
Abstract
Objectives
We present a clinical case illustrating the feasibility of endovascular treatment of superior mesenteric aneurysm associated with an arteriovenous fistula.
Methods
The patient presented with abdominal pain and diarrhea on admission. Computed tomography angiography revealed an aneurysmal dilatation of the superior mesenteric artery and vein with an arteriovenous fistula. Endovascular therapy successfully managed the condition by reconstructing the artery, closing the fistula, and occluding the aneurysm.
Results
No aneurysm rupture or endoleak occurred, and the patient’s symptoms on admission resolved.
Conclusions
Endovascular treatment is a viable alternative for patients with superior mesenteric aneurysms and arteriovenous fistulas, but larger studies and further follow-up are needed to evaluate the safety and long-term efficacy of endovascular treatment.
The patient, a 69-year-old man, was presented with abdominal pain and melena. The patient had positive tenderness on palpation of the abdomen, with no obvious muscle guarding or rebound tenderness. There were no other specific physical examination findings. The patient had no history of abdominal trauma, pancreatitis, or gastrointestinal infection. Computed tomography angiography (CTA) revealed aneurysmal dilatation of the superior mesenteric artery (SMA) and the superior mesenteric vein (SMV) along with an arteriovenous fistula between the two vessels (Figure 1). Additionally, thrombosis of the SMV and splenic vein was observed. Given the size of the aneurysm, open resection was considered high risk, and an alternative approach utilizing endovascular therapy was pursued. The patient’s superior mesenteric artery aneurysm (SMAA) measured approximately 72 mm in diameter, which posed a significant risk. The patient had no history of smoking but occasionally consumed alcohol. Upon admission, the patient’s hemodynamic measurements were within the normal range, indicating stable cardiovascular status. After careful consideration and discussion, an operative plan involving endovascular therapy was chosen. Coated stents (Viabahn, W.L. Gore & Associates, Flagstaff, AZ, USA) were utilized to reconstruct the superior mesenteric artery, effectively isolating the arteriovenous fistula. Coil embolization was successfully performed to occlude the aneurysm cavity, minimizing the risk of rupture or further expansion (Figures 2 and 3). The endovascular therapy proved successful in managing the patient’s condition. By reconstructing the SMA and closing the arteriovenous fistula, the abnormal communication between the SMA and SMV was eliminated. Furthermore, coil embolization prevented further enlargement of the aneurysm and reduced the risk of complications associated with its rupture. We conducted a 7-month follow-up on this patient and performed a CTA re-examination 4 months (Figure 4) after the surgery. The patient currently has regular daily bowel movements with no abdominal pain, discomfort, or bloating. (a) CTA on admission showed an embolism aneurysmal dilatation of the SMA and the SMV. (b) Contrast medium appeared in the mesenteric vein during the arterial phase of CTA. (c) Sagittal scans demonstrated aneurysmal dilation of the SMA. (d) A 3-dimensional volume-rendered image derived from the CTA showed the SMA aneurysm. (a) and (b) DSA showed the aneurysm from different angles and contrast medium appearing in the mesenteric vein and inferior vena cava. (c) Superselective distal SMAA angiography observed the SMA branches. DSA after stent insertion and transarterial embolization demonstrated no flow to the aneurysm. DSA confirmed collateral perfusion of the bowel. (a) CTA performed 4 months after discharge showed no apparent development of the SMV and thrombus of the SMAA. (b, c, d) The SMA stent was unobstructed, although the coil affected some imaging. The shape and position of the support were good, and aneurysm isolation was complete. CTA, computed tomography angiography; SMA, superior mesenteric artery; SMV, superior mesenteric vein; DSA, digital subtraction angiography; SMAA, superior mesenteric artery aneurysm.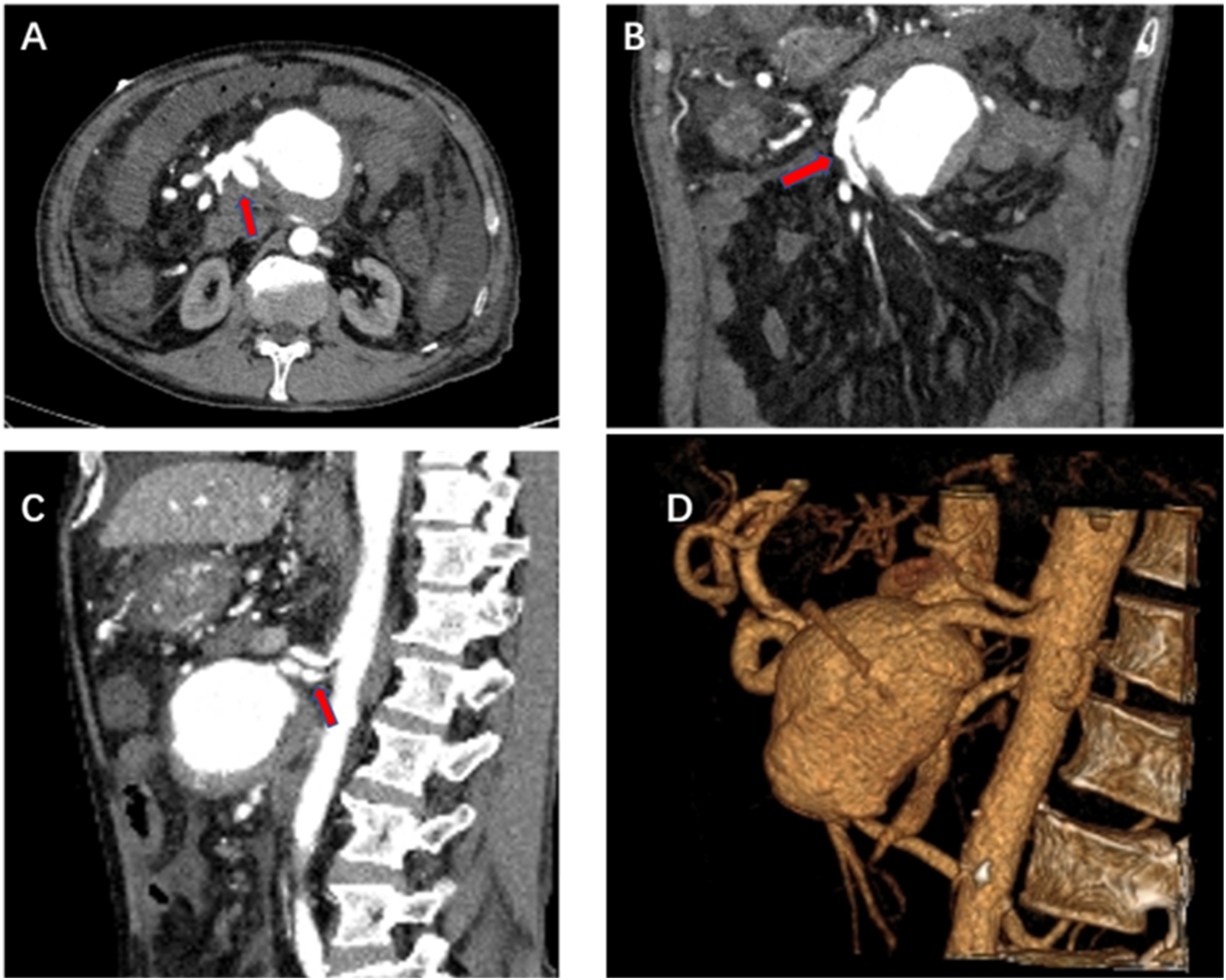



Discussion
Superior mesenteric arteriovenous fistula (SMAVF) is a rare condition in clinical practice, and its clinical symptoms are often atypical. Patients with SMAVF may present with abdominal pain and diarrhea, which can be attributed to intestinal ischemia resulting from high-flow shunts.
1SMAVF is characterized by an anomalous communication between the SMA and the SMV. This condition can be either congenital or acquired, with bowel surgery and abdominal trauma being the most common causes of acquired SMAVF. 1 Iatrogenic SMAVF typically arises from mass ligation during intestinal resection or from ligation of the mesentery without precise localization of the bleeding point. 2 In this case, the patient had no history of abdominal trauma, pancreatitis, or gastrointestinal infection and no obvious scars were observed on the patient’s abdomen during the physical examination. It was determined that the patient’s SMAVF was likely congenital. Treatment options for SMAVF include surgical and endovascular interventions, with the latter being preferred in most cases due to its association with reduced morbidity, lower costs, and the ability to repeat the intervention if necessary; case reports indicate that endovascular interventions may involve coil embolization and stent placement.3,4 SMAA are rare, accounting for 6% to 15% of all visceral aneurysms (VAAs). 5 While infection is believed to be the most common cause of SMAA, current evidence suggests that degenerative conditions, connective tissue diseases, and inflammatory disorders (such as pancreatitis, vasculitis, spontaneous dissection, fibromuscular dysplasia, and polyarteritis nodosa) are potential causes. 6 According to the Society for Vascular Surgery VAA guidelines, all SMAA and pseudoaneurysms should be repaired regardless of their size. 7 Recent trends have shifted toward endovascular repair using covered stents and transcatheter embolization. 8 Evidence for endovascular VAA repair indicates success rates ranging from 93.3% to 98.3%, with major and minor complication rates ranging from 1.8% to 3.6% and 8.9% to 10.5%, respectively. Procedure-related complications may include hematoma, vascular dissection, splenic infarction, intestinal ischemia, aneurysm reperfusion, and stent thrombosis.8,9
In this case, endovascular therapy provided a viable alternative to open resection for a patient with a large aneurysm and arteriovenous fistula of the superior mesenteric artery. By utilizing covered stents and coil embolization, the abnormal vessel communication was addressed, and the aneurysm was effectively managed. This case highlights the importance of considering individual patient factors and tailoring the treatment approach accordingly to achieve optimal outcomes in complex vascular conditions. Further follow-up and monitoring will be necessary to evaluate the long-term efficacy and durability of the endovascular treatment.
Footnotes
Author contributions
Feifei Wang: preliminary writing of the article and selection of images. Xiaojun Shu: selection of case and revision of the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Gansu Province Education Technology Innovation Project No. 2022B-009, the fund from the First Hospital of Lanzhou University Fund: ZX-62000002-2021-247, and Young Scientists’ Fund of the Gansu Provincial Science and Technology Program No. 23JRRA1615.
Ethics statement
The study was conducted in accordance with the ethical guidelines and principles outlined by The First Hospital of Lanzhou University. The use of all materials during the patient’s surgery was composed of commercially available and approved materials known to be safe. Prior to the surgery, the patient provided informed consent, acknowledging the nature of the procedure and potential risks involved. The patient’s consent was obtained prior to submission of this article.