) is performed subsequent to the diagnosis of compartment syndrome. 10 Both PF and TF are performed using a standard four-compartment release technique with two longitudinal incisions on the medial and lateral aspects of the leg. After either PF or TF was performed, every patient was scheduled for wound closure with a split-thickness skin graft once their clinical condition improved in the same admission. Fasciotomy wound infection is defined as an infection occurring within 30 days after the operative procedure, involving the skin or soft tissue at the fasciotomy site, and presenting with at least one of the following signs or symptoms: pain, tenderness, localized swelling, redness, heat, or abscess formation. 11 Leg contracture refers to the loss of movement and stiffness of the knee or ankle joint. Foot drop is characterized by weakness in the forefoot, resulting in abnormal gait and an inability to perform dorsiflexion.
The primary outcomes of this study are 30-day amputation-free survival (AFS) and mortality defined as 30-day overall survival (OS). Secondary outcomes include AFS and OS at 1 to 5 years, 30-day amputation rate, mortality rate, length of hospital stay, foot drop, wound infection, and leg contracture. Statistical analysis will be conducted using STATA version 16 Statistical Package. The study design is cohort-based, with categorical data compared using the Chi-squared test and numerical data compared using either the t test or rank sum test, depending on the distribution of the data. To address pre-treatment selection bias, factors such as high Rutherford classification, prolonged ischemic time, male gender, younger age, and elevated creatine kinase levels that may influence the surgeon’s decision to perform prophylactic fasciotomy were controlled using propensity score weighting. Confounding variables were further adjusted post-weighting with propensity scores. Variables considered include age, gender, body mass index, comorbidities (as defined by the Charlson comorbidity index), preoperative laboratory results, duration of ischemia, Rutherford’s classification of acute limb ischemia, level of arterial occlusion, etiology of acute limb ischemia, revascularization technique (embolectomy/thrombolysis/bypass/percutaneous transluminal angioplasty), and intra-operative intravenous fluid balance. Statistical significance is defined as a p-value less than 0.05.
Results
A total of 357 patient records were collected. All patients underwent emergency revascularization following a diagnosis of acute limb ischemia. Prophylactic fasciotomy (PF) was performed in 56 patients (15.7%). The remaining 301 patients received revascularization without fasciotomy (non-prophylactic fasciotomy, NPF). All patients were admitted to intensive care units and monitored postoperatively. In the NPF group, 29 out of 301 patients (9.6%) developed post-reperfusion compartment syndrome necessitating therapeutic fasciotomy.
Characteristic of acute limb ischemia patients undergone revascularization.
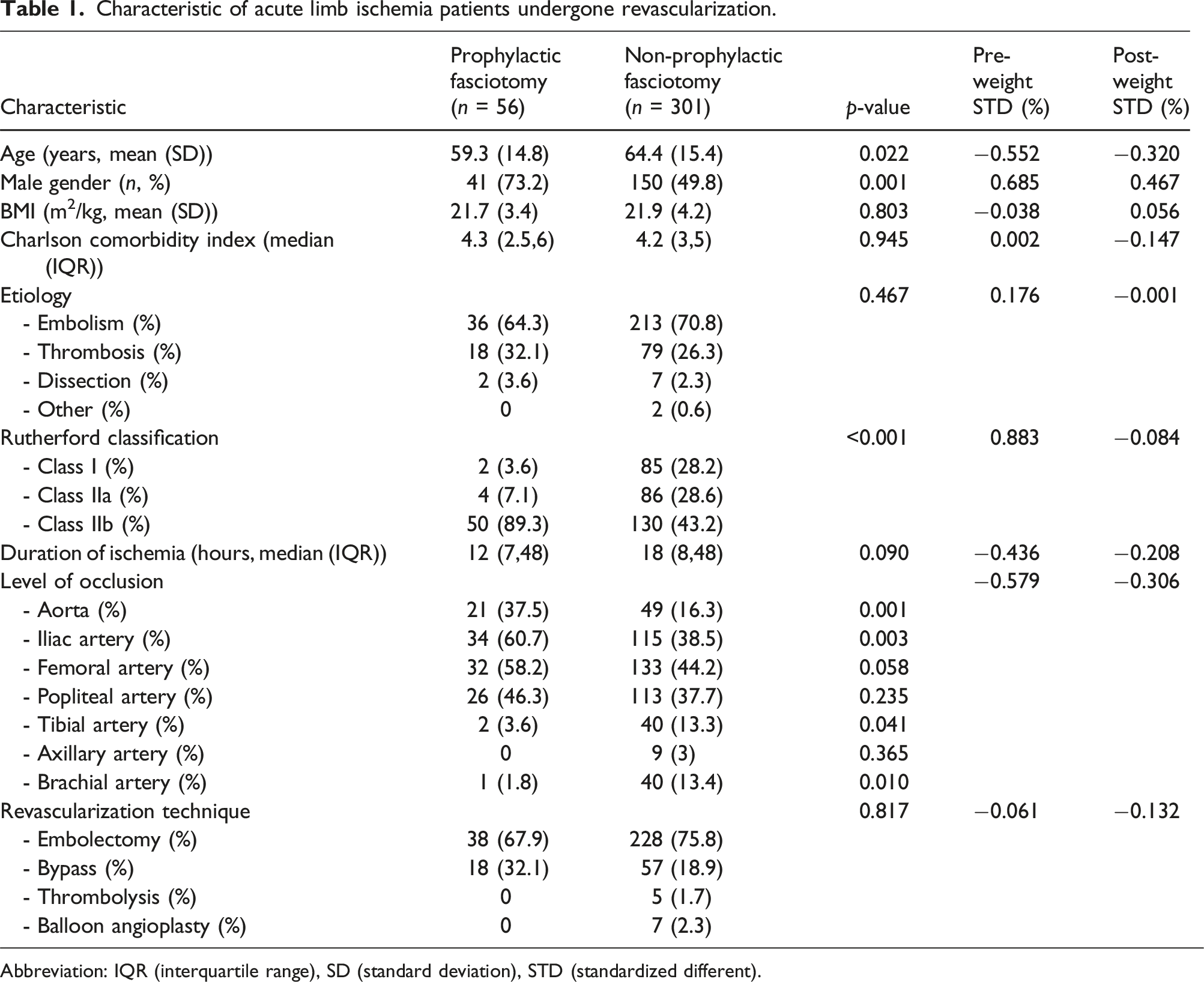
Abbreviation: IQR (interquartile range), SD (standard deviation), STD (standardized different).
Short- and long-term amputation-free survival (AFS) and overall survival (OS) between prophylactic fasciotomy and non-prophylactic fasciotomy after propensity score weighting and double adjustment with confounders.

Abbreviation: CI (confidence interval), HR (hazard ratio).
Sub-group analysis (high-risk group) of 30-day amputation-free survival (AFS) and overall survival (OS) between prophylactic fasciotomy and non-prophylactic fasciotomy after propensity score weighting and double adjustment with confounders.

Abbreviation: CI (confidence interval), CCI (Charlson comorbidity index), CK (creatine kinase), HR (hazard ratio).
Other clinical outcomes between prophylactic fasciotomy and non-prophylactic fasciotomy after multivariable logistic regression.

Abbreviation: CI (confidence interval), RR (risk ratio).
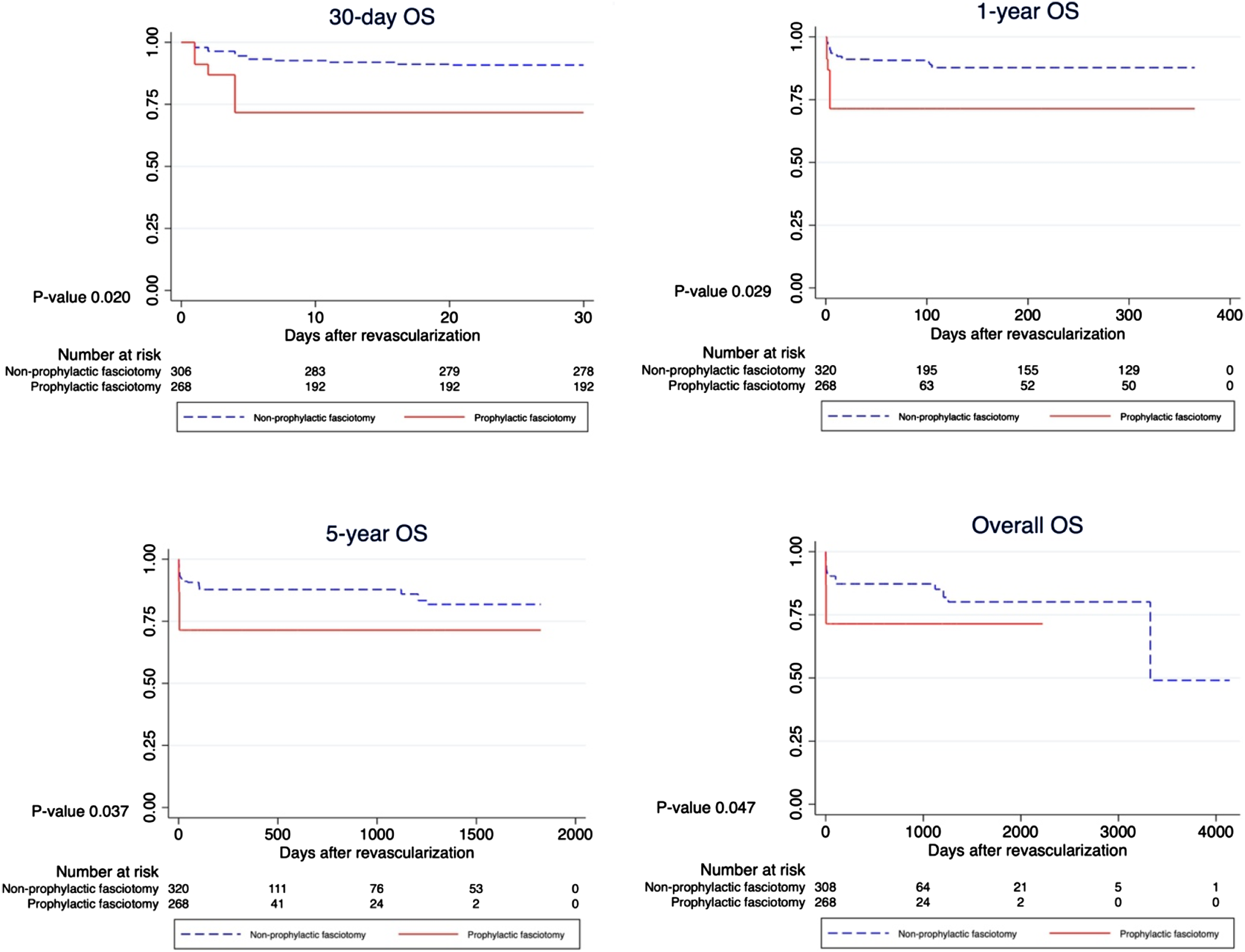
As depicted in Figure 1, the Kaplan-Meier curve shows no statistically significant difference in AFS between PF and NPF groups across short-term (within 30-day) to long-term (within 5-year and overall follow-up) periods. However, OS exhibited a decrease in every follow-up period, as illustrated in Figure 2. The most notable decline in OS was observed in the short-term period (within 30-day). Amputation-free survival (AFS) graph of prophylactic fasciotomy versus non-prophylactic fasciotomy. Overall survival (OS, mortality) graph after prophylactic fasciotomy versus non-prophylactic fasciotomy.
Discussion
In this retrospective observational cohort study, we have identified the primary outcome that 30-day AFS did not differ significantly between PF and NPF patients, even among those at high risk for compartment syndrome. AFS also showed no significant difference between PF and NPF groups within the 1-year, 5-year, and overall follow-up periods. OS was statistically lower in the PF group compared to the NPF group across all follow-up periods, particularly within the initial 30 days. The length of hospital stay was similar between PF and NPF groups but was statistically longer in the TF group compared to the PF group.
From previous studies, surgeons have shown a preference for performing prophylactic fasciotomy in patients at high risk of developing post-reperfusion compartment syndrome. 4 One study has shown that a delay in fasciotomy may lead to an increase in major amputations within 30 days, suggesting a liberal approach to prophylactic fasciotomy. 12 However, fasciotomy may increase the length of hospital stay and complications due to fasciotomy wound, such as nerve injury, wound infection, and leg contracture. 5 Surgical site infections (SSIs) may contribute to the increased overall mortality in patients undergoing PF. At our hospital, surgeons prefer delayed skin closure after fasciotomy rather than early closure, opting for skin grafts to prevent skin necrosis caused by overly tight sutures. This approach can lead to a higher incidence of SSIs, with delayed closure being a known risk factor. 13 Furthermore, in our hospital, surgeons tended to perform PF in high-risk patients who presented with more complicated diseases and high risk for postoperative compartment syndrome compared to those in the NPF group. These high-risk patients included those with ischemic times exceeding 6 hours, Rutherford class IIB, and elevated serum creatine kinase levels. High-risk patients are more susceptible to ischemia-reperfusion injury than low-risk patients, which manifests not only as post-reperfusion compartment syndrome but also as injury to remote organs such as rhabdomyolysis, acute kidney injury, and liver failure. 14 These risk factors, despite adjusting for some of these confounders in our analysis, could potentially explain the lower short- and long-term OS in PF patients. Another contributing factor to decreased OS in PF patients is fasciotomy wound infection, which is more prevalent than in NPF patients. Conversely, PF did not improve AFS in the short- or long-term, even among high-risk patients for post-reperfusion compartment syndrome. Moran et al. observed similar amputation rates in their study comparing prophylactic fasciotomy (PF) with therapeutic fasciotomy (TF) in patients with traumatic vascular injuries, aligning with our findings. 15 Specifically, patients with ischemic times exceeding 6 hours and Charlson comorbidity index scores greater than 4 may experience a decrease in OS due to PF, while AFS remains unchanged.
One recent data has shown contrasting results. Natour et al. found that 12% of patients developed acute compartment syndrome after revascularization and required TF, which was delayed and resulted in an increased rate of amputation within 30 days. 16 This study compared PF and TF, where TF would have a higher rate of AFS due to delayed diagnosis. This differs from our study, which compares PF to NPF. Our study includes patients who were later diagnosed with compartment syndrome and underwent TF, as well as patients without postoperative compartment syndrome, which should yield better outcomes in NPF group. While two studies have shown consistent results with our study, Karonen et al. found that in ALI, prophylactic fasciotomy improved in-hospital renal function but increased wound complications, suggesting a more conservative approach to fasciotomy. 17 On the other hand, in traumatic limb ischemia, Rao et al. found that sparing prophylactic fasciotomy and monitoring postoperatively could be performed without increasing limb complications. 18 Schupbach et al. also mention in their case report that prophylactic fasciotomy in cases where it is not necessary may lead to complications. They proposed new technology that allows continuous compartment pressure monitoring postoperatively. 19 Based on the results of our study, PF provides no benefit as it not only decreases OS but also demonstrates similar AFS compared to NPF. Therapeutic fasciotomy should be reserved for patients who meet the criteria for acute compartment syndrome, which is diagnosed during intensive postoperative monitoring.
A limitation of this study is its retrospective design. Some data may be missing, necessitating the use of complete case analysis. Preoperative risk factors, such as ischemic time, may be unreliable due to patients not recalling the exact onset of symptoms. Despite surpassing our sample size goal, which was calculated to differentiate AFS between groups (191 cases), pre-treatment biases influencing the decision to perform PF or not, as well as other peri-operative confounding factors, may affect outcomes even after weighting with propensity scores. Future prospective randomized cohort studies may be warranted, but ethical considerations must be carefully addressed.
Conclusion
Post-reperfusion compartment syndrome is an emergency consequence following revascularization in acute limb ischemia. Emergency fasciotomy is considered the gold standard treatment for acute compartment syndrome. This study demonstrates that amputation-free survival rates are similar between prophylactic fasciotomy and non-prophylactic fasciotomy groups. Overall survival is lower in the prophylactic fasciotomy group compared to the non-prophylactic fasciotomy group, particularly within the initial 30 days. This study suggests that routine prophylactic fasciotomy immediately after revascularization may not be necessary. Instead, postoperative close monitoring for acute compartment syndrome and performing therapeutic fasciotomy if indicated may be the appropriate approach for managing post-reperfusion compartment syndrome.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Statements and declarations
This research, titled “Outcomes of Prophylactic Fasciotomy in Patients with Non-Traumatic Acute Limb Ischemia,” was selected for presentation in the Charing Cross Symposium 2024 abstracts on-demand program, held from April 23rd to 25th, 2024, in London, United Kingdom. During the preparation of this work, the authors used ChatGPT version 3.5 in order to correct grammars. After using this tool/service, the authors reviewed and edited the content as needed and take full responsibility for the content of the publicat.