
Abstract
Objectives
Basilic vein transposition (BVT) surgery is a crucial option for vascular access in hemodialysis patients when other alternatives are unavailable. One of the primary complications affecting the long-term function of arteriovenous fistulas (AVFs) is the development of pseudoaneurysms, often caused by repeated punctures at the same site. This study aims to evaluate whether increasing the length of the basilic vein available for cannulation during the second stage of BVT surgery reduces the risk of puncture-related pseudoaneurysms, thereby improving fistula longevity and functionality.
Methods
We selected 39 hemodialysis patients unsuitable for cephalic vein AVF creation or who had failed brachiocephalic fistulas. Eligibility criteria included a basilic vein diameter of more than 2.5 mm with appropriate venous anatomy confirmed via ultrasound. In the first stage of surgery, the median basilic vein was anastomosed to the superior surface of the brachial artery. One month later, once the vein had matured (diameter ≥4 mm), a second stage was performed, which involved liberating an extended segment of the basilic vein down to the forearm. The basilic vein was then anastomosed end-to-end with the median basilic vein to increase the cannulation area. Patients were followed for 1 year to evaluate outcomes.
Results and Conclusions
All 39 patients successfully underwent the modified BVT technique. Over the 1-year follow-up period, none experienced significant AVF complications, particularly pseudoaneurysm formation. By increasing the usable length of the basilic vein for cannulation, multiple puncture sites were available, reducing the risk of repeated needle insertions at the same site. The modified BVT technique shows promise in reducing the risk of pseudoaneurysm formation and improving AVF patency, potentially enhancing the longevity and functionality of AVFs in hemodialysis patients. Further studies are necessary to confirm the efficacy of this technique in larger patient populations.
Keywords
Introduction
Basilic vein transposition (BVT) surgery plays an essential role in vascular access in hemodialysis patients, especially when other options are unavailable. In 1976, Dagher et al. introduced the BVT technique. 1 Since then, BVT surgery has undergone several modifications and adaptations. 2 One of the complications that can affect the function and lifespan of the fistula is the development of a pseudoaneurysm caused by multiple punctures of the vein at the same site. 3 Additionally, one factor that appears to improve the fistula’s performance is the basilic vein’s length, which is available for puncture during hemodialysis cannulation. We believe that increasing the length of the basilic vein during the second stage of BVT surgery will allow more areas of the patient’s arm for hemodialysis puncture. This could reduce the likelihood of complications, such as the formation of a puncture-induced pseudoaneurysm, by minimizing the probability of puncturing previously punctured sites. 3
Patient selection
This technique is considered for patients who lack a suitable cephalic vein for AVF creation or those whose brachiocephalic fistula has failed. The procedure is appropriate when there is no evidence of limb edema or thrombosis in the deep venous system and the basilic vein has a diameter greater than 2.5 mm with appropriate anatomy. A critical anatomical requirement is at least one basilic vein branch in the cubital fossa (like the median cubital vein) measuring over 2 mm in diameter, with the basilic vein extending along the medial aspect of the forearm.
Technique
After ultrasound-guided venous mapping confirms the basilic vein’s anatomical suitability, the patient becomes a candidate for AVF surgery if appropriate. In the first stage, the branch of the basilic vein in the cubital fossa (median basilic vein) is anastomosed to the superior surface of the brachial artery using a 6/0 Prolene suture.
One month after the surgery, or once the vein diameter reaches at least 4 mm, the patient is eligible for the second stage. In this second stage, following venous mapping with ultrasound and precise marking of the vascular route, a longitudinal incision is made on the medial aspect of the arm, extending to the medial side of the upper forearm (Figure 1). Subsequently, the basilic vein is meticulously explored and freed from the arm and forearm. Ultrasound-guided venous mapping before the surgery.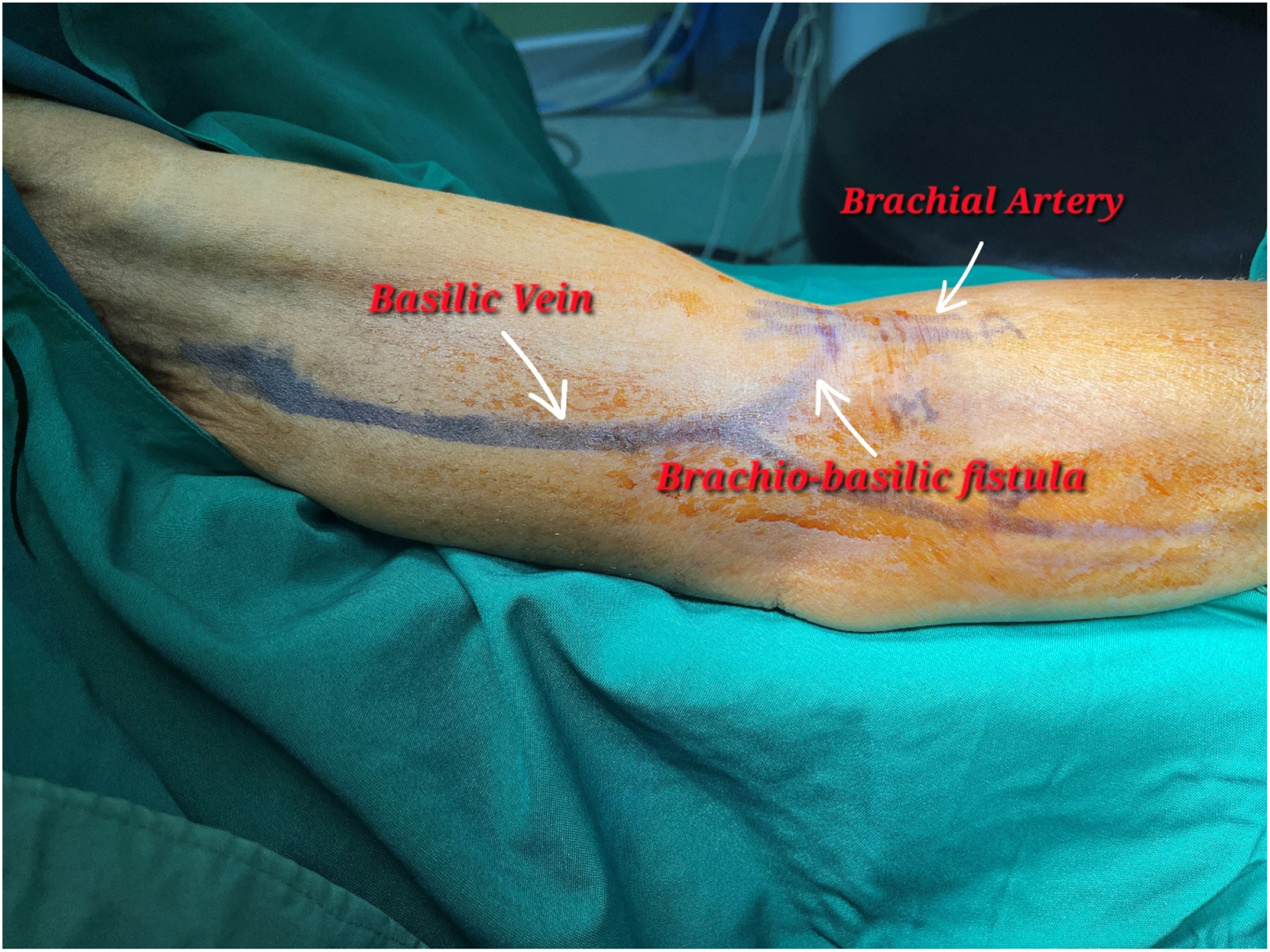
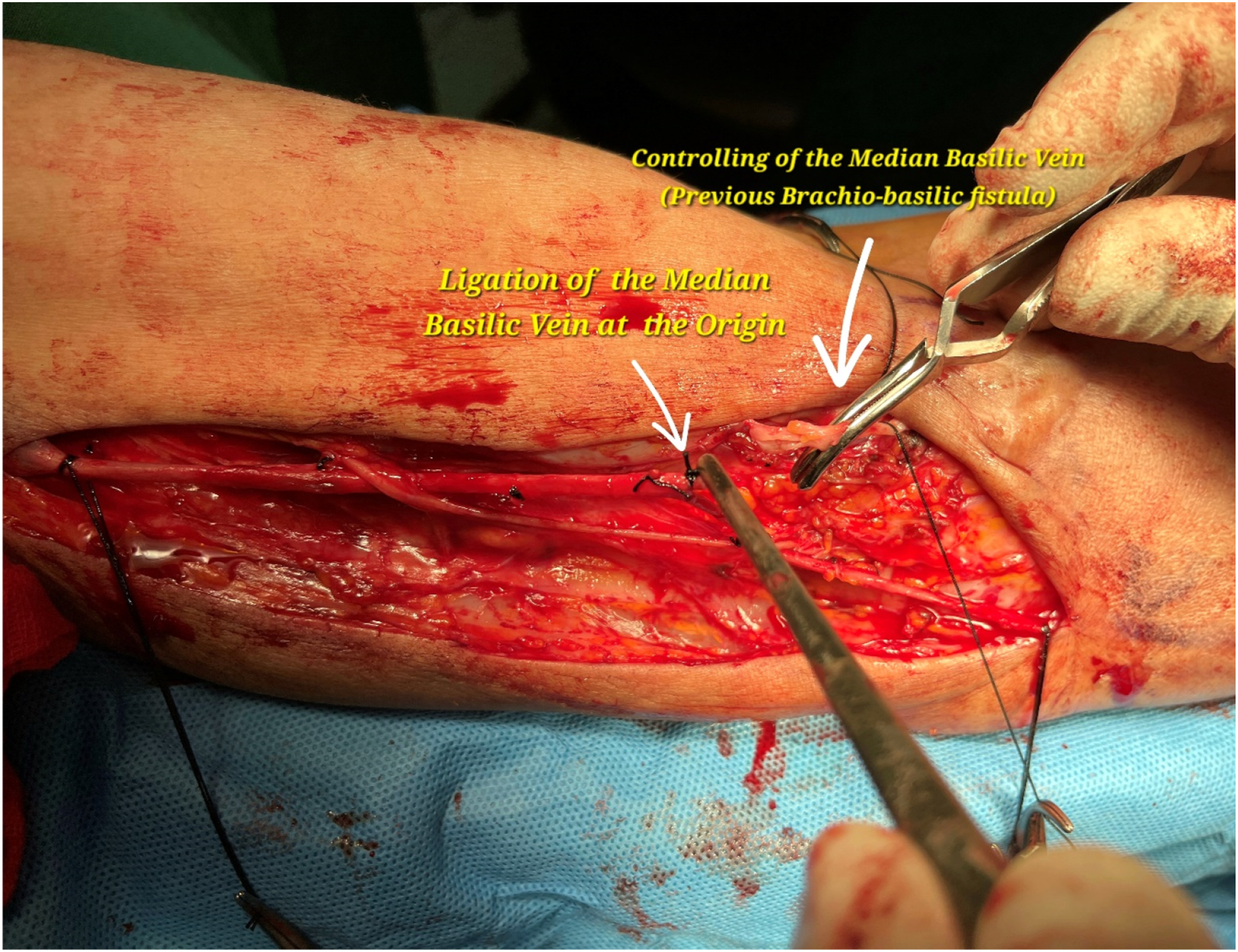
Once the basilic vein is fully liberated and its side branches ligated, exploration is performed to free the median basilic vein up to the site of the first-stage anastomosis (Figure 2). Using Putz scissors, the median basilic vein is carefully dissected at its junction with the basilic vein, and the resulting defect is repaired using a 7/0 Prolene suture (Figure 3). After full liberation of the basilic vein with ligation of its side branches, the median basilic vein is explored and freed up to the site of the first-stage anastomosis. The median basilic vein is controlled and cut at its origin, while the defect in the basilic vein wall is repaired with 7/0 Prolene suture.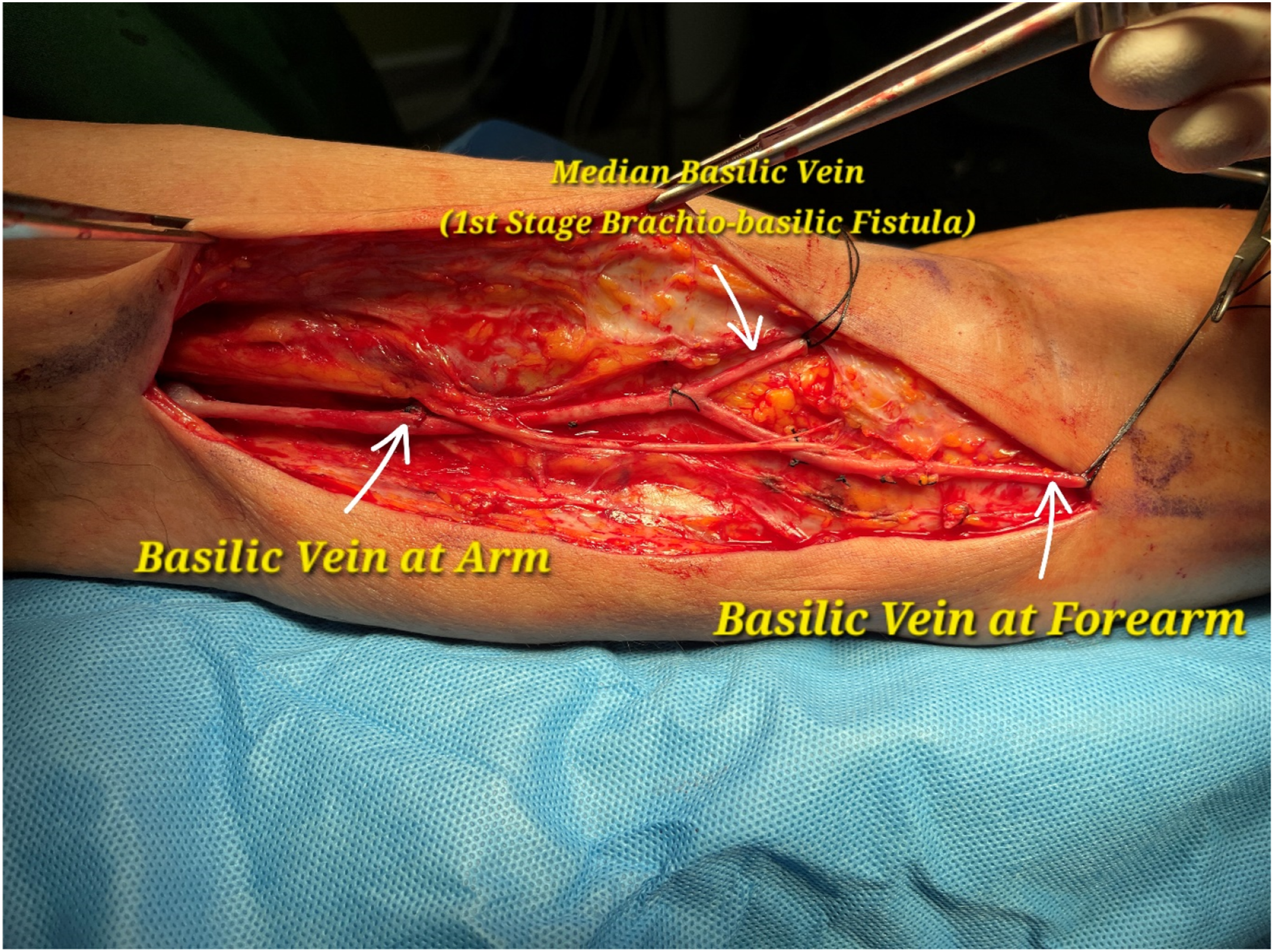
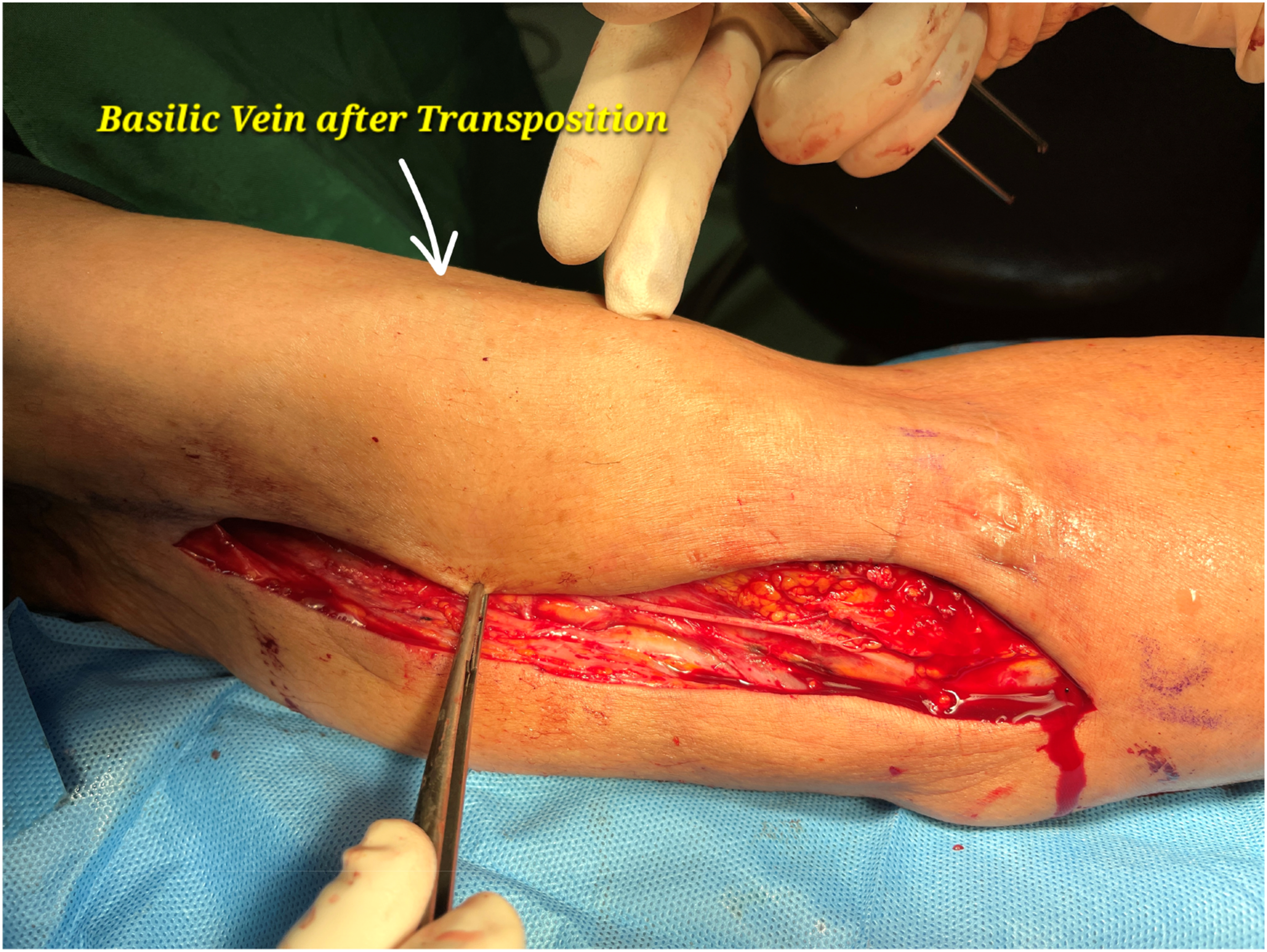
The distal end of the basilic vein in the forearm is transected, and after spatulation, it is anastomosed end-to-end to the distal end of the median basilic vein. Following creating a flap in the arm, the basilic vein is positioned in a tension-free curved manner in the appropriate location. After the final evaluation of the anastomosis, the subcutaneous tissue and skin are closed (Figures 4 and 5). The distal basilic vein is transected, spatulated, and anastomosed end-to-end with the median basilic vein and then positioned in a tension-free curve after flap creation. Basilic vein after elevation and transposition.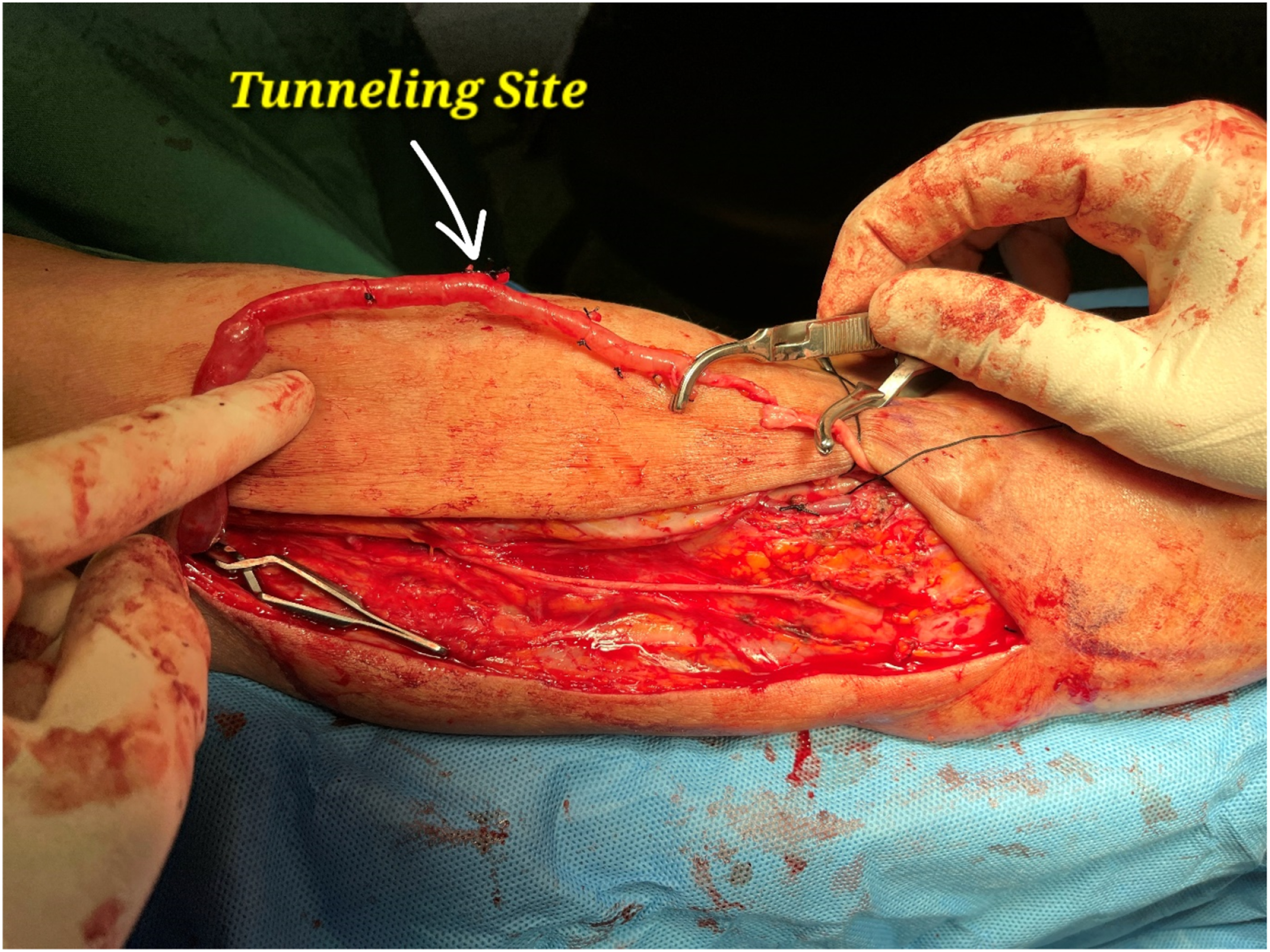
Discussion and conclusion
In this modified approach, the basilic vein is tracked down to the forearm, and a more extended segment of it is freed to be anastomosed end-to-end with the distal portion of the median basilic vein. It is important to note that in the first stage, the median basilic vein was anastomosed to the superior surface of the brachial artery to prevent tension and preserve alignment after the basilic vein is transposed in the second stage.
We performed this modified technique at our center on 39 carefully selected hemodialysis patients. After reviewing their 1-year follow-up, none of the patients experienced significant arteriovenous fistula (AVF) complications, particularly the formation of pseudoaneurysms. We believe this approach, which extends the basilic vein’s usable length for cannulation, may reduce the likelihood of pseudoaneurysm formation by providing multiple puncture sites and minimizing the risk of repeated needle insertions at the same site. As a result, it may enhance the fistula’s longevity and functionality in hemodialysis patients. Further clinical studies will be necessary to validate the efficacy of this technique in a broader patient population.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.