
Abstract
Introduction
Ultrasound is the modality of choice in the evaluation of neonates and young children with suspected adrenal lesions including adrenal haemorrhage and congenital adrenal hyperplasia. It is also the initial imaging modality in children presenting with an upper abdominal mass, which may be adrenal in origin.
Introduction
Ultrasound is an ideal diagnostic tool in the assessment of adrenal pathology in paediatric patients, as it allows good visualisation of the glands particularly in neonates. Ultrasound is also often the initial imaging modality for paediatric patients presenting with upper abdominal masses, some of which may arise from the adrenal gland. Additionally it has advantages over other imaging modalities as it is non-invasive, relatively low cost, portable, and avoids the use of ionising radiation.
This paper will review the normal anatomy and anatomical variants, as well as the ultrasound appearances of benign and malignant conditions affecting the adrenal glands.
Scan technique
Ultrasound assessment of the adrenal glands is normally performed as part of a full abdominal or renal ultrasound scan, and the child should ideally have been fasted prior to the examination. The scan should be performed in a quiet room with the support of the carer accompanying the child. Warmed ultrasound gel should be used, and toys or a television to distract the child help to obtain adequate images. The upper abdomen should be examined with a transducer of the highest possible frequency for the child’s age and body habitus, which could be a linear 12–15 MHz transducer in a neonate or a 3–5 MHz curvilinear transducer in a large teenager.
The right adrenal gland is best visualised from the right flank or intercostal region using the liver as an acoustic window, and the left adrenal gland from the posterior axillary line through the spleen and left kidney. It is possible to visualise the right adrenal in 97–100% of neonates and the left adrenal in only 83–96% of neonates due overlying stomach or bowel gas.1,2 Due to their small size in later life, normal adrenal glands might not be visible in an older child. If possible, scanning the child in a decubitus or prone position may aid visualisation.
Anatomy and sonographic appearance
The adrenal glands are paired endocrine organs that lie within the retroperitoneum at the superior margin of the perirenal fascia separated from the kidney by perirenal fat. 3 The right gland lies anterosuperior to the right kidney, lateral to the right diaphragmatic crus, medial to the right lobe of the liver, and posterior to the IVC. In comparison, the left adrenal gland is positioned anteromedial to the left kidney, lateral to the aorta and left diaphragmatic crus, and medial to the spleen (Figure 1).
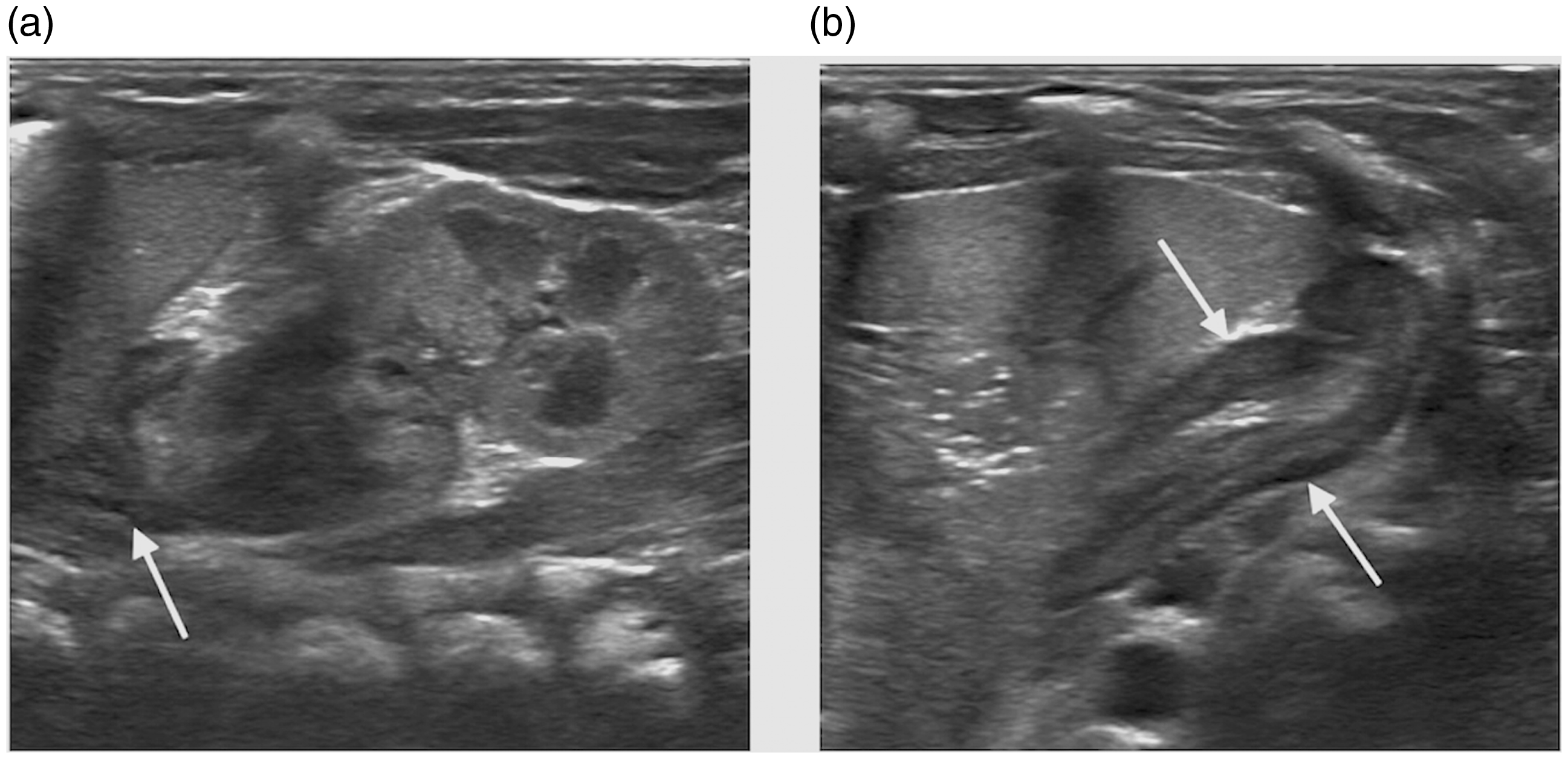
Normal left adrenal gland in a newborn. (a) Longitudinal section shows the adrenal gland between the spleen and kidney (arrow) and (b) axial section shows the two limbs of the adrenal (arrows). The normal neonatal gland has a hyperechoic medulla and a hypoechoic cortex.
At birth the adrenal gland is relatively large at one-third of the size of the kidney. This reduces to one-thirtieth of the size of the kidney in the adult.3,4 However, the mass of an adrenal gland is similar at birth compared to adulthood; it weighs about 5 g. The gland atrophies after birth and serial sonographic examinations have shown a decrease in size of up to 50% in the first six weeks postnatally. 5 From the second year of life it slowly grows and reaches adult size at puberty 3 , 5 (Figure 2). It is possible to measure the gland on ultrasound with the normal neonatal adrenal length described as between 0.9 and 3.6 cm (mean 1.5–1.7 cm) and limb thickness between 0.2 and 0.5 cm (mean 0.3 cm). 1 , 5 In older children and adults, the adrenal gland measures 4–6 cm in length with 0.2–0.6 cm in limb thickness. 6
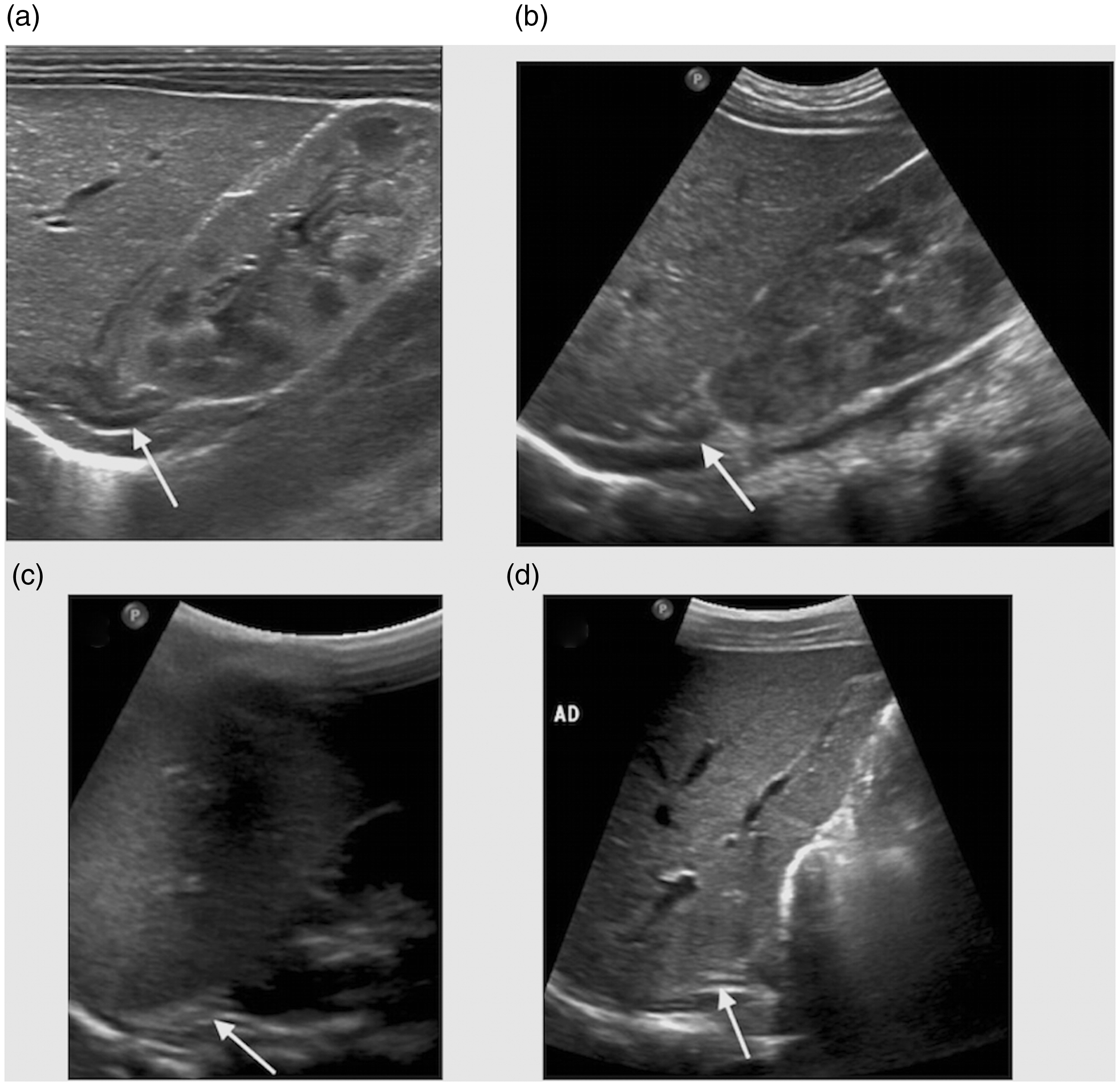
Normal right adrenal gland at different ages. Longitudinal section of the right adrenal gland (arrow) in (a) a neonate, (b) in a six-week-old child, (c) at three years of age, and (d) eight years of age. Later in life the adrenal gland appears hypoechoic with surrounding hyperechoic fat.
Although there can be considerable variation, the right adrenal gland is usually triangular or pyramidal in shape, whilst the left is normally semilunar. 3 When viewed in longitudinal section, the adrenals adopt an inverted V or Y shape, and in transverse section they appear as L, V, or Y shaped (Figure 1).
The ultrasound appearances of the normal adrenal gland change with age.7,8 The gland consists of a central hyperechoic medullary layer; this develops from neuroendocrine tissue and is responsible for the production of catecholamines. The cortex arises from coelomic mesoderm and is hypoechoic. 4 In the neonate the large hypoechoic cortex comprises a thick transient inner foetal zone that atrophies over time, and a thin outer zone, that becomes the permanent adult cortex. 5 The cortex differentiates into three zones and secretes aldosterone, glucocorticoids, and androgens. 4 , 8 At approximately 5–6 months, the entire gland can appear hyperechoic as most of the hypoechoic foetal zone has atrophied, replaced by fibrous tissue. As the fibrous tissue regresses the gland becomes hypoechoic in appearance, and after one year of age it resembles the hypoechoic adult gland surrounded by hyperechoic fat. 7
Assessment of the adrenal glands
Adrenal disease can be evaluated by subjectively assessing the overall shape of the gland, the margins, and the relative size compared to the adjacent kidney and the opposite gland. Considering the normal variation in the size of the gland, focal or diffuse enlargement is more important than a single measurement. The surface of the gland should be smooth without focal nodules, cysts, or masses and the limb thickness should be constant. In older children and adults, the body of the adrenal gland should not measure more than 10 mm in thickness, and each adrenal limb not more than 6 mm.4,6,9 If measurements exceed this, then further investigation is required.
Congenital anomalies
In addition to adrenal agenesis, adrenal fusion anomalies or accessory gland tissue may be seen. A circumrenal or round adrenal gland is related to fusion of the two limbs of the gland (Figure 3). 10 A horseshoe adrenal gland is similar to a horseshoe kidney with fusion of the medial limbs of the two adrenal glands.10,11 On ultrasound, this would be seen as a solitary adrenal gland lying in the midline with a fused portion anterior to the aorta. This can be associated with asplenia, neural tube defects, and renal anomalies. An adrenal gland requires a normal anatomically located kidney to achieve its typical triangular, Y or V shape. The adrenal gland is straight, elongated, or discoid in shape in cases of unilateral renal agenesis or renal migration anomalies (Figure 4). 12 Unilateral renal agenesis is often detected incidentally. A straight, elongated, or discoid adrenal gland should prompt careful examination of the entire abdomen to identify a pelvic kidney. However, post-nephrectomy, the gland retains its normal shape.
Round or circumrenal adrenal gland in a neonate. Transverse image shows a round appearing left adrenal gland (arrow).
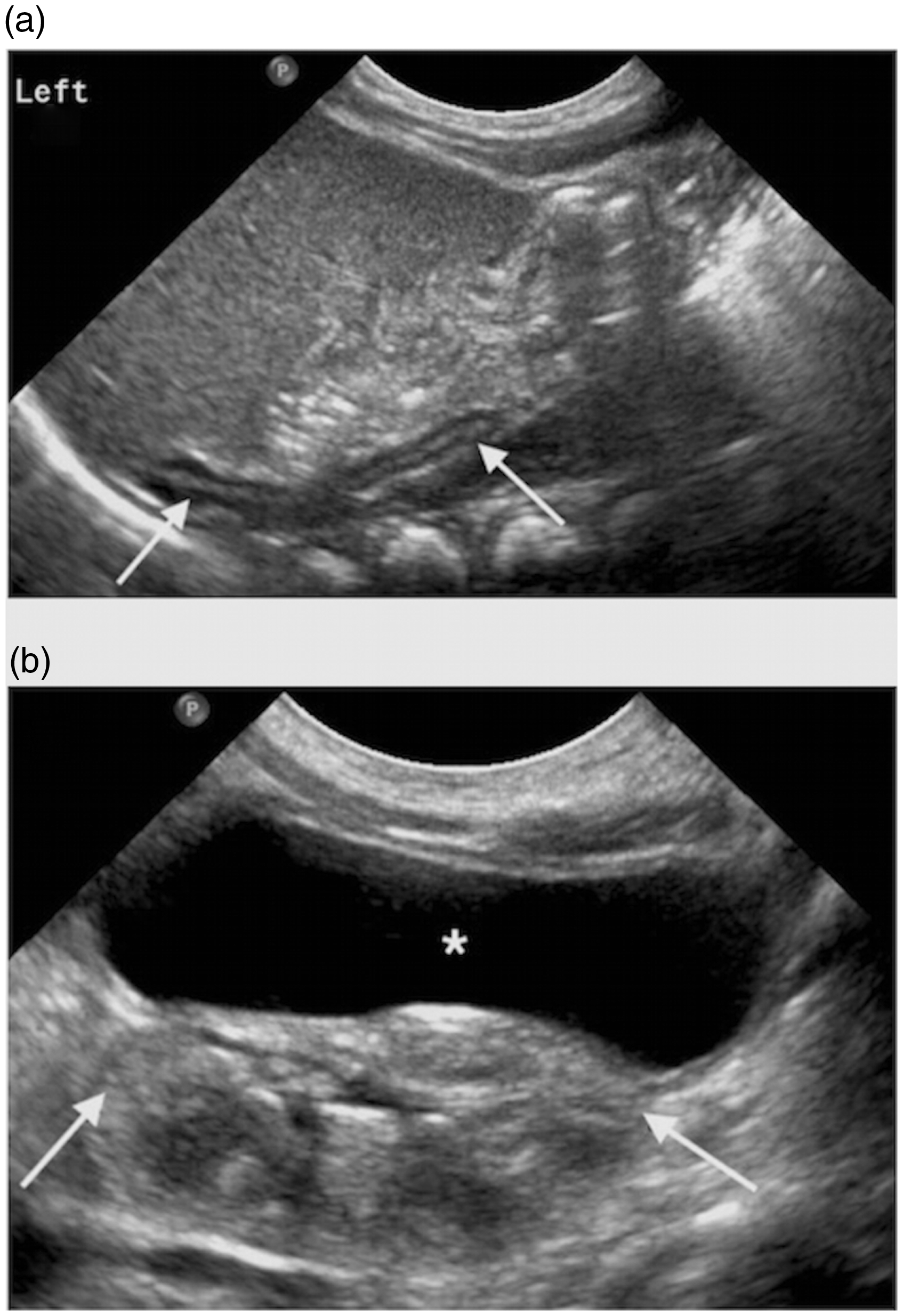
Straight adrenal gland in a neonate with a pelvic kidney. (a) Longitudinal image of the left adrenal shows a long straight gland (arrows) and no kidney in the normal position and (b) longitudinal section of the pelvis shows a malpositioned and rotated pelvic kidney close to the urinary bladder (asterisk).
Congenital adrenal hyperplasia (CAH)
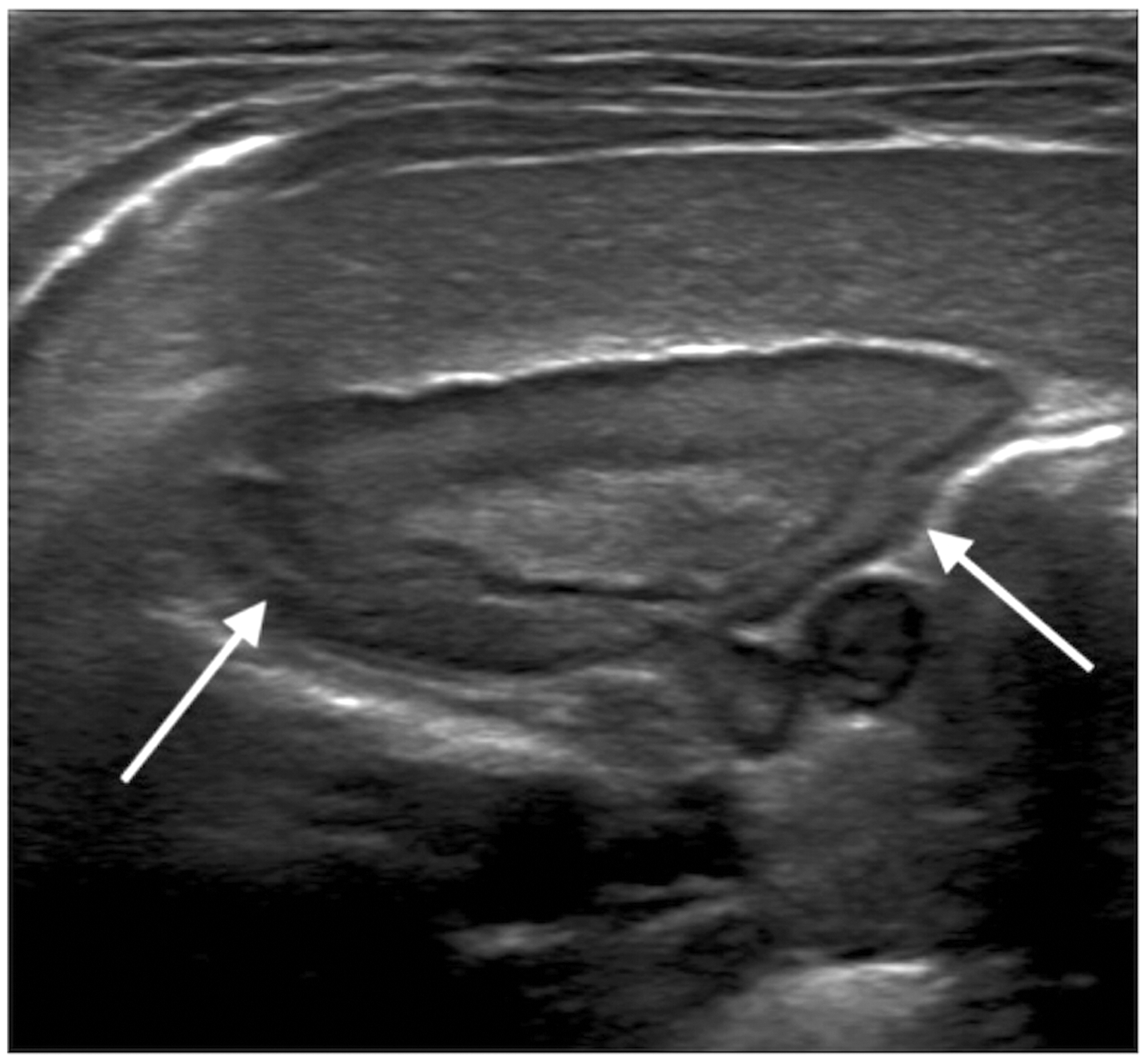
CAH is an autosomal recessive condition caused by an enzyme deficiency in adrenal corticosteroid metabolism, typically 21-hydroxylase deficiency. It presents clinically at birth with ambiguous genitalia in an affected girl. The only sign in an affected boy is salt loss which can be life threatening. 13 Ultrasound is very useful in the assessment of these neonates with a high sensitivity and 100% specificity. 14 Adrenal glands in CAH are enlarged, with measurements of adrenal length over 20 mm and limb width over 4 mm usually considered to be abnormal.14–16 Sonographic features include preserved corticomedullary differentiation; diffuse or nodular enlargement of the gland; stippled echogenicity; and a wrinkled, lobulated, or cerebriform cortex (Figure 5).14–17
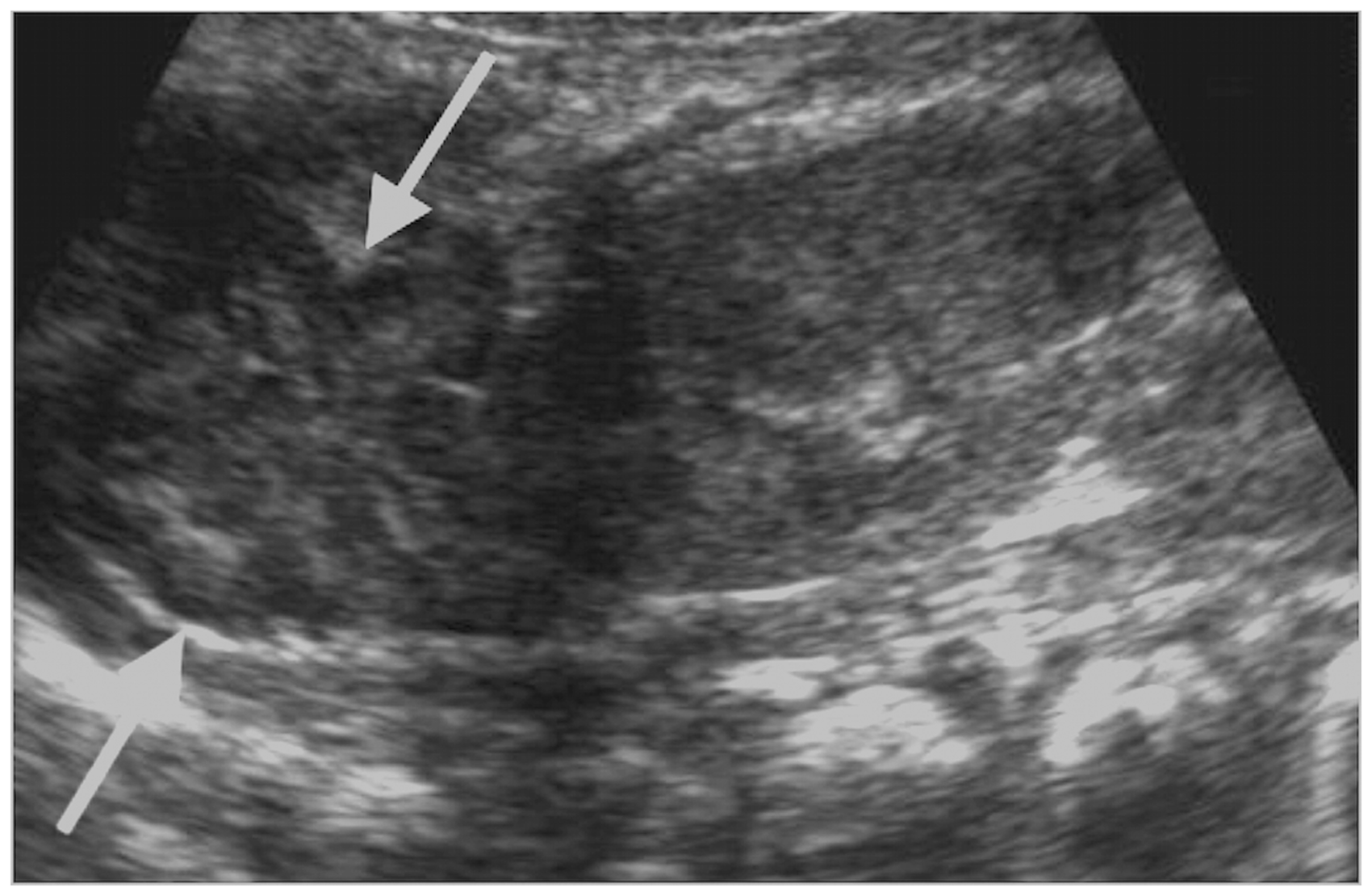
Neonate with CAH. The baby girl presented with ambiguous genitalia. Longitudinal image of the right adrenal area shows an enlarged gland with a cerebriform surface (arrows).
Adrenal cysts
True epithelial-lined adrenal cysts are rare in childhood and are usually detected incidentally (Figure 6).18,19 These appear as anechoic lesions on ultrasound with increased through transmission and without vascular flow on colour Doppler. The presence of septations, nodularity, or calcification is suggestive of an alternative diagnosis such as a pseudocyst or adrenal neoplasm. 19 Pseudocysts lack an epithelial lining and are often related to previous adrenal haemorrhage.
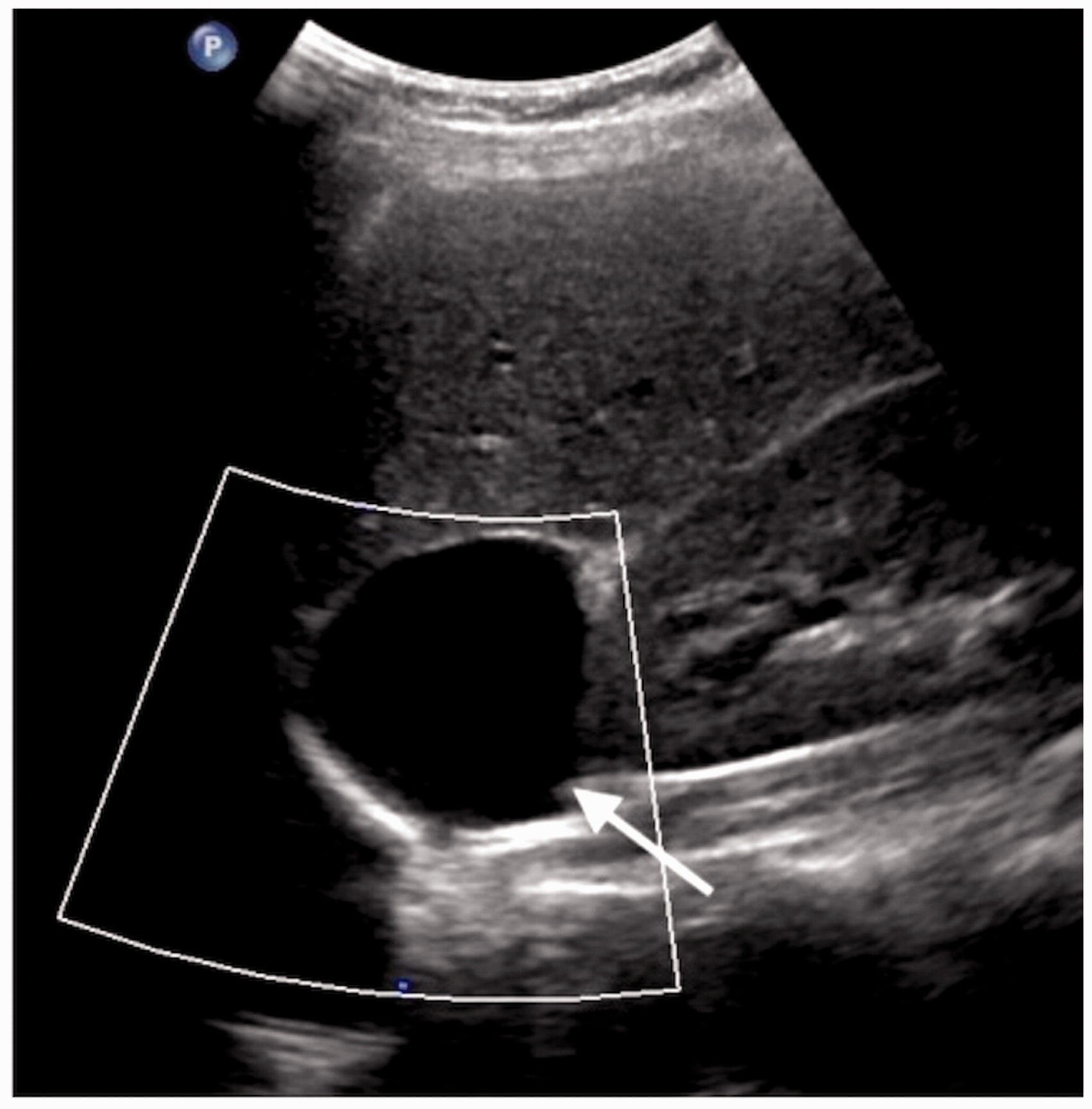
A 12 year old with left adrenal cyst. Longitudinal Doppler ultrasound image demonstrates a well-defined cyst in the left suprarenal area without mural nodularity, calcification, and vascularity.
Adrenal haemorrhage
Spontaneous adrenal haemorrhage primarily occurs in neonates due to birth trauma, macrosomia, anoxia, stress, sepsis, or dehydration. It can also be due to maternal diabetes, hypoxia, sepsis, or coagulopathy.9,17 A large study showed 0.28% of term neonates are affected, although most remain asymptomatic. 20 The haemorrhage is thought to occur due to shunting of blood from the visceral bed in response to perinatal stress or hypoxia, and compression of the IVC during delivery. 9 Clinical features of adrenal haemorrhage include a palpable flank mass, anaemia, jaundice, and rarely hypovolaemic shock or renal failure due to associated renal vein thrombosis. 9 It has previously been reported that the right adrenal is more commonly involved. However, a recent large study in term neonates demonstrated that both adrenals are equally affected. 20
On ultrasound, acute haemorrhage appears as a round or triangular shaped suprarenal hyperechoic mass replacing the entire gland or occasionally limited to one limb of the gland.9,17,21 It is hypovascular on colour Doppler. 22 The appearance of the haemorrhage changes over time: within several days there is liquefaction, making it appear more cystic with a hypoechoic centre, and over several weeks it will reduce in size. 23 Adrenal haemorrhage normally fully resolves but can leave calcification (Figure 7). The main differential diagnosis of a suprarenal mass in a neonate is congenital neuroblastoma. Whilst adrenal haemorrhage will change in appearance over 1–2 weeks becoming cystic, a neuroblastoma will remain hyperechoic, and stable or increase in size, and demonstrate vascularity on colour Doppler (Figure 8). 22 A congenital cystic neuroblastoma is rare and will become more complex with larger solid elements.23,24 Calcifications seen within a mass early on are also more suggestive of neuroblastoma rather than adrenal haemorrhage. 21 Localised neonatal neuroblastoma has a relatively good prognosis and often shows spontaneous regression. 25 Serial follow-up ultrasound scans with assessment of urinary catecholamines are an accepted diagnostic approach to try and differentiate difficult cases.9,24
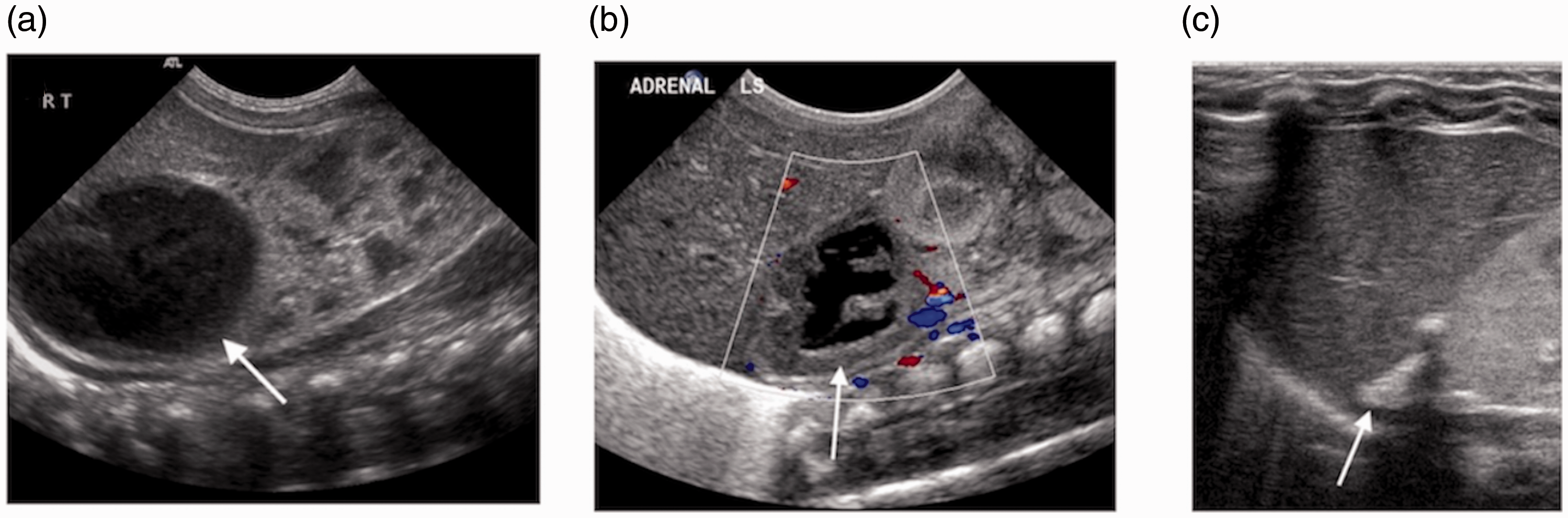
Adrenal haemorrhage. (a) Longitudinal image shows acute right adrenal haemorrhage (arrow) in a five-day-old infant, (b) Doppler ultrasound image shows no internal vascularity in a partly cystic appearing adrenal haemorrhage (arrow) at two weeks of age, and (c) adrenal calcification (arrow) after neonatal adrenal haemorrhage, image taken at four months.
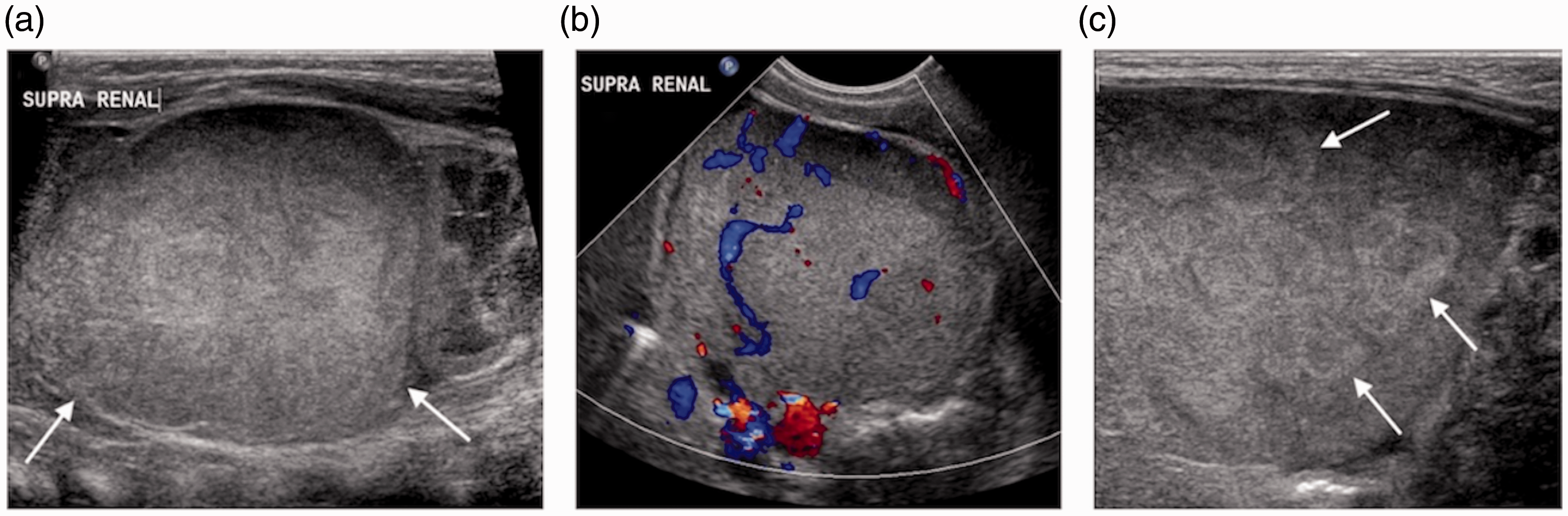
Neuroblastoma in a neonate. (a) Longitudinal image of the left suprarenal area shows a large hyperechoic mass (arrows), (b) Doppler ultrasound image of the mass demonstrates internal vascularity, and (c) high resolution imaging of the liver shows multiple metastases.
In older children, adrenal haemorrhage is seen after blunt trauma, e.g. a road traffic accident or fall from a height, and therefore more commonly diagnosed with computed tomography (Figure 9). It can be associated with other visceral injuries such as liver or splenic lacerations. Most adrenal injuries are self-limiting and do not require intervention. 26 The sonographic appearances are the same as in neonates.

Adrenal haemorrhage after trauma. CT image of the upper abdomen performed after road traffic accident in a teenager shows haemorrhage within the right adrenal gland (arrow).
Neuroblastoma
Neuroblastoma, ganglioneuroblastoma, and ganglioneuroma are part of a spectrum of tumours arising from primitive sympathetic ganglion or neural crest cells. Neuroblastoma is the most common extra-cranial solid cancer of childhood 27 and 46% arise from the adrenal gland. 28 The remainder of tumours occur along the sympathetic chain in the posterior mediastinum, retroperitoneum, or pelvis. Patients present with a palpable abdominal mass, abdominal distension, pain, or with paraneoplastic syndromes such as opsoclonus myoclonus ataxia syndrome. 29 The prognosis of children diagnosed with neuroblastoma varies with age. Those diagnosed before the age of one have a higher five-year survival rate than those diagnosed later but prognosis also depends on histologic and biological characteristics of the tumour. 28 Urinary catecholamines are positive in 90% of patients. Two-thirds of patients have metastatic disease at presentation usually in regional lymph nodes or in the bone marrow. Liver metastases may be identified on ultrasound (Figure 8). Ultrasound is usually the first imaging modality to investigate a child with a suspected abdominal mass. A neuroblastoma typically appears as a solid heterogeneous suprarenal mass displacing the ipsilateral kidney (Figures 8 and 10).28,29 Identifying the kidney separately helps in differentiating neuroblastoma from Wilms’ tumour. The mass may show hypoechoic cystic areas due to necrosis or haemorrhage, and hyperechoic foci due to calcification. 9 , 28 , 29 Colour Doppler usually demonstrates internal vascularity. A cystic neuroblastoma is a variant of a congenital adrenal neuroblastoma that needs to be differentiated from adrenal haemorrhage using careful Doppler assessment to look for vessels within the mass and if necessary serial follow-up ultrasound imaging (Figure 11). 23 Neuroblastoma can extend across the midline and encase or displace vessels rather than infiltrate them (Figure 10).9,28 The aorta and IVC are often displaced anteriorly, and the renal and mesenteric vessels may be surrounded by the mass. 29 Although rare, tumour thrombus can occur and vessel patency should be assessed, particularly of the renal vessels and IVC. 28 , 29 Ultrasound can be used to assess if a lesion is invading neighbouring structures by identifying differential movement between the mass and that structure, e.g. the liver.
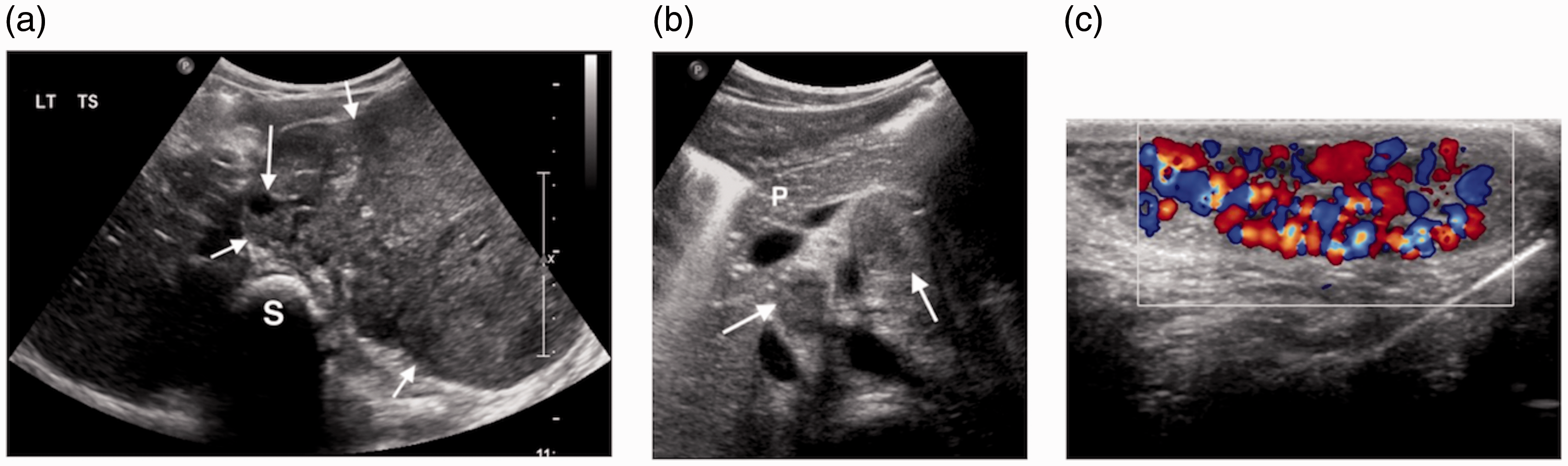
Large neuroblastoma presenting with a varicocele. (a) Transverse image of the upper abdomen shows a large left adrenal mass (short arrows). It extends across the midline and surrounds the aorta (long arrow) anterior to the spine (S). (b) Transverse image superior to (a) shows multiple enlarged paraaortic lymph nodes and pancreas (P). (c) Colour Doppler image of the left testis demonstrates increased vascularity in a varicocele.
Three-month-old infant with cystic neuroblastoma and paraaortic lymphadenopathy. (a) Longitudinal image of the right adrenal area shows a large partly cystic mass (short arrows) displacing the kidney (long arrow) and (b) transverse image of the upper abdomen shows extensive lymphadenopathy (arrows).
Staging requires cross-sectional imaging and metaiodobenzylguanidine imaging to evaluate for image-defined risk factors before surgical intervention according to the International Neuroblastoma Risk Group Staging System.27,30
Other adrenal masses
Ultrasound cannot differentiate neuroblastoma from other tumours of the same spectrum such as the benign ganglioneuroma (Figure 12) or from other adrenal tumours including pheochromocytoma or adrenal cortical carcinoma.
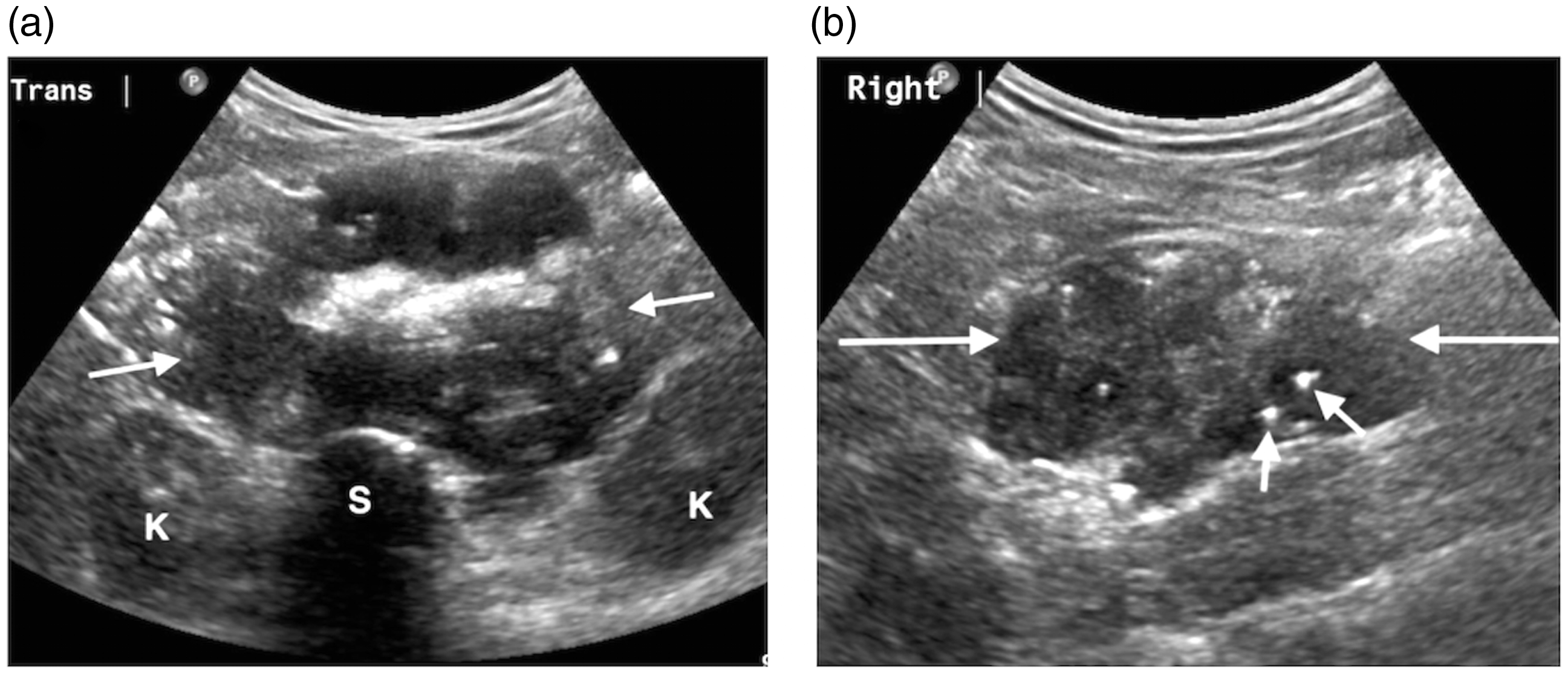
Three year old with ganglioneuroma. (a) Transverse image of the upper abdomen shows a large mass (arrows) that arises from the right suprarenal area, extends across the midline anterior to the spine (S), and displaces the kidneys (K) and (b) longitudinal image of the right flank shows the mass (long arrows) with small hyperechoic flecks of calcification (short arrows) that were incidentally found on an abdominal radiograph for constipation.
Phaeochromocytoma is a rare catecholamine-secreting tumour of chromaffin cells of the adrenal medulla.9,31 Children present with sustained hypertension, headaches, and tachycardia and the tumours may be discovered during renal ultrasound. 8 , 9 On ultrasound, these tumours appear as well-defined homogeneous or heterogeneous solid round or oval masses. 9 Pheochromocytomas are more common and often multiple or bilateral in multiple endocrine neoplasia syndromes and von Hippel–Lindau disease. 9 The diagnosis is usually established by identifying raised serum catecholamine or urine metanephrine levels.
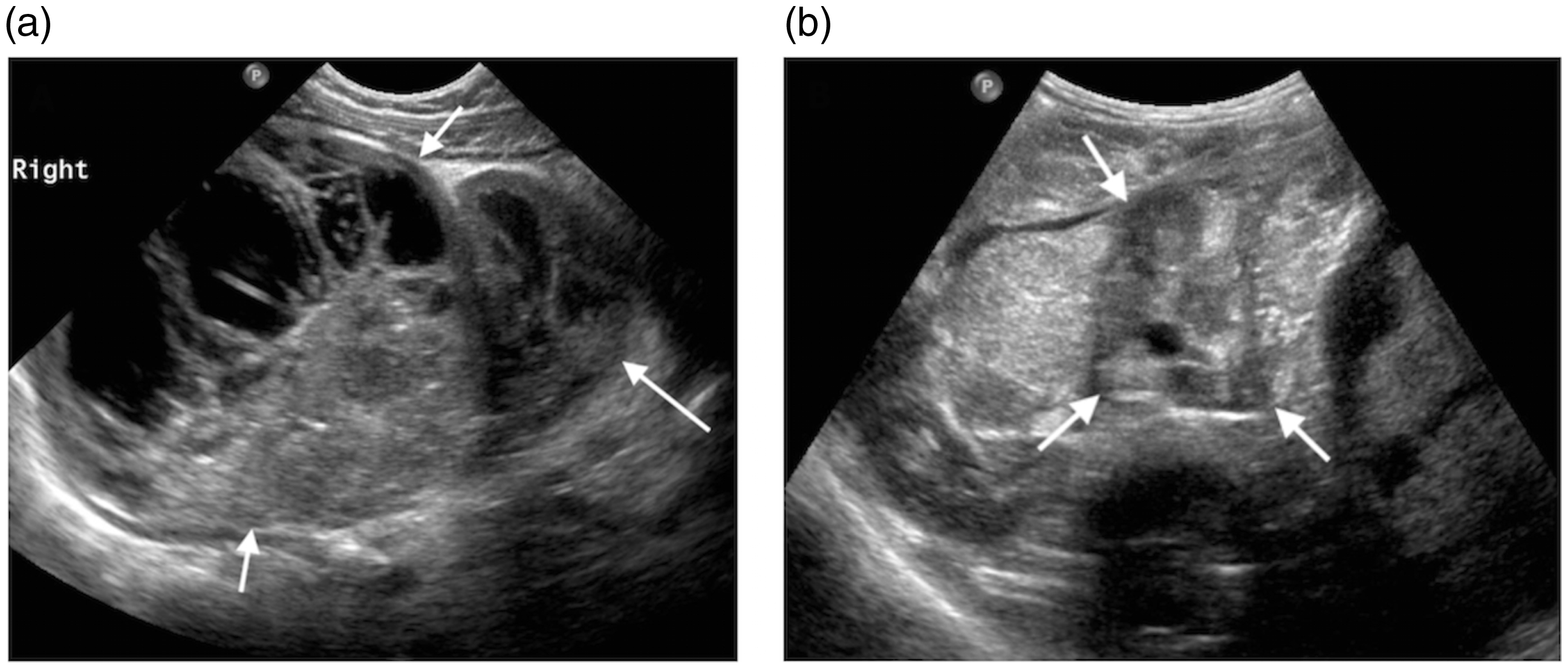
Adrenocortical carcinoma is a rare, highly malignant tumour that occurs in young children. 9 As tumours are hormonally active, patients present with precocious puberty, symptoms of Cushing’s, and virilisation/feminisation rather than with a palpable mass. 29 On ultrasound, it appears as a solid heterogeneous mass (Figure 13). Larger lesions often have areas of necrosis, haemorrhage, and calcification and may be associated with lymphadenopathy. Ultrasound is particularly useful to assess for IVC invasion. 29
Adrenocortical carcinoma. (a) Longitudinal image of the right flank shows a large round solid mass in the suprarenal area (arrow). It displaces the right kidney (K) and is separate from the liver (L). (b) Longitudinal image of the IVC demonstrates tumour invasion (arrows).
Differential diagnosis
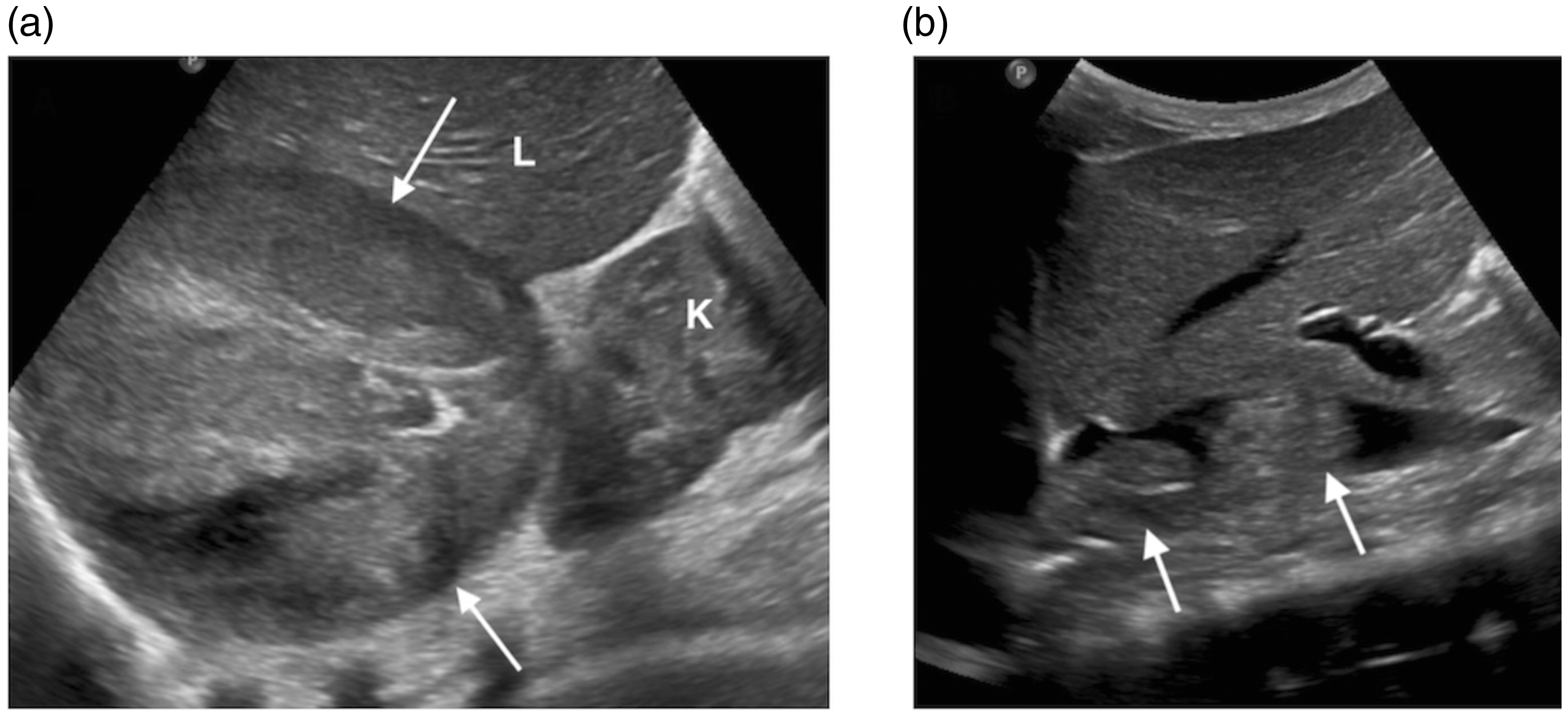
Careful ultrasound evaluation may help to differentiate renal from adrenal masses. An infradiaphragmatic extralobar sequestration, which is more commonly seen on the left, may be confused for an adrenal lesion in a young child. 29 Extramedullary haematopoiesis, which can be seen in children with chronic haemolytic anaemias such as thalassaemia or sickle cell disease, may also present as a paravertebral perirenal or suprarenal mass (Figure 14). 17
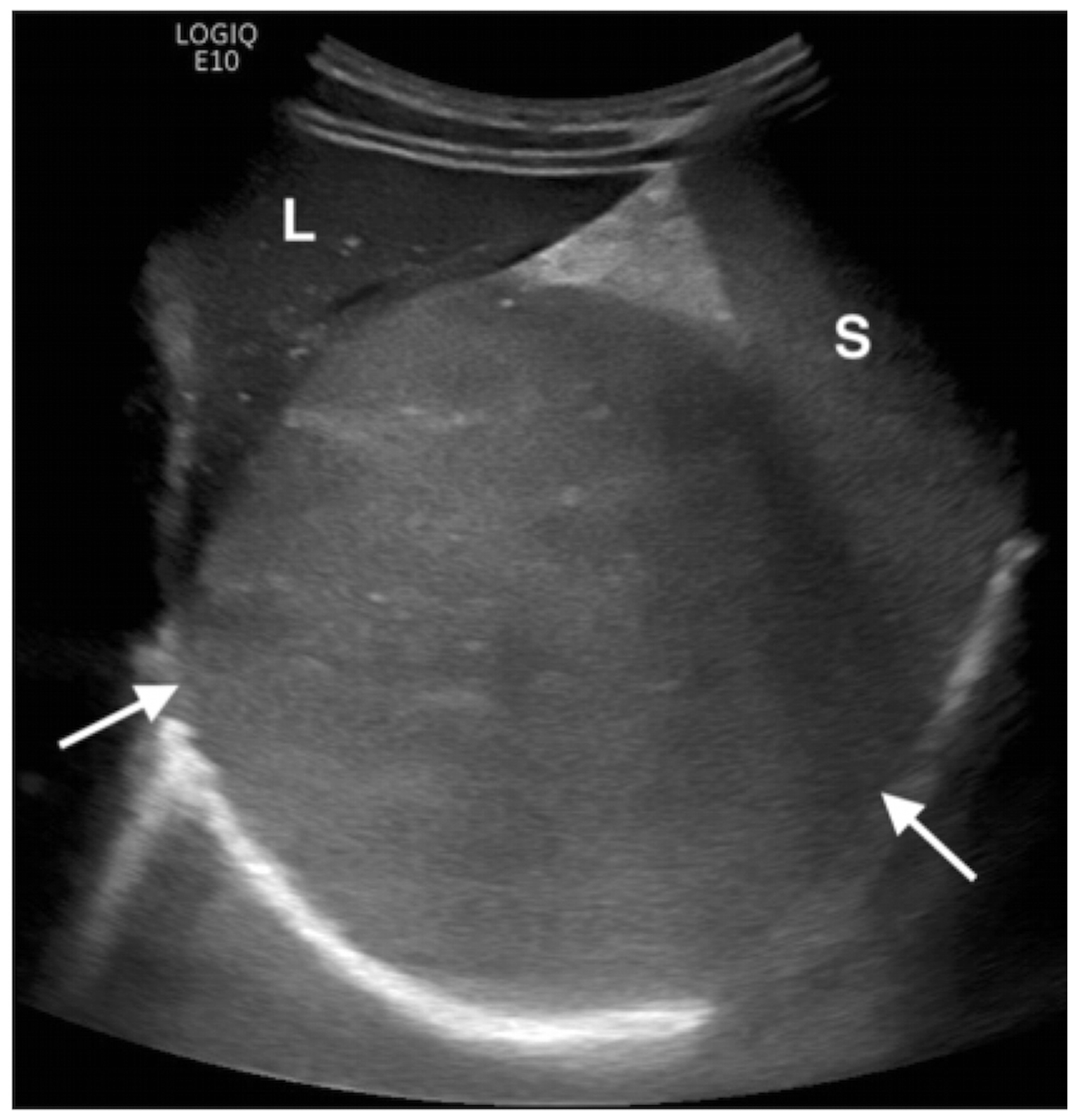
Extramedullary haematopoiesis in a young child with sickle cell anaemia. Image of the left upper abdomen demonstrates a large solid mass (arrows) close to the liver (L) and spleen (S) but not infiltrating them.
Conclusion
Ultrasound is a useful primary imaging modality in the assessment of the adrenal gland in young children, and when evaluating a child with a palpable abdominal mass. The ultrasound appearances of the adrenal gland change with age. Congenital adrenal anomalies are often associated with renal anomalies. Differentiating between adrenal masses can be challenging due to shared ultrasound characteristics, therefore correlation with biochemical findings, multimodality imaging, and histology is usually required.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
For this type of review article ethical approval is not required.
Guarantor
TA/JK.
Contributors
TA and JK researched literature. TA wrote the first draft of the manuscript. JK found appropriate cases for inclusion. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Acknowledgments
None.