
Abstract
Although leadership literature increasingly recognizes that leadership is a complex, co-creational process among leaders, followers, and context, destructive leadership scholarship has only recently embraced this paradigm. This article contributes to the toxic triangle debate by linking destructive leadership theory and disaster research in a case study of Bristol Royal Infirmary, a UK hospital that experienced a crisis in its pediatric cardiology unit resulting in the death of dozens of babies undergoing surgery. Thus, the article expands the literature on organizational failure by offering an assessment of how seemingly good, well-intentioned professionals can nonetheless create destructive leadership dynamics and proposes a new, more nuanced theoretical framework called organizational Munchausen syndrome by proxy as a way to analyze what went wrong.
The story of the paediatric cardiac surgical services in Bristol is not an account of bad people. Nor is it an account of people who did not care, nor of people who willfully harmed patients. It is an account of people who cared greatly about human suffering, and were dedicated and well-motivated … [Instead] there was a lack of leadership … in the care provided to very sick children.
Professor Ian Kennedy, chair of the Public Inquiry into children’s heart surgery at the Bristol Royal Infirmary, UK (Kennedy, 2001: 1)
Introduction and outline
Research has shown how bad, intentionally destructive leaders can have a detrimental influence on organizational performance (Aasland et al., 2009; Delbecq, 2001; Einarsen et al., 2007; Padilla et al., 2007; Schyns and Schilling, 2013; Thoroughgood and Padilla, 2013; Thoroughgood et al., 2011, 2012a, 2012b; Tourish and Vatcha, 2005). Yet, leadership scholars have paid less attention to the ways that seemingly good, well-intentioned leaders can nonetheless become destructive, in part, because there are few frameworks available to guide us in this analysis (Karakitapoğlu-Aygün and Gumusluoglu, 2013; Reed, 2012; Schilling, 2009). This case study of Bristol Royal Infirmary (BRI) provides just such a framework, analyzing how a complex confluence of unusual organizational dynamics created a destructive environment despite the good intentions of medical professionals and contributed to the death of dozens of babies undergoing open heart surgery (Kennedy, 2001). Pressured by outraged parents and a concerned media, the hospital finally terminated the questionable surgical operations. Nevertheless, the BRI incident was “dubbed the medical scandal of the century” and sparked the largest, most expensive medical inquest in UK history (Dyer, 1998: 1691).
Much has already been written about the BRI case in medical, science, and law journals (See for example, Aylin et al., 2001, 2004; Baker, 2001; Horton, 1998; Kewell, 2011; Klein, 1998; Quick, 1999; Weick and Sutcliffe, 2003). Yet despite this attention, few leadership scholars have investigated the leadership failures that the Parliamentary Inquiry so clearly emphasized in the quote above. Moreover, analysis of how such a destructive dynamic developed and was sustained for seven years among purportedly dedicated, caring, and highly trained medical professionals has been conspicuously absent. This article focuses on this question offering an example of how organizational performance can suffer from unintentionally destructive leaders and susceptible followers in a conducive environment (Padilla et al., 2007), particularly when leaders become fixated on the pursuit of idealized goals (Kayes, 2004, 2005) and the use manipulative methods of influence (Krasikova et al., 2013).
In order to understand the dynamics of the toxic triangle at BRI, a new theoretical framework called organizational Munchausen syndrome by proxy will be introduced. The theoretical underpinnings of this framework are based on the psychological disorder Munchhausen, a term first adopted by British physician Richard Asher in 1951 to describe patients who fabricate ailments in order to gain attention, and through their illness, manipulate others (Mart, 2002). In 1977, Roy Meadow introduced a variation called Munchhausen syndrome by proxy to describe a caregiver who systematically concocts stories about another person’s health—typically a child or elder parent, even intentionally making the person sick—as a way to gain access to power within the healthcare system. Since then Munchhausen by proxy has been studied extensively in the medical field (Chan et al., 1986; Day and Moseley, 2010; Libow and Schreier, 1986; Mart, 2002; Meadow, 1982, 2002; Murray, 1997; Parnell, 1998; Rogers, 2004; Rosenberg, 1987; Schreier and Libow, 1993; Sheridan, 2003; Wilczynski, 1995).
Although there is little unified agreement on the defining dynamics of Munchhausen by proxy, one agreed-upon element is that it is grounded in a collusive fantasy that draws family, medical professionals, and outsiders into a web of dysfunctional dynamics that continues to escalate, often ending with the death of the child (Libow and Schreier, 1986; Schreier and Libow, 1993). While Munchhausen by proxy is more common in mothers, fathers often play a part too by acting as passive colluders either through physical absence or emotional distance. Physicians collude as well becoming drawn into the Munchhausen fantasy through a complicated need to be perceived as caring, helpful, and concerned, and their own hubris to solve a difficult medical case and be seen as competent amongst their peers. Outsiders and other medical professionals join in too by not questioning, confronting, or clarifying the mother’s stories, contacting the father to gain more insight, or investigating the peculiar situation (Schreier and Libow, 1993).
Critical motivations behind Munchhausen by proxy mothers’ dysfunctional behaviors is an obsession with control, fixation on authority, and overwhelming need to be in a relationship with physicians and medical institutions in order to feel important. The child becomes just an object, used to gain access to authority figures and maintain connection to power. However, far from appearing strange, Munchhausen mothers often seem intelligent, articulate and caring: the ideal mother. Well educated about medical conditions, they often work within the healthcare field. Yet, incongruently, they can lack basic social skills, display inappropriate emotions and be simply “too intense” to deal with (Schreier and Libow, 1993: 87). Obsessed with obtaining medical treatment, these doctor-addicts are not interested in hearing medical advice. They are only interested in getting an authority figure to take action. When one doctor denies them the attention they need, they seek treatment elsewhere, going from one medical professional to another (Gregory, 2003). Hence their nicknames as doctor addicts, hospital hobos, and peregrinating problem patients (Libow and Schreier, 1986).
Although Munchhausen by proxy occurs as the result of a complex interplay between destructive caregivers, susceptible groups, and conducive environments making it a helpful heuristic to understand dysfunctional workplace behaviors, it has only recently been applied in the analysis of organizations (Fraher, 2011b). This article expands this application, advancing in more detail the theoretical framework of organizational Munchhausen by linking it with theories of destructive leadership and the case study of BRI.
The article begins by describing the methods used in this study and providing an overview of the BRI case. It then reviews the literature on destructive leadership, clarifying the use of the term within this article, and provides an overview of disaster research. Next, I expand Padilla et al.’s (2007) ‘toxic triangle’ model by analyzing how a confluence of destructive leaders, susceptible followers, and conducive environments allowed organizational failure to occur at BRI. Third, through the use of organizational Munchausen, I address leadership scholars call for theoretical models which uncover the “mechanisms which underlie the empirical relationships between destructive leadership and its antecedents and consequences” (Schyns and Schilling, 2013: 151). During this discussion, I apply Kayes (2004, 2005) and Krasikova et al. (2013), while offering a more nuanced way to analyze the repercussions of the pursuit of idealized goals and destructive methods and the negative organizational outcomes they can produce. I close with a discussion of the implications of this study and a conclusion. By linking destructive leadership theory with disaster research in the application of organizational Munchausen, this study provides a nuanced framework by which to analyze how organizations can drift slowly into decline despite the well-meaning intentions of organizational members.
Methodology
This article predominantly draws on the empirical evidence compiled by the UK government during the Parliamentary Inquiry described previously. In particular, I analyzed the interim and final reports, minutes of meetings, memorandums and other detailed documents, and 96 days of oral evidence and transcripts comprising over 12,000 pages of text available online at the UK’s National Archives.11 In addition, I drew on other references such as books, articles, and newspapers to support my arguments. My decision to focus on this material was influenced by the growing popularity of text-based case studies in organizational research such as Brown (2005) and Stein’s (2000) analysis of Barings Bank, Grey’s (2014) study of Bletchley Park, and Tourish and Vatcha (2005), Stein and Pinto (2011), and Stein’s (2007) examinations of Enron, among other text-based studies.
Methodologically, I read and re-read the archival material breaking the data down into more manageable chunks and compiling lists of potentially interesting features as I tried to tease out the leadership failures the Parliamentary Inquiry emphasized. It quickly became apparent how complex the leadership issues were and why so few organizational scholars had tackled this puzzle. Overtime, I found myself drawn to the lengthy and revealing interviews of, and comments about, three key stakeholders at BRI: the surgeon, the anesthesiologist, and the chief executive. This was when patterns began to materialize and a series of questions emerged in my mind (e.g. what were stakeholders’ motivations to seek or resist confrontation and change? Who would benefit? Why were the pediatric cardiology unit’s (PCU) dysfunctional dynamics allowed to proceed for so long unaddressed?). The answers to these questions began to structure my analysis.
As I repeatedly reviewed and coded the interview transcripts, I embraced Alvesson and Kärreman’s (2007: 1265) suggestion to “aim for more creative ways of theorizing” and sought to identify points of tension or “mysteries” to solve. I adopted Alvesson’s (2010: 195) recommendation to “widen the imagination” and consider connections within the empirical material that may not initially be obvious. I began to see what Gioia et al. (2012: 16) described as emerging “social construction processes” which required me to “focus more on the means by which organization members go about constructing and understanding their experience and less on the number and frequency of measurable occurrences.” Ultimately, I came to recognize that the leadership failure at BRI was a complex, systemic breakdown and through this lens the theoretical construct of organizational Munchausen emerged.
Description of the case
The article’s analysis focuses on events transpiring over a seven-year period beginning in 1988 when BRI pediatric surgeons began a risky new form of open heart surgery and ending with the last infant fatality in 1995, a boy named Joshua Loveday. During this period at least 35 more babies died after open heart surgery than might be expected had BRI been up to the standard of care at other British hospitals (Kennedy, 2001: 4). I begin with Joshua’s death because, although he is the last fatality, events leading up to his operation provide a clear example of organizational Munchausen dynamics.
On 10 January 1995, 18-month old Joshua arrived with his parents at BRI to meet with a cardiac surgeon. Joshua was suffering from a rare congenital heart deformity called transposition of the great arteries in which his heart’s aorta and pulmonary arteries were reversed, connected to the wrong sides of his heart. As a result of this misplacement, oxygen-rich blood circulated back to Joshua’s lungs rather than to his body while un-oxygenated blood circulated throughout his body, often turning him blue (Kennedy, 2001). To rectify young Joshua’s problem, the surgeon recommended a new medical procedure called an arterial switch operation. During this surgery, Joshua’s heart would be stopped and his body sustained by a heart–lung bypass machine so his heart’s arteries could be ‘switched’ to the correct side. Although risky, the operation was imperative because Joshua’s life expectancy was less than seven months without the procedure (Liebman et al., 1969). If the surgery was successful, he had a 90% chance of living an active life into adulthood, an excellent reason to accept the risk and attempt the switch operation (Martins and Castela, 2008).
It was a difficult and demanding medical procedure for the surgeon and his operating room team. Since the arteries of Joshua’s small heart were only about 1 mm in diameter, to complete successfully this delicate operation demanded extensive surgical skill, recent practice, and coordinated teamwork. As it was often impossible to predict exactly what the team would encounter once surgery got underway, doctors had to work together and think on their feet, making decisions quickly so as not to delay the operation and increase the patient’s risks (Kennedy, 2001; Weick and Sutcliffe, 2003). Because of these risks, an emergency meeting had been called within Bristol’s PCU the day before the operation, unbeknownst to Joshua’s parents. Although doctors all agreed that the switch procedure was warranted, some felt Joshua might be better served at a different hospital, one with more experience conducting this unusual operation and a better track record of success (BBC News, 8 June 1998). Yet, despite these concerns, the surgery proceeded as scheduled. Joshua Loveday died after eight hours on the operating table. In response, BRI stopped conducting the difficult and risky switch operation and began an investigation as did the UK government.
The government inquiry determined that BRI had significantly higher mortality rates for babies after open heart surgery than other British hospitals (Kennedy, 2001; Weick and Sutcliffe, 2003). When Bristol’s pediatric cardiac surgical program began in 1988, its performance was roughly equivalent to that of other UK hospitals. However, as other programs improved over the next seven years, BRI did not. Although there were significant clues to indicate things were not progressing well, little was done to intervene. Although doctors possessed the technical skills required to conduct Joshua’s operation, this article demonstrates that a fixation on idealized goals and use of manipulative methods of influence created a destructive leadership dynamic that undermined organizational performance.
Literature review
Leadership literature increasingly recognizes that leadership—positive and negative—is a complex, co-creational process among leaders, followers, and context. As Hunter et al. (2007: 441) described it, “Leadership is an inherently multi-level phenomenon with relationships occurring between leaders and subordinates, leaders and teams, leaders and other organizational leaders, as well as leaders and leaders of other organizations”. Yet, workplace leadership studies often continue to focus on leader traits and behaviors, largely ignoring ways this interrelatedness between leaders, followers, and their environment plays out in real organizations (Padilla et al., 2007; Thoroughgood and Padilla, 2013; Thoroughgood et al., 2012a). Similarly, much of the destructive leadership literature largely ignores destructive leadership as a multilevel phenomenon in favor of examining destructive leader behaviors in individuals. In addition, Alvesson and Sveningsson (2003) noted, leadership is rarely conceptualized as occurring in ordinary mundane, day-to-day work activities. In contrast, research often focuses on heroes (Alvesson and Sveningsson, 2003), celebrities (Thoroughgood and Padilla, 2013), chief executives (Heifetz and Linsky, 2002), and other more romantic images of leaders and leadership (Bligh et al., 2011; Fraher, 2011a). I propose that there is a dearth of research examining how destructive leadership as a multilevel phenomenon occurs in the ordinary, mundane, day-to-day operation of organizational life as well. One cause for this void is the lack of a systemic framework nuanced enough to capture the complex interrelatedness between leaders, followers, and their environment. In this article, I offer such a conceptual framework called organizational Munchhausen to provide one way to account for this destructive collective dynamic.
Destructive leadership
A perennial debate remains within leadership scholarship about the definition of destructive leadership, in part, because definitions of leadership itself are so ephemeral. One side of the destructive leadership dialogue builds upon Yukl’s (2006: 3) definition of leadership as “a process whereby intentional influence is exerted by one person over other people” in a group and organization. By adopting Yukl’s “intentional influence” definition, destructive leadership becomes narrowly defined and limited to repeated inappropriate leader behaviors directly aimed at influencing followers (Harvey et al., 2007; Schyns and Schilling, 2013; Thoroughgood et al., 2011, 2012b). Therefore, to be classified as destructive, a leader must be acting in an intentionally harmful manner toward followers by, for example, bullying, coercing, or otherwise abusing subordinates (Delbecq, 2001; Ferris et al., 2007; Harvey et al., 2007; Reed and Bullis, 2009).
There are limitations to this perspective. It assumes that certain behaviors are always destructive and that the leader displaying these behaviors has bad intentions. In contrast, several recent studies reported ways that bad leader behaviors may actually produce positive results in terms of follower motivation and performance, at least in the short term (Kellerman, 2004; Padilla et al., 2007; Shaw et al., 2011). And other studies found that a destructive leader may simultaneously display good and bad, destructive and constructive behaviors (Einarsen et al., 2007; Hogan and Hogan, 2001). As such, leadership scholars have identified a need for different theoretical constructs.
In contrast to the previous discussion, several destructive leadership scholars have recently shifted the research focus away from questions of intent towards the destructive leader’s capacity to generate negative organizational outcomes (Krasikova et al., 2013; Padilla et al., 2007). Through this lens, an array of possibilities has opened up. For instance, Einarsen et al. (2007) observed that destructive leadership included unintentional acts, highlighting the ways that thoughtlessness, ignorance, insensitivity, or incompetence can be just as destructive as intentionally reckless behaviors. In addition, studies by Skogstad et al. (2007) and Aasland et al. (2009) found that passive leader behavior is widely reported as extremely harmful in organizations. As a result, these authors argued, laissez-faire leadership is not simply a leadership void but should instead be considered a form of destructive leadership.
Krasikova et al. (2013: 1312) attempted to side step the question of intentionality altogether by proposing to judge leader’s destructiveness in two ways: setting destructive goals and using destructive methods of influence. In their definition, adopted in this study of BRI, leaders have agency to decide which goals to pursue and how to achieve them yet, in contrast to previous definitions, destructive leaders may not intend to do harm or even be consciously aware of the harmful implications of their actions. Interestingly, Krasikova and colleagues found that the more a leader perceives their goal achievement is at risk, the more likely he or she is to engage in destructive responses. Similarly, Illies and Reiter-Palmon (2007) studied the relationship between a leader’s pursuit of self-interest and their willingness to be destructive. They found that individuals’ value systems defined and structured leadership problems which in turn affected the way people developed solutions, generating a sort of self-fulfilling prophesy linking flawed values with problematic solutions. Harvey et al. (2007) similarly reported that leaders can become destructive by prioritizing their own personal goals above organizational goals often adopting a short-term decision horizon that benefited them at the expense of the organization.
Kayes (2005: 391) also examined the ways leaders’ goals can result in organizational disaster and identified a dynamic called “the destructive pursuit of idealized goals” as a factor. In an effort to create a desired future, Kayes argued, leaders can become fixated on goal achievement creating unanticipated consequences and followers can be drawn in, highly identifying with the leader’s romanticized image in ways that make it difficult for leaders to abandon their goals even when identified as dangerous or unattainable (Kayes, 2004). “When goals replace learning as a primary motivator, the destructive pursuit of goals begins to take form” (Kayes, 2005: 391). I will return to these important points later in my analysis.
Padilla et al. (2007: 178) similarly shifted destructive leadership definitions away from questions of intent toward a matter of outcomes, noting “the essence of destructive leadership concerns negative organizational outcomes”. As such, they find destructive leadership is seldom entirely destructive, is usually based on leaders’ selfishness and need to manipulate and control, and is rarely intended to directly cause harm. Finally, and most importantly for analysis of the BRI case, Padilla et al. (2007) noted the resultant organizational outcomes are the product of destructive leaders, susceptible followers and a conducive environment.
Researchers who study organizational failure agree that disasters rarely spontaneously occur out of nowhere (Dekker, 2005; Elmes and Barry, 1999; Fraher, 2011b; Kayes, 2004; Perrow, 1984; Reason, 1990; Snook, 2000; Watkins and Bazerman, 2003; Weick, 1993, 1997). Instead, problems often “incubate,” (Turner, 1976: 381) sometimes for years, as organizations slowly “drift towards failure” (Dekker, 2005: 18). These disasters are so inevitable, and the warning signs that precede them are often so clear, scholars have taken to calling them “normal accidents” (Perrow, 1984), not because of their frequency, but because they are the normal consequence of increasingly complex human systems. Bringing destructive leadership theory together with disaster research helps explain how the leadership failures at BRI were not behavioral characteristics of one destructive individual but rather the result of an increasingly complex system’s slow yet steady decline to failure over a seven-year period.
Findings
To understand how this decline occurred, let us now return to the central argument of this article. The following section presents the findings of this case study by first analyzing the three domains of Padilla et al.’s (2007) toxic triangle and then detailing how organizational leaders’ pursuit of idealized goals (Kayes, 2004, 2005) contained manipulative methods of influence (Krasikova et al., 2013) that combined over time and culminated in organizational Munchausen.
A toxic triangle at BRI
A conducive environment
To understand the context within which this tragedy developed, I begin by describing the changes that occurred within the UK National Health Service (NHS) and pediatric cardiology during the period studied. The NHS was established after World War II to provide a comprehensive government financed healthcare system virtually free to all citizens. Between 1948 and the mid-1970s, the NHS organizational structure changed very little (Jones, 2006). But by the mid-1980s, when Joshua’s surgeon was first hired at BRI, it was a system in significant transition. The fundamental driving force behind these changes was a strong political push to control costs and reduce public spending, making governance more efficient. The result was a widespread restructuring and creation of NHS “Trusts” to manage medical affairs at the local level. Fifty-seven healthcare providers including BRI were certified in 1991, four years before Joshua’s death (Jones, 2006).
Destructive leaders
The new NHS Trusts hired hospital managers under renewable contracts which provided an incentive to produce fast results in a short period of time, often at the expense of long-term planning; a factor Illies and Reiter-Palmon (2007) and Harvey et al. (2007) identified as potentially destructive. Most managers hailed from business and industry, not from the healthcare field, making doctors’ behaviors, hospital culture change, and quality of patient care specific areas they were reluctant to address (Kennedy, 2001). As a physician himself, the Bristol CEO was a slightly unusual NHS manager with unique insights into the medical culture. His goal was for BRI to be led by self-managing doctors who were “self-teaching” and “self-correcting” (Kennedy, 2001: 68). As Skogstad et al. (2007) and Aasland et al. (2009) warned, laissez-faire leadership such as this can become destructive and this factor, along with the CEO’s reliance on doctor’s self-management, became a critical factor leading to Joshua’s death and other babies like him.
In addition to changes in the physical structure of the NHS, a shift in thinking about children’s healthcare occurred in the 1980s. No longer viewed as simply ‘little adults’, children were accepted as a unique group of patients with special physiological and psychological needs prompting an increased emphasis on the pediatric healthcare service environment.22 Yet, progress was slow in achieving improvements, particularly at BRI, where there were insufficient numbers of pediatrically trained staff (Kennedy, 2001). In 1986, Joshua’s surgeon was hired as a cardiac surgeon and although he reported feeling welcomed, there was only one other cardiac surgeon on staff and only minimal pediatric cardiology services. He testified at the Parliamentary inquiry that he found Bristol’s facilities “primitive” and felt he had “to find his own place, his own mechanism, and to ask for what he wanted” to build his practice (Kennedy, 2001: Surgeon interview: 16).
Joshua’s surgeon was eager to make his mark and began experimenting with new medical procedures in pediatric cardiology. He recalled, “Right from the beginning, I thought Bristol should really come on par with other” pediatric cardiology centers that I had seen, “if not better” (Kennedy, 2001: Surgeon interview: 67). To accomplish his goals, the surgeon said he tried new ideas and surgical techniques to repair babies’ birth defects at an earlier age. One of these procedures was Joshua’s arterial switch operation. “It was well-known”, the surgeon explained, that this “group of patients” had a “very high mortality; so that is why this” risky operation was first tried with these babies. They had very little chance of living to adulthood without it (Kennedy, 2001: Surgeon interview: 71).
Although Joshua’s surgeon had never tried the ‘switch’ procedure himself and had only assisted another physician once, five years prior, he nonetheless felt confident he was ready. Yet he confessed that when starting a new operation, he did anticipate some infant fatalities as he improved his skills. The surgeon explained: Nobody exactly knew what a learning curve was except for saying that whenever you start any new operation you are bound to have unfortunately high mortality … I do not think any surgeon wants to be seen as in a way practising with his patients but that is the definition of ‘learning curve’ (Kennedy, 2001: Surgeon interview: 42–43).
As one Bristol anaesthetists noted, “there is a particular rivalry between surgery and anaesthesia” and “it is legendary”. The dynamic still exists today, he observed, probably because we “work so closely together … Surgeons do not like to be told what to do by anaesthetists and anaesthetists do not like to be told what to do by surgeons” (Kennedy, 2001: Anaesthetist interview: 132). This anaesthetist also joined Bristol’s PCU in 1988, initially working closely with Joshua’s doctor and the other surgeons. Departmental meeting minutes support that initially the doctors got along well, maintained a professional relationship and spoke often. Yet over time, this anaesthetist claimed, “a clear picture of a problem” emerged within the PCU which he felt “needed to be reviewed” (Kennedy, 2001: Anaesthetist interview: 63). Surgeries were taking too long, he worried, and anaesthetized babies were spending too much time on the heart-bypass machine.
Susceptible followers
As a result of this growing discord, PCU teams fragmented into professional cliques—surgeons became defensive, nurses became skeptical, and anaesthetists became uneasy—undermining leadership, communication, and collaboration in operating room teams. Although there were signs of this performance breakdown along the way, little was done to intervene. Hospital managers’ focus on the short-term and interest in developing a self-managerial model meant there was a reluctance to exercise leadership, monitor doctors’ behaviors, address hospital culture, or improve patient care (Kennedy, 2001). As the Unit slowly drifted towards failure over the years, people struggled to cope with their increasing anxieties, and several dysfunctional organizational dynamics emerged (Dekker, 2005; Fraher, 2011b). Yet, few people raised questions or challenged the decision making of key medical professionals. Parents, desperate to have their sick babies made well, continued to request service.
Destructive goals and methods
Although organizational leaders did not intend to be destructive at BRI they nonetheless pursued idealized goals using destructive methods of influence, often striving for short-term gains of personal interest that harmed the organization (Harvey et al., 2007; Illies and Reiter-Palmon, 2007). For instance, the CEO’s goal was for BRI to be a self-managing hospital, Joshua’s surgeon’s goal was to perfect the switch operation, and the anaesthetist’s goal was to be viewed as the savior of sick babies (Figure 1). Each pursued their respective goal with passion over the seven years preceding Joshua’s death, using whatever means necessary, manipulative and otherwise, to achieve their aim (Krasikova et al., 2013).
Destructive leadership ‘toxic triangle’ at Bristol Royal Infirmary.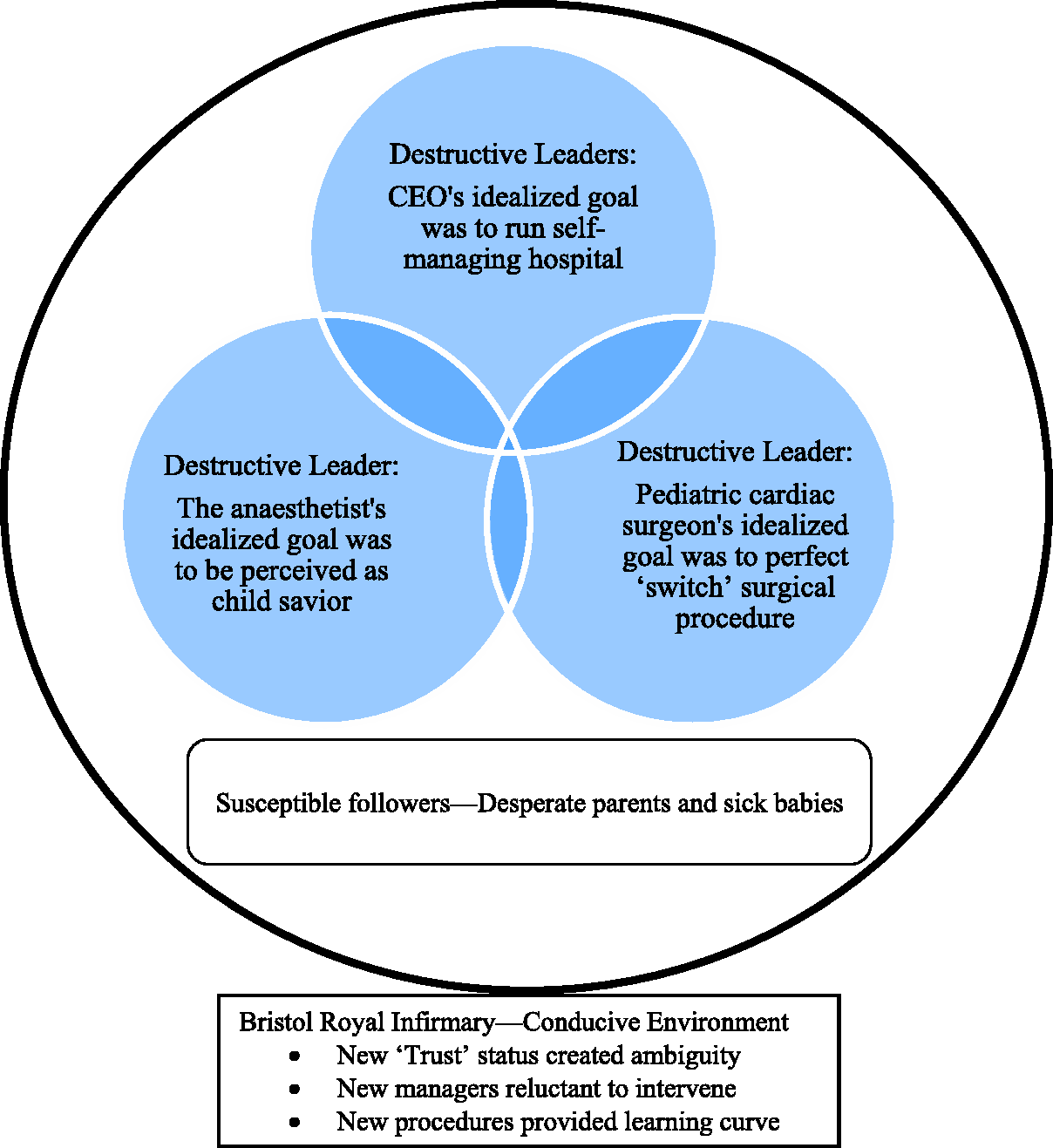
As Krasikova et al. (2013) observed, the more a destructive leader perceives their goal achievement to be at risk, the more he or she engages in harmful activities. There is evidence of this at BRI.
A letter
In 1989, after yet another baby died during cardiac surgery at BRI, the anaesthetist confided to a senior colleague that he suspected there was “a problem” within the PCU. This colleague recalled that the anaesthetist was “absolutely distraught” because he felt surgery at Bristol was taking too long and putting babies at greater risk. However, the senior colleague quickly emphasized, the anaesthetist was not very tactful or “introspective,” and could be volatile, lacking social skills. He “wanted to broadcast” his concerns to “the whole world” without necessarily “having the evidence to back it up.” So the colleague suggested the anaesthetist collect hard data to support his concerns before speaking with anyone else (Kennedy, 2001: Senior colleague interview: 4–5).
Yet, the anaesthetist disregarded this advice, and instead sent a letter to Bristol’s CEO igniting a series of conflicts within the PCU. In retrospect, the anaesthetist claimed his motivation for writing the letter was out of concern “for the safety of children that were dying unnecessarily” and the desire for an open, public review of the PCU’s performance (Kennedy, 2001: Anaesthetist interview: 111). Yet, he never used the word “safety,” never asked for “data,” never demanded an “open review” or even mentioned “unnecessary deaths” in the letter. Perhaps even more revealing about his motivations was his reflection that “the reason for bringing the Chief Executive in” was that “I was a member of the” PCU and surgical data “was not being given or shared with me” (56).
In keeping with new management’s goals of running a self-managing hospital, the CEO took a laissez faire approach and dismissed this letter as inconsequential. Yet, the anaesthetist later conceded his actions created disharmony and mistrust within the unit. Surgeons were angry that a fellow doctor voiced criticism to outsiders and the anaesthetist’s peers were dismayed that established avenues of communication had not been followed and feared they would all look bad with negative consequences for their working relationships with surgeons. As a result, the anaesthetist told the Parliamentary Inquiry that he felt afraid and isolated (Kennedy, 2001: Anaesthetist interview: 113–114).
A study
Yet, the anaesthetist continued his quest to achieve his goal to save sick babies, partnering with an experienced medical researcher to compile secretly their own pediatric cardiology data in hopes of formalizing a complaint. When this researcher wanted to inform the surgeons of their intended study, the anaesthetist disagreed, arguing that talking with surgeons “would impede their task” (Kennedy, 2001: 139). In 1993 after collecting data sets on 233 children who had undergone open-heart surgery at BRI in 1991 and 1992 the study seemed complete.
The results could have been a pivotal opportunity for PCU doctors to discuss ways to improve team performance and jointly consider the open review investigating infant safety that the anaesthetist allegedly desired. Although he had numerous opportunities to raise his concerns publically, the anaesthetist chose to share his data informally, chatting in corridors, in the break room, in taxicabs or dropping by peoples’ offices unscheduled rather than raising his concerns in a formal way. Colleagues repeatedly suggested that he share his data and concerns directly with the surgeons, yet the anaesthetist refused because “he thought this might limit his access” (Kennedy, 2001: 144). Several people questioned the validity of the anaesthetist’s data calling it raw and difficult to interpret. The Clinical Director of Cardiac Services was similarly concerned and directed the anaesthetist to recheck his figures and report back. Yet, the anaesthetist never returned.
An article
Instead of heeding the advice of his colleagues to make his concerns known, the anaesthetist met with a medical reporter from a satirical magazine, Private Eye, and provided information for a series of articles which embarrassingly referred to BRI as “The Killing Fields.” When confronted, the anaesthetist initially denied being the magazine’s source, yet later confessed that he did provide the information because, he told the Parliamentary inquiry, “I needed action,” (Kennedy, 2001; Anaesthetist interview: 53).
As one might expect, the anaesthetist’s lies and actions had a detrimental impact on dynamics within the PCU affecting surgeons’ willingness, in particular, to share information with their anaesthetist colleagues. However, the anaesthetist’s quest to achieve his goal remained undiminished. He shared his research data with a senior medical officer at the Department of Health, who similarly urged him in writing to speak directly with his colleagues and voice his concerns through the proper communication channels established within his hospital. However, the anaesthetist did not and the pattern continued.
In fact, the anaesthetist visited dozens of medical professionals to share his raw and unreliable data. At times, he would be waiting for feedback from one person while continuing to reach out to others, asking them to take action on his behalf. When given advice, he rarely followed it, choosing instead to approach someone new. Most importantly, he never shared his research with either of BRI’s pediatric cardiology surgeons (Dunn, 1998). As a result, it seems clear that although the anaesthetist claimed to be looking for resolution, the manner in which he chose to share his concerns ensured there would be none. To understand more clearly what transpired within the toxic triangle at Bristol’s PCU, I will now discuss the organizational Munchausen framework, providing a definition, and then applying the concept to BRI.
Discussion
Organizational Munchausen defined
A form of destructive leadership, organizational Munchausen syndrome by proxy is a psychological construct that describes an organizational dynamic in which seemingly good, well-intentioned leaders can nonetheless behave irrationally, putting the organization’s health in peril, as they fixate on their pursuit of idealized goals. Like its Munchhausen by proxy namesake, organizational Munchausen is grounded in a collusive fantasy that draws destructive leaders and susceptible followers into a web of dysfunctional dynamics that continues to escalate until death or disaster. Under certain systemic conditions, organizational Munchausen can emerge when three key roles become filled: the abusive “mother,” passive “father,” and collusive community. These roles are metaphoric and may be filled by one or more individuals or groups enacting the dysfunctional patterns of behavior.
Abusive mother role
Organizational members enacting the abusive mother role are attention-seekers who often seem like intelligent, articulate and caring individuals. Yet they deny reality, are obsessed with control and fixated on authority. They often have a frenetic demeanor, lack basic social skills, resist advice, display inappropriate emotions, and are very intense to work with. They live in a fantasy world of their own creation and thrive on manipulating others. For example, as Schreier and Libow (1993: 85) described it, in the Munchhausen by proxy mother’s mind she “becomes the perfect mother in a perverse fantasized relationship with a symbolically powerful physician.” A key sign of organizational Munchausen is the Munchhausen mother’s goal to remain in the limelight, no matter what the cost.
Passive father role
Organizational members enacting the father role play an important part in facilitating organizational Munchausen by acting as passive colluders either through physical absence or emotional distance from the developing organizational dynamics. Fathers may appear less intelligent, incompetent, or uncaring, preferring to defer to others than exercise their own authority. Organizational Munchausen fathers may seem aloof or less devoted, apparently unaware that there is even a problem. Although signs of the organization’s decline may appear obvious, organizational Munchausen fathers rarely raise questions. It is only after disaster strikes that they are shocked into recognizing the severity of the situation. This detachment and surprise is a critical indicator of the presence of organizational Munchausen.
Collusive community role
In order for organizational Munchausen to fully develop, there must be a conducive environment. Just as physicians collude in the Munchhausen by proxy fantasy through a complicated need to be perceived as caring and competent, so too do other organizational leaders play an important part in organizational Munchausen dynamics. Thus the critical third element in the organizational Munchausen triad involves the surrounding community which must also collude with the abusive mother and passive father by not questioning, confronting, or investigating the peculiar situation.
Organizational Munchausen applied
Anaesthetist as organizational Munchausen mother
Like a Munchhausen by proxy mother, the BRI anaesthetist sought out one medical professional after another, over 25 in total, to share his confusing and unreliable data about the PCU’s performance. He manipulated information to suit his needs, while simultaneously depicting himself as the victim: misunderstood, isolated, and powerless. Similar to a Munchhausen mother, he claimed his actions were solely motivated out of concern for children’s health. Yet, when he was advised numerous times to clarify his research results and then use the proper channels of communication to openly discuss his concerns, he never did. In fact several months before Joshua’s death, he had another perfect opportunity to collaborate openly.
Three BRI doctors invited the anaesthetist to dinner with the aim of surfacing his concerns about pediatric cardiology services and clearing the air within the unit. Yet, the anaesthetist did not speak up. Later he explained, he would have “contributed to a debate” if someone else started the conversation but “I did not want to raise the issue” myself. Instead, he said, he wanted others to take action. “That was why I was going through every other route possible to press alarm bells to get somebody to come and deal with the issue,” he emphasized in the Parliamentary Inquiry (Kennedy, 2001: Anaesthetist interview: 180–182). Similar to a Munchhausen by proxy mother, the anaesthetist seemed to revel in the spotlight and the power he gained by manipulating others in authority to take action based on his information. As long as the PCU and babies within it stayed sick, the anaesthetist could continue to strive to achieve his goal as child savior and retain his central role communicating with the media and outside medical community.
While Munchhausen by proxy mothers are typically critical of the hospital’s treatment of their child, they often talk in laudatory terms about the physician him/herself. Preying on the doctor’s hubris is an important part of the Munchhausen by proxy fantasy. Similarly, the anaesthetist was known to describe Joshua’s surgeon as a deeply caring, hardworking doctor who could be found at all times day and night serving the needs of his patients. In fact, the anaesthetist called him “the best paediatric cardiac surgeon in the South West region” (Kennedy, 2001: Anaesthetist interview: 8).
It is difficult to reconcile these competing images and the purpose they served organizationally but the organizational Munchausen model once again proves helpful. Like the anaesthetist, Munchhausen mothers often work within the healthcare field identifying with doctors as an idealized parent, allowing them to deny their own intense dependency needs. Yet they find themselves in a perplexing bind: While they need doctors on whom to project their unresolved ego needs, they simultaneously devalue the very people from whom they seek nurturance. Therefore, although Munchhausen mothers crave attention, they are unable to accept the care they do receive as genuine, leaving them trapped in a hopelessly escalating cycle of frustration (Schreier and Libow, 1993: 87).
Similarly, the anaesthetist seemed to need idealize Joshua’s doctor as “the best surgeon” while also demonizing him for his role in children “dying unnecessarily” (Kennedy, 2001: Anaesthetist interview: 18 & 109). He simultaneously craved attention from the media and outside medical community, yet could not accept that people were interested and listening. This perplexing double-bind led the anaesthetist to act out, becoming overly emotional and highly frustrated at times, as several of his colleagues testified. Although many people urged him to calm down, think before he acted, use appropriate communications channels and talk with the surgeons directly; he could not bring himself to do it and risk losing his position of influence.
Surgeons as organizational Munchausen fathers
Despite the anaesthetist’s secret telephone calls to the Department of Health and the media, and obvious trepidation on the part of some PCU doctors, Joshua’s operation nonetheless went forward. To understand why, we must now examine how Joshua’s surgeon enacted the role of absent and neglectful father in the organizational Munchausen drama. Although the anaesthetist never directly shared his data or his concerns with Joshua’s surgeon, it is difficult to understand how he could not suspect something was amiss or why he remained so aloof. Similar to the unfolding Munchhausen by proxy family dynamic, where it is nearly incomprehensible that fathers do not suspect something unusual is occurring, it remains difficult to explain the surgeon’s inaction. Yet by applying organizational Munchausen it becomes clear. We know of Joshua’s surgeon’s eagerness to perfect his surgical skills and bring Bristol into the forefront as a leading pediatric cardiac surgery center. Because of the surgeon’s fixation on these idealized goals, he was apparently blinded to the unfolding dynamics and unaware that there was even a problem. When called to testify at the Parliamentary Inquiry, Joshua’s surgeon was shocked to recognize the severity of the situation and why people were so concerned about his “learning curve.”
Medical establishment
The critical third element in this organizational Munchausen example is the surrounding medical establishment, the collusive community. As the old NHS system transitioned to the new Trust status, there was confusion at a national level about who was responsible for monitoring quality. Specifically lacking was a clear protocol to monitor new surgical techniques and surgeons’ proficiencies. As a result, the Parliamentary Inquiry found, a gentlemen’s club culture grew at BRI where an imbalance of power put “too much control in the hands of too few individuals” to pursue their individual goals during which “vulnerable children were not a priority” (Kennedy, 2001: 2). Although “Bristol was awash with data”, the inquiry concluded, it was “often partial, confusing and unclear” research with little information provided openly to parents or the general public (3).
During the rocky transition to Trust status, a number of leadership challenges emerged. However, most new managers hailed from business not from healthcare, making supervision of doctors, hospital culture change, and quality of patient care areas they were reluctant to get involved with. As Bristol’s chief executive noted, the widespread understanding of the manager role was “to provide and coordinate the facilities which would allow [doctors] to exercise their clinical freedom,” not to try and influence their behaviors (Kennedy, 2001: 68). The organizational dynamic of deference to authority, overreliance on doctor’s self-management, and reluctance to confront each other’s behaviors became a particularly destructive element.
Implications and conclusion
The events surrounding the deaths of the Bristol babies became the subject of the longest medical inquiry in UK history at a cost of over $20 million (Baker, 2001). Written evidence from 577 witnesses including 238 parents, medical records of over 1800 children, and 900,000 pages of documents were considered along with individual testimony taken over 96 days (Kennedy, 2001: 1). In sum, Kennedy’s (2001) Parliamentary Inquiry reported pediatric cardiac surgical services at Bristol were “frankly not up to the task” (7). Rather than “a deterioration in standards,” the government inquiry found a lack of leadership and “a failure to progress” in the surgical learning curve in young infants (4–5). However, BRI organizational leaders did not intend to be destructive. As the public inquiry noted, this case involved good, well-meaning people who cared greatly about human suffering, and were motivated and dedicated. They simply failed to learn as several key stakeholders pursued idealized goals using manipulative methods of influence.
This article offered a conceptual framework nuanced enough to unpack the dynamics of this organizational failure called organizational Munchhausen syndrome by proxy. Through this framework it becomes apparent how destructive leadership can be a multilevel phenomenon occurring between well-intentioned leaders, followers, and their environment in the ordinary, mundane, day-to-day operation of organizational life. However, additional ways to understand how organizational failure can become embedded in the everyday operations of work life and cause a slow, steady drift towards failure are required. For example, although the results of disasters such as the 2010 British Petroleum Deepwater Horizon oil spill in the Gulf of Mexico, 2011 Fukushima Daiichi nuclear power plant meltdown in Japan, or 2014 General Motors recall of over six million cars due to ignition failures that caused at least 13 deaths, have demonstrated dysfunctional organizational dynamics, less is known about how these dynamics developed over time and through what means.
What could have been done to break this dysfunctional cycle? Like its namesake, Organizational Munchausen can only emerge when the three critical roles are fully enacted. Therefore, if people question suspicious dynamics, challenge taken for granted assumptions, and confront others’ behaviors, organizational Munchausen cannot take hold. However, as the Parliamentary inquiry noted, “Even today it is still not possible to say, categorically, that events similar to those which happened at Bristol could not happen again in the UK; indeed, are not happening at this moment” (Taylor, 2001: 11). Therefore, the field of leadership studies needs more theoretical frameworks and analysis of real-world case studies in order to better understand the nuance of how destructive leadership dynamics can occur in the workplace. Only then might we begin to understand ways to avoid the events that transpired at Bristol.
Footnotes
Acknowledgement
Thanks go to Nadine Tchelebi, Kathleen Jones, Dennis Tourish, and the anonymous Leadership reviewers for their helpful comments.