
Abstract
Introduction
There is a lack of a quality framework in most emergency departments despite the set national standards for storing point-of-care ultrasound (PoCUS) examinations. To explore and address this problem, a quality improvement project was undertaken in an emergency department.
Results
Over a 10-month period (September 2018–July 2019), there were three PDSA cycles, which included a total of 195 performed emergency department PoCUS examinations. The implemented quality framework led to 90% of examinations stored to PACS, with a mean of 63%. No negative impacts were reported, and feedback was positive.
Conclusion
Implementing a quality framework for storing emergency department PoCUS examinations on PACS is feasible and significantly improves practice. Further work is required to sustain and improve the process.
Introduction
Available knowledge
Point-of-care ultrasound (PoCUS) examinations are carried out on a daily basis to enhance patient assessment, care and safety in emergency medicine. The Royal College of Emergency Medicine (RCEM), Royal College of Radiologists (RCR) and the British Medical Ultrasound Society (BMUS) recommend that all images from ultrasound examinations are stored on a picture archiving and communication system (PACS).1–3 This is also supported by the general principles of Digital Imaging and Communications in Medicine, and the General Data Protection Regulation.4,5 However, clinical governance and administration has not kept pace with the speed of adaptation and expansion of PoCUS in clinical practice, 6 which in itself needs more refined application to have the maximum impact and benefit. 7 The Emergency Care Research Institute (ECRI) states ‘adoption of point-of-care ultrasound is outpacing safeguards’, and lists PoCUS as second in the 2020 Top 10 Health Technology Hazards. 6 To improve practice, specific PoCUS pillars have been suggested to be established, which are governance, infrastructure, administration, education and quality. 8 In the UK, there is a limited published quality improvement project (QIP) to establish PoCUS governance and administration, apart from one that implemented a standard proforma for recording scans performed in an emergency department (ED), 9 but there has been no further work to tackle other aspects such as recording and storage of images on PACS.
Problem
The lack of agreed and established local protocols for handling and storage of ED PoCUS examination images often leads to so-called ‘ghost scans’, which are performed as part of the initial assessment and decision making but without appropriate record keeping.10 Sometimes the examinations could even be performed without the right level of competence or supervision, which carry obvious potential adverse effects. For example, incorrect and inappropriate clinical judgements could be made such as commencing on a specific treatment, or requesting further imaging such as contract-enhanced computed tomography, or referral to a speciality, and transferring the patient to a tertiary centre. Furthermore, poor clinical governance and administration of PoCUS in ED could have other wider impacts on patients, ED staff and other departments such as radiology. For example, requesting unnecessary repeat scans could lead to increased patient anxiety and decreased satisfaction with the services, not allowing comparison and further follow-up scans, and less informed decision making in the outpatient clinics and multidisciplinary team meetings. Additionally, the radiology department and colleagues could be put under excessive burden if resources are not appropriately utilised.
In order to demonstrate the problem in our department, the 10 most recent consecutive PoCUS examinations performed in ED and saved on the ultrasound machine’s internal memory drive were audited. As expected, none of the images was transferred and stored on the PACS.
Rationale and aim
The views of emergency, PACS and radiology staff were sought informally. This led to analysis of the cause and effect of the problem to see if the assumed causes were in keeping with current practice and processes (Appendix 1). The main problem areas were broadly categorised into equipment, system, people and environmental factors. A QIP was initiated with the aim to implement a framework for secure handling and storage of ED PoCUS examinations on PACS (Appendix 2).
Interventions
A stakeholder analysis matrix was completed to assess the current system and the impact potential changes may have on interested parties such as EM consultants and registrars, the clinical director, integrated clinical environment (ICE), PACS and radiology. It also assisted with who, how and when to approach teams and individuals, in particular to highlight the problem and explore the dissatisfaction with the lack of system from the start. To minimise any early resistance to the QIP vision, key steps and interventions aimed at improving practice were clearly explained to all and training was provided. To ensure ongoing support and cooperation with the project, the interventions were designed to be intuitive and in line with other current systems and processes, and continually refined through ongoing analyses and feedback.
First steps
The ED PoCUS machine (Samsung HM70A, Samsung Healthcare, Seoul, South Korea) was assigned a specific Internet Protocol number and connected to the hospital network by Information and Communications Technology. This allowed the examination images saved on the ultrasound machine to be securely transferred and stored to PACS (Intervention 1). Of note, the lung US and echocardiography examination cine clips were also agreed to be stored on PACS, even though it was anticipated that there might be a need for expansion of the storage capacity. The second intervention was the creation of specific electronic requesting order sets on ICE for ED PoCUS examinations by collaboration with the PACS team. These requests automatically prepopulated the corresponding computerised radiology information system (CRIS) codes needed for the correct booking, merging and storing of PoCUS images on PACS (Table 1).
Computerised radiology information system codes for ED PoCUS examinations.
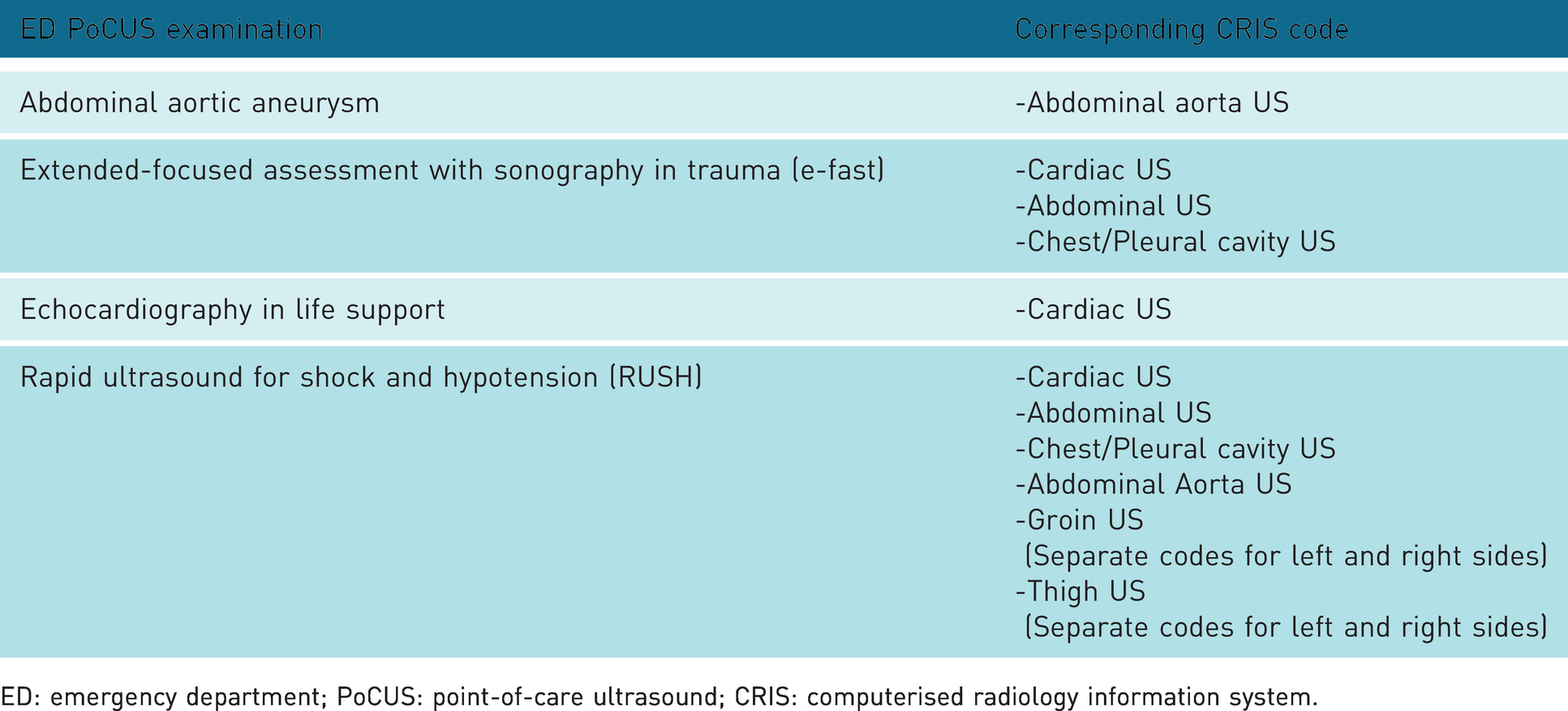
ED: emergency department; PoCUS: point-of-care ultrasound; CRIS: computerised radiology information system.
When requesting the ED PoCUS examination on ICE, a specific pop-up screen was designed that would appear stating ‘Has this request been performed by a competent/supervised physician and will an accredited PoCUS ED physician view all the images and reports?’. Furthermore, an auto-report on CRIS for such requests was set up that would show on PACS as the report with the text stating ‘Point-Of-Care Ultrasound (PoCUS) performed in the Emergency Department. Please refer to the handwritten entry in the Emergency Department clinical notes for the results’.
The ICE requests could be made retrospectively up to a week after discussion and agreement with PACS and radiology. This allowed for scans that were performed on clinically unstable patients such as in suspected ruptured abdominal aortic aneurysm (AAA) or ectopic pregnancy, trauma, and peri-cardiac or cardiac arrest. However, this created extra administration to assign the images uploaded from the machine at the time of the scan with the later requests as well as the need to check that the practitioner performing the scan had adhered to protocol. One method to counteract this was to disable the automatic uploading option for the images from the PoCUS machine on PACS once connected to the network. Instead, the practitioner would make the request, label all the images and delete the unwanted ones, and then manually select the ones needing to be uploaded before sending. However, this also created a problem as the images might never be sorted and sent to PACS, but a compromise had to be made and therefore it was assumed that the practitioner was a responsible healthcare professional.
As the third and final intervention, a paper sticker proforma was designed, approved in the ED clinical governance meeting and ordered (Crown Labels Mfg Co. Ltd) for reporting the performed PoCUS examinations in the patients’ notes (Appendix 3). New guidelines and protocols were written and stored on the intranet, and complemented with posters and notices displayed around the department including in the newsletter (Appendix 4). To reinforce and communicate the new way of practice introduced by the QIP, there were repeated verbal announcements at morning and evening medical handovers, a section written on the monthly departmental newsletter, and notices sent by email to medical staff. Teaching and drop-in sessions were also organised.
Studying the interventions
In collaboration with PACS and radiology, a central register was created to record the ED PoCUS requests made on ICE and the successful transfer of the images to PACS. To gather more information and validate findings, the patients’ notes stored on the ED electronic system were also audited on a monthly basis. In particular, close attention was made to determine if observed results were due to the QIP interventions. All the information was used for the ongoing plan, do, study, act (PDSA) cycles.
Measures
The outcome measure was the number of stored examinations on PACS. Other intervention measures were adherence to reporting, appropriate competence and supervision, reported adverse incidents and harms, and the overall operational impact on ED and other departments. The central register was handled independently by PACS and radiology. The data were complete on all 195 ED PoCUS examinations audited throughout the QIP. Furthermore, underlying characteristics of the QIP that could affect the impact were considered to have an overview of the inherent nature of the interventions and determine the trajectory of the outcomes. The SWOT (strength, weakness, opportunities and threats) tool was utilised to facilitate this undertaking.
The strengths of the QIP were national standards by RCEM, RCR and BMUS; mandate from the main stakeholders such as ED consultants; the paper sticker reporting proforma; specific ICE orders with automatic CRIS booking and option for retrospective requests; and secure hospital network connection for transfer and storage of images on PACS. Conversely, there were some weaknesses such as an unassigned ED consultant to lead and oversee the overall PoCUS practice including supervising this QIP; uncertified, unsupervised, unrequested and unreported scans could still be performed; and the network connection was only by wire. Nevertheless, the QIP led to opportunities, for example improving the relationship between ED and other departments including PACS, radiology and ICE teams. Moreover, ED consultants, trainees and advanced nurse practitioners could be better supported with certification, maintenance and improvement of skills, and appraisal and revalidation. Threats included changes to the normal department operations and practice as well as its priorities, the constant workload and time constraints, locum doctors and other new personnel being unfamiliar with the processes, and the long-term sustainability of the QIP and plans for improving it.
Results
Analysis
Over the 10-month period, three PDSA cycles were completed with monthly measurements, which included 195 ED PoCUS examinations. The implemented interventions led to a significant upward trend in the mean (from 0% to 63%) for correct storage of examinations on PACS. In the final six months of the QIP, the mean fluctuated between 50% and 90% demonstrating not only significant improvement in the outcome but also suitability. There were a couple of months, in particular January and April 2019, in which about 90% adherence was achieved (Figure 1). Such results not only required successful transfer of images to PACS but completed requests on ICE for CRIS booking. Interestingly, this also correlated with successful completion of the paper sticker proforma for reporting the examinations in patients’ notes.

Statistical process control for the correct storing of ED PoCUS examination on PACS.
In mid-February and March, there were fluctuations in the adherence. This could be attributed to the combination of new medical personnel starting in ED combined with departmental pressures faced over the winter period. Some clinicians also reported not being able to access the order sets on ICE for requesting the ED PoCUS examinations, leading to no CRIS bookings. This resulted in images being uploaded on PACS but only saved when the request was finally completed retrospectively after a significant delay. This shortfall in the system led to an increased workload for the PACS and radiology teams. However, the overall feedback from all the key stakeholders and departments remained positive.
Discussion
The PoCUS examinations performed in our ED prior to the QIP were not in keeping with national standards.1–3 This posed a potential significant clinical risk to patient care and safety, and could also lead to conflict between ED, PACS and radiology departments.
Strengths
The QIP demonstrated that simple interventions aligned with recommendations from key professional bodies could lead to a significant improvement in the clinical governance and administration of ED PoCUS practice. Equally the trend of adherence seemed to be sustainable and moved towards 100%, showing effectiveness and sustainability particularly if proper stewardship, amongst other factors, was in place. Furthermore, the QIP utilised the current systems and resources in the hospital without requiring any additional funding. Besides, the project contributed to enhancing awareness, education and innovation within the ED and hospital. It also improved the working relationships with other departments, mainly within PACS and radiology.
There seems to be only one published similar work in the UK, which had limited interventions that was introducing a standard proforma to improve the documentation of ED PoCUS examinations. 9 On the other hand, the QIP undertaken and presented here had several interventions running and complementing one another, and in keeping with the standards and recommendations by RCEM, RCR and BMUS.1–3 They were also akin to those set out in a recent publication outlining the need for establishing pillars of PoCUS that are suggested to be governance, infrastructure, administration, education and quality. 8 On top of that, the project considered and began to address the significant concerns and recommendations recently raised by ECRI regarding potential hazards from PoCUS. 6
Similar QIPs could be undertaken in other UK National Health Service EDs as well as acute medicine and critical care departments where PoCUS is now becoming part of routine clinical practice and standard of care. Most if not all utilise similar systems such as ICE, CRIS and PACS as well as similar processes and infrastructure. Such infrastructures could be adapted to address the increasing use of handheld PoCUS devices such as the Butterfly iQ+
Weaknesses
The data in this QIP were analysed by one individual due to the lack of personnel and resources. In order to offset any bias, the data were collected from all the ED PoCUS examinations with a clear pre-set data collection template and cross referenced with the notes. The PACS and radiology departments managed the central data register independently and verified all information. Moreover, even with the implemented interventions, there is still potential for uncredentialled, unsupervised, unrequested and unreported PoCUS examinations, sometimes by other teams visiting the department to assess a patient. To reduce the risk of this, clear posters and notices were displayed on and around the machine and the department, including in the newsletter (Appendix 4), an automatic pop-up screen as a disclaimer was in place when requesting ED PoCUS on ICE. Other measures included a checklist on the paper sticker proforma, regular review of the database and scans, investigation and follow-up of poor clinical practice, and access to training and education sessions as per ECRI recommendations. 6 To ensure the continued safeguarding and stewardship, as well as improvement of the quality framework, the project was handed over to a permanent ED medical staff agreed by the consultant bodies.
Despite all the implemented interventions, there are still improvements that could be made to this ED PoCUS quality framework such as setting up individual log-ins for each end user on the PoCUS machine, digital rather than a paper sticker proforma for reporting, adding advanced PoCUS scanning on ICE, for example renal and hepatobiliary examinations for those who are certified to do so, regular reviews and follow-up of the performed scan by a certified ED physician and establishing costing for performing each PoCUS examination.
Conclusion
The QIP demonstrates that it is important, feasible and requires no additional funding to implement and maintain a standard quality framework by simple and timely interventions aligned with national guidelines for storing ultrasound images, including ED PoCUS examinations, to PACS. This may lead to improvement in patient care and safety, as well as offering obvious benefits to the service providers and key stakeholders.
Footnotes
Acknowledgements
The author would like to thank Dr Julian Humphrey, Emergency Medicine Consultant, Barnsley Hospital NHS Foundation Trust and Dr Jennifer Cochrane, Emergency Medicine Consultant, NHS Lanarkshire.
Declaration of conflicting interests
NM is an associate of the Butterfly Network, Inc.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
N/A.
Guarantor
N/A.
Contributors
NM is the sole author and principal researcher.