
Abstract
Background
The global adoption of endovascular aortic techniques has progressed rapidly, yet the extent of Latin America’s participation in this revolution requires comprehensive evaluation. This review examines the region’s current capabilities, innovations, and barriers in aortic endovascular therapy.
Methods
We conducted a systematic analysis of published experiences and institutional reports from across Latin America, focusing on three key areas: ascending/arch aortic interventions, thoracoabdominal repairs, and endoleak management strategies.
Results
The region has demonstrated significant progress in adopting complex endovascular therapies despite resource limitations. Several centers have successfully implemented advanced techniques, including total percutaneous arch repairs, hybrid debranching procedures, and customized endograft solutions. Experience with thoracoabdominal pathologies shows promising outcomes with fenestrated and branched endografts, while innovative approaches to endoleak management have been developed, particularly for challenging type II and III cases. However, variability in outcomes persists due to disparities in technology access, training opportunities, and follow-up protocols. The available evidence, while growing, remains largely limited to single-center experiences with modest sample sizes.
Conclusion
Latin America has made measurable strides in aortic endovascular therapy, demonstrating both technical capability and innovative adaptations to local challenges. The establishment of a Latin American Aortic Registry (LATAR) would address critical gaps in data standardization, facilitate outcome benchmarking, and promote equitable technology dissemination. Such structured collaboration is essential for the region to fully participate in the global advancement of aortic care.
Introduction
The field of aortic endovascular surgery has experienced transformative advancements in recent years, reshaping the management of complex aortic pathologies worldwide. However, the extent to which Latin America has embraced these innovations remains a topic of debate. The unique demographic, socioeconomic, and healthcare landscapes of the region present both opportunities and challenges for adopting state-of-the-art endovascular techniques. Factors such as limited access to advanced technologies, disparities in healthcare infrastructure, and variability in training programs have impacted the widespread implementation of endovascular procedures. Despite these obstacles, Latin American centers have demonstrated resilience and adaptability by advancing expertise in minimally invasive techniques, developing region-specific protocols, and participating in global clinical trials. Nevertheless, the question remains—has Latin America fully integrated into the global aortic endovascular trend, or are there still gaps to be addressed? This editorial aims to explore the current state of aortic endovascular interventions in Latin America, highlighting key achievements, barriers, and the critical steps needed to ensure the region’s prominent position in the ongoing revolution.
Ascending aorta and arch aortic
In recent years, endovascular techniques have been increasingly applied to the management of ascending aorta and aortic arch diseases, offering a less invasive alternative to traditional open surgery. Numerous studies across the Latino America region have reported on the feasibility, technical success, and outcomes of endovascular repair of these high-risk aortic pathologies. The data suggests a promising future for these approaches, particularly for patients who are not suitable candidates for traditional open surgery in Ascending aorta and arch aortic.
The main research contributor in the region is Brazil, with several case reports and large cohorts. Among their isolated casuistry, we remark on the endovascular treatment of an ascending aorta pseudoaneurysm in a 32-year-old female patient who had undergone lung transplantation with extracorporeal membrane oxygenation (ECMO) support. The pseudoaneurysm was limited to the 0 zone (5 × 37 × 31 mm, defect distancing 30 mm from the coronary arteries and 33 mm from the brachiocephalic trunk), and traditional open repair was denied due to their higher risk. The endovascular approach was performed using an aortic cuff extension graft [34 × 42 mm], which resulted in the successful exclusion of the aneurysm. This study emphasized the feasibility of using endovascular techniques for complex aortic pathologies with a significant reduction in surgical risk. 1
In addition, a case of a 71-year-old male with a large aortic arch aneurysm (76 mm) and previous acute Stanford type A aortic dissection repaired with open ascending aorta replacement 10 years ago. Despite their higher mortality risk, the team performed a totally percutaneous endovascular repair using both axillary arteries, the left common carotid artery, and the right femoral artery. The use of the chimney graft technique to preserve the supra-aortic branches proved successfully supported by a Thoracic Endovascular Aortic Repair (TEVAR), stent grafts of 100 and 150 mm (left common carotid and left subclavian arteries) and 16 × 135 mm for the brachiocephalic trunk. This case remarked the highly complex procedures percutaneously speak to the growing technical capabilities within the Brazilian region. Although the case was singular, the technique’s feasibility, as reported in this and other studies, is anticipated to become more common with further advancements. 2
A Brazilian study of Physician-Modified Endovascular Grafts for Zone-2 Thoracic Endovascular Aortic Repair by André B. Queiroz et al. demonstrated the feasibility and early success of physician-modified endovascular grafts (PMEGs) for aortic arch disease in zone 2, ensuring left subclavian artery patency (LSA). All cases achieved immediate technical success without Type-I endoleaks or LSA occlusion at 30 days. These findings suggested that PMEGs may reduce complications associated with standard TEVAR on aortic arch territories. 3
Another challenging case from Brazil involved assessing the feasibility of combining endovascular repair of ascending aorta pseudoaneurysms with coronary stent implantation in a single procedure. A 56-year-old patient with a history of CABG [left internal mammary artery patent and vein grafts occluded in the right coronary position] and previously treated mediastinitis. The patient developed a small pseudoaneurysm in the mid-ascending aorta a few months later (29 mm in diameter and 8.5 cm distance from the coronary ostia to the brachiocephalic trunk). The successful endovascular approach entailed two abdominal aortic cuff extensions (31.5 mm × 45 mm) and three stents in the right coronary artery. The integration of coronary stenting with aortic repair is a novel and time-efficient strategy, particularly beneficial for patients with concurrent coronary artery disease and aortic pathology. While the sample size was small, this dual approach is being considered for broader clinical adoption. 4
On the other hand, Marcelo Ferreira et al. propose several endovascular approaches for aortic arch conditions supported by a new technique using a custom-made multi-branched arch endograft that features three inner branches. This innovative strategy’s use of only upward-facing inner branches allowed the procedure to be performed via a single transfemoral approach, bypassing the need for additional surgical access. This modification of traditional approaches simplifies the procedure, minimizes patient risk, and improves procedural outcomes. Although still early in its application, the technique has the potential to expand the applicability of endovascular treatments for aortic arch pathologies. 5 Furthermore, another Brazilian group and many Latino-American countries, many times, prefer a hybrid approach for managing aortic diseases that combines traditional aortic arch debranching with endovascular stenting from the aortic arch and descending aorta (TEVAR). Their higher applicability achieves a significant volumetric reduction of aneurismatic conditions, with a median volume shrinkage of 9.3%. The follow-up data indicated that no patient required reintervention within 300 days, and only 66% had freedom from reintervention at 600 days. This approach offers a promising and friendly strategy for treating complex aortic pathologies, particularly in high-risk patients. 6
In countries like Colombia, the presence similar individual cases where patients with an ascending aorta pseudoaneurysm in the third mid, resulting from coronary artery bypass surgery. This case required emergent repair with a thoracic aortic stent graft (34 mm × 52 mm) for percutaneous endovascular repair, which led to a successful outcome with no recurrence of symptoms at one-year follow-up. 7 Likewise, in Argentinean casuistry, the use of chimney stent grafts for aortic arch aneurysm repair in a high-risk surgical patient with previous coronary and ascending aorta surgery was reported. This case included the successful use of a TEVAR (40 mm × 210 mm), double chimney graft implantation (brachiocephalic trunk, 20 × 56 mm and left common carotid, 9 mm × 100 mm), and left common carotid artery to left subclavian artery extraanatomical bypass. The follow-up demonstrated that a moderate type I endoleak was resolved within 2 years. This case highlighted the complexity of endovascular aortic arch repair and the effectiveness of chimney grafts in preserving vital blood flow to critical branches, especially in patients with left internal mammary artery patents. 8
An interesting Chilean retrospective study on the use of inner branch arch endografts in the management of non-standard supra-aortic target vessels. 83% of patients had a previous type A aortic dissection, 42% with a thoracic or thoracoabdominal aortic aneurysm associated, and 33% with an arch aneurysm. Likewise, it showed that 71% had complications related to the innominate artery, including dissection and short landing zones. The technical success rate was 100%, and seven patients required reinterventions during follow-up, mainly due to continuous false lumen perfusion and endoleaks. This study indicates that the use of inner branch endografts is a feasible approach for managing complex aortic arch pathologies, with promising early and mid-term outcomes.
9
In other Latin American countries, there are neither publications nor evidence of surgical experiences related to treatments for the ascending aorta or aortic arch; however, a remarkable experience was recorded in Peru with the novel aortic arch stent graft system, which was successfully implanted for the first time in Latin America. The patient presented with a Type A aortic dissection, leading to a favorable postoperative outcome. This achievement marked a significant milestone in the advancement of endovascular surgery in both Peru and Latin America (Figure 1). First successful implantation of an aortic arch stent graft system in Latin America: A milestone in endovascular surgery.
While ascending aorta and aortic arch techniques show great promise, additional validation through multicenter studies is necessary to assess their long-term safety and efficacy across diverse patient populations. Moreover, expanding regional research initiatives and promoting institutional collaboration will be crucial for optimizing outcomes in our Latino-American community.
Thoracoabdominal aorta
The management of thoracoabdominal aortic conditions across Latin America shows unique challenges due to the diversity in healthcare systems, technology access, and medical expertise. Several studies from countries such as Colombia, Argentina, Chile, Brazil, and Peru remark on insights linked with current practices regarding approaches to the thoracoabdominal aorta.
In Colombia, the Marfan Syndrome (MFS)-related aortic disease at the Fundación Cardioinfantil-La Cardio was evaluated for 17 years and 50 patients underwent 56 aortic interventions (70% aneurysms vs 30% dissections). The thoracoabdominal aneurysm repair was 8.92% of cases. It showed a low in-hospital 30-day mortality rate of 4% and a reintervention rate of 17%. These results underline the importance of developing effective follow-up programs to reinforce high survival rates and early detection of complications after surgical treatment for MFS-related thoracoabdominal aortic conditions. 10
In addition, the application of 3D printing for surgical planning and treatment of thoracoabdominal aortic aneurysms has shown promise in Latin America, especially in Colombia and Peru.11,12 A study introduced a low-cost digital toolkit for preoperative planning and sizing in Endovascular Aortic Repair (EVAR) for Abdominal Aortic Aneurysms (AAA). The use of 3D printing allowed a cost-effective, patient-specific approach to planning EVAR, with cheaper models and a manufacturing time of less than 24 h. This method provided an acceptable error margin of 2.61% and improved surgical outcomes in a region with limited access to advanced technologies. 11
In Argentina, the management of complex aortic aneurysms has evolved with the introduction of standard, fenestrated, and branched endografts. Mariano Ferreira et al. reviewed 50 cases with Fenestrated Endovascular Aneurysm Repair (FEVAR), Branched Endovascular Aneurysm Repair (BEVAR), and Chimney Endovascular Aneurysm Repair (ChEVAR). The study remarked the technical success rate of 100%; however, 6% of patients died within 30 days post-surgery, and complications such as renal artery occlusion and endoleak were observed during follow-up. The overall survival rate at 1 year was 88.6%, demonstrating that these advanced techniques are viable for treating complex aortic pathology in Argentina. On the other hand, EVAR in octogenarians was associated with a lower perioperative mortality rate compared to open repair, supporting the advantages of the minimally invasive approach in this vulnerable group. Additionally, the long-term follow-up results showed a promising survival rate, with patients exhibiting favorable outcomes in terms of quality of life and aneurysm-related mortality in the Argentine population.13–15
A Brazilian nationwide study examined data over 11 years, covering 13506 cases of AAA repairs. EVAR was predominant, especially in emergency cases, and associated with lower mortality rates, unlike open repair [13.8% vs 52.1]. These findings suggest that EVAR is increasingly favored due to its lower mortality and shorter recovery times, reflecting a global shift in treatment trends. 16
Chile’s experience with Infective Native Aortoiliac Aneurysms (INAA) provides another perspective on the management of aortic pathologies in Latin America. They analyzed 35 patients and revealed that 57.1% of patients were treated successfully by endovascular treatment. The study highlighted the challenge of treating these rare but severe conditions, noting that early mortality was 14.2% and overall survival at 5 years was 50.9%. Endovascular treatment offered comparable survival outcomes to open surgery, and it may offer a safe alternative in this context. 17
In Peru, a study compared the outcomes of EVAR and open repair for Unruptured Infrarenal Abdominal Aortic Aneurysms (UIAAA). The study included 251 patients and demonstrated that while the short-term mortality was lower in the EVAR group (0% vs 2.92% in open repair), long-term survival was comparable. However, the EVAR group experienced a higher rate of reinterventions, particularly due to endoleaks, with a reintervention-free survival rate of 47.82% at 5 years. These findings align with global trends, indicating that while EVAR offers reduced short-term mortality, the long-term need for reinterventions remains a significant challenge. 18
These studies collectively highlight the growing role of advanced endovascular techniques, particularly in managing thoracoabdominal aortic aneurysms. The evidence from some Latin American countries underscores the importance of tailored, patient-specific approaches in improving surgical outcomes. Despite challenges such as the need for follow-up interventions and the complexities of treating complex aneurysms, the region is making significant strides toward more effective and accessible treatments for thoracoabdominal aortic diseases.
Treatment of main aortic endoleak complications
Type II endoleak
Aortic endoleaks remain a significant complication, and their management continues to evolve, with new techniques and strategies emerging across Latin America. Type II endoleak is considered the main cause of all aortic endoleaks and a lot of information is regarding it.
A recent Brazilian systematic review by Quilici Belczak et al. analyzed seven main studies involving 201 patients undergoing TEVAR with intentional LSA coverage. They identified that type II endoleaks had a prevalence of 21.7% and only 1% required an LSA coverage treatment. On the other hand, the findings revealed a low left-arm complication rate of 4.5%, with only 0.5% requiring revascularization due to subclavian steal syndrome. These findings suggested routine prophylactic LSA revascularization may not be necessary in elective TEVAR cases. 19
The presence of type II endoleaks in post-EVAR follow-up is a fascinating topic, and Latino-American evidence shows an incidence of 20–30%. These endoleaks will lead to aneurysm rupture and higher mortality associated when it is not opportunely treated. Some individual reports show the possibility of using computed tomography-guided percutaneous embolization in an aneurysm sac secondary to type II endoleak. A 90-year-old woman treated with EVAR presented an endoleak produced by the right lumbar artery patency. Their successful management was the direct puncture of the aneurysm sac via trans lumbar route guided by CT-fluoroscopy and its tip was directed to the origin of the lumbar arteries with a next injection of 3000 UI of human thrombin. This technique demonstrated a practicable, suitable, and minimally invasive alternative for a challenging type II endoleak situation. 20 On the other hand, a Mexican case report described a 102-year-old patient who underwent endovascular aneurysm repair (EVAR) and developed a type II endoleak-related rupture 12 years post-procedure. The patient underwent iliolumbar artery embolization, but the procedure was unsuccessful, necessitating an endograft extension. Despite achieving a technically successful outcome, the patient ultimately succumbed to respiratory complications. This case underscores the critical importance of lifelong surveillance in elderly EVAR recipients, highlighting that while timely embolization or endovascular techniques can offer promising results, they are closely linked to the patient’s quality of life and long-term surveillance. It emphasizes that careful monitoring is essential for detecting complications early and optimizing patient outcomes, particularly in this high-risk age group.
At the same time, another Latino-American 20-year prospective cohort study evaluated survival factors in 229 asymptomatic patients with AAA treated with EVAR. Among the patients, 80.3% had no endoleak, while 19.7% developed one (90% II type and 10% I, III, and IV). The study found that the 30-day mortality rate was 3.4%, and in multivariable analysis, the presence of an endoleak was an independent risk factor for survival (HR 2.23, 95% CI, 1.11–4.51, p < 0.05). Specifically, endoleaks were associated with higher mortality rates, underscoring the critical role they play in long-term patient outcomes. 21
A multicenter study conducted across Argentina, the USA, and Ireland analyzed 1555 aortic interventions, including 910 EVAR procedures, to evaluate evolving re-intervention strategies such as the EVAR GORE SalvAge Fabric Technique (ARAFAT), aortic sac double breasting with endograft preservation, and stent-graft explantation. The study also aimed to identify factors associated with endoleaks. A total of 9% of patients developed endoleaks, with 85% being type II, 6% type I, 5% type III, and 4% type IV. Among these, 4.84% required re-intervention, with ARAFAT being the most common approach, followed by fewer instances of double breasting and explantation. The mean duration from primary EVAR to EL detection was 53.3 ± 6.82 months, and the mean time to re-intervention was 70.20 ± 6.98 months. The mean sac size before primary EVAR was 6.00 ± 1.75 cm, increasing to 7.51 ± 1.94 cm after re-intervention. These findings emphasize the significance of graft preservation strategies, such as endovascular relining and aortic sacotomy, for managing concealed endoleaks, particularly in cases involving aortic hygroma 22
Type I endoleak
A Peruvian EVAR cases cohort showed a higher type I endoleak in close to 20% of cases; however, there are limited longer casuistry published related to type I endoleak in Latino-American aortic centers. 18 Individual cases associated with AAA are even more frequent. Type IB endoleaks, found in 3–10% of post-EVAR cases, require close monitoring as they pose a high risk of rupture. Endovascular reintervention remains the preferred treatment approach, as evidenced by a case involving a 79-year-old man with a 7.5 cm AAA. Initially, after EVAR using a bifurcated Treovance stent graft, a type IB endoleak from the right common iliac artery was promptly addressed with a stent extension, leading to successful aneurysm exclusion. However, 2 years later, the patient presented with abdominal pain, hypotension, and renal failure, and imaging revealed signs of an aortic rupture, aortic-left renal vein arteriovenous fistula (ALRVAF), and persistent type IB endoleak. The endoleak was linked to an insufficient sealing zone in the left iliac limb, potentially exacerbated by a graft hook penetrating the retroaortic left renal vein. A second EVAR was performed, addressing both the type IB endoleak and the ALRVAF. Post-procedure imaging confirmed complete aneurysm exclusion and renal function improved, demonstrating the importance of timely endoleak detection and intervention to prevent severe complications. 23
On the other hand, type IB endoleaks can typically be managed using endovascular techniques, such as coil embolization of the hypogastric artery or the deployment of additional stents or stent graft extensions, as mentioned previously. However, a hybrid procedure would offer substantial outcomes like a challenging case reported with a type IB endoleak at the distal end of a monoiliac conical stent graft used to treat an AAA extensively involving both common iliac arteries. A computed tomography scan revealed cranial migration of the endograft, leading to incarceration within the contralateral iliac aneurysm. The patient underwent a hybrid procedure combining both endovascular and limited open surgical techniques. To secure the proximal implantation site, a 26 mm balloon catheter was used. A Gibson incision was made to gain control over the iliac arteries, and an interpositional 8 mm regular Dacron graft was sutured end-to-end between the endograft and the external iliac artery. This approach effectively addressed the complex endoleak, ensuring successful repair. 24
An interesting Argentinian experience remarked that challenging anatomical conditions can increase the risk of EVAR complications, particularly type IA endoleaks. The ChEVAR technique has been proposed to address this issue by extending the sealing zone in patients with hostile neck anatomy. They compared EVAR in favorable anatomy with ChEVAR in hostile necks, evaluating outcomes such as type IA endoleak incidence, chimney occlusion, reintervention, migration, rupture, acute limb ischemia, sac growth, and aneurysm-related mortality over a median follow-up of 11.5 months. The ChEVAR group had a shorter neck length than EVAR (7.88 mm ± 5.73 vs 36.28 mm ± 13.73, p < 0.001). Despite the challenging anatomy, type IA endoleak incidence did not differ significantly between the two groups (p = 0.309). The same situation was identified in sac regression, reintervention rates, and other complications, including migration, rupture, acute limb ischemia, and aneurysm-related mortality. They suggested that ChEVAR is a viable alternative in anatomically complex cases, providing similar safety and efficacy to EVAR in favorable anatomies while mitigating the risk of type IA endoleaks. 25
Type III endoleak
A retrospective study evaluated the incidence and risk factors associated with endoleaks in patients who underwent EVAR at a single Latin American hospital. Endoleak incidence was assessed at 1-, 6-, and 12 months post-intervention using control tomography. Endoleaks were detected in 11% of patients, with type III in 2%. Although no significant associations were found between endoleaks and factors such as age, gender, smoking, COPD, or hypertension, an aortic aneurysm diameter exceeding 60 mm showed a trend toward statistical significance as a risk factor (30% vs 6%; p = 0.073). These findings highlight the importance of monitoring aneurysm size to anticipate endoleak risk after EVAR. 26
The management of this type of endoleak is a challenging situation, and many times, it is necessary to use another endograft. An Argentinian case report showed a patient previously treated with EVAR and large type III endoleak with aortic rupture, confirmed by computed tomography angiography. The initial treatment involved deploying an aorta-uni-iliac endograft (30 mm × 18 mm x 105 mm) within the existing stent graft, extending across the defect, followed by occlusion of the contralateral limb and creation of a femoro-femoral bypass. Despite initial technical success, a recurrent endoleak was detected at the aortic bifurcation. Given the presence of active infection and limited access options, a previously undescribed bilateral transradial access (TRA) approach was employed. It included the use of two extra stiff guidewires into the right limb of the first graft through the right and left radial arteries. Using the “bare on the wire” technique, simultaneous balloon angioplasty was performed with peripheral balloons (8 × 40 mm and 10 × 40 mm), achieving controlled low-pressure insufflations to effectively seal the defect. The decision to avoid placing a third stent graft was critical due to the risk of infection, and the innovative TRA approach successfully resolved the endoleak. Follow-up controls confirmed endograft patency and complete resolution of the endoleak. 27
Some Latin American vascular groups are trying to identify potential predictors related to the type IIIa endoleak approach. A retrospective cohort study evaluated patients undergoing EVAR and focused on the impact of changes in the aortic tortuosity index (TI) over time. The analysis included 173 patients, of whom 12.1% developed type IIIa endoleak. Kaplan–Meier analysis revealed cumulative freedom from this endoleak of 99.4%, 92.5%, 86.1%, and 83.3% at 1, 3, 5, and 8 years, respectively. The Contal and O'Quigley method identified a 0.03 increase in aortic TI and a 15 mm decrease in Device Components Overlap (DCO) as critical thresholds predicting endoleak occurrence. Multivariate analysis demonstrated that increased aortic TI (OR 4.56), DCO decrease >15 mm (OR 6.13), maximum preoperative aortic diameter (OR 1.09), smoking (OR 26.67), and initial DCO (OR 0.91) were significant risk factors (p < 0.05). These findings underscore the importance of vigilant long-term follow-up using tomographic imaging to monitor aortic TI and DCO in patients treated with anatomic fixation endografts. Early intervention is recommended when risk factors are present to mitigate the risk of type IIIa EL. 28
Conclusion
Latin America has made significant progress in aortic endovascular surgery, adopting advanced techniques and hybrid approaches despite resource limitations. The region has demonstrated innovation in managing complex cases, including endoleak repair through transradial access and graft preservation strategies. However, fragmented data and unequal access to technology hinder standardized care. To address these gaps, we propose the Latin American Aortic Registry (LATAR)—a multicenter initiative to track outcomes, identify regional trends, and promote collaboration (Figure 2). By pooling data from high-volume centers, LATAR will establish benchmarks, guide policy, and support training programs, ensuring the region’s continued integration into the global endovascular landscape. This registry will not only improve patient care but also position Latin America as a key contributor to aortic surgery innovation. Unified efforts through LATAR can transform challenges into opportunities, solidifying the region’s role in the aortic revolution. Latin America’s aortic revolution: Current practices and future directions with potential registry.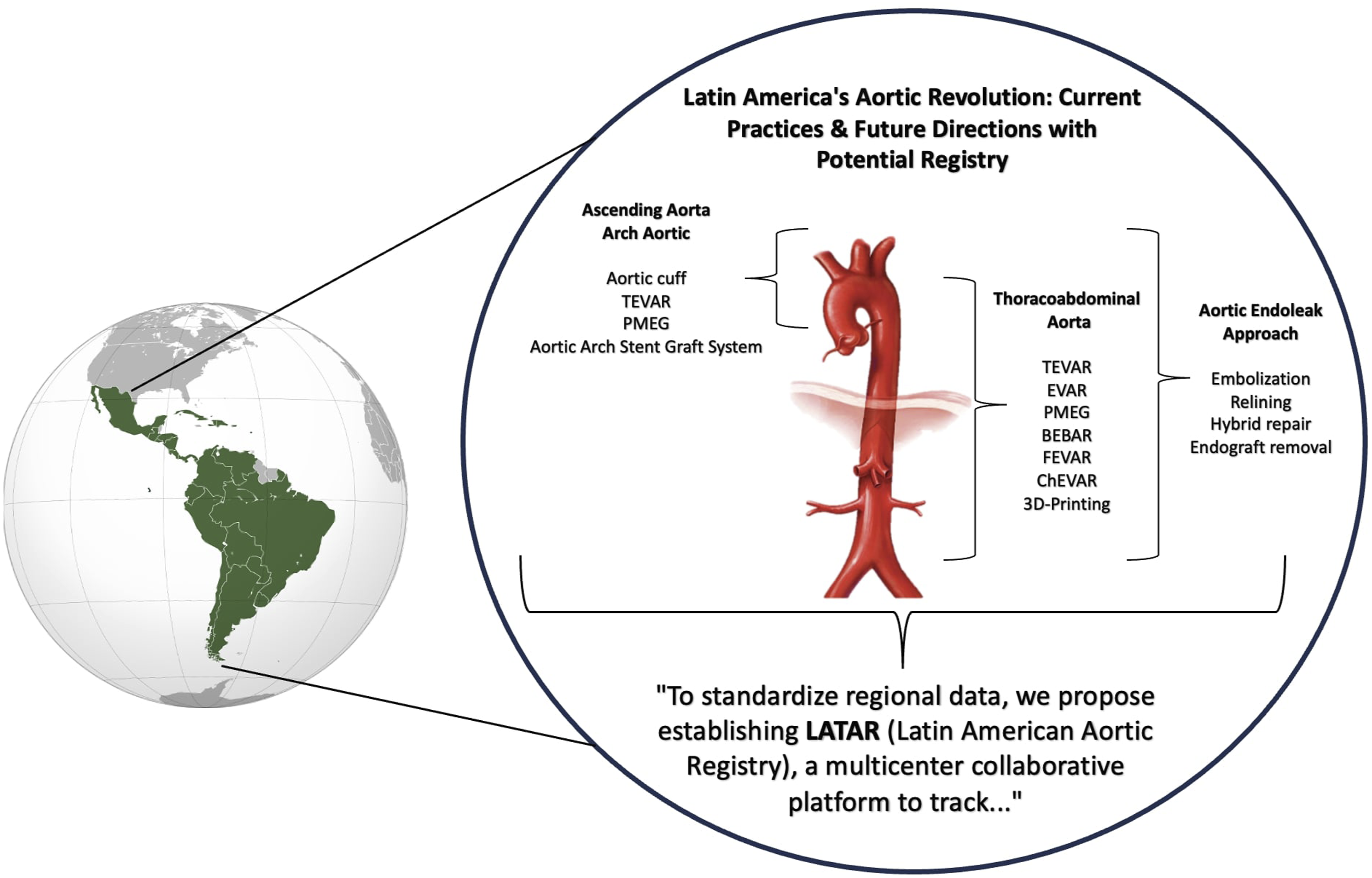
Footnotes
Author contributions
All authors contributed equally to the idea, data collection, drafting, and final approval of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.