
Abstract
Background
The use of multiparametric magnetic resonance imaging (mpMRI) within active surveillance of prostate cancer programmes is identified by the UK National Institute for Health and Care Excellence (NICE guideline NG 131 2019) as having a role for monitoring disease. The widespread demands on mpMRI capacity may limit its use in surveillance. It is therefore timely to review the options that modern ultrasound imaging present to this cohort of patients in the monitoring of prostate cancer.
Methods
Between April and September 2020, 10 databases were searched to recruit studies for the review. Three reviewers evaluated the publications for inclusion. Characteristics including the inclusion criteria for the study cohort, how disease was determined, identification of disease progression, and the modality and mode of imaging used were reviewed. Given the paucity of full text articles, a meta-analysis was not possible. A narrative review was undertaken.
Results
In total, 12 studies, utilising the range of ultrasound parameters of B-mode, micro-ultrasound, colour Doppler, contrast ultrasound and elastography were included. The review demonstrated that micro-ultrasound offers promise as an imaging tool comparable with mpMRI. However, this is an emerging technology with limited availability. Analysis of the data further demonstrated that by combining the diagnostic features provided by multiple modes reviewed, ultrasound has a role in the diagnostic imaging of patients on active surveillance.
Conclusion
Providing a multiparametric approach is utilised, stable ultrasound findings may allow for increased intervals between biopsy for men on surveillance. The advent of micro-US offers promise as an imaging modality within an active surveillance pathway but requires further verification.
Keywords
Introduction
Despite the fact that active surveillance (AS) has been advocated as a useful, safe and effective pathway in the management of prostate cancer (PCa) for over 10 years,1,2 recent publications by Merriel et al. 3 and Bruinsma et al. 4 both highlight a lack of consistency in AS monitoring protocols. In particular, there is little consistency in the guidelines for the recommended use of multiparametric magnetic resonance imaging (mpMRI) 4 ; however, the PROMIS study 5 demonstrated that incorporating mpMRI into the diagnostic pathway as an initial test prior to prostate biopsy may improve the detection of clinically significant prostate cancer. The Prostate Cancer UK consensus statement 3 highlighted that the application of mpMRI for monitoring disease is evolving but also acknowledged that there are significant gaps in the literature surrounding the best use of mpMRI in AS, despite mpMRI being included with the 2019 NICE guideline NG 131. 6 For this to be a valuable imaging modality, regular access to high-quality mpMRI, in terms of both imaging protocols and reporting standards is required. 7 There is known variability between the reporters of mpMRI despite the use of a standardised reporting tool. 8 This variability, coupled with the challenges associated with mpMRI including poor visualisation of equivocal and/or mpMRI invisible lesions which may be present in patients on AS, has resulted in a reduced sensitivity of mpMRI being reported. 9 Despite the limitations of mpMRI in AS, there are emerging data that support its role in selecting and monitoring men on such a pathway.10,11 However, formalising this into routine practice, given the very real variation in AS programmes 3 and in the variable access to imaging, is a significant challenge. 12 There are persistent and ongoing barriers to the widespread use of mpMRI for AS, including quality, cost and capacity. 11 It is therefore timely to review the option that the modern, alternative imaging modality of ultrasound presents to this cohort of patients.
Ultrasound technology
Publications from the early 2000s related to imaging of patients on monitoring programmes do mention ultrasound (US), 13 but the technological capabilities of the early machines precluded this modality from having a useful role. Technological advances within the last decade have potentially changed that and there is now limited evidence that the use of US may, indeed, have a useful function in the identification of PCa.7,14,15 A meta-analysis by Zhang et al. in 2019 16 assessed the sensitivity and specificity of high frequency micro-ultrasound (micro-US) detection of PCa. This technology has been widely utilised in US imaging of superficial structures 17 but is a relatively new technique in the field of transrectal imaging. 18 Despite the limitations of US at frequencies in the range of 29 MHz, there are promising results from published studies7,18 which supports its use in PCa. The 2019 meta-analysis 16 suggests that micro-US is a more convenient and cost-effective method of imaging and detecting clinically significant PCa, although the study did not specifically evaluate its use in AS and concluded that a comprehensive evaluation remains a necessity.
There is significant heterogeneity across AS guidelines and protocols 19 including regarding the use and timing of mpMRI. Recent publications suggest the role of micro-US 16 adds further choice, but there is a lack of clarity around its use and may hinder or confuse clinician choice in pathway selection. Given the earlier technological limitations of standard frequency US it is, perhaps, understandable why clinicians may not have the confidence to use this modality in the monitoring of patients in such a sensitive and crucial pathway. If US cannot identify the critical window 20 where intervention is required, consequently resulting in a negative impact on patient outcome, its use within a surveillance pathway is significantly restricted. However, the improvements in US described may lead to this modality being a useful adjunct to the monitoring of PCa and thus relieve demand on mpMRI.21,22 Encouragingly, recent publications7,23 have identified good correlation between mpMRI detected lesions of prostate imaging reporting and data system (PI‐RADS) 3, 4 and 5 and identifiable features on US. A range of US parameters to assess PCa, including standard frequency ultrasound imaging, 23 tissue perfusion assessment with Doppler, 24 elastography 25 and the emerging high frequency micro-US, 18 have also been investigated independently, leading to the suggestion that there may be a useful role for multiparametric ultrasound (mpUS) imaging in PCa, 26 other than primarily as a tool to guide tissue sampling biopsy procedures.
Aim
The aim of this study was to perform a systematic review to better understand the role of diagnostic US within the active surveillance pathway of PCa and to clearly identify where gaps in knowledge and data exist.
Methods
Search strategy
The search protocol for this study was submitted for registration to the PROSPERO database of the National Institute for Health Research 27 (registration number: CRD42020199936). Between April and September 2020, 10 databases were systematically searched for eligible articles: AMED, BNI, CINAHL, EMBASE, EMCARE, HMIC, Medline, PsycINFO, Web of Science and Google Scholar. Publications dated between January 2000 and September 2020 were included in the search. Boolean operators were used to construct and combine searches, and the search term ‘NOT’ was used to ensure articles which may use the search term ultrasound for guided biopsy rather than diagnostic procedures were excluded given the extensive use of this search term within literature. Table 1 summarises the search terms used. The results were filtered to include only English language abstracts. Little evidence was expected to be found during the search; therefore, no restrictions were placed upon type of articles included.
Search terms.

Study selection
A preferred reporting item for systematic review and meta-analysis (PRISMA) protocol flow process was followed to identify relevant publications 28 (Figure 1). On identification of potentially relevant titles, the selected articles were independently screened by three reviewers with each full-text article or abstract assessed for relevance using the predetermined inclusion and exclusion criteria described in Table 2.
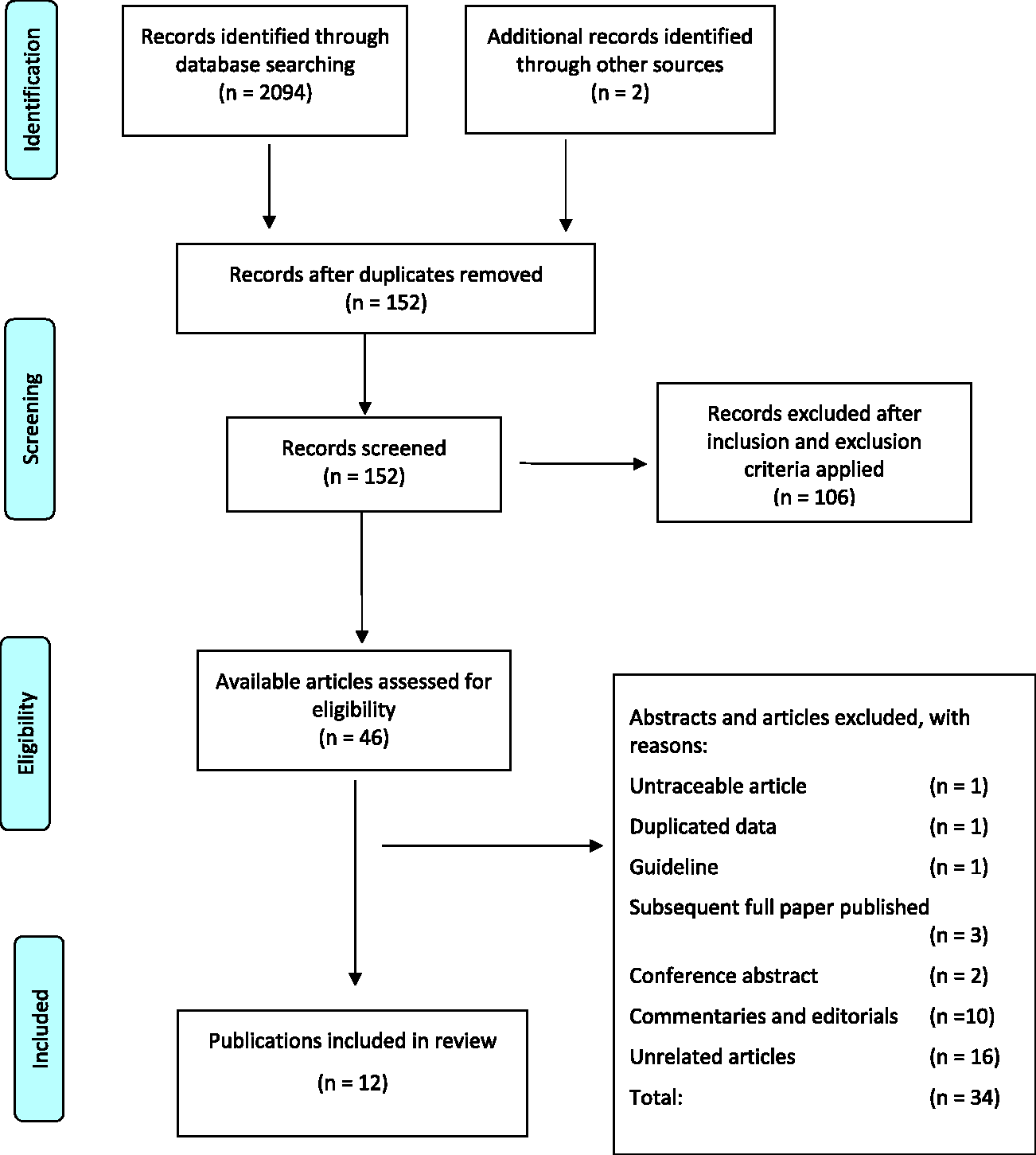
Flow diagram of the process used to select studies for systematic review. Ten databases were systematically searched: AMED, BNI, CINAHL, EMBASE, EMCARE, HMIC, Medline, PsycINFO, Web of Science and Google Scholar.
Inclusion and exclusion criteria for study eligibility.
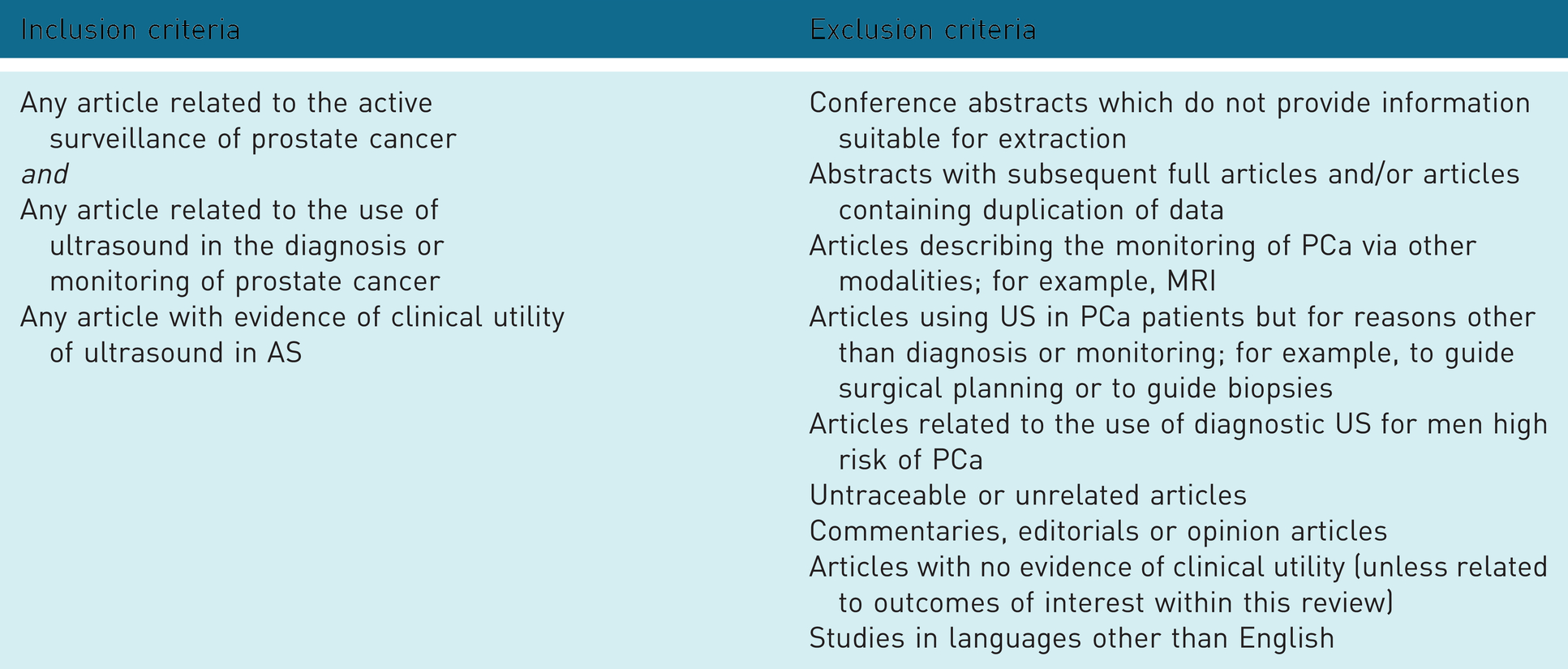
Whilst conference abstracts were included within the literature search, these were excluded from the review if the methodology was of a poor quality or if the data were of insufficient detail to confidently judge quality.
Quality assessment
To evaluate the robustness of the eligible papers, a risk of bias assessment was performed according to the Quality Assessment of Diagnostic Accuracy Studies version 2 (QUADAS-2) tool.
29
A standardised form was utilised to extract the following data from each eligible article:
year of publication type of study described the cohort size the criteria used to describe clinically significant PCa the criteria used to describe disease progression the modality of imaging used within the study the mode of US imaging used within the study
Given the limited number of full-text original research articles available for review, and level of reporting of data, a meta-analysis of findings was not possible. A narrative review of the data was completed.
Results
The PRISMA diagram 28 was used to summarise the literature search (Figure 1). The narrow range of evidence sourced is an indication that diagnostic US is not in widespread use within AS protocols and few randomised control studies or peer reviewed multicentre trials exist. The articles included describe the clinical utility of the use of US in AS.
Evidence synthesis
The initial search identified 2094 titles with a further two papers found by forward backward reference searching. Duplicates were identified and excluded. This yielded 152 potentially eligible articles. Of these, 106 articles were excluded on primary screening because US was used solely to guide biopsy procedures. The remaining 46 published studies were reviewed for eligibility; 23 available articles were reviewed by reviewers 1 and 2 and 23 available articles reviewed by reviewer 1 and 3.
Inter-reviewer agreement
The inter-reviewer agreement was assessed using the Cohen k coefficient. Between reviewers 1 and 2, the Cohen k coefficient was 0.82 and between reviewers 1 and 3, 0.75. Despite the substantial agreement between reviewers 1 and 3, there were six publications in which these reviewers disagreed about their inclusion. A second review of these publications was made by reviewer 2 and a consensus agreement made.
Quality assessment
A total of 12 eligible articles were taken forward to the quality assessment stage. These were scored using the defined matrix and agreed parameters within the QUADAS-2 tool. 29 Three articles discuss the technology of US and its use in the diagnosis of PCa, rather than the role of US specifically in AS23,30,31 but were included as the potential role of US could be inferred from the data extracted from these publications.
From the QA, seven publications had a low concern of applicability for inclusion,7,13,21,32–35 two had a moderate concern30,36 and two had a high concern of applicability for inclusion23,31 within the review. The characteristics of the studies were reviewed to assess the study inclusion criteria and study design, how disease was determined, including identification of disease progression if applicable and the modality and mode of imaging used. Study design, patient and inclusion characteristics for each published study are presented in Table 3. Disease and imaging characteristics are presented in Table 4.
Study, patient, and inclusion characteristics

*PSA – prostate specific antigen
** TNM staging system – T = tumour; N = node involvement and M = metastastic spread
*** PRIAS - Active Surveillance for Low-Risk Prostate Cancer Worldwide: The PRIAS Study (37)
**** PSAD - prostate specific antigen density = PSA / prostate volume
***** DRE – digital rectal examination
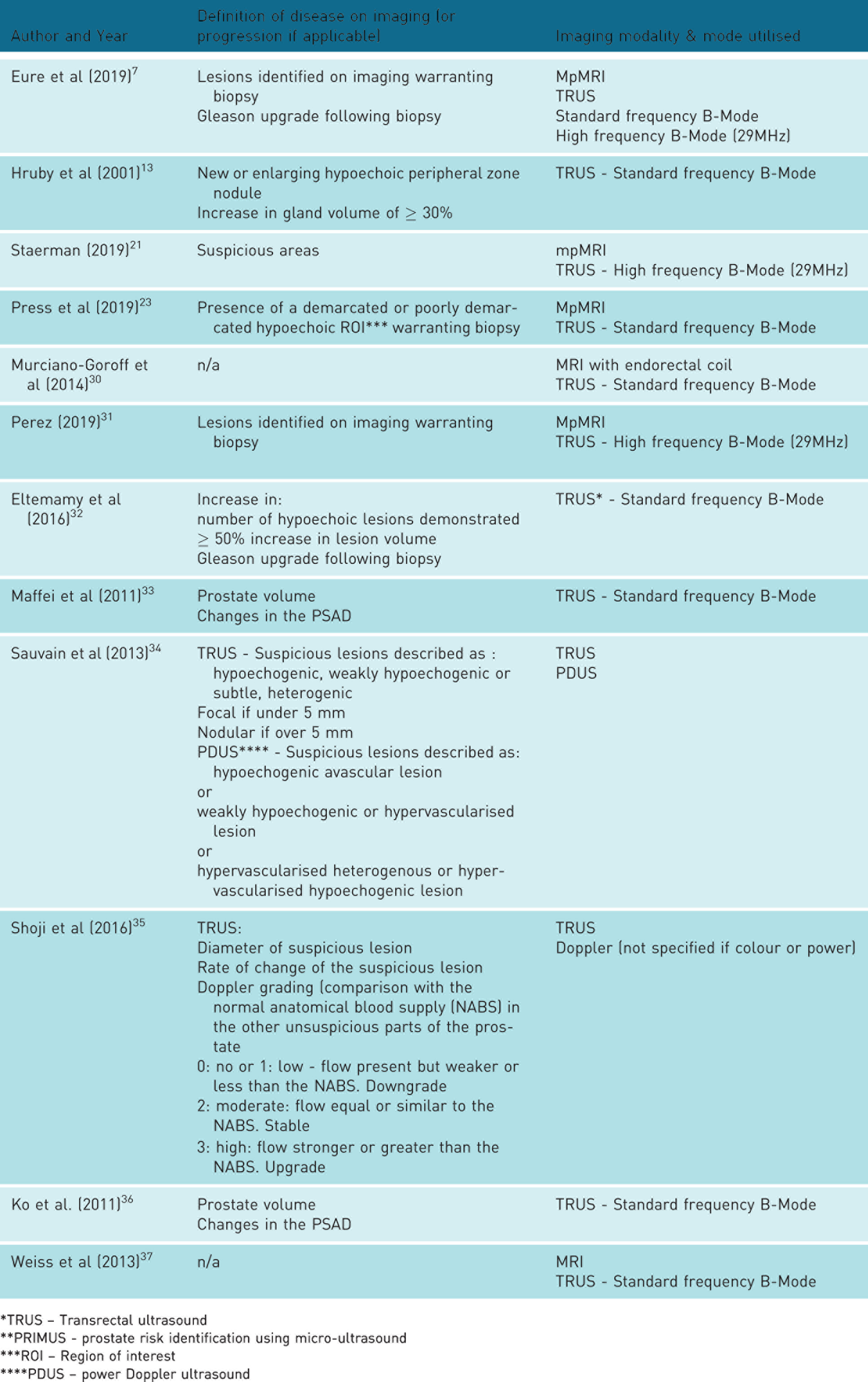
Definition of disease, imaging modality and mode characteristics
*TRUS – Transrectal ultrasound
**PRIMUS - prostate risk identification using micro-ultrasound
***ROI – Region of interest
****PDUS – power Doppler ultrasound
The study characteristics are widely varied; in six studies, the prostate-specific antigen (PSA) was an indicator for inclusion;7,13,31,32,34,35 in four studies, the Gleason score provided an inclusion criterion;13,21,30,32 as did the clinical stage and whether radical treatment was planned in three other studies.7,13,32 Other inclusion criteria included patient’s age, the outcome of the digital rectal examination (DRE) and the prostate volume. Overall, however, it is difficult to draw direct comparisons between publications due to the heterogeneity of sample inclusion criteria applied. The target condition defined for this review is the histopathology-proven progression or upgrade of PCa. In all studies, the cohort of patients had histologically-proven PCa.
Imaging: Identifying disease and progression
Each of the publications was reviewed to determine how disease was defined and to ascertain the imaging modality and mode employed to identify disease, identify disease progression, or monitor disease. Table 4 describes the disease characteristics described within the publications.
Whilst MRI was a ubiquitous imaging modality within the studies, the use and mode of US varied between publications. Most commonly, in eight studies, standard transrectal ultrasound (TRUS) was utilised;13,23,30,32,34–36,37 three studies investigated micro-US21,31,33 and one study employed both standard and micro-US. 7 Defining or identifying disease with the differing US modes, however, is less varied. Lesion identification, using either standard TRUS or micro-US, was the primary diagnostic feature in all studies. The authors used features inherent in US, such as changes to the echogenicity of the suspected lesions, changes to the size of lesions or whether lesions were well demarcated. Identifying changes on US is challenging in all studies, but data suggest that micro-US has improved sensitivity and specificity over standard TRUS. 7
The next most frequent US mode employed within the studies reviewed was Doppler to assess the perfusion of the prostate and suspected lesions.34,35 Doppler assessment is an operator-dependent technique and, as Sauvain et al. 34 identified, transducer pressure may compress microvasculature within small peripheral lesions, thereby compromising the accuracy of this mode of imaging. However, Shoji et al. 35 found that an upgrade in the Doppler signature of a lesion was a significant risk factor for biopsy-proven disease progression.
Sensitivity and specificity
To gain a better understanding of the sensitivity and specificity of each US mode in the detection of clinically significant PCa, data were extracted from each study where there was a confirmatory gold standard documented. The gold standard was either histopathological confirmation of PCa or, as in the two papers evaluating the reliability of prostate volume calculations with TRUS, MRI.30,36 An overview of the study outcomes including the sensitivity and specificity of each imaging mode, where given, is documented in Table 5.
Sensitivity & specificity of US modes utilised within each study

Of the 12 articles, reliable sensitivity and specificity data could be extracted from only six.7,21,23,31–34 Sensitivity of over 80% was reported in four studies using micro-US (range 84%–93.3%)7,21,31,33 and one study using standard TRUS. Press et al. 23 identified changes in US appearance of regions of interest (ROIs) as an indicator of disease progression with sensitivity increasing to a maximum of 76% in lesions that are well demarcated and of a widely different echogenicity to the background prostate. Equivocal sensitivity was reported by Eltemamy et al. 32 with only 49% of biopsy-proven progression being identified on TRUS imaging. A far poorer sensitivity was inferred in the article by Hruby et al. 13 with only 25% of the study cohort with biopsy-proven progression demonstrating any changes on TRUS, although it is acknowledged that this study was performed using now out-dated technology; a repeat of this study, with up to date imaging, may yield improved results.
Specificity is reported in only three studies7,31,33 (range 27.5%–45%) and all used micro-US. Eltemamy et al. 32 demonstrated a reasonable agreement between the TRUS findings and the histopathology results post-biopsy of 66% where there was no evidence of disease progression. No comparable sensitivity and sensitivity data could be extracted from the articles related to the assessment of prostate volume,36,37 although both of these articles have argued that US measurements are comparable with MRI and can be used to assess disease progression. Hruby et al. 13 however, had extremely poor results when using prostate volume to assess progression with only 3.5% of the cohort demonstrating any significant change. Whilst appearances on imaging may change with updated technology, volume measurements are an inherent calculation in any machine and, therefore, a degree of caution is required when using prostate gland volume measurement alone to assess progression. Shoji et al. 35 demonstrated that a change in ROI size, rather than overall gland volume, as well as changes to the Doppler signature, could both be used as a predictor of disease progression. This supports the findings by Sauvain et al. 34 that indicated a normal power Doppler signature was a strong indicator of the absence of clinically significant PCa. Combining changing US features of prostate appearance, ROI appearance, gland and ROI volumes and Doppler signature all suggest that mpUS has a role in the diagnostic imaging of patients on an AS pathway.
Discussion
TRUS
Despite the poor results of standard TRUS reported by Hruby et al. 13 the study by Eltemamy et al. 32 reported TRUS progression criteria in terms of lesion size and site and concluded that stable TRUS findings may allow for increased intervals between biopsy for men on AS. Press et al. 23 demonstrated an increasing sensitivity for disease detection when there were greater changes in appearance of an ROI compared to the background gland echogenicity. Prostates with hypoechoic regions visible on TRUS were reported to experience worse oncological outcomes than men without, suggesting a correlation of ultrasonography findings with disease aggressiveness. 23 The findings of both Eltemamy et al. 32 and Press et al. 23 demonstrate the potential use of TRUS to assist in the risk stratification prior to biopsy among men with stable TRUS and/or low suspicion MRI findings. Men with low or equivocal MRI suspicion could potentially avoid biopsy if no discernible ROI is present on imaging using TRUS. 23 There are limitations to this study in that US ROIs not seen on MRI were not included or scrutinised. However, the purpose of this large cohort prospective study was to compare mpMRI lesions, and the findings do indicate a role for TRUS in this setting. In addition, only lesions with decreased echogenicity on US were considered for review despite previous papers38,39 describing other US features indicating suspicious prostatic lesions in high-grade disease and which were subsequently correlated with radical prostatectomy. Not all lesions can be identified with ultrasound; some histologically proven lesions are known to be isoechoic to the surrounding prostate 38 and as such, operators would need to proceed with caution if B-mode US features alone were to be considered as diagnostic.
Micro-ultrasound
Despite the inherent limitations, US imaging, in particular micro-US, can detect clinically significant PCa.15,22 The sensitivity for disease detection using micro-US ranged from 84% to 93.3%.7,21,31,33 Indeed, Maffei et al. 33 upgraded the Gleason Score to ≥ 7 cancer in 31 patients using micro-US findings alone to indicate the site of confirmatory biopsy. The study by Staerman 21 demonstrated a good concordance rate between mpMRI and micro-US in the identification of suspicious lesions and benign findings in biopsy-proven normal prostate. Micro-US has a reduced depth of field of imaging which hinders assessment of the whole gland, although technological improvements may reduce the negative impact of this fundamental ultrasound limitation. Despite this limitation, the findings of our review indicate that whilst TRUS can identify suspicious ROIs, particularly as disease grading increases, micro-US is an emerging technique that is comparable with MRI. However, this review has also identified that there is only a small number of researchers publishing in this field and few full-text papers are available for analysis, meaning potential difficulties with this new technology cannot be readily assessed. Further multicentre trials of this emerging technology are indicated.
Lesion detection
Being able to identify ROIs within a prostate is an important feature of any imaging mode, be that standard TRUS or micro-US. The key consideration for the use of imaging in AS is the ability to demonstrate longitudinal change of quantitative image-related variables that can be used confidently as a clinical predictor for disease progression, such as diameter or volume of an ROI or the Doppler signature. 35 Shoji et al. 35 describe a high specificity associated with Doppler signature when analysed over the duration of the patient’s follow-up, although they found two major limitations. The first was the limitation of visibility of very low-volume cancer, rendering Doppler imaging difficult to assess. The second was that the threshold volume of clinically significant cancer that could be identified was 0.5 mL; therefore, small but clinically significant cancer may be missed or underestimated by imaging. Volume may be calculated using either the three dimensions with the standard semi-ellipsoid formula inherent within ultrasound machines or using planimetry as used in MRI. Calliper placement for any calculation requires clear demarcation of the tissue-tumour boundary which ultimately depends on clear grey-scale visibility on ultrasound. This inherent limitation of ultrasound may render volume calculations unreliable. However, volume calculations have been investigated and good correlation with gold standard MRI demonstrated. Murciano-Goroff et al. 30 identified the optimum parameters for prostate volume calculations as different methods produced disparate volumes. Ko et al. 36 found that in 95% of their cohort, variability in TRUS-guided prostate volume measurement did not affect PSAD calculations sufficiently to affect management. The study by Weiss et al. 37 demonstrated a high degree of correlation between TRUS- and MRI-based prostate volumes. The authors concluded that given the high degree of accuracy and reproducibility, in the hands of an experienced sonographer, a TRUS-based examination is a reasonable modality for estimating prostate size in all patients with disease of the prostate. In patients with biopsy-proven disease progression, 15% had changes to the ROI volume as the sole indicator of progression on TRUS. 32 Whilst the volume of the ROI is limited by visibility and a finite size, the evidence suggests that the use of this, as an US parameter to monitor disease progression, is clearly beneficial on an AS pathway. However, it is noted that the lesion volume size in these studies were compared to lesion volume on mpMRI and evidence to support direct validation with histologically proven volumes was not found during this literature search.
Perfusion characteristics
Perfusion characteristics of the ROI are a good indicator of normality. 34 Sauvain et al. 34 identified that a normal power Doppler signature (PDS) was associated with a 96% probability of not having a high-risk cancer. They concluded that a normal PDS may be used to delay biopsy in patients with low risk disease. Doppler grading, assessed as a longitudinal variable, also had a positive bearing on assessment of disease progression in the study by Shoji et al. 35 A limitation of any Doppler technique is its reliance on operator performance. Unfortunately, transducer pressure may compress microvasculature within small peripheral lesions, which may lead to misinterpretation of the Doppler signature. 35 A further consideration is the qualitative assessment of the Doppler signature. Shoji et al. 35 used a subjective Doppler grade of blood flow signal within the lesion and classified from grade 0 to 3. Quantitative assessment of perfusion using solely Doppler has demonstrated that the mean speed of coloured pixels and speed-weighted pixel density are good discriminators for PCa in periurethral and the peripheral regions, 40 although this technique has not been widely tested nor utilised in an AS pathway. Technological advances in the identification of microvasculature are now available on modern ultrasound machines but remain under-investigated in the field of prostate cancer. This technique is worthy of consideration in future research given that no published studies have been identified in this systematic review and may contribute to the understanding of perfusion in prostate cancer progression.
Perfusion can also be evaluated using contrast-enhanced ultrasound (CEUS). Whilst good results have been demonstrated for CEUS of lesions 0.5 mL or larger, (sensitivity of 58–69% and specificity of 93–95%), 26 a study by Qi et al. 41 found that three section CEUS was able to detect 92.3% of patients with cancer, whereas standard TRUS identified only 70.7%. The cohort for both studies, however, all had clinically significant cancer (Gleeson ≥ 7) and had subsequent prostatectomy. Techniques quantifying perfusion using contrast are available but have not been investigated in the assessment of prostate cancer under active surveillance. The role of this has not been evaluated within this review, given the absence of published date. There is, indeed, an absence of evidence for the use of CEUS in an AS pathway and, given its limitations of scan duration and contrast agent cost (£92.00 per scan 2019/2020 NHS tariff), 42 it is unlikely to be considered as a viable imaging alternative to mpMRI for patients on AS. However, the strong evidence presented by Sauvain et al. 34 and Shoji et al. 35 suggests that perfusion of the prostate and/or ROI should be considered as part of the mpUS assessment.
Elastography
An US imaging mode that has been trialled in the diagnosis of PCa is elastography, utilising both strain and shear wave techniques. Zhai et al. 43 performed a rigorous study of consecutive patients scanned prior to prostatectomy specifically looking at acoustic radiation force impulse (ARFI). The authors noted that the bilateral stiffness asymmetry created by PCa in ARFI images may provide a convenient means to identify suspicious malignancy in the prostate by being able to differentiate between stiff abnormal tissue and stiffness caused by chronic benign prostatic calcifications that in strain elastography (SE) create false-positive findings. A further study by Pelzer et al. 44 comparing SE with endorectal MRI (eMRI) demonstrated that SE detected PCa in 46 of the 50 positive cancer cohort (92%), whilst eMRI detected PCa in 42 (84%). SE was found to be more sensitive in the apical and mid prostate; eMRI more sensitive in the base (peripheral zones) and transitional zone. In both studies, the patients all had known clinically significant PCa. The limitations of both studies, and with the technique generally, are the uncertainty as to how ARFI or SE can assist in AS when the elastography findings in a normal prostate or in the presence of benign disease are unknown.
Strengths and limitations
This systematic review is the first specifically evaluating the role of all modes of US within an AS pathway. A key strength in of this study is the quality assessment, systematic approach to searching and the robust review of the literature available by a team of reviewers. The eligibility of articles was rigorously reviewed by three independent reviewers which resulted in 12 publications eligible for inclusion. Of these, only eight full-text articles were available despite the authors of the published abstracts being contacted to determine if their data were available as a journal publication. The paucity of full-text articles is an indication of the limited current use of US within an AS pathway. Indeed, the variability of inclusion criteria between studies reflects the lack of consistency of practice within this clinical field. This variation is a challenge for clinicians and patients when planning care pathways and when radical intervention is required. 4 The review has demonstrated that micro-US offers promise as an imaging tool comparable with mpMRI in AS with five7,21,23,31,33 of the 12 papers included related to studies assessing the utility of this modality. However, this review has relied on data related to this emerging technique extracted from conference abstracts with only one full-text paper being eligible for inclusion. Bias could potentially be introduced into the review findings, although the authors acknowledge the lack of published trials. The small cohort of researchers publishing in this field limits the scope of papers available. Literature searching for new and updated relevant publications will continue.
A second limitation of this review is the variability of the modes of US imaging used within the included studies. A meta-analysis was not possible because of the wide heterogeneity across the studies which reduced the comparative data eligible for review. It has been difficult to combine the results of the varied studies to produce a generalisation for clinical practice. Fusion-guided ultrasound imaging has a significant role to play in prostate biopsy following mpMRI and may aid targeted follow-up. 45 Fusion-guided imaging has not been included in this systematic review, as there have been no studies evaluating its use in an active surveillance programme. This remains an area for future research and evaluation. However, this review has indicated that US does have a role in monitoring disease progression provided a multiparametric approach, which includes prostate volume, lesion volume, lesion demarcation, lesion echogenicity and an assessment of the Doppler signature as baseline imaging modes, is utilised. Micro-US shows promise despite the limitations of the publications included. Its use in the routine clinical setting remains uncertain and the technique, including the confidence of image interpretation, will require careful evaluation to fully understand its usefulness and acceptability.
Context of clinical practice
There are significant capacity issues within the National Health Service (NHS) in the UK 46 that limits access to MRI. Waiting times published in the NHS England January 2020 diagnostic dataset 46 document a duration from MRI referral received to examination performed of between 19 and 25 days. Priority is given to urgent cancer diagnosis over follow-up in many institutions, and therefore the ability to fulfil the NICE criteria, 6 where the evidence for such practice continues to be updated, 3 is likely to be limited. There is, however, less of a capacity issue within alternative imaging modalities, such as in diagnostic US, and any evidence that would support the safe transfer of diagnostic imaging from MRI would be welcome at a performance level. Indeed, waiting times for US in England are, on average, 10 days. 46 Whilst capacity for diagnostic imaging is already at a premium, the full impact of the 2020 coronavirus pandemic has yet to be fully realised, but it is certain to have resulted in significant delays for diagnosis and hindered any imaging required on a surveillance pathway. 47 There is mounting evidence of the impact of COVID-19 on the PCa pathway with delays to diagnosis being reported in many of the UK cancer alliances, 48 and this is an issue that is likely to be repeated worldwide. The challenges of providing healthcare to the level required, and comparable with pre-COVID-19 delivery, will be faced for many years to come, although significant interruption to normal practice does provide an opportunity for services to be redesigned and a restart button be pushed. 49 Now is the time to review existing pathways and seek alternatives that are safe for patients, sustainable for future delivery and release capacity in the high demand modalities, such as MRI. Randomised control trials are essential if this technique is to be embedded into everyday clinical practice and US offered as a much needed, viable alternative to mpMRI for patients on AS.
Conclusion
A range of publications has been evaluated and has had to include conference abstracts due to the paucity of data available leading to a limitation of this systematic review. However, it has demonstrated that there may be a role for mpUS for patients with known PCa within an active surveillance pathway despite the evidence being less robust than the evidence for the use of mpMRI. Although not all lesions can be identified on ultrasound, an imaging protocol that combines prostate volume, lesion volume, lesion demarcation, lesion echogenicity and an assessment of the Doppler signature will provide a reasonable sensitivity and specificity but any such model will need testing prior to implementation. Whilst the data demonstrate that standard TRUS is not comparable with mpMRI, it does indicate that, providing an mpUS approach is utilised, stable TRUS findings may allow for increased intervals between biopsy for men on AS. The advent of micro-US, with its reported sensitivity in the range of 84%–93.3%, offers more promise for a truly comparable imaging modality to relieve capacity issues within MRI. Further research is needed to optimise and evaluate mpUS and micro-US for the monitoring of patients with low risk PCa.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval is not required for this systematic review.
Guarantor
PP.
Contributorship
PP, MT and PW researched literature and conceived the study. PP and TP performed the initial review of literature. PP, MT and PW reviewed the literature for eligibility for inclusion in the systematic review. PP wrote the first draft of the article. All authors reviewed and edited the article and approved the final version of the article.
Acknowledgments
We would like to thank Trevor Parker for his assistance and guidance in this systematic review.