
Abstract
Background
Superior vena cava syndrome (SVCs) is a common complication in hemodialysis patients due to central vein occlusions, often caused by prior catheterizations. Management can be challenging.
Objective
To describe a successful endovascular approach to managing SVCs caused by right innominate vein (RIV) occlusion in a hemodialysis patient with a non-functional LeVeen shunt.
Method
An 80-year-old dialysis patient with upper limb edema and vascular access dysfunction was diagnosed with complete RIV occlusion around a long-standing LeVeen shunt. Recanalization was achieved via a percutaneous approach, including angioplasty and placement of a balloon-expandable covered stent, leaving the LeVeen shunt in situ to reduce risks.
Results
The procedure restored venous patency and improved vascular access functionality. Postoperative imaging confirmed excellent stent positioning and reduced venous congestion. At a 6-month follow-up, central vein patency was maintained.
Conclusion
Endovascular recanalization is a safe and effective strategy for managing SVCs, even with a retained central venous device. This approach preserved vascular access and ensured successful long-term dialysis, offering insights for treating complex venous occlusions.
Keywords
Introduction
SVCs resulting from central vein occlusion are very common in hemodialysis patients with a history of previous central venous catheterizations (CVC).
Repeated damage to the endothelium caused by CVC and the turbulent flow induced by arteriovenous fistulas (AVFs) can boost the formation of stenosis in the central venous system and superior vena cava (SVC). Typically, symptoms of venous congestion take a while to manifest as extensive collateral vessels ensuring sufficient venous drainage. Symptoms of SVCs include dyspnea upon exertion, orthopnea, headaches, dilated neck veins, facial and neck swelling, and drooping eyelids.1,2
LeVeen shunt is a special catheter used to create a peritoneal-caval shunt in patients with chronic liver failure and refractory ascites. It used to be tunneled subcutaneously along chest wall to reach the superior vena cava or the internal jugular vein. The ascites liquid could be drained into the central venous system.3,4
The case we report concerns a patient with a right upper limb vascular access malfunctioning due to fibrotic occlusion of the right innominate vein (RIV), site of insertion of an old LeVeen shunt that was no longer used.
Case report
We report a case of an 80-year-old man, on three-weekly dialysis treatment with autologous AVF of the right upper limb, who developed SVCs due to the obliteration of the RIV.
The patient had a peculiar history of chronic liver disease treated for many years with a subcutaneous LeVeen shunt positioned from the peritoneum to the right atrium by cannulation of the right innominate vein.
Following a successful liver transplantation, the catheter was no longer used but it was left in place.
Over the years, the patient developed chronic renal failure (CKD) and began hemodialysis through an autologous arteriovenous access to the right arm, a brachiocephalic elbow fistula that functioned adequately for over 4 years.
Subsequently, the patient experienced SVCs with edema of the right upper limb, visible and dilated chest wall venous collateral networks, and vascular access malfunctioning with high return pressures. These signs and symptoms led to the suspicion of the presence of an altered central venous drainage.
It was confirmed by a Computed Tomography (CT) angiogram that documented a complete fibrotic occlusion of the right innominate vein around the LeVeen catheter in the innominate right vein.
The presence of the shunt in the central veins for many years had led not only to the complete fibrosis of the right brachiocephalic vein but also to the development of significant hypertrophic collateral branches. The aim was to preserve these enlarged collateral branches, which accounted for most of the central venous outflow (Figure 1). Preoperative angio-computed tomography in coronal (a) and axial (b) planes which show obliteration of the right innominate vein after its origin. 3D reconstruction highlights the LeVeen catheter insertion site at the confluence of the right subclavian and right internal jugular (c).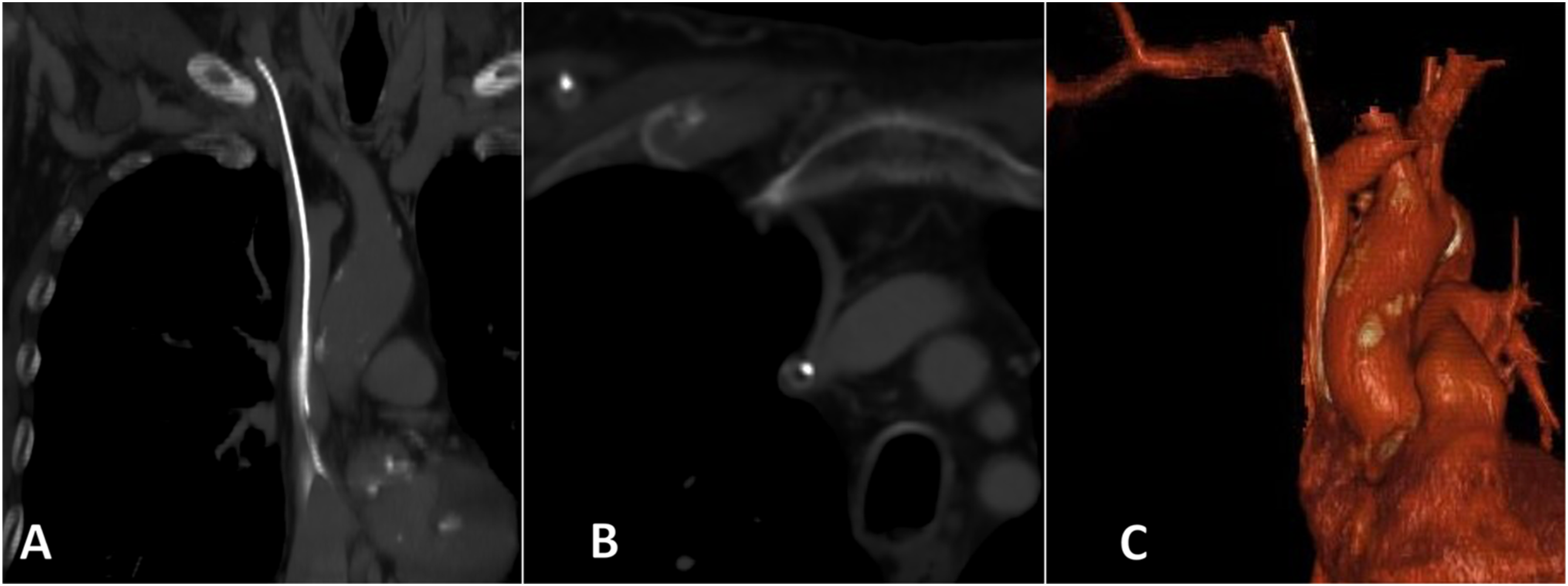
The patient did not suffer from severe manifestations of SVCs such as laryngeal edema or headache but, in order to safeguard the access, a recanalization procedure of the RIV was planned despite the persistence of the LeVeen shunt.
The procedure was performed under local anesthesia, via percutaneous access to the arterialized right cephalic vein. Few attempts were made to recanalize the stenosis using different types of guidewires. A right femoral access was obtained trying to cross the occlusion retrogradely using a hydrophilic 0.035” stiff guidewire supported by a guiding catheter (Destination, Terumo, Tokyo, Japan), which also failed. A successful attempt was done with a 0.018” guidewire (Astato, Asahi Intecc, Aichi, Japan) and a guiding catheter (Berenstein, Cordis, Hialeah, USA). Pre-dilatation was performed with a 3 × 150 mm ultra-non-compliant balloon (Ultraverse, Bard Peripheral Vascular, Tempe, AZ, USA). The lesion was stented with an 8L × 59 mm balloon-expandable covered stent (Viabahn VBX; W.L. Gore & Associates, Newark, DL, USA) delivered through an 8 Fr guiding sheath (Destination, Terumo, Tokyo, Japan) on a stiff guidewire. Employing the guiding sheath was crucial for preventing stent migration and disconnection from the balloon when crossing the stenosis. A post dilatation up to 10 mm with a non-compliant 10 × 20 mm balloon (Atlas Gold, Bard Peripheral Vascular, Tempe, AZ, USA) was performed to adapt the proximal and distal edge of the stent to the vein diameter, obtaining appropriate flaring.
The final phlebographic study showed excellent patency of the stent with no signs of residual stenosis, an excellent thrill of the AVF was immediately obtained and there was an initial decrease in venous collaterals on the chest and arm. The patient was discharged the same day on (DAPT) with Clopidogrel 75 mg and Cardioaspirin 100 mg for 6 months. (Figure 2) Venography of the right upper arm showing central vein stenosis with prominent collateral branches (a). Percutaneous transluminal angioplasty was performed with an ultra-noncompliant balloon to pre-dilate the occlusion (b). Completion venography reveals optimal deployment and apposition of the covered stent with no signs of recoiling (c).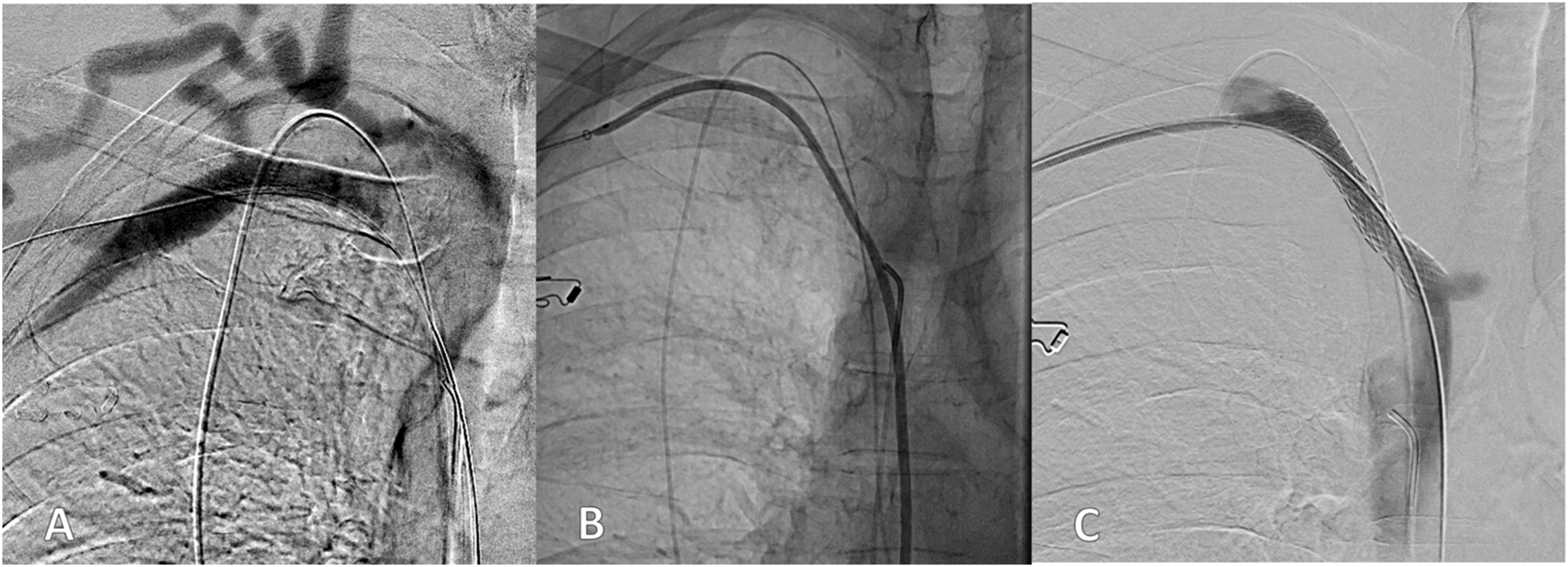
Four months later, the patient came to our attention presenting right arm edema secondary to right cephalic vein stenosis which was not present at the time of our first intervention. He underwent a percutaneous angioplasty of the stenosis. Intraoperatively a phlebographic study of the central veins was performed demonstrating the good outcome of the previous procedure with regular patency of the previous stent on the central venous district (Figure 3) A venography conducted 4 months after the first procedure revealed a durable result, with persistent patency of the implanted stent.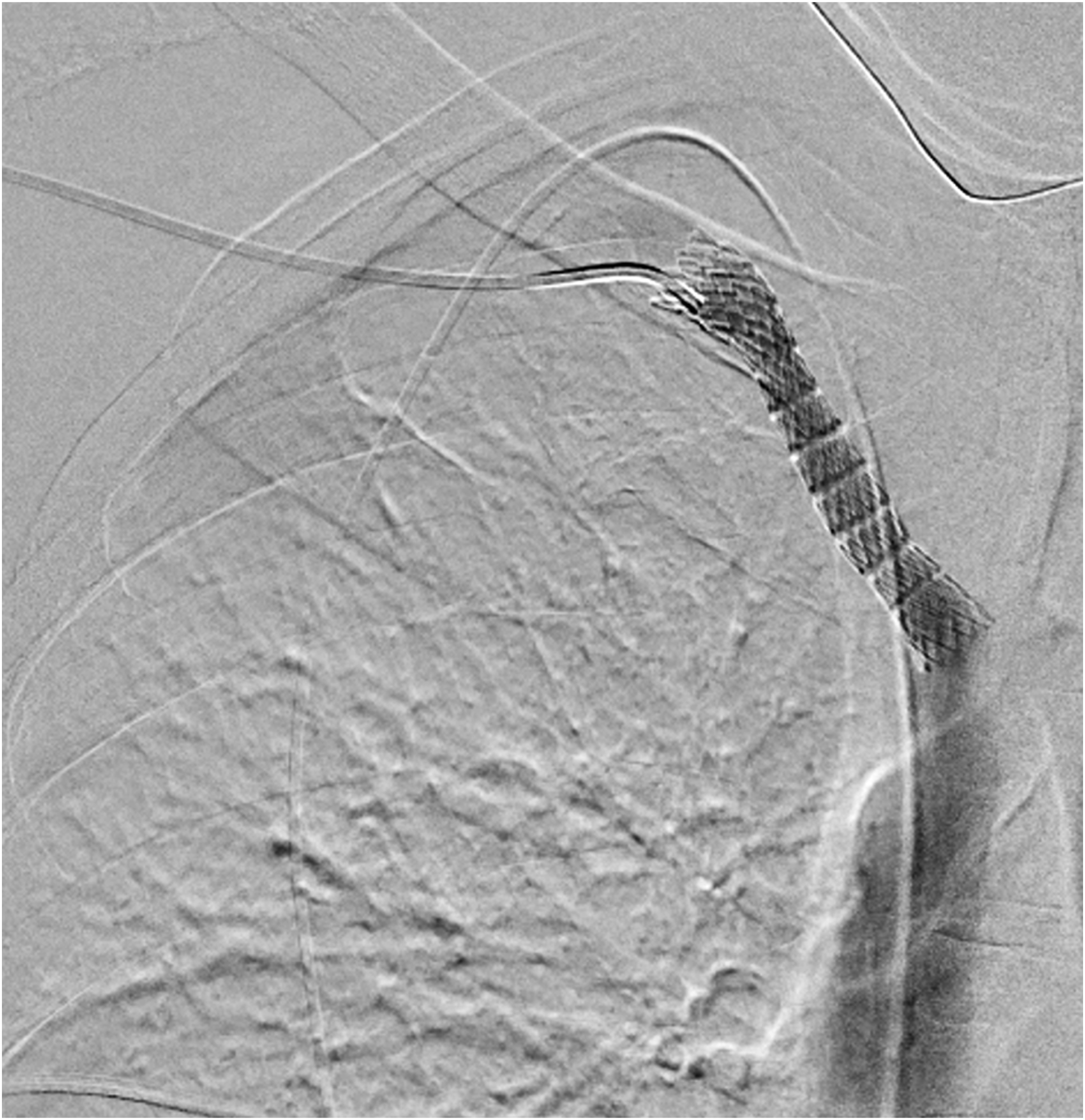
At 6 months, the patient performs regular and effective dialyses which represent our benchmark for follow up.
The patient has provided informed consent for the publication of this case report, including the use of its medical information and data.
Discussion
Central venous catheters represent a common cause of failure of vascular accesses of the upper limbs and overload syndromes. The formation of fibrous stenoses at the site of catheter positioning which hinders venous drainage is very common.
Endovascular treatment such as percutaneous angioplasty and stent placement are the first choice for the purpose of central veins recanalization to prevent serious forms of edema of the cervico-brachial and cerebral district and restore vascular access functionality. 5
It is rather atypical, however, to perform these recanalization procedures with the persistence of a central venous device still in place. 6
In this case, a permanent peritoneal-caval shunt had been in place for many years and was no longer in use. Its removal would have been rather complex and risky given the presence of innominate vein fibrosis and thrombosis and not useful for the purposes of the recanalization procedure. Therefore, recanalization of the RIV was performed with the catheter left in place. The positioning of a covered stent was planned from the beginning to enhance procedural safety in case of vessel laceration, reduce thrombus migration risk and make the recanalized site more homogeneous. This also seems to foster greater long-term patency rates with fewer stenosis recurrences.
The initial access was via the upper limb vascular access site, but due to suboptimal results, a second access was established from the right femoral vein using a long and rigid introducer for better guidewire support enhancing its pushability.
Recanalization was eventually obtained after repeated attempts from the proximal access with the use of an Asahi-type guide which has the characteristics of having a weighted tip specifically designed for intraluminal recanalization of chronic total occlusions with excellent penetration in highly calcified or fibrotic lesions.
The choice of VBX was related to its excellent navigability in the occluded sections, without dissociating from the balloon with a structure that allows excellent adaptability and conformability even in complex vascular anatomy. Post-implant overdilation is an added value that allows optimal sealing. These features contribute to a calibrated and precise release.
In conclusion, vascular access rescue is crucial for hemodialysis patients, this peculiar case of recanalization of an innominate vein with chronic fibrous and thrombotic occlusion in concomitant presence of a LeVeen-type peritoneal-caval shunt 7 may helpful technical highlights for the treatment of SVCs.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.