
Abstract
Introduction
Implantation of a gestational sac in a previous Caesarean section scar of the lower uterine segment is a rare form of ectopic pregnancy.
Case report
We report a case of Caesarean scar ectopic pregnancy in a 25-year-old female, diagnosed by ultrasonography and confirmed by magnetic resonance imaging. We present the clinical details, imaging findings, and management of the patient.
Discussion
Imaging plays an important role in the diagnosis of ectopic pregnancy and ultrasonography is the modality of choice. Ultrasonography features of scar ectopic pregnancy include empty uterus and cervix with normal endometrium and endocervical canal, gestational sac (with embryo and/or yolk sac) in the anterior part of the lower uterine segment in the region of the Caesarean scar with a thin myometrial layer between the bladder wall and gestational sac. Magnetic resonance imaging may be used as an adjunct imaging modality in cases with inconclusive or equivocal sonographic findings. Termination of pregnancy in the first trimester should be considered and treatment options should be individualized as there is no universal agreement on the best or most preferred treatment modality.
Conclusion
Awareness of specific ultrasound features of scar ectopic pregnancy is crucial for early recognition, correct diagnosis, and initiating prompt management to prevent complications.
Keywords
Introduction
Caesarean scar pregnancy (CSP) is a rare complication of pregnancy after Caesarean delivery, in which the gestational sac (GS) is implanted in the anterior wall of the lower uterine segment in a previous Caesarean scar. 1 It is the rarest form of ectopic pregnancy reported in only 0.15% of pregnant women with a history of Caesarean delivery. 1 Its incidence is increasing with the rise in Caesarean sections and early detection with the widespread use of ultrasonography (USG) and magnetic resonance imaging (MRI). This condition is associated with life-threatening complications such as hemorrhage, uterine rupture, abnormal placentation, and even maternal death if not managed properly. Early diagnosis is usually made by USG and can be confirmed by MRI, which helps in prompt treatment. We present a case of CSP detected in a symptomatic woman in early pregnancy and highlight the key imaging features.
Case report
A 25-year-old woman (Gravida 3, Para 2) presented after 10 weeks amenorrhea to her obstetrician complaining of intermittent vaginal bleeding for three days. The symptoms had worsened one day prior to admission with intermittent lower abdominal pain. She had a past history of two Caesarean sections. On examination, her vital signs were stable and she had no abdominal tenderness. The cervical os was closed with minimal blood in the vagina. Her urine pregnancy test was positive and serum beta-hCG measured 35,000 mIU/mL. Remaining laboratory values (complete blood count, liver function test, kidney function test) were within normal limits.
Transabdominal sonography (TAS) revealed an anteverted uterus with a GS in the anterior myometrium of the lower part of the uterus in the region of isthmus. Heterogeneous echoes in keeping with blood clots were seen in the endometrial cavity and the cervical canal was empty (Figure 1(a)). Doppler examination showed increased vascularity in the hyperechoic rim of choriodecidual reaction and anterior myometrium (Figure 1(b)). On transvaginal sonography (TVS), the myometrium anterior to the GS and adjacent to the urinary bladder was thin (Figure 2(a)). A live embryo of crown-rump length (CRL) 26.2 mm corresponding to nine weeks three days was seen (Figure 2(b)). No adnexal abnormality was identified. These sonographic findings with a history of previous Caesarean sections were considered highly suspicious for Caesarean scar ectopic pregnancy.
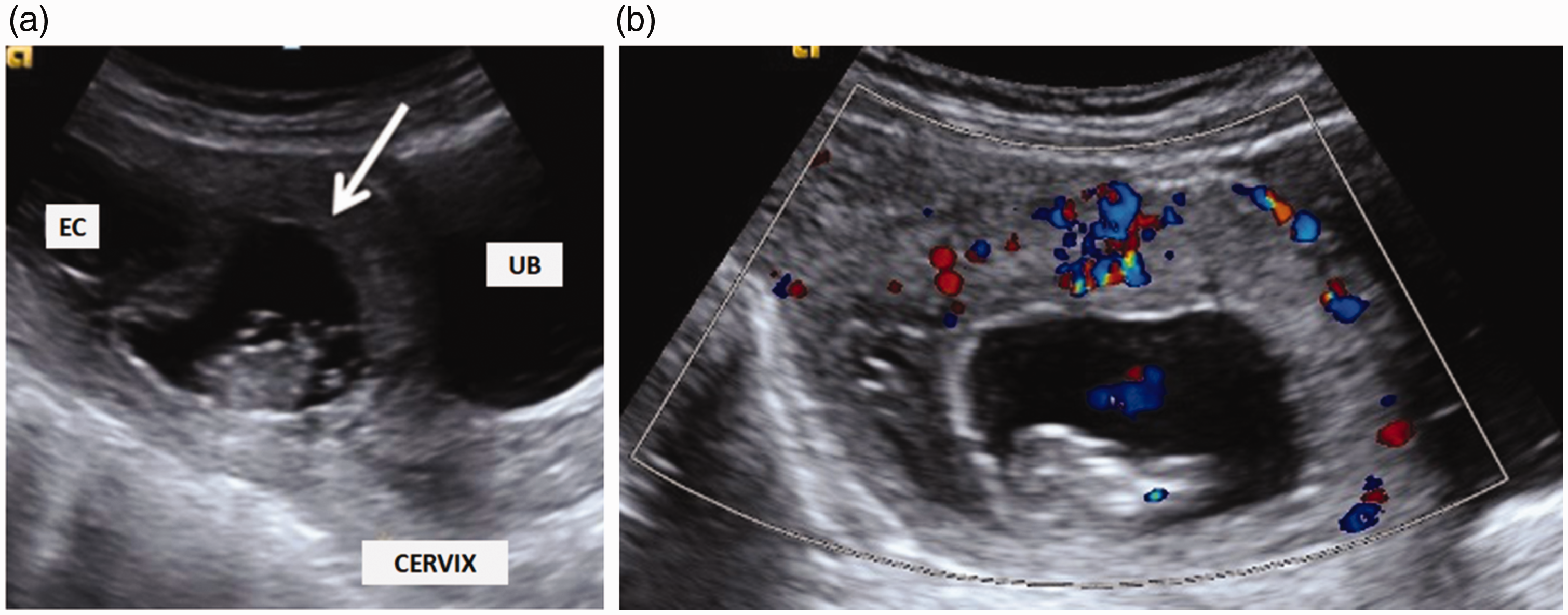
Transabdominal sonography sagittal image (a) showing the gestational sac with embryo in anterior myometrium of the lower uterine segment (white arrow). The cervical canal is empty, whereas the endometrial cavity (EC) is distended with heterogeneous blood clots. Color Doppler image (b) showing increased vascularity in the hyperechoic choriodecidual reaction and color flow within the embryo.

Transvaginal sonography image (a) showing peripheral choriodecidual reaction with thinning of anterior myometrium anterior to the gestational sac (white arrow) adjacent to the urinary bladder (UB). The echogenic anterior trophoblastic tissue is visualized under the thin myometrium. Transvaginal sonography image (b) showing a well-formed embryo with CRL measurement corresponding to nine weeks three days.
MRI was requested on the following day by the treating obstetrician for confirmation and planning the management. MRI pelvis was performed in a 3.0-T MRI scanner (Siemens Healthineers AG, Erlangen, Germany). The study confirmed a GS bulging into the anterior myometrium of the uterine isthmus at the scar site of the previous Caesarean section with thin myometrium between the urinary bladder and GS (Figure 3(a) and 3(b)). Posteriorly, the GS was seen extending into the endometrial cavity in the lower uterine segment. The posterior myometrium was of normal thickness. There was no obvious invasion of the urinary bladder wall. The endometrial cavity in the upper uterine segment was distended with heterogeneous blood products and the cervical canal was empty.

Sagittal T2-weighted MR image (a) showing a gestational sac bulging through the anterior myometrium of the lower uterine segment in the region of previous Caesarean section scar. The gestational sac with embryo is surrounded by a good decidual reaction. The posterior aspect of the sac extends into the endometrial cavity of the lower uterine segment. Anterior to the gestational sac, the myometrium is markedly thinned (white arrow). There is no placental invasion of the urinary bladder. Axial T2-weighted image (b) through the pelvis showing gestational sac and surrounding decidual reaction with a thin rim of myometrium covering the anterior aspect of the gestational sac (thick white arrow). The posterior myometrium shows good wall thickness (thin white arrow).
The patient was managed by systemic methotrexate (MTX) followed by laparotomy and excision of the gestational mass. The intraoperative finding revealed a GS within the anterior uterine wall at the site of the Caesarean section scar with a very thin myometrial wall (Figure 4). Resection of the old scar followed by new uterine closure was done to reduce the risk of recurrence.

Intraoperative photograph of the same patient showing the gestational sac along the anterior wall of the lower uterine segment at the site of Caesarean section scar with a thinned myometrial wall.
Discussion
The first case of CSP was reported in English medical literature in 1978. 2 Currently CSP has increasing occurrence with the rise in Caesarean deliveries. The estimated incidence is now 1 per 1800–2226 pregnancies, more than that of cervical ectopic pregnancies.1,3,4 Though its pathophysiology is unclear, it has been postulated that the anterior lower uterine segment has poor vascularity that impairs post-Caesarean healing in some women and is vulnerable to the formation of small dehiscent tracts and defects in which a trophoblast can implant.4,5 Although myometrial defects are most often the result of prior Caesarean section, scar pregnancies have also been reported after other uterine interventions, including dilatation and curettage (D&C), myomectomy, hysteroscopy, and metroplasty.2,3,5 Up to 50–72% of CSPs occur in women who have had two or more Caesarean sections.4,6 There are varied opinions regarding the risk of CSP development and its relation to the number of previous Caesarean sections. Some believe that women undergoing multiple Caesarean sections are at increased risk of scar implantation due to increased scar surface area. 4 However, others do not support this concept.3,7,8
Clinical presentation of CSP often includes vaginal bleeding and abdominal pain, but there may be no symptoms. Severe acute abdominal pain or heavy vaginal bleeding are concerning for impending rupture, while hemodynamic instability may indicate the rupture of CSP through the myometrium. CSP can present at any time during gestation; presentation and management depend on the degree of implantation abnormality. Scar pregnancies with minimal or absent overlying myometrium are typically diagnosed in the first trimester and carry an increased risk of hemorrhage and uterine rupture.1–3,6 Lin et al. retrospectively reviewed 109 patients with CSP and categorized them into four grades based on the ultrasound appearance. Grade I CSP indicated the GS embedded in less than one-half thickness of the lower anterior myometrium; and grade II CSP represented the GS extended to more than one-half thickness of overlying myometrium. Grade III CSP implied the GS bulged out of the Caesarean scar, and grade IV CSP denoted that the GS became an amorphous tumor with rich vascularity at the Caesarean scar. They demonstrated a significant association between the invasiveness of the surgery and degree of ultrasound detected implantation abnormality with the majority of higher grade CSP requiring hysterotomy or hysterectomy. 9
TAS being readily accessible in most primary clinical settings is the first-line investigation. It provides a panoramic large field of view. TVS gives a detailed relationship of the GS with Caesarean section scar and endometrial cavity. TVS remains the imaging modality of choice for diagnosis of CSP in the first trimester.2–4 A sagittal view along the long axis of the uterus through the plane of the GS allows accurate localization within the anterior lower uterine segment.2,5 The following sonographic criteria have been proposed for diagnosis of CSP:2,4,10–14
Empty uterus with normal endometrium Empty cervix with normal endocervical canal GS seen in anterior part of lower uterine segment in the region of Caesarean scar Thin myometrial layer between bladder wall and GS (<5 mm) Presence of embryo with or without cardiac activity and/or yolk sac in GS Increased peritrophoblastic vascularity at the area of Caesarean scar on Doppler evaluation
CSP needs to be differentiated from cervical pregnancy and incomplete miscarriage.2,4,13,14 In cervical pregnancy, ultrasound will show a thick myometrium between the maternal bladder and GS, together with the ballooned cervical canal, giving rise to an “hourglass” appearance of the uterus. 14 In incomplete miscarriage, the internal os is usually open and there is no trophoblastic flow; whereas in CSP, the internal os is always closed and the GS appears well-perfused on Doppler examination. 4
The incidence of abnormally invasive placentation resulting in CSP or placenta accreta is increasing because of the rising Caesarean section rate. Many authors have proposed that pathogenesis of placenta accreta and scar pregnancies are similar with the site and level of invasion being different.15,16 With placenta accreta, the placenta is abnormally adherent to the myometrium with the GS growing into the lumen of the uterus. A CSP is implanted entirely within the Caesarean scar and is surrounded by myometrium and fibrous tissue.2,5,15 CSP may be a precursor to second or third trimester placenta accreta, with the thickness of the scar, depth, and progression of invasion dictating the subsequent course.15,17 Sonographic signs of accreta may be evident in the first trimester. These include low lying GSs, with most appearing to be attached to the uterine scar with thinning of the myometrium as well as echolucent areas within the placenta and abnormal vascularity at the uterus–bladder interface.18,19 In early gestation, distinguishing placenta accreta from a CSP may be difficult as in our case due to similar imaging appearance, and they more likely form a continuum rather than separate entities with an overlap in the outcome and clinical management. 15 Diagnosis of placenta accreta is usually made in the second or third trimester and typical ultrasound findings include the absence of normal linear hypoechoic area between the placenta and the myometrium (retroplacental clear space), relatively bulky placenta with multiple sonolucent lacunae of turbulent flow, thinning of the retroplacental myometrium, and increased vascularity at bladder serosa interface. Early transvaginal ultrasound in all women with prior Caesarean sections should be considered to screen for developing placenta accretas or CSPs.15,17 This could be incorporated into the 11–14 week combined screening scan. 20 Although the placenta is evaluated routinely during fetal anatomic screening at 20 weeks, the placental site should be thoroughly assessed for signs of accreta especially in low anterior placentas overlying previous Caesarean scars.
MRI is used as an adjunct to ultrasound evaluation.2,15 It provides excellent soft-tissue detail with a comprehensive assessment of the uterine wall and peritoneal cavity. MRI is specifically indicated in cases with inconclusive or equivocal USG findings and in patients where placenta accreta cannot be excluded on ultrasound.8,13,21 T1- and T2-weighted images in axial and sagittal planes of the pelvis are used to confirm the presence of the GS in the lower uterine segment scar. Sagittal T2-weighted images are best for visualizing the scar, which appears as low signal. 21 T1-weighted imaging may be helpful in the detection of blood products in the canal and pelvis. MRI helps in determining the growth pattern of the GS (whether primarily within the scar or within the uterine isthmus). It also helps in the evaluation of placental location and assessment of relation to adjacent structures along with better delineation of the degree of myometrial thinning and bladder invasion. Thus additional information obtained from MRI helps the clinician to decide an appropriate management strategy. If surgical management is considered, MRI helps with better surgical planning and improves intraoperative orientation. In more advanced pregnancies, MRI optimally demonstrates findings of the placenta accreta spectrum. The dark, irregular intra-placental band with varying width and distribution on T2-weighted sequence primarily on the maternal side has a strong association with placentation abnormality. 22
CSP can be managed conservatively by medical treatments or surgically, but there is no standardized approach for its treatment.2,14,23,24 Management decisions are dictated by gestational age and size, severity of implantation abnormality, clinical stability, and patient’s desire for future fertility. 2 Early termination by conservative methods in the first trimester is preferred to preserve fertility and lower the risk of complication; however, there is no universal agreement on the best or most preferred treatment modality.2,14 Medical treatment options include systemic or local administration of MTX, local injection of embryocides-like potassium chloride into the GS, or a combination of both.2,23 Surgical options include combined medical treatment with surgical sac aspiration, D&C, hysteroscopic evacuation, laparoscopic and transvaginal resection, open hysterotomy with resection or hysterectomy.2,23 Another minimally invasive option is combined medical treatment with uterine artery embolization (UAE). 14 Other combined or sequential management options include UAE followed by dilatation and evacuation/surgical resection and MTX followed by surgical evacuation or resection after an interval. 23
Medical management with systemic MTX is the least invasive treatment and can be considered for hemodynamically stable women with minimal symptoms particularly in pregnancies of less than eight weeks of gestation and beta-hCG level less than 5000 mIU/mL.2,23 However, it requires a long period of follow-up for beta-hCG to decline to normal levels and for the gestational mass to resolve completely. Some authors have proposed to avoid systemic MTX as a single treatment of choice. 16 Intralesional injection of MTX (with sac aspiration) under ultrasound guidance has a higher success rate and can also be considered as an option for stable women. 23 UAE is more commonly used as a part of combination treatment in cases with risk of severe bleeding and should not be used as a primary treatment. 16
Surgical treatment should be considered for women with significant symptoms or failure to medical therapy. Some authors suggest D&C under ultrasound guidance as a management option in selected cases with gestational age less than seven weeks and sufficient communication of the GS with the endometrial cavity and no indication of deep sac implantation. 24 However, in other cases, uterine curettage as a primary treatment should be avoided as it is associated with profuse hemorrhage and high failure rate, consequently requiring more invasive operative interventions. 16 Therefore, it was not considered as a management option in our case with a relatively advanced gestational age. A hysteroscopic resection can be chosen for the CSP that grows inwards toward the uterine cavity (endogenous) and carries less risk of perforation, whereas surgical resection with resuturing should be considered for women with a deeply implanted CSP growing toward the abdominal cavity and bladder (exogenous).2,23 For surgical resection, a transvaginal or laparoscopic approach should be considered over laparotomy where facilities and expertise are available. 23 Laparotomy followed by wedge resection of the lesion (hysterotomy) should be considered in women with advanced gestation and in patients with failed conservative medical and/or surgical treatments. Moreover, with the excision of the old scar, this treatment modality avoids the possibility of leaving residual trophoblasts and removes the microtubular tracts, which may reduce the risk of recurrence. Our case was managed by systemic MTX followed by laparotomy and resection of the CSP. The treatment option chosen was considered to be the best for our case.
Birch Petersen et al. have evaluated as many as 14 different treatment approaches in their recent systematic review of 2037 CSP cases. 25 This retrospective literature review supported an interventional rather than medical approach for CSP management. Considering efficacy and safety, they recommended only five approaches for treating CSP, depending on availability, severity of patient symptoms, and surgical skills. These include (1) resection through a transvaginal approach, (2) laparoscopic resection, (3) UAE in combination with D&C and hysteroscopy, (4) UAE in combination with D&C, and (5) hysteroscopic evacuation. However, the safest and efficient clinical approach to CSP is still not determined and treatment options need to be individualized.
Conclusion
CSPs present unique diagnostic and therapeutic challenges. In recent times, there has been a relative increase in the number of Caesarean deliveries and associated complications. Early transvaginal ultrasound combined with the 11-14 week screening scan should be considered in patients with multiple prior Caesarean sections for precise localization of early pregnancies and to look for CSPs or developing placenta accreta. Early recognition by imaging and prompt diagnosis of CSP is critical to prevent maternal morbidity and mortality. The awareness of specific ultrasound features of uncommon locations of ectopic pregnancies, such as scar ectopic pregnancy, is crucial for making a correct diagnosis and initiating prompt management to prevent complications and preserve patient fertility. Termination of the pregnancy in the first trimester should be considered and treatment options should be individualized.
Footnotes
Acknowledgments
None
Contributors
S, MSS, and AG contributed with image acquisition and interpretation. MSS researched the literature and wrote the first draft of the manuscript. S wrote the final version of the manuscript. AG critically reviewed the content of the manuscript. All authors reviewed and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
Not applicable. Permission was obtained from patient(s) or subject(s) in writing for publishing their case report.
Funding
This work received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors
Guarantor
M. Sarthak Swarup