
Abstract
Introduction
Spinal cord ischaemia (SCI) is a well-known complication of thoracic endovascular aortic repair (TEVAR), with reported incidence rates ranging from 2.5% to 11%. 1 Risk factors include extended aortic coverage, 1 emergency operation, previous aortic surgery, perioperative hypotension, and reduction in spinal cord perfusion pressure. 2 Haemodynamic stabilization and drainage of cerebrospinal fluid are the main treatment strategies for paraplegia after TEVAR. 3 More innovative approaches such as staged segmental artery embolization and neurological monitoring of collateral network have been proposed. 4 Most of these treatment options are invasive and require intensive monitoring. Pharmacological adjuncts, including corticosteroids, to reduce ischaemic damage to neuronal cell membranes; naloxone, to lessen the release of excitatory neurotransmitters; and mannitol, to reduce intraspinal pressure, have been presented, but their effectiveness as rescue therapies has not been well-established. 5
We report a patient who developed two episodes of delayed paraplegia on days 8 and 13 after TEVAR associated with hypotension. The first episode of delayed paraplegia was effectively treated with lumbar cerebrospinal fluid drainage, and the second episode was successfully reversed with phenylephrine and then midodrine, an oral alpha 1-adrenoreceptor agonist. This drug is typically prescribed for treatment of postural hypotension.
Case presentation
A 73-year-old man with multiple medical comorbidities, including hypertension, hyperlipidaemia, diabetes mellitus, and chronic renal impairment with a baseline creatinine of 150 umol/L, was admitted to his local hospital for sudden onset right-sided abdominal pain and shortness of breath. Physical examination in the Accident & Emergency Department showed reduced air entry over right chest and abdominal distension. Blood tests revealed a haemoglobin level of 12.9 g/dL, a white cell count of 28.4 ×109/L, and deranged renal function with a creatinine level of 302 umol/L. Creatine kinase was grossly elevated while troponin T level remained normal. No microorganism was identified in blood or sputum culture. Initial chest radiography showed right pleural effusion, the patient was treated as chest infection with empirical amoxicillin and clavulanate (Augmentin), subsequently stepped up to meropenem.
In view of pleural effusion and persistent abdominal pain and distension, an early computed tomography of the thorax, abdomen, and pelvis was performed 16 days after admission. It showed a 7.5 cm suspected mycotic thoracic aortic aneurysm (Figure 1(a)). The patient was transferred to our institution, a tertiary referral vascular centre, for specialist management. He had severe pain and was hypotensive on arrival to our institution, an emergency TEVAR was therefore performed. On-table aortogram showed a 7.5 cm ruptured descending aortic aneurysm above the paravisceral segment from T9 to T11 level (Figure 1(b)). In order to have good proximal and distal landing zones to exclude the aneurysm, a stentgraft (ZTA-PT-34-30-161, Cook Medical, Bloomington, USA) was deployed from T6 with distal landing zone 7.5 mm proximal to the celiac axis (Figure 1(c)). Completion aortogram demonstrated successful exclusion of the aneurysm sac with no evidence of endoleak, and the procedure was uneventful. Postoperatively, the patient was nursed in a high-dependency unit with close monitoring. His back pain improved, he remained afebrile with stable haemodynamics, full motor, and sensory functions in all limbs, and was discharged to general ward on postoperative day 2. Subsequent pleural drainage yielded blood-stained fluid, culture was negative for aerobic and anaerobic organisms, as well as acid-fast bacilli, and cytology showed no malignant cells. At the recommendation of microbiologists with a suspected mycotic aneurysm, he required a 4-week course of intravenous ceftriaxone and vancomycin, followed by lifelong oral cotrimoxazole. (a) Pre-operative CT showing a 7.5 cm suspected mycotic thoracic aortic aneurysm of the descending thoracic aorta. (b) Emergency operation and on-table aortogram showing the aneurysm extended from T9 to T11 level). (c) A stentgraft was deployed to exclude the aneurysm with good proximal and distal landing zones. (d) Postoperative CT scan showing successful treatment of the thoracic aneurysm with no endoleak.
On postoperative day 8, after a period of sitting out on a chair in the ward, he developed sudden onset bilateral lower limb paraesthesia and weakness with power of 2 out of 5. He was transferred back to high-dependency unit for close monitoring with arterial line and hourly neurological observation. Bilateral lower limb pulses were all palpable. Blood pressure at that time was 92/50 mmHg (Figure 2(a)). Urgent computed tomography showed no intracranial pathology, the aneurysm was successfully treated as evidenced by the interval reduction of sac size and absence of endoleak (Figure 1(d)). The patient was evaluated by neurosurgeons and orthopaedic surgeons. In view of a low mean arterial pressure of 70–85 mmHg, an emergency spinal drain was inserted by neurosurgeons and was kept at bed level; daily output was around 200 mL. Lower limb strength gradually improved and was completely recovered 10hours later. The spinal drain was elevated 5 cm per day with no recurrence of lower limb symptoms. It was reviewed by neurosurgeons and removed 3 days later. Blood pressure charts taken as patient developed first (a) and second (b) episode of delayed paraplegia.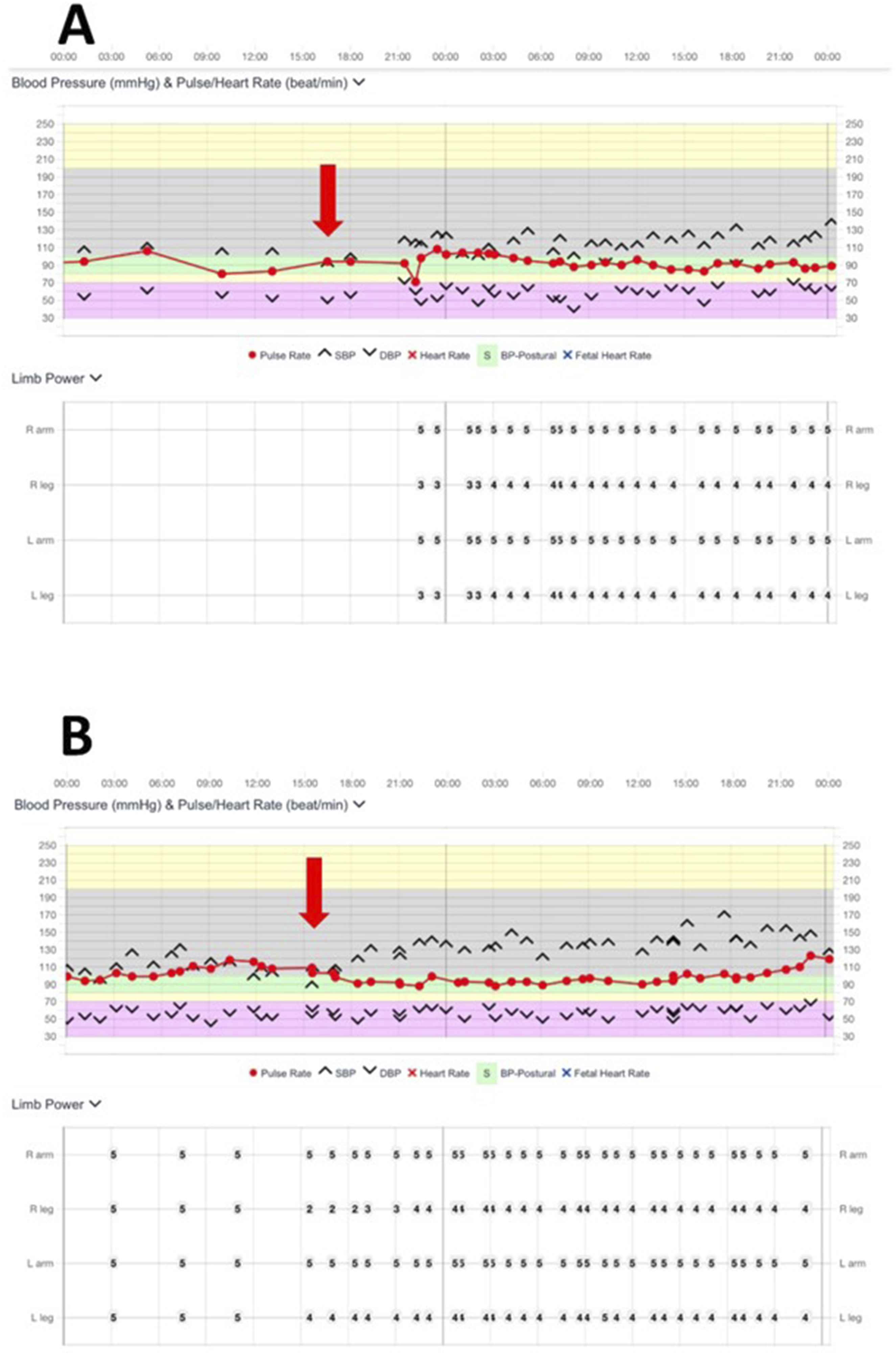
However, 1 day after spinal drain removal (postoperative day 13), patient complained of another episode of bilateral lower limb numbness and weakness after sitting out, with lower limb power of 2 out of 5. The patient experienced transient hypotension with blood pressure of 90/55 mmHg at that time (Figure 2(b)). Neurosurgeons were consulted, close monitoring and maintenance of systolic blood pressure between 120–140 mmHg was recommended prior to considering repeat spinal drain insertion. Phenylephrine was commenced promptly at 0.25 mcg/kg/minute, and blood pressure was optimized within 2 h from onset of paraplegia. With systolic blood pressure maintained above 120mmHg, lower limb power gradually improved and completely recovered 7 hours later. A cerebrospinal fluid (CSF) drain was therefore not required. Patient was kept in high-dependency unit with phenylephrine support to maintain blood pressure.
Midodrine is an alpha 1-adrenoreceptor agonist commonly used to treat postural hypotension. It is hydrolyzed to form its active metabolite, desglymidodrine, after oral administration. Oral midodrine 2.5 mg TDS was initiated on postoperative day 15 concurrently to maintain the systolic blood pressure. Phenylephrine was slowly weaned off over 3 days after commencing midodrine. Patient’s systolic blood pressure maintained at 120–140 mmHg with midodrine alone and was discharged to general ward. The patient achieved complete neurological recovery and walked well.
Midodrine was weaned off 1 month later when patient’s blood pressure stabilized. Patient walked well without lower limb weakness. He was discharged from hospital after completing course of intravenous antibiotics, and was kept on lifelong oral cotrimoxazole for his mycotic aneurysm.
Discussion
We report the use of midodrine to reverse paraplegia induced by transient hypotension secondary to post-TEVAR spinal cord ischaemia (SCI).
Post-TEVAR SCI was defined as postoperative neurological deficit of the lower limbs, including paraesthesia, paraparesis, and paraplegia, not attributable to other causes. 6 The onset time of neurological deficits ranged from 0 to 229 h (median 10.6 h). Delayed-onset SCI was defined as development of postoperative neurological sequelae after initial intact neurological functions. 7 Ullery et al. 8 reported that patients with delayed SCI demonstrate better prognosis and were more likely to experience functional improvement compared to those with immediate SCI, despite comparable life-expectancy. 8 Patients with TEVAR were more likely to experience delayed SCI, compared to those undergoing traditional thoraco-laparotomy.8,9
The aetiology for delayed SCI is multi-factorial, but relative hypotension in patients with tenuous spinal cord blood supply after TEVAR seems to be an important contributing factor. 10 It is known that spinal cord perfusion pressure is the difference between mean arterial pressure (MAP) and intraspinal pressure (ISP). The cornerstone for treatment of delayed SCI includes early and accurate diagnosis, maintenance of spinal cord perfusion pressure, and improvement of oxygenation. 11 A case report of SCI in Philadelphia demonstrated the causal relationship between transient hypotension and lower extremities paraesthesia and paralysis, in which symptoms were immediately reversible by inducing hypertension with phenylephrine and norepinephrine. 12 Another case report, also from Philadelphia, exhibited striking similarity to the present case. The patient in that report presented with ruptured thoracic aortic aneurysm and underwent emergent TEVAR, subsequently developed delayed SCI 3 days later, associated with orthostatic hypotension while getting out of bed. The episode was reversed with phenylephrine, norepinephrine and vasopressin. Yet, the patient experienced a second episode of bilateral lower limb weakness upon weaning of inotropic support, requiring emergent placement of a lumbar drain. 13 Both episodes of hypotension in our patient were similarly related to sitting out from bed, suggestive of orthostatic hypotension inducing SCI. These cases demonstrated that both active blood pressure management to increase MAP and lumbar drainage to decrease ISP act jointly to reverse SCI.
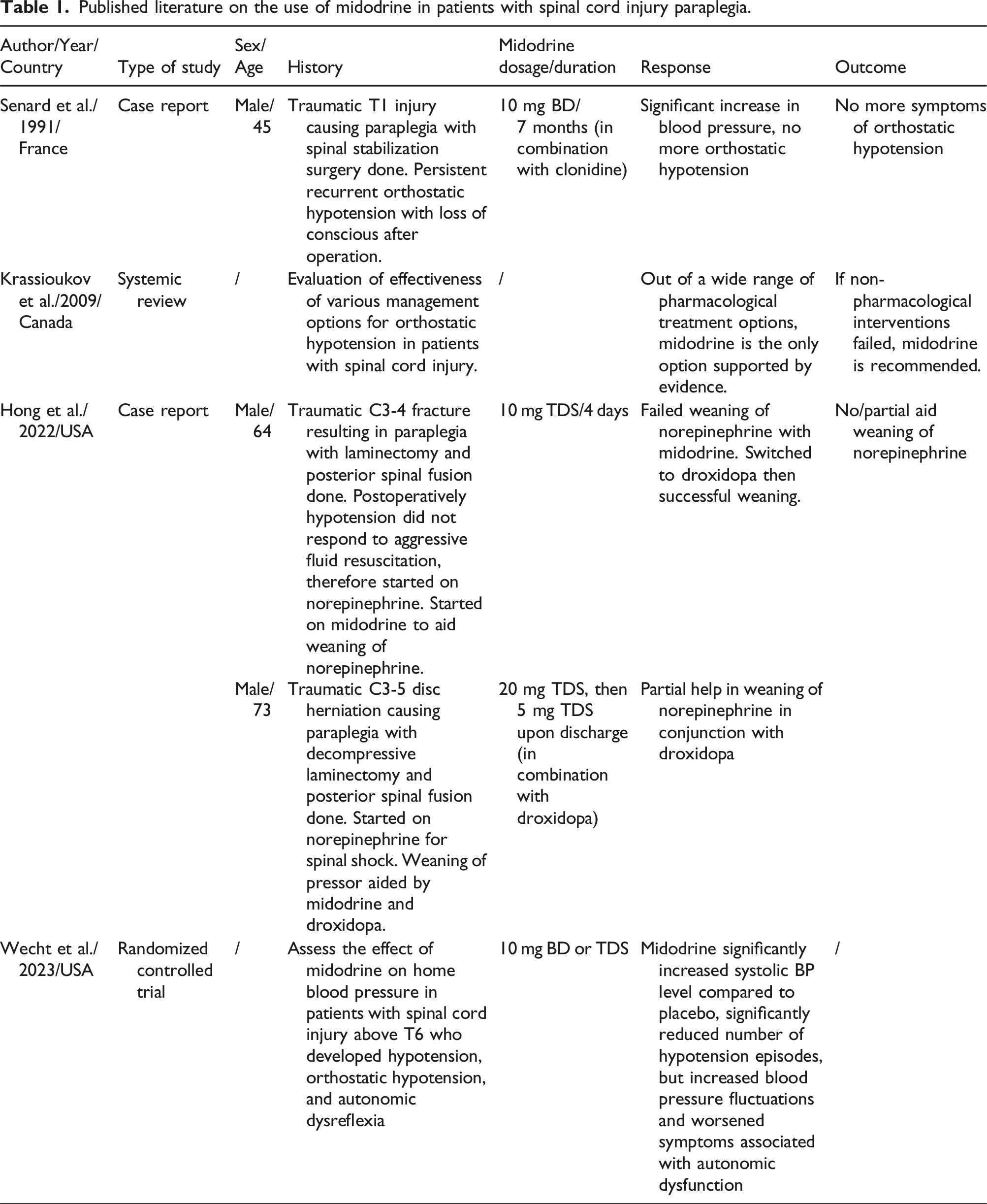
Published literature on the use of midodrine in patients with spinal cord injury paraplegia.
Midodrine was proven to effectively increase MAP. 15 Additionally, multiple studies have shown that midodrine improves cerebral perfusion or cerebral blood flow in patients with autonomic dysfunction and orthostatic hypotension secondary to high spinal cord injury.14,16–18 For the same principle, it is believed that midodrine, through increasing mean arterial pressure and in turn spinal cord perfusion pressure, could improve spinal perfusion and alleviate, or even reverse, symptoms of SCI. However, no prior studies have directly measured the effect of midodrine on spinal perfusion.
This is the first paper to report the use of midodrine as an adjunctive rescue therapy for a patient who presented with two episodes of delayed paraplegia after TEVAR associated with transient hypotension. The second episode was completely reversed through prompt blood pressure management with the aid of oral midodrine. Further studies are required to establish the effectiveness of midodrine in improving spinal perfusion, but this oral medication appears to be a safe and non-invasive treatment for paraplegia in patient post-TEVAR.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Consent for publication
The patient gave full written consent for this paper to be published.