
Abstract
The COVID-19 pandemic is generating great change and challenge to unparalleled levels across the National Health Service, UK. With insufficient and still emerging evidence on this little known virus, recommendations and guidance are changing continually and still evolving. The authors outline some of the planning through the initial stages of the pandemic within a clinical radiology ultrasound service at one UK tertiary centre. Patient triaging, infection control, equipment, staff mental wellbeing, ongoing training and recovery are all subjects of focus. By sharing our experience and strategies, we anticipate that other similar departments may benefit.
Introduction
In December 2019, a novel coronavirus was isolated from a cluster of patients presenting with viral pneumonia in Wuhan, China. 1 Never previously identified in humans and a new strain, little was and is known about this virus. It was temporarily named ‘2019-nCoV’ and subsequently is now named ‘COVID-19’. Human-to-human transmission is efficient, spreading quickly and exponentially with no therapeutics or vaccines proven to treat or prevent. 2 Based on direct experience and personal reflection, the authors aim to outline the planning within a radiology ultrasound (US) service during this unique, ever changing, global crisis. In doing so, we expand the knowledge base to help others facing this evolving pandemic and also assist in the preparedness for similar future diseases.
Background
This centre is one of 14 Scottish National Health Service (NHS) health boards (HB) providing healthcare for three mixed rural and urban council areas serving a combined population of more than 400,000. The geographical area is spread over 2903 square miles. Radiology provides US services across three main hospital sites. There are several smaller satellite outpatient centres spread throughout the region. The US service includes general imaging for the community as well as acute and elective secondary care with more specialised scanning including gynaecology, head and neck, musculoskeletal, paediatrics and urology. There are annual ultrasound referrals of approximately 40,000. The HB has been preparing for the crisis response since early this year. At the time of writing, there have been 298 deaths (to 7 June 2020) involving COVID-19 registered in the HB area. 3
Other groups have published articles on how radiology departments can tackle the risks of virus transmission,4–6 but little review has been made specifically from an ultrasound setting. Whilst there are clear similarities throughout a clinical radiology department, there are also a few relevant variations between modalities, which are crucial to understand for optimal preparation.
Patient triaging
With all senior staff representation, the radiology leadership team met in early March to discuss the emerging crisis and synchronise thinking. The main focus was on patient triaging as well as limiting exposure of staff and patients. Plans were discussed around the potential of staff illness which within a small group, such as our ultrasound department, could be overwhelming. To date, those concerns have not been realised with sonographer team sickness at normal levels below 5% and none due to COVID-19. Leadership team teleconference ‘huddles’ are ongoing each weekday.
Elective work across the wider organisation was postponed as the hospitals remodelled and prepared for the expected influx of patients with COVID-19. The largest teaching hospital was targeted as the COVID-19 admission site centred on the infectious diseases block. Additional intensive care capacity was swiftly created throughout the adjacent hospital area including theatre areas.
Trends began to emerge among patients with prebooked ultrasound appointments. Many failed to arrive or cancelled appointments due to anxiety and fear of attending. As the primary contact for many patients, general practitioner (GP) surgeries were being overwhelmed and those patients still being scanned were understandably confused about how to get the result and what would happen next. Immediate post-scan verbal reassurance was valuable and appreciated but would not always be appropriate.
On 23 March, staff in the Radiology Department cancelled all planned routine work and future appointments. In-patient emergency services and out-patient urgent referrals were maintained. For many, the risk of being in a hospital environment now outweighed the benefit of having an US examination. A momentous administrative-clinical collaborative team effort then ensued across all modalities. Within the radiology information system (RIS) all US waiting lists, planned lists and new referrals were reviewed by the sonographer team and allocated a code of either P5 ‘urgent’ or P4 ‘indefinite hold.’ Priority ‘urgent’ examinations continued including deep venous thrombosis (DVT) pathways and infant screening and management scans for developmental dysplasia of the hips. Although done with professionalism, the process caused a significant amount of anxiety that should not be underestimated for eroding morale. There was fear for the patient if placed in the wrong group and also personal fear of future litigation if this happened.
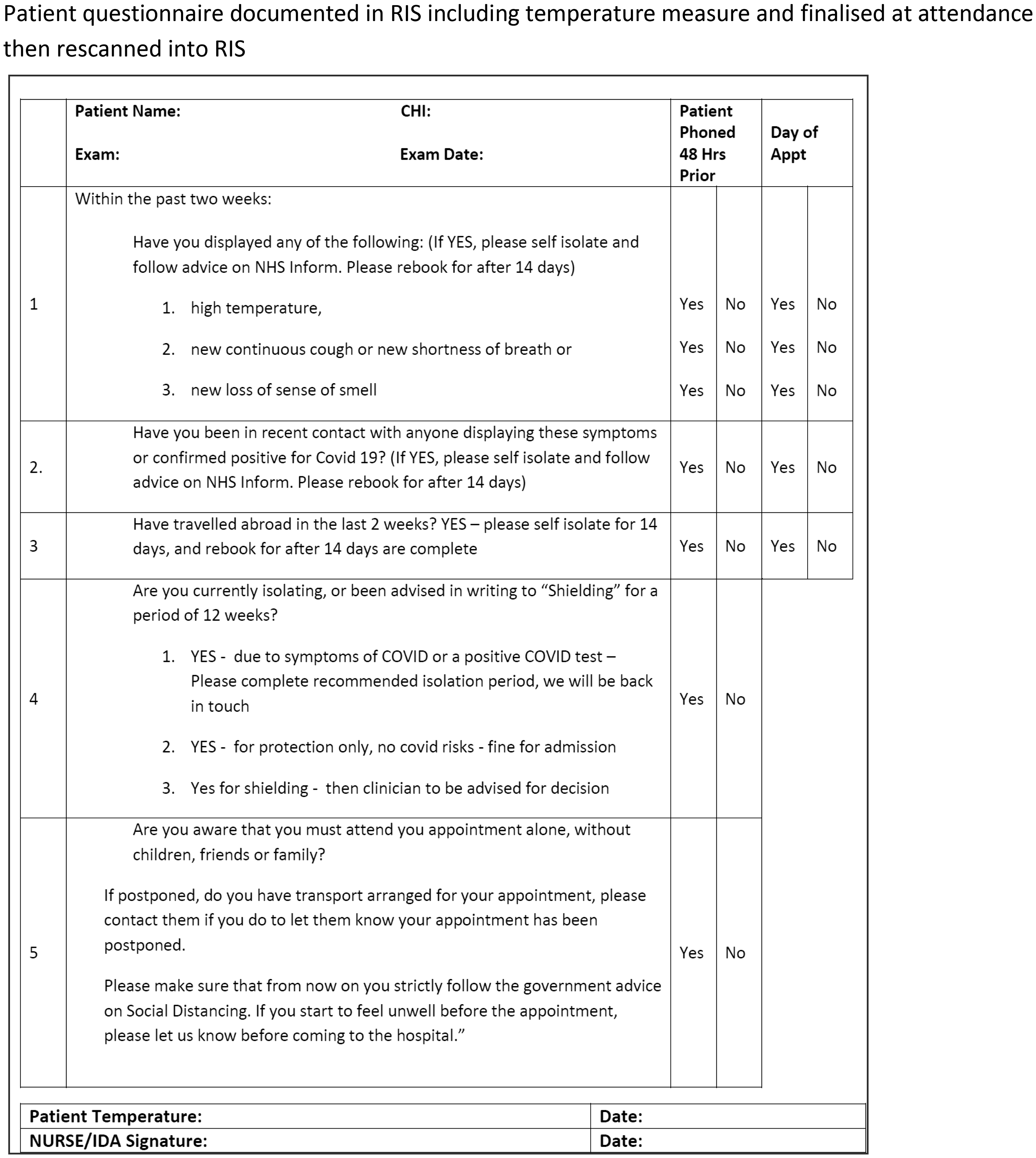
A new process of out-patient booking and attendance was created. Mandatory questions were asked via a telephone call, 48 h pre-attendance. Temperatures were checked with further questions at attendance and all logged and tracked electronically in patients’ event files on the RIS (Figure 1(a) to (c)
Flow charts of out-patient booking and attendance – linked with questions in Figure 2.
Protocol for outpatient booking appointments during COVID-19.
In May, a further agreed process of review of P4 patients (those on indefinite hold) was commenced to establish any status change, this time conducted by referrers. Patients were categorised into three groups; cancel and no longer required, remain on hold or change to urgent then grouped into GP practices or secondary care referral service. Patient groups were communicated to the referrer using spreadsheets between services to establish any updated status before formal changes were made on the RIS. Referrers updated the spreadsheet after discussion with patients and returned results to the Radiology Department to be updated. At the time of writing, this process is ongoing but early results for GP requests suggest that the majority of US examinations remain on hold with equal numbers in the region of 10–15% changing status for each group respectively; cancel and no longer required or change to urgent. Interestingly, across all modalities 86% of cancellations were US examinations.
Infection control
An in-depth appraisal of the extensively media-reported debates around personal protective equipment (PPE) and specific decontamination products is beyond the scope of this paper. However, early indications from China suggest that ultrasound practitioners may be at increased risk compared to other healthcare specialties. This was thought to be due to close patient contact for lengthy examinations and inadequate PPE. 7
Staff anxiety around PPE was high initially. Ultrasound staff felt especially vulnerable being in such close, prolonged contact with the patients. New evidence began to emerge about viral transmission trends and further updates made clear the necessity for PPE if breaking the 2 m social distancing rule, which US imaging clearly does.8,9 PPE confusion was morale draining for the US team despite a slightly faster local radiology roll out than national guidance. There is growing evidence in the literature of increased stress, anxiety, depressive symptoms and insomnia in healthcare workers during the COVID-19 pandemic. One direct causal factor cited is poor access to or use of PPE causing anxiety about personal safety that elevates such equipment’s importance beyond a simple physical barrier.10,11
Decontaminating US equipment is not straightforward. The dust collecting array of knobs and buttons with delicate transducers is a challenge for any decontamination process and the multiplicity and differing manufacturers’ recommendations can be even more confusing. Evidence to support environmental and device cleaning for COVID-19 is limited and Health Protection Scotland’s (HPS) current recommendations could potentially be harmful to some elements of US units. 9 Thankfully covers can be easily used to protect the transducers. In addition, we have an assiduous but pragmatic decontamination team who worked with us to find solutions to what at times felt like an impasse of differing advice.
Equipment
Generally, the ultrasound service does not support routine portable examinations. The time it takes to go to the patient is significantly longer than a departmental scan. Clearly this could vastly alter staff scanning capacity if more portable scans were required to scan patients with COVID-19 in dedicated areas. Additionally, ward scans are ergonomically and quality-handicapped on several levels and portable equipment is generally only used to answer narrow focussed questions. Subsequently, there were no ‘spare’ portable units to locate and designate specifically for patients within the COVID-19 area of the hospital. It became clear that an equipment review was needed. The main hospital had quickly realigned the wards into ‘red’ (positive for COVID-19) and ‘green’ (negative for COVID-19) areas. When caring for patients who were unwell with confirmed or possible COVID-19, any required US examination could be done at the bedside if possible to limit the spread of infection. Two dedicated touch screen US units were quickly procured which have a good range of functionality, manoeuvrability and are ergonomically optimal. With no console or keyboard they are easier to clean and can also be covered completely with transparent sheeting (image intensifier clear sterile covers). Diagnostic acumen is increased, examinations potentially done faster and with more confidence, thus reducing staff exposure to infectious patients.
In addition to portable scanning and with some degree of assistance from the Estates Department, Infection Control and Information Technology team, a static scanner from the main department was relocated into a radiography room within the red COVID-19 admission area. This was to provide US imaging for COVID positive out-patients e.g. suspected DVT or other urgent speciality intervention such as breast abscess. As community transmission and admission rates decrease and routine scanning recommences, this facility has been stood down but it can quickly be re-established in the event of re-escalation.
Staff wellbeing and morale
Rapidly changing processes, environment and workload has been difficult. There is fear and anxiety around safety, becoming ill, family and home situations and the uncertain future. Also, there is significant fear for patients who may have undiscovered pathologies due to the pause of much of our service. Paradoxically, waiting times have slipped well down priority lists. There is clear value in meeting regularly and ensuring there are mechanisms for communicating together. We use group messaging and weekly virtual team meetings to build an informative and supportive environment for each other. Good communications, empathy, understanding and leadership are crucial to limiting the many stress-triggering factors we are currently dealing with. Importantly, the HB provides easy to access useful resources including mental health and wellbeing, on its intranet.
Training
Most direct training in US scanning is paused but in the longer term this would not be acceptable. Future delivery of training to sonographer and radiology trainees will be challenging. Virtual technology can be predicted to evolve and develop to support live interactive training sessions. There is particular apprehension as to how to deliver training to ‘beginners’ with no established grounding in the basics. This would normally be done with trainer, trainee and patient all in very close proximity for extended periods of time. With social distancing, limits to staff present and limited examination times, this all becomes much harder to achieve. Simulators seem a potential solution but at cost. Previously difficult to fully justify financially, we find simulators more valid and very worthy of a business case.
We have established an US training leadership team of radiology tutors and sonographer mentors to progress strategies around effective registrar and sonographer training. A key foundation we are using for this process is the recent British Medical Ultrasound Society guidance and principles to assist us with resuming safe, practical clinical training in ultrasound. 12 Clear, concise, useful information is vital for both trainee and trainer and we are grading our approach into differing levels dependent upon stage of training.
Recovery
With waiting lists increasing to extraordinary levels we now face a monumental task. Avoiding bottlenecks of patients arriving and avoiding crowded waiting areas to reduce transmission of infection have now become a central concern with social distancing normal for all. New patient pathways are emerging such as ‘reverse barrier’ shielding patients for elective surgery (pre surgical isolation). Ambulatory patient pathways are created to limit in-patient stays and limit opportunities for viral transmission. Scanning and reporting must be swift and US services must be adaptable to assist wider hospital patient flows.
Staff reporting and office areas must now be reconsidered and risk assessed as do staff break, changing and kitchen areas. Perspex screens are planned for reception desks and waiting areas. All meetings are now conducted virtually using Microsoft Teams and we are all on a steep technological learning curve.
Routine US activity is slowly recommencing. Everything must be planned and phased, starting slowly and built up, assessing continuously what works and what does not. We must be flexible and unfortunately we must also plan for the possibility of another surge in disease. Maintaining staffing levels and potential illness is always a concern especially with the Government’s ‘test, trace, isolate, support’ strategy as society transitions from lockdown. 13 Staff must be vigilant in social distancing and safety precautions especially when interacting with fellow staff, to avoid large groups of staff from the same area being forced to isolate.
In general the US areas use shared space within the Radiology Department and appointments must be synchronised with other modalities to avoid overlap and crowding. The HB is evaluating a centralised main entrance temperature screening camera but currently we temperature check each attendance individually. Radiology patients are asked not to arrive early and it is difficult to accommodate them if they do. They are re-routed via back doors and fire exits and on busier sites, entrance coordinators will be used to direct patients away from main receptions quickly. A patient needing time and space to fill their bladder for optimal US assessment was inconsequentially common before the COVID crisis but now it is difficult to accommodate them as waiting space is at a premium. Appointment times are doubled, again to prevent crowding and also allow post attendance cleaning. Even when we get all rooms active again, capacity is reduced by almost half. Evening and weekend working must be explored to try to minimise this, the cost of which is going to be significant.
Conclusion
This is a single centre reflective experience about a still evolving crisis, shared for useful learning. Different hospitals will have their own pathways and processes created according to national and regional guidelines and local advice. However, we anticipate that other departments may also gain benefit from our experience and strategies as the pandemic continues and in the event of new outbreaks.
Footnotes
Contributors
MT, PGR.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
MT.