
Abstract
Objective:
We hypothesised that distinct patterns of serial cervical length change in dichorionic diamniotic twin pregnancies are associated with differential risks of preterm birth.
Methods:
A retrospective cohort study was conducted at the Twins Clinic of a tertiary fetal medicine unit. In total, 389 women with uncomplicated dichorionic diamniotic twin pregnancies underwent four weekly cervical length measurements. Changes in cervical length were classified into Pattern I (stable cervical length), Pattern II (early rapid shortening), Pattern III (late shortening) and Pattern IV (early shortening with a plateau). Association of each pattern with preterm delivery was assessed.
Results:
Pattern I was observed in 37.5% cases, Pattern II in 11.8%, Pattern III in 32.6% and Pattern IV in 18%. The proportion of patients delivering preterm was significantly higher in Pattern II (early rapid shortening), followed by Pattern III (late shortening). The mean period of gestation at delivery was 35.5 weeks in cases of Pattern I (stable cervical length), 30.7 weeks in Pattern II (early rapid shortening), 34.2 weeks in Pattern III (late shortening) and 34.9 weeks in Pattern IV (early shortening with a plateau). Patients in Pattern II (early rapid shortening) had a significantly shorter mean cervical length at both the nuchal scan and between 20–24 weeks, as well as a significantly greater decline in cervical length between these two time points, compared with those in Pattern IV (early shortening with a plateau).
Conclusion:
Distinct patterns of cervical length shortening in uncomplicated dichorionic diamniotic twin pregnancies are linked to varying risks of preterm birth, thus making serial assessment more predictive than single measurements.
Keywords
Introduction
Preterm birth (PTB) falls among the most important causes of neonatal morbidity and mortality. 1 It is also associated with an increased incidence of neurodevelopmental delay and growth retardation. 2 The incidence of preterm births has shown an increase in recent times, which can be attributed not only to the reduced gestational age of viability with the advances in neonatal care but also to the increase in the incidence of twin pregnancies secondary to increasing maternal age and the use of assisted reproductive techniques.3,4
Spontaneous preterm labour (PTL) still remains the leading cause of preterm delivery, accounting for more than 67% of these cases. 5 Twin gestations are at a higher risk of PTB as compared to singletons, with an estimate of 60% of deliveries occurring before 37 weeks’ gestation, 20% before 34 weeks and 11% before 32 weeks. 6 The chance of PTB in twin pregnancy is 4–5 times higher than in singletons. 7 The overall rate of PTB (before 34 weeks) with twins is estimated to be up to 13%, compared to 1% for singleton pregnancies.8,9
The timely detection of twin pregnancies that are at risk of PTB is of paramount importance as these pregnancies require closer surveillance, and may benefit from interventions like progesterone supplementation, placement of a cervical cerclage and timely steroid and magnesium sulphate administration.10–18
In recent years, research has focused on identifying the ultrasonographic, biophysical and biochemical markers which may be used as predictors of spontaneous preterm delivery. Ultrasonographic measurement of cervical length and fetal fibronectin levels are the most commonly used techniques that can help to predict the risk. 19
The definitions of a short cervix in published literature are varied and range from 10 to 35 mm. 20 As cervical length measurements are dynamic and change as gestation advances, it has been proposed that serial cervical length measurements may be more predictive of the risk of PTB and may enhance the identification of pregnancies at risk.21,22 There are limited data on the predictive ability of serial cervical length measurements and identification of various patterns of cervical length shortening across gestation, especially in relation to multifetal pregnancies. 23 We aimed to study the patterns of cervical length shortening across gestation in uncomplicated dichorionic diamniotic (DCDA) twin pregnancies and the association of each pattern with the risk of PTB.
Materials and methods
A retrospective cohort study was conducted between January 2010 and April 2025 in the Twins Clinic of a tertiary fetal medicine unit. The database of the Fetal Medicine Department was searched over a span of 15 years, during which the examination data of 484 women with DCDA twin pregnancies was analysed. The demographic details of each patient, obstetric history, associated comorbidities, pregnancy complications, need for intervention in the form of cerclage, the timing of delivery and the neonatal outcomes were recorded. Pregnancies which were complicated by any of these conditions were excluded: cervical cerclage, fetal gross congenital anomaly, maternal or fetal condition which necessitated indicated PTB, less than four cervical length measurements across gestation, or single fetal demise. In total, 389 patients who fulfilled the inclusion and exclusion criteria were included in the study. The bias of the use of progesterone supplementation was common across all the groups.
Cervical length measurement was performed with a transvaginal technique according to the guidelines of the Fetal Medicine Foundation. The patient was made to lie down after emptying her bladder in the dorsal lithotomy position. The transvaginal ultrasound probe was introduced into the anterior fornix, making sure to avoid undue pressure on the cervix. A sagittal view of the cervix was obtained such that the entire endocervical mucosa was visible. Callipers were then used to measure the linear distance between the internal os and the external os. At each visit, a minimum of three transvaginal cervical length measurements were obtained, and the shortest technically acceptable measurement was recorded for analysis. The ultrasound examinations were performed using the Voluson E-series machines (E8 and E10, GE Medical Systems, Austria) and equipped with a 5–9 MHz transvaginal probe. All examinations were performed by examiners with certification of competence from the Fetal Medicine Foundation for cervical length assessment. It is our practice to do regular ultrasound examinations for uncomplicated DCDA twin pregnancies starting from the nuchal scan, an anomaly scan at 20 weeks, followed by 4 weekly ultrasound examinations thereafter (in accordance with the guidelines proposed by the ISUOG). 24 Serial cervical length measurements were taken at the time of each scan and recorded. The cervical length measurement was done more frequently in patients with evidence of shortening.
The changes in the cervical length measurement across gestation were analysed by visual inspection and then classified into four distinct patterns. Shortening was defined by a decrease of at least 5 mm between two successive cervical length measurements. Each pattern was characterised taking into account various parameters such as the gestation at which shortening started (early shortening vs. late shortening (LS) classified as before or after 24 weeks’ gestation), the rate of cervical length shortening, and if a plateau was achieved (defined as absence of ⩾5 mm shortening on serial measurements). Microsoft Excel 2024 was used to confirm the classification of the trajectory of cervical length for each patient.
Four patterns of change in the cervical length on serial measurement across gestations were identified (Figure 1):
Pattern I: Stable cervical length (St CxL): defined by the absence of any ⩾5 mm shortening between successive measurements throughout gestation.
Pattern II: Early rapid shortening (ERS): characterised by one or more ⩾5 mm decreases occurring before 24 weeks’ gestation over a short interval, without subsequent stabilisation.
Pattern III: Late shortening (LS): defined by cervical shortening (⩾5 mm) occurring after 24 weeks’ gestation.
Pattern IV: Early shortening with a plateau (EPl): cases with early shortening before 24 weeks followed by a period of relative stability without further ⩾5 mm decreases. Regression lines of the mean of cervical length for each pattern with 95% confidence intervals were plotted (Figure 2). For graphical representation, gestational age categories were displayed at uniform intervals on the x-axis to facilitate visual comparison of cervical length trajectories across patterns.
Although a ⩾5-mm change in cervical length was used for pattern classification in our retrospective analysis, clinical intervention (progesterone supplementation, cervical cerclage placement, inpatient monitoring, etc.) was based on absolute cervical length thresholds. Final management decisions were individualised based on the judgement of the treating clinician and patient preference.
The association of each pattern of cervical length shortening with preterm delivery was assessed. The neonatal outcomes and the birth weights were recorded. The flowchart of the methodology of the study is demonstrated in Figure 3.
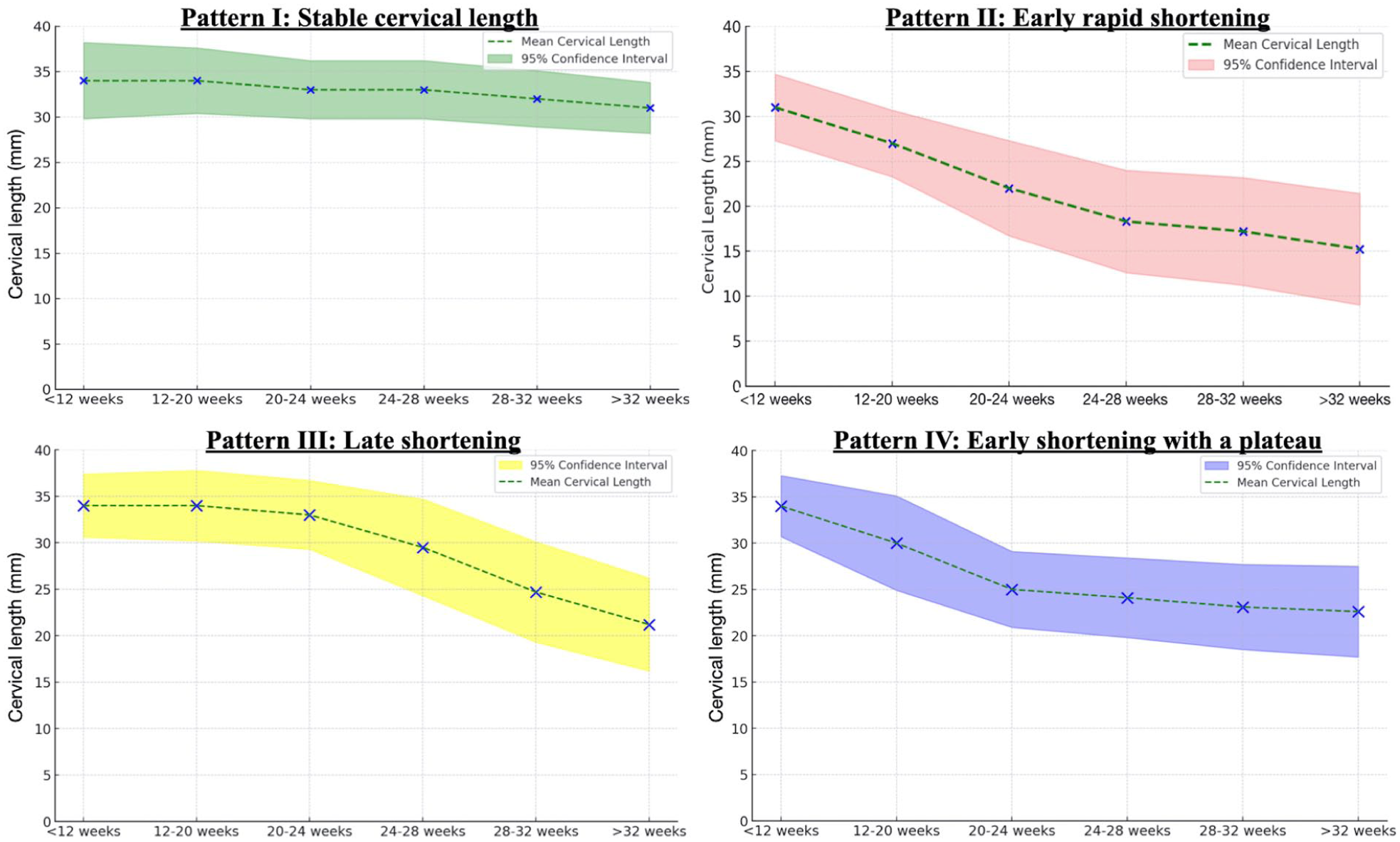
Patterns of cervical length shortening across gestation – Pattern I (Stable cervical length), Pattern II (early rapid shortening), Pattern III (late shortening) and Pattern IV (Early Shortening with a plateau).
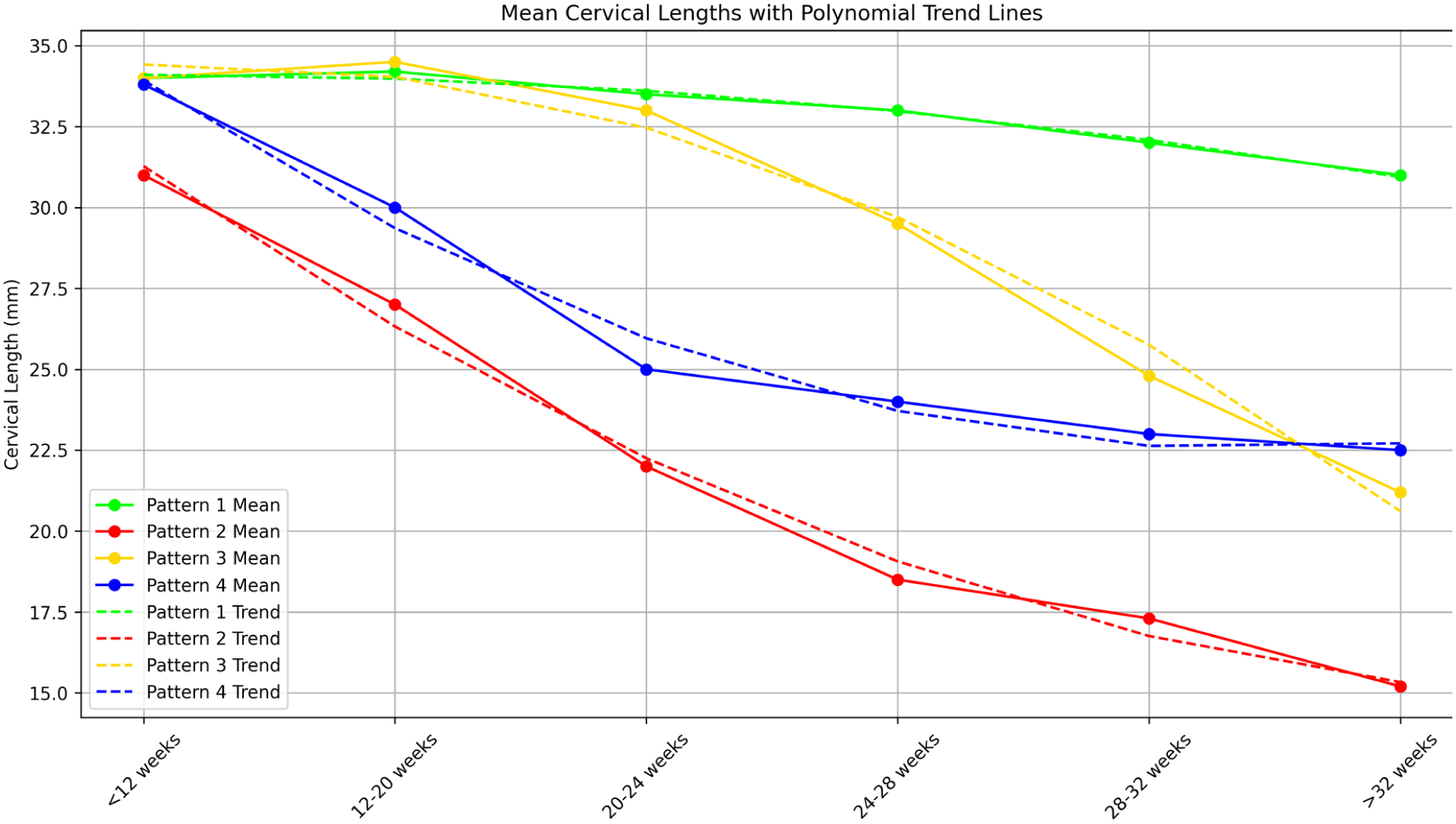
Mean cervical lengths of each pattern with polynomial trend lines.
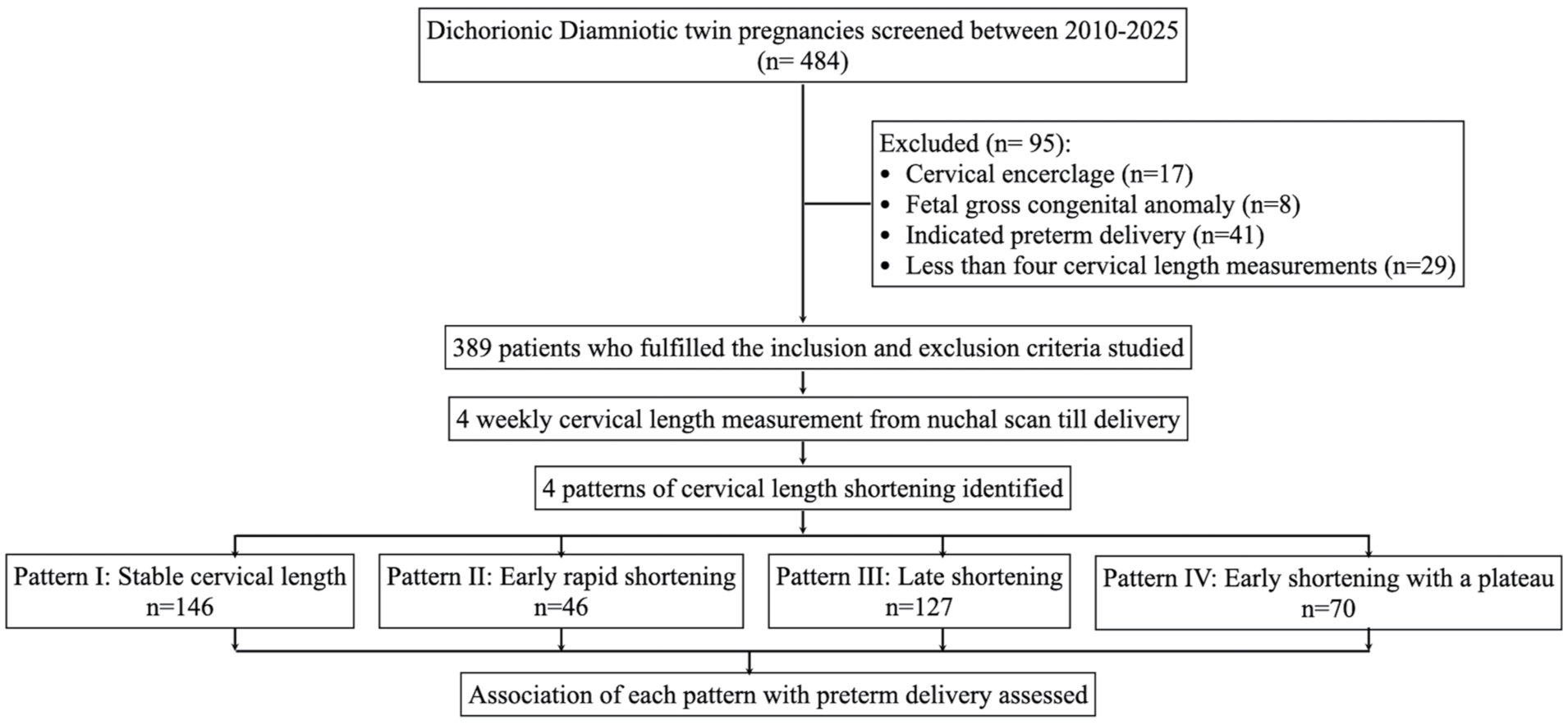
Flowchart of the methodology of the study.
SPSS version 29 was used for hypothesis testing. The data were entered in Microsoft Excel and analysed. Quantitative variables between the different groups were compared using the unpaired Student’s t-test. A one-way analysis of variance (ANOVA) calculator was used to compare means across the four groups. Post hoc Turkey HSD (honestly significant difference) (Beta) was used for pairwise comparison within ANOVA data. The proportions of PTBs across the four patterns were compared using the chi-square test. A t-test calculator for comparison between two independent means was used to compare the mean cervical length between Patterns II and IV at different gestations. A p-value of less than 0.05 was taken as significant.
Results
Baseline characteristics of the study population
We analysed 389 women with DCDA twin pregnancy who underwent a total of 1915 cervical length measurements across gestations. Each woman had a median of five cervical length measurements performed during pregnancy. The period of gestation (POG) at delivery, birth weight and the gender were recorded. The baseline characteristics of the study population are shown in Table 1.
Baseline characteristics of the study population.
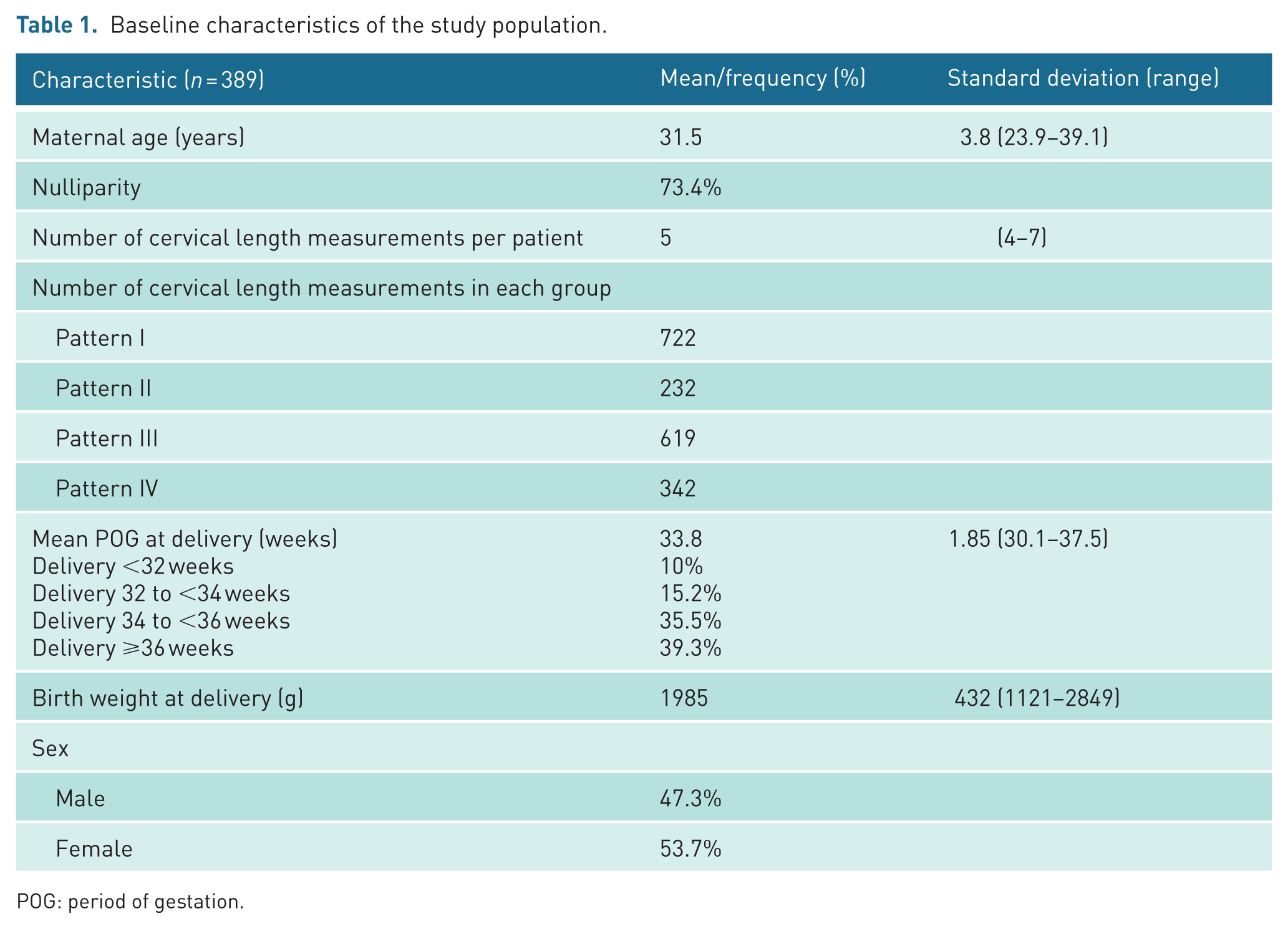
POG: period of gestation.
Patterns of changes in cervical length measurements across gestation
Four distinct patterns of changes in cervical length across gestation were recognised. Pattern I – St CxL was observed in 37.5% cases (n = 146), Pattern II – ERS before 24 weeks’ gestation was found in 11.8% (n = 46), Pattern III – LS after 24 weeks’ gestation in 32.6% (n = 127) and Pattern IV – EPl in 18% (n = 70). The incidence of each pattern of cervical length shortening is demonstrated in Figure 4.
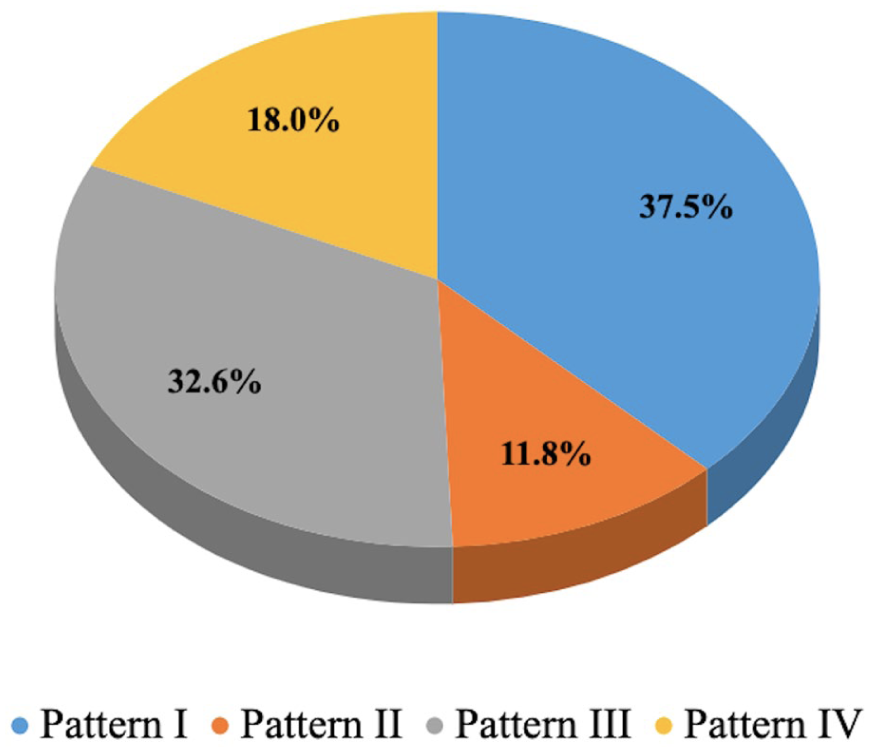
Incidence of each pattern of cervical length shortening.
Rate of preterm delivery in each pattern
To assess the prognostic value of each pattern of cervical length shortening, the rate of preterm delivery in each pattern was analysed. Using 32 weeks’ gestation as the WHO-defined cut-off for “very preterm” birth, the number of patients delivering before 32 weeks was compared across the four groups. The proportion of patients delivering preterm was highest in Pattern II (ERS), followed by Pattern III (LS) and least in Patterns I (St CxL) and IV (EPl), and this difference was statistically significant (Table 2). Pattern I (St CxL) was found to have the highest association with term delivery (at or after 36 weeks). The rate of PTB associated with each pattern of cervical length shortening is demonstrated in Figure 5.
Proportion of patients delivering preterm (before 32 weeks of gestation).

EPl: early shortening with a plateau; ERS: early rapid shortening; LS: late shortening; St CxL: stable cervical length.
The comparison wherein the values are statistically significant (p-value less than 0.05) have been bolded.
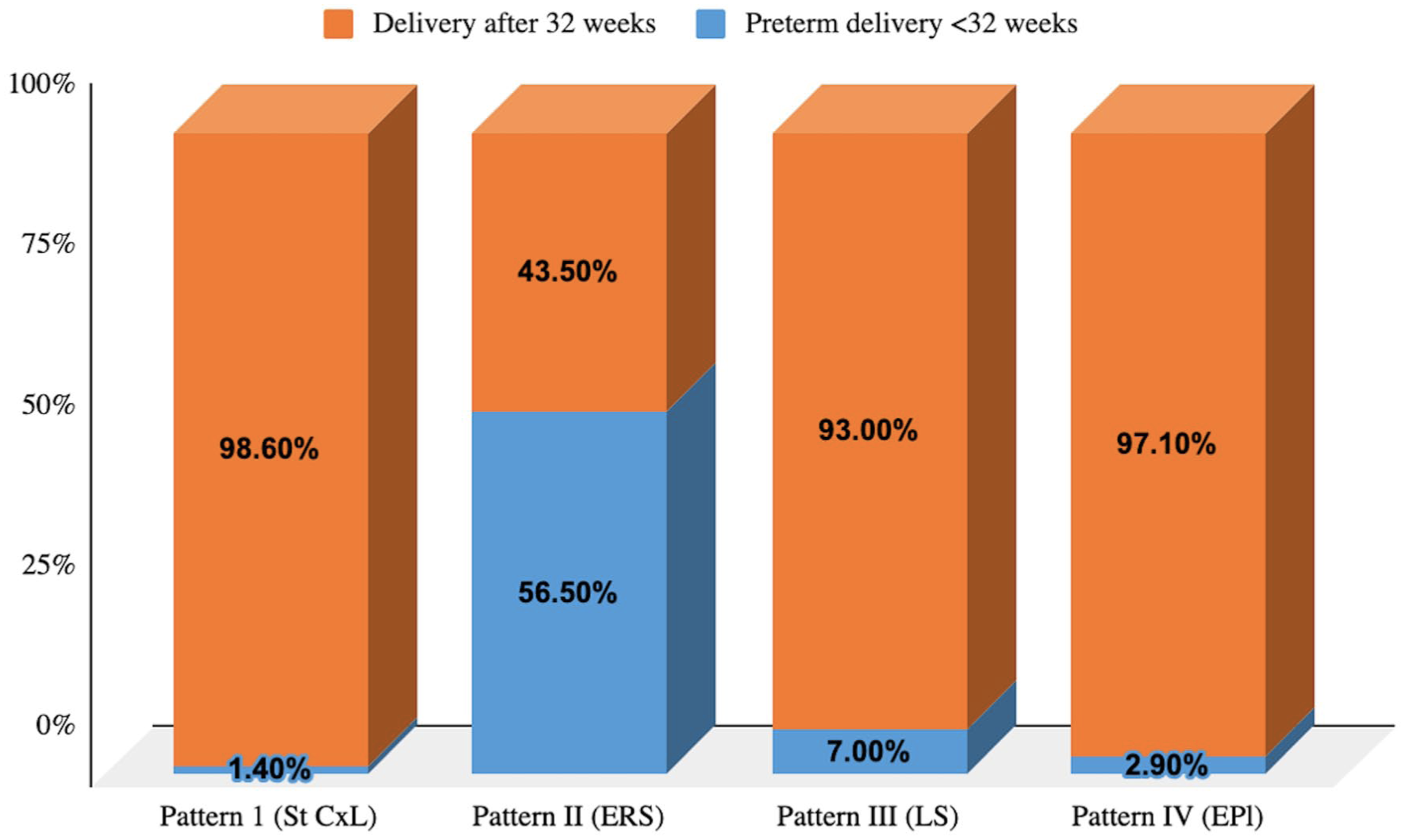
Rate of preterm birth associated with each pattern of cervical length shortening.
The mean POG at delivery was 35.5 weeks in case of Pattern I (St CxL), 30.7 weeks in Pattern II (ERS), 34.2 weeks in Pattern III (LS) and 34.9 weeks in Pattern IV (EPl), and this difference was statistically significant. The mean POG at delivery in each pattern of cervical length shortening is shown in Table 3. Pairwise comparison showed a significant difference in the rates of PTB between Patterns I and II, I and III, II and III, and II and IV (Supplemental Table 1).
Period of gestation at delivery.
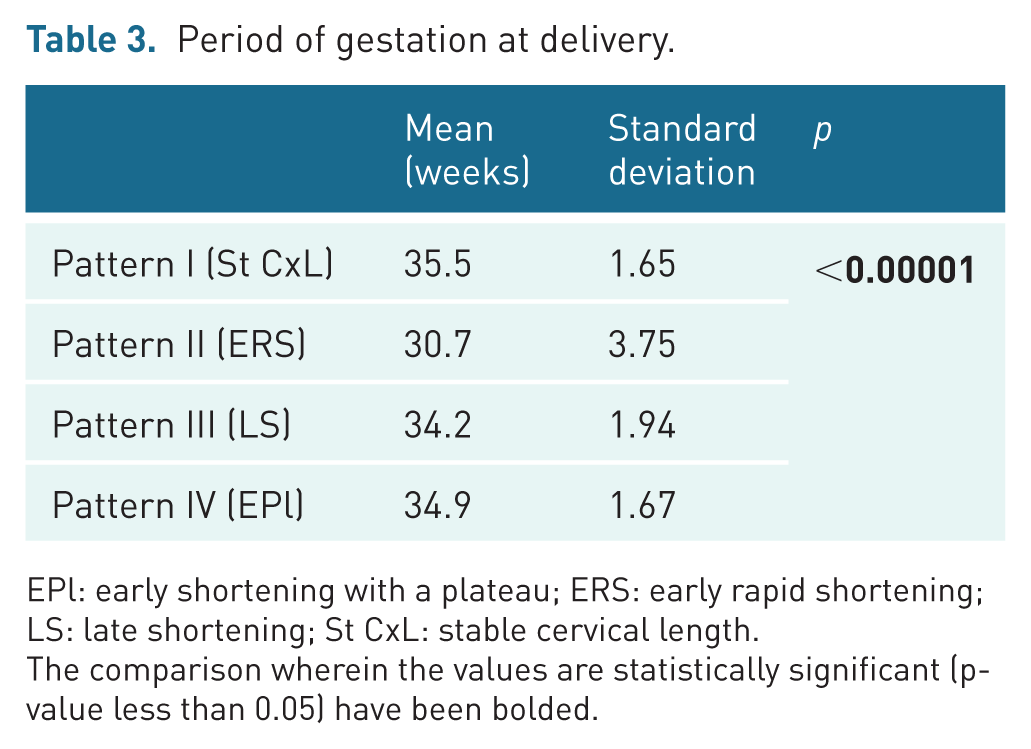
EPl: early shortening with a plateau; ERS: early rapid shortening; LS: late shortening; St CxL: stable cervical length.
The comparison wherein the values are statistically significant (p-value less than 0.05) have been bolded.
Birth weight at delivery
As the neonatal outcomes depend not only on the POG at delivery but also on the weight of the baby at birth, the birth weights were compared across the groups. The mean birth weight at delivery was highest in Pattern I (St CxL), followed by Pattern IV (EPl), and least in Pattern II (ERS), and this difference was statistically significant (Table 4). Pairwise comparison showed a significant difference in the birth weights between Patterns I and II, I and III, II and III, and II and IV (Supplemental Table 2).
Birth weight at delivery.
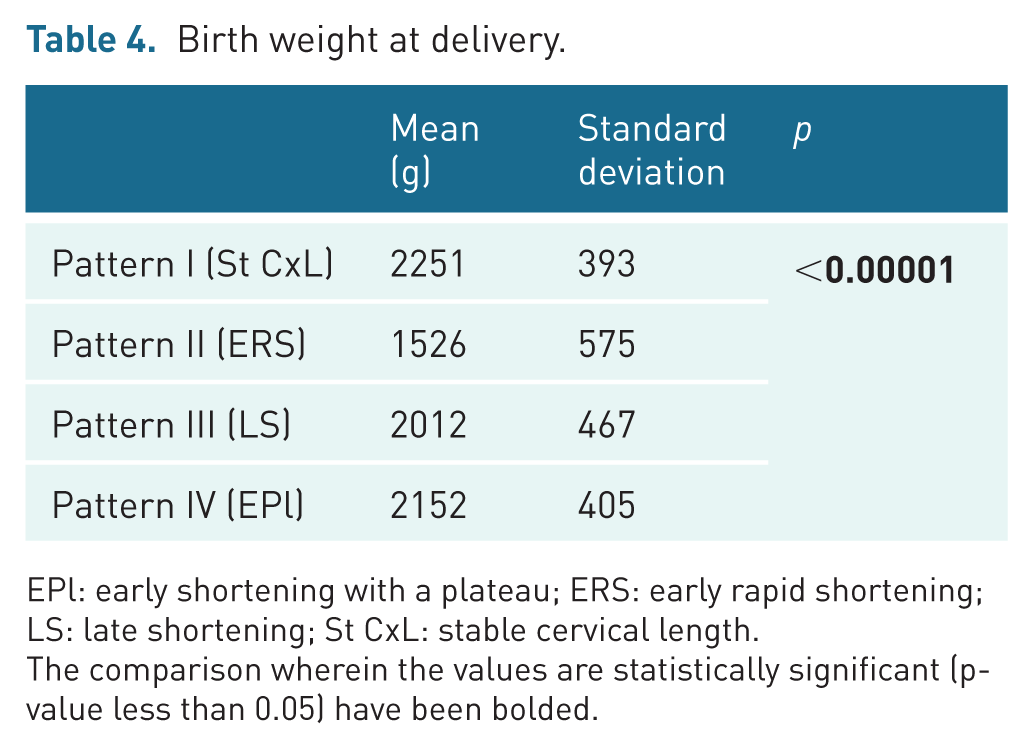
EPl: early shortening with a plateau; ERS: early rapid shortening; LS: late shortening; St CxL: stable cervical length.
The comparison wherein the values are statistically significant (p-value less than 0.05) have been bolded.
Comparison between Patterns II and IV
As Pattern II (ERS) and Pattern IV (EPl) are both associated with early shortening but with dramatically different outcomes, parameters differentiating the two were studied. The mean cervical length was found to be significantly less in Pattern II (ERS) as compared to Pattern IV (EPl) at the time of nuchal scan and between 20 and 24 weeks. The change in cervical length (delta) between 12–20 weeks and 20–24 weeks was significantly greater in Pattern II (ERS) as compared to Pattern IV (EPl). A comparison between the mean cervical length measurements between Patterns II and IV is depicted in Table 5.
Comparison between mean cervical lengths (mm) between Patterns II and IV.
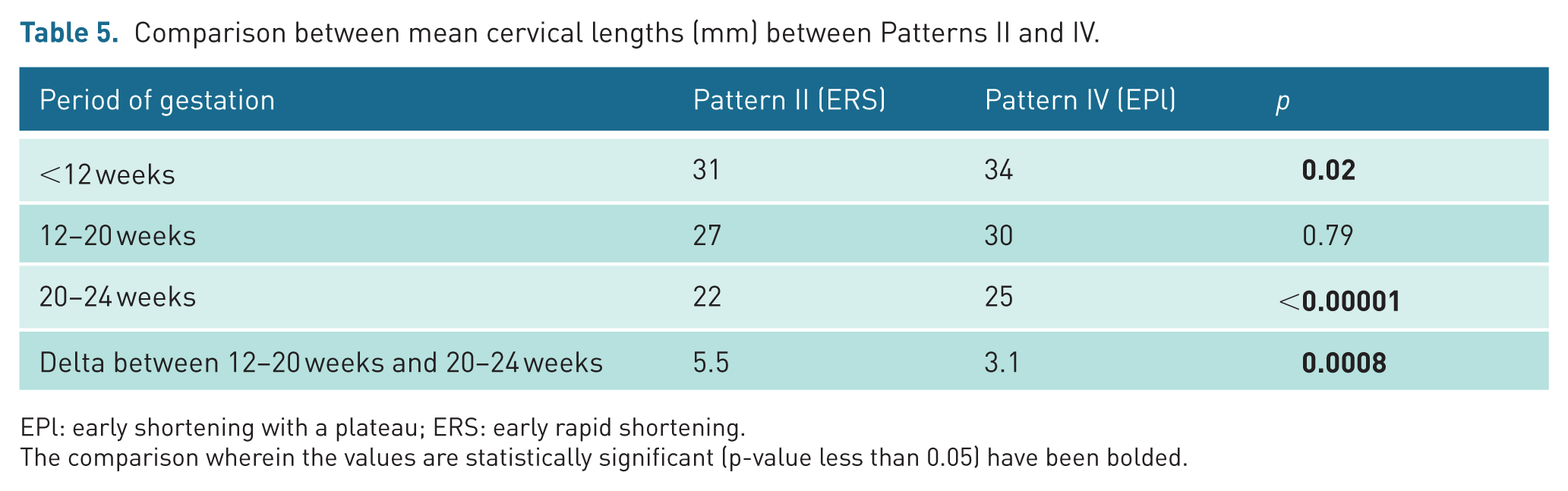
EPl: early shortening with a plateau; ERS: early rapid shortening.
The comparison wherein the values are statistically significant (p-value less than 0.05) have been bolded.
Discussion
Principal findings of the study
Four patterns of changes in cervical length across gestation were found in uncomplicated DCDA twin pregnancies – Pattern I (St CxL), Pattern II (ERS), Pattern III (LS) and Pattern IV (EP1). The proportion of patients delivering preterm was significantly higher in Pattern II (ERS), followed by Pattern III (LS) and least in Patterns I (St CxL) and IV (EPI). The mean POG at delivery was 35.5 weeks in case of Pattern I (St CxL), 30.7 weeks in Pattern II (ERS), 34.2 weeks in Pattern III (LS) and 34.9 weeks in Pattern IV (EPl). Patients in Pattern II (ERS) had a significantly shorter mean cervical length at both the nuchal scan and at 20–24 weeks, as well as a significantly greater decline in cervical length between these two time points, compared with those in Pattern IV (EPl).
Results and clinical implications
Cervical length measurement using the transvaginal route is the most widely used and pragmatic method for predicting the risk of spontaneous PTL. 25 Most studies propose a cervical length cut-off of 25 mm to assess the risk of PTL. 26 Although multifetal pregnancies are at a higher risk of PTL, the data on the normal cervical length in these pregnancies are limited. 27 Akar et al. 27 proposed a value of 36 mm as the median of cervical length in twin gestations. The earlier a short cervix is detected, the higher the risk of PTL.6,7
Although cervical length shortening can predict increased risk of PTB, conversely, a normal cervical length is not equally accurate in ruling it out. 23 Pagani et al. 28 in a retrospective study questioned the utility of cervical length assessment in asymptomatic females with twin gestations. The measurements of cervical length in their study were found to overlap between pregnancies that delivered preterm and in those that progressed beyond 32 weeks’ gestation, and hence, they concluded that cervical length assessment will likely fail to detect a significant number of twin pregnancies that ultimately deliver preterm. 28 We hypothesised that, rather than relying on a fixed cervical length cut-off, classifying pregnancies based on patterns of cervical shortening may offer a more effective approach in stratifying the risk of PTL.
Serial monitoring of cervical length in twin pregnancies is now being adopted to allow timely detection of pregnancies at risk. 29 A possible strategy of interpreting changes in cervical length measurements across gestation is by dividing them into various recognisable patterns, 21 as was also used in our study. Serial measurements and classification into patterns can help in classifying patients at risk better than a single mid-trimester measurement. 21 The data on patterns of cervical length shortening and their individual associations with the risk of PTB are still limited and conflicting.23,25
Wu et al. 25 classified the patterns of cervical length shortening into two categories, namely stable cervix and shortened cervix. They concluded that the risk of PTL was two times higher in the shortened cervix subgroup. 25 Melamed et al. 21 identified four patterns of shortening and concluded that the subgroups that showed cervical length shortening were associated with a significantly higher risk of PTL. Khalil et al. 30 reported no difference in the predictive values of first cervical length measurement at 20–23 weeks, a follow-up measurement 3–5 weeks later and a change between the two. A similar observation was made by Levêque et al., 31 who compared the cervical length at 22 weeks and 27 weeks. However, these studies may be limited by the variability in the POG at which the cervical length measurements were done and by the different definitions of cervical length shortening used. Also, most of the published studies are restricted by the comparison of only two successive cervical length measurements. 21 The primary strength of our study was the number of cervical length measurements done for each patient (a median of five measurements per patient), which allows for better identification of the pattern of shortening. Our study also shows that each pattern is associated with a different risk of preterm delivery, with Pattern II (ERS) showing the highest risk at 56.5%, followed by Pattern III (LS) at 7%, while Patterns IV (EPl) and I (St CxL) had significantly lower risks at 2.9% and 1.4%, respectively.
As the International Society of Ultrasound in Obstetrics and Gynecology guidelines on the management of twin pregnancies already suggest four weekly scans in dichorionic twins, 24 an opportunistic transvaginal cervical length assessment at each visit can prove truly beneficial in recognition of pregnancies at risk of PTL. However, patient acceptability with respect to multiple transvaginal ultrasounds examinations remains to be studied.
In published literature, the mid-trimester cervical length measurement before 24 weeks’ gestation is considered to be the best predictor of the risk of PTL 6 in both singleton 32 and twin pregnancies.32–37 Given that by 24 weeks’ gestation, the mechanical pressure exerted on the cervix due to the fetal weight is sufficient to induce shortening in cases of an incompetent cervix, this gestational age can be considered an appropriate time for routine cervical length assessment in twins as well. Although pattern recognition is typically retrospective, 24 weeks can be used as a reference point since it marks the threshold of viability in Western countries. Even in countries with a viability threshold of 28 weeks, 24 weeks is more pragmatic, as many women come for a mid-trimester scan around this time. Also, as in our study, by this time most pregnancies have undergone at least three cervical length measurements, allowing clinicians to estimate which pattern they are likely to follow.
Identification of the patterns of shortening can help in the timely detection of pregnancies that may benefit from interventions. It is well established that the use of vaginal progesterones is effective in the prevention of spontaneous PTL. 38 Cervical cerclage also has an important role in preventing PTL in twin pregnancies. 39 We hypothesise that the pregnancies falling into Pattern II (ERS) may reflect subclinical inflammation (e.g. intrauterine infection and deciduitis) or cervical insufficiency, where the cervix structurally weakens early in pregnancy, causing abrupt shortening even in the absence of contractions. These pregnancies may benefit from the timely placement of a cervical cerclage. The other group associated with an increased risk of PTL, that is, Pattern III (LS) could be associated with increasing mechanical stress from fetal growth and uterine distension, especially in the third trimester, or with hormonal triggers closer to natural parturition. These are likely to benefit from the use of progesterone supplementation, especially in cases of cervical length <30 mm. 40 These hypotheses are speculative and should be interpreted cautiously, given the retrospective design of the study and absence of standardised intervention protocols. Prospective studies are required to establish the pathophysiology of each pattern, the timing of the insult that activates remodelling of the cervix at a specific gestation and to determine whether management tailored to cervical length patterns improves outcomes. This can help to assess the type of intervention that will benefit each.
The findings of our study can help not only in counselling patients about the risk of preterm delivery but also in making other important decisions, such as the timing of administration of steroids for fetal lung maturity and MgSO4 for fetal neuroprotection, thus achieving a favourable perinatal outcome.
Research implications
Further prospective studies with a larger sample size are warranted to determine the different patterns of cervical length shortening and to determine tailored interventions for each pattern. It is possible that more than four patterns of changes in cervical length may be identified if a larger sample size is used.
Strengths and limitations
The primary strength of the study was the large sample size, measurement of cervical length performed at a single centre by trained examiners using a standardised technique and exclusion of the cases who underwent cervical cerclage and those with indicated or iatrogenic PTB. To the best of our knowledge, this is the second study that involves the evaluation of more than two cervical length measurements for each patient. By emphasising a structured visual classification of cervical length trajectories, our study offers a pragmatic approach, enabling clinically meaningful pattern recognition. The primary limitation is the retrospective nature of the study. Further limitations include a lack of information about the groups excluded from the study, non-uniform timing of cervical length assessments, a lack of specified time intervals that define the patterns and incomplete availability of data on certain established risk factors for PTB, such as prior preterm delivery, prior cervical surgery and screening for maternal infections such as asymptomatic bacteriuria. Exclusion of the cases with insufficient cervical length measurements (to allow classification into one of the predefined cervical length patterns) may have caused selection bias, as pregnancies with very early PTB or, conversely, very favourable outcomes may be underrepresented. The effect of the use of progesterone supplementation on the change in cervical length was not assessed in our study. It can be argued that the use of progesterone supplementation could have reduced the risk of preterm delivery. Although the use of progesterone was broadly similar across groups, residual bias may still exist due to the retrospective nature of the study. Because management decisions were individualised and not protocolised, the observed associations between cervical length patterns and PTB should be interpreted as descriptive rather than causal. Prospective studies with standardised management protocols are needed to validate these findings.
Conclusion
In uncomplicated DCDA twin pregnancies, distinct patterns of cervical length shortening can be observed across gestation, each carrying a distinct risk of PTB. As the trajectory of cervical change over time can be more informative than a single measurement, routine cervical length assessment at successive ultrasound examinations may provide a practical approach for identifying pregnancies at higher risk of preterm delivery.
Supplemental Material
sj-docx-1-ult-10.1177_1742271X261443849 – Supplemental material for Tracking the trajectory of cervical length dynamics in uncomplicated dichorionic diamniotic twin pregnancies: A retrospective cohort study
Supplemental material, sj-docx-1-ult-10.1177_1742271X261443849 for Tracking the trajectory of cervical length dynamics in uncomplicated dichorionic diamniotic twin pregnancies: A retrospective cohort study by Ishita Agarwal, Akshatha Prabhu, Vartika Mohan and Anita Kaul in Ultrasound
Supplemental Material
sj-docx-2-ult-10.1177_1742271X261443849 – Supplemental material for Tracking the trajectory of cervical length dynamics in uncomplicated dichorionic diamniotic twin pregnancies: A retrospective cohort study
Supplemental material, sj-docx-2-ult-10.1177_1742271X261443849 for Tracking the trajectory of cervical length dynamics in uncomplicated dichorionic diamniotic twin pregnancies: A retrospective cohort study by Ishita Agarwal, Akshatha Prabhu, Vartika Mohan and Anita Kaul in Ultrasound
Footnotes
Acknowledgements
None.
Ethical considerations
The study was approved by the Institutional Review Board of Indraprastha Apollo Hospital (approval number: IAH-BMR/032/09-25). The study was conducted in accordance with the ethical principles of the Declaration of Helsinki.
Guarantor
On behalf of all authors, Dr Akshatha Prabhu will act as the guarantor and will guarantee the manuscript’s accuracy and contributorship of all co-authors.
Contributors
I.A. played a central role in drafting the manuscript. A.P. and V.M. were involved in conceptualization and designing the manuscript. The data analysis and interpretation were performed by I.A. A.K. provided mentorship for the project.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Permission from patient(s) or subject(s) obtained in writing for publishing their case report
Yes: Written informed consent was obtained from the patients for their anonymous information, including the images to be published in this article.
Permission obtained in writing from the patient or any person whose photograph is included for publishing their photographs and images
Yes.
Confirm that you are aware that permission from a previous publisher for reproducing any previously published material will be required should your article be accepted for publication and that you will be responsible for obtaining that permission
Yes.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.