
Abstract
Background:
Musculoskeletal disorders are increasingly recognized as conditions involving extracellular matrix dysregulation, characterized by fibrosis, calcification, fascial adhesions, and altered nociceptor signaling. These features highlight the role of mechanobiology in pain generation and modulation. Ultrasound-guided hydrodissection has emerged as an intervention capable of perturbing the extracellular microenvironment, with potential downstream effects on nociceptive pathways.
Methods:
A structured literature search was conducted across PubMed/MEDLINE, Embase, Scopus, Web of Science, and the Cochrane Library (January 2000–March 2026) to identify clinical and mechanistic studies investigating ultrasound-guided hydrodissection, mechanical needling, and sterile water injection. Eligible studies were synthesized qualitatively.
Results:
Thirty studies were included, encompassing randomized trials, observational studies, and mechanistic investigations across multiple pain conditions. Evidence suggests that mechanical and osmotic perturbation of the extracellular matrix may disrupt fibrotic architecture, facilitate fascial plane separation, and modify the local biochemical microenvironment. Hypotonic sterile water has been associated with activation of mechanosensitive and osmosensitive ion channels, including TRPV1, PIEZO1/2, and ASIC, leading to calcium influx–mediated modulation of neuronal excitability. These processes may contribute to peripheral and central nociceptive modulation through integrated mechanobiological and microvascular mechanisms.
Conclusions:
Ultrasound-guided mechanical needling with sterile water hydrodissection represents a mechanobiological approach to modulating nociceptive signaling through extracellular matrix perturbation and ion channel activation. This framework provides a translational basis for targeting structural and microenvironmental contributors to pain.

Keywords
Introduction
Musculoskeletal disorders are a leading cause of years lived with disability worldwide, substantially impairing mobility, functional independence, and quality of life while imposing a significant socioeconomic burden.1–3 This burden continues to rise with population aging, sedentary lifestyles, and increasing metabolic and degenerative conditions.
Contemporary pain science has evolved from a predominantly inflammatory paradigm toward a mechanobiological framework, in which structural, cellular, and neurophysiological processes interact dynamically.4,5 Within this framework, the extracellular matrix functions as an active regulator of tissue mechanics and cellular signaling. Disruption of extracellular matrix homeostasis contributes to pathological remodeling, including fibrosis and calcification, leading to increased tissue stiffness, impaired fascial gliding, and persistent nociceptive input.6,7
Fibrosis, characterized by excessive extracellular matrix deposition and dysregulated tissue repair, alters tissue elasticity and load distribution, while calcification further reduces compliance and may mechanically irritate adjacent neural and soft tissue structures.7,8 In addition, altered fascial structure and reduced tissue glide have been associated with chronic pain, reflecting a close interaction between connective tissue and the nervous system.5,9
At the cellular level, mechanotransduction provides the biological interface linking mechanical stimuli to cellular responses. Cells function as integrated mechanical systems capable of transmitting forces across cytoskeletal and extracellular networks, enabling the conversion of mechanical inputs into biochemical signaling. 10 Mechanosensitive ion channels, including TRPV1 and PIEZO, play key roles in mediating responses to mechanical and osmotic stimuli, contributing to neuronal excitability and peripheral sensitization.11,12
Despite these advances, current management remains largely pharmacological. Long term use of non steroidal anti inflammatory drugs is associated with significant adverse effects, 13 while opioids provide limited sustained benefit and carry risks of dependence and adverse outcomes. 14 Clinical guidelines increasingly emphasize non pharmacological and rehabilitation based approaches, although implementation remains inconsistent. 15
Accordingly, there is a growing need for targeted, image guided, and drug sparing interventions that address both structural and neurophysiological drivers of pain. Ultrasound guided mechanical needling combined with hydrodissection represents a promising approach, integrating mechanical modulation of pathological tissue alterations with mechanobiological mechanisms of pain modulation. 16
This narrative review synthesizes current clinical and mechanistic evidence and proposes a clinically applicable mechanobiological framework for ultrasound guided mechanical needling and hydrodissection in the management of chronic musculoskeletal pain.
Literature search strategy
This review integrates relevant clinical and mechanistic evidence on ultrasound guided mechanical needling, hydrodissection techniques, and sterile water injection in the management of musculoskeletal pain.
A structured literature search was conducted across major electronic databases, including PubMed MEDLINE, Embase, Scopus, Web of Science, and the Cochrane Library, covering publications from January 2000 to March 2026. Additional studies were identified through Google Scholar and manual screening of reference lists to ensure inclusion of recent and clinically relevant evidence.
Search terms included procedural keywords such as ultrasound guided injection, mechanical needling, hydrodissection, and sterile water injection, combined with condition specific terms including musculoskeletal pain, myofascial pain, lumbar spinal stenosis, and facet joint syndrome. Mechanistic terms included fibrosis, fascia, mechanotransduction, and mechanosensitive ion channels such as TRPV1 and PIEZO.
Both clinical studies, including randomized controlled trials, cohort studies, and observational investigations, and mechanistic or translational studies were included to provide a comprehensive understanding of biological mechanisms and therapeutic effects. Studies lacking clear clinical or mechanistic relevance, or available only as conference abstracts, were excluded.
Given the heterogeneity in study design, patient populations, and intervention protocols, findings were synthesized narratively, with emphasis on integrating clinical outcomes with mechanistic insights to support a coherent and clinically applicable mechanobiological framework.
Overview of evidence
This review identified a focused body of 30 studies examining ultrasound guided hydrodissection, mechanical needling, and sterile water injection in the management of musculoskeletal pain (Figure 1).

PRISMA flow diagram of the literature search and study selection process.
The majority of clinical evidence relates to ultrasound guided hydrodissection applied in peripheral nerve entrapment syndromes and myofascial pain conditions. Across randomized controlled trials and observational studies, consistent reductions in pain and improvements in functional outcomes have been reported, primarily attributed to mechanical separation of fibrotic tissue planes and restoration of neural mobility.17–29
Hydrodissection using isotonic saline or dextrose solutions reduces mechanical compression on peripheral nerves and improves fascial gliding, thereby facilitating restoration of biomechanical function.17–29 These structural effects are supported by mechanistic and translational evidence demonstrating that disruption of connective tissue adhesions and restoration of tissue mobility contribute to reduced nociceptive input and functional improvement.17–29
At the molecular and experimental level, mechanosensitive responses to mechanical and fluid mediated stimuli provide a biologically plausible basis for therapeutic effects. Experimental and translational studies indicate that tissue deformation and fluid interface modulation contribute to neuromodulation and altered nociceptive signaling.30–36
Evidence specific to sterile water injection demonstrates consistent analgesic effects across multiple randomized controlled trials and clinical pain models, supporting a mechanism involving transient nociceptive activation followed by engagement of endogenous inhibitory pathways, consistent with conditioned pain modulation.30–36
Direct comparative evidence remains limited, particularly in distinguishing the relative contributions of mechanical versus injectate-specific effects. However, randomized controlled trials in intra-articular interventions demonstrate that saline injection, often considered inert, may produce clinically meaningful improvements, supporting a role for mechanical distension and local tissue effects independent of pharmacological action.29,37–40
Taken together, the therapeutic effects of ultrasound guided mechanical needling and hydrodissection appear to arise from a multimodal interaction involving mechanical tissue release, neuromodulation, and restoration of microenvironmental function, including improved tissue mobility and local physiological conditions.17–29,30–36
However, the current evidence base remains heterogeneous, with variability in procedural techniques, injectate selection, and outcome measures.
Overall, the available evidence supports the biological plausibility and emerging clinical relevance of ultrasound guided mechanical needling combined with sterile water hydrodissection as a structurally targeted and mechanism informed intervention for chronic musculoskeletal pain.41–46
Additional evidence from clinical pain models further supports the neuromodulatory mechanism of sterile water injection, demonstrating transient nociceptive activation followed by engagement of endogenous inhibitory pathways consistent with conditioned pain modulation.30–36,47–49
A summary of representative clinical and mechanistic studies is provided in Table 1.
Representative clinical and mechanistic studies of ultrasound-guided hydrodissection and sterile water injection in pain management (n = 30 studies).
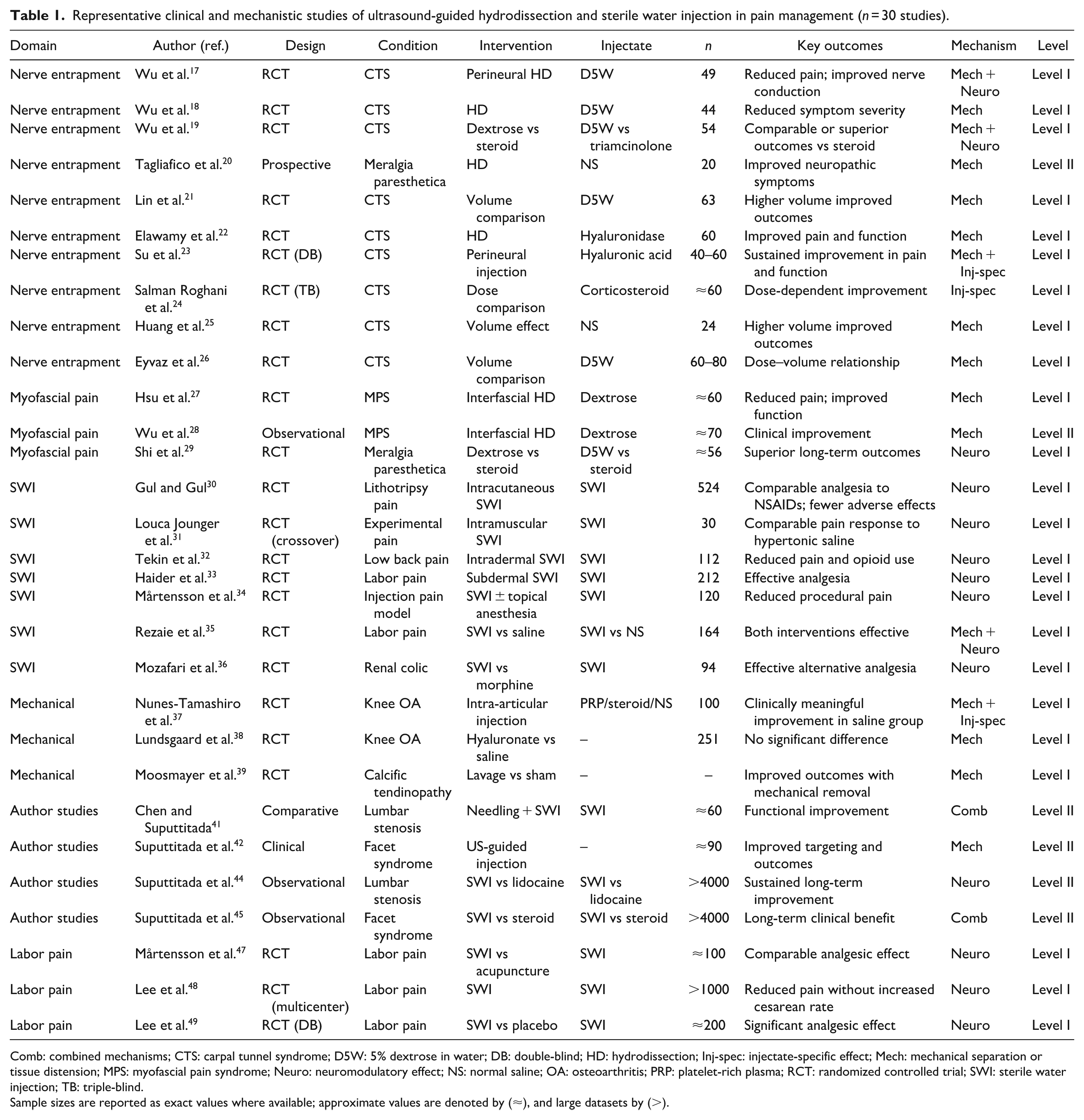
Comb: combined mechanisms; CTS: carpal tunnel syndrome; D5W: 5% dextrose in water; DB: double-blind; HD: hydrodissection; Inj-spec: injectate-specific effect; Mech: mechanical separation or tissue distension; MPS: myofascial pain syndrome; Neuro: neuromodulatory effect; NS: normal saline; OA: osteoarthritis; PRP: platelet-rich plasma; RCT: randomized controlled trial; SWI: sterile water injection; TB: triple-blind.
Sample sizes are reported as exact values where available; approximate values are denoted by (≈), and large datasets by (>).
Discussion
Chronic musculoskeletal pain represents a major global health burden and is increasingly conceptualized as a multiscale disorder involving extracellular matrix (ECM) dysregulation, fibrosis, altered biomechanics, and persistent nociceptive sensitization rather than a purely inflammatory condition.1–3 The ECM functions as a dynamic mechanosensitive network that regulates force transmission and cellular signaling, and its disruption leads to increased tissue stiffness, impaired fascial gliding, and abnormal load distribution.4–6 These structural changes are strongly associated with persistent nociceptive input, particularly in conditions such as chronic low back pain, where reduced fascial shear strain and mechanical restriction have been demonstrated.8,9 These structural abnormalities are directly visualized on clinical imaging (Figures 2 and 3), where calcification and fibrosis at the facet joint contribute to localized mechanical compression and altered load transmission. This imaging–pathology correlation reinforces the role of targeted, ultrasound-guided interventions in addressing both structural and mechanobiological drivers of pain.4,7,37,53
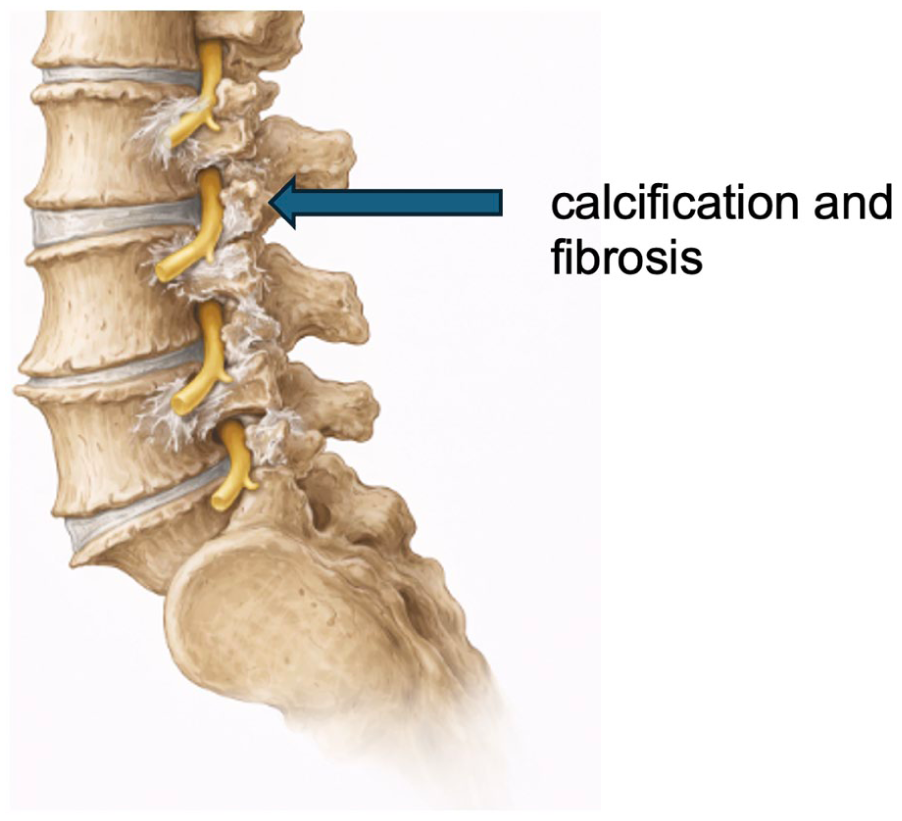
Degenerative structural changes of the lumbar spine. Structural alterations, including disc degeneration, osteophyte formation, and narrowing of the neural foramina, contribute to nerve root irritation and persistent musculoskeletal pain.

Ultrasound-guided needle targeting of the facet joint. Real-time ultrasound imaging demonstrates needle advancement into regions of calcification and fibrosis within the facet joint, enabling precise mechanical needling and hydrodissection.
Mechanotransduction provides the molecular link between structural pathology and pain signaling, whereby mechanical and osmotic stimuli are converted into intracellular biochemical responses.6,10 Mechanosensitive ion channels, including transient receptor potential vanilloid 1 (TRPV1) and PIEZO1/2, play a central role in this process by mediating cation influx, membrane depolarization, and nociceptor activation.11,12 These channels operate within an integrated ECM–cytoskeletal system, in which mechanical forces are transmitted across cellular structures, amplifying nociceptive signaling in fibrotic and mechanically restricted tissues.6,10 In addition, persistent peripheral input may contribute to central sensitization, further sustaining chronic pain states. 52
Hydrodissection targets these mechanisms at the structural level by mechanically separating tissue planes, releasing adhesions, and decompressing entrapped neural structures.16,54 Clinical studies in peripheral nerve entrapment, including carpal tunnel syndrome, demonstrate that hydrodissection can improve symptoms and function, with outcomes influenced by injectate volume and distribution.17–19,21–23 Similar benefits have been reported in myofascial pain and meralgia paresthetica, supporting the role of mechanical decompression and restoration of tissue mobility in reducing nociceptive input.20,27–29 These multilevel effects are systematically summarized in Table 2, which integrates structural, neuromodulatory, and microvascular mechanisms into a unified mechanobiological framework.
Mechanobiological framework of ultrasound-guided mechanical needling with sterile water hydrodissection.

The choice of injectate further modifies these effects through distinct physicochemical and biological mechanisms. Normal saline, as an isotonic solution, acts primarily through mechanical hydrodissection, increasing interstitial volume and reducing tissue compression.13–15 Its limited effect on transmembrane ionic gradients suggests minimal direct activation of mechanosensitive ion channels, and its analgesic effects are therefore largely attributable to biomechanical decompression.13–16 Nevertheless, clinical studies in knee osteoarthritis demonstrate that saline injections can produce meaningful improvements, highlighting the therapeutic importance of mechanical factors such as tissue expansion and pressure modulation.37,38,43
Dextrose-based injectates (D5W) provide additional biochemical and metabolic modulation beyond mechanical effects. Glucose may influence neuronal metabolism, ATP-dependent ion transport, and inflammatory pathways, contributing to stabilization of membrane excitability and reduction of neurogenic inflammation.17–19,21–23 Randomized trials have demonstrated sustained benefits of D5W hydrodissection in carpal tunnel syndrome, with evidence suggesting both mechanical and biochemical contributions.21,25,26 However, the presence of glucose introduces metabolic and osmotic considerations, particularly in multi-site procedures or in individuals with altered glucose homeostasis, such as diabetes mellitus, where local tissue responses may differ. Importantly, D5W does not create strong osmotic gradients and therefore has limited capacity to directly activate ion channels such as TRPV1 or PIEZO.11,12
Sterile water represents a mechanistically distinct injectate characterized by its hypotonicity and its ability to induce osmotic-driven cellular responses. The resulting osmotic gradient leads to rapid water influx, transient cellular swelling, and membrane deformation, directly activating mechanosensitive and osmosensitive ion channels, including TRPV1 and PIEZO1/2.11,12 This activation produces rapid cation influx, particularly calcium, resulting in transient nociceptor excitation followed by desensitization and reduced neuronal excitability. This biphasic response is consistent with conditioned pain modulation, whereby a brief nociceptive stimulus activates endogenous inhibitory pathways and leads to net analgesia.30–36,47–49
Importantly, sterile water exerts integrated effects across multiple tissue compartments within a single intervention. At the neural level, it modulates nociceptive signaling through ion channel activation and reduces peripheral sensitization.11,12 At the muscular level, mechanical needling combined with fluid injection may disrupt myofascial trigger points and reduce localized hypertonicity. At the fascial level, hydrodissection restores tissue gliding and reduces stiffness, improving force transmission across connective tissue planes.4–7,9,55 At the joint level, mechanical decompression and modulation of periarticular tissues may reduce intra-articular pressure and improve joint biomechanics, as supported by studies in osteoarthritis and facet joint syndrome.37,38,53 At the vascular level, decompression of microvascular structures and changes in interstitial pressure may enhance tissue perfusion and oxygenation.16,54
The vascular component is particularly important in chronic pain states. Microvascular compromise and local ischemia are common in fibrotic tissues, where increased ECM density can compress small vessels and impair perfusion.4,7,9 Endothelial cells are highly mechanosensitive and respond to shear stress and mechanical forces through pathways involving cytoskeletal–ECM coupling and ion channel activation.6,10 These processes regulate nitric oxide production, vascular tone, and inflammatory signaling, all of which influence nociceptive sensitivity. Restoration of microvascular dynamics through mechanical decompression and osmotic modulation may therefore contribute to both tissue recovery and pain reduction.6,10,16
Author-derived studies further support this integrated mechanistic model. Mechanical needling combined with sterile water injection has demonstrated sustained clinical improvement in lumbar spinal stenosis and facet joint syndrome, suggesting that targeting both structural and molecular mechanisms leads to more durable outcomes.41–45 These findings are consistent with a framework in which simultaneous modulation of neural, muscular, fascial, joint, and vascular components produces synergistic therapeutic effects.
These differences across injectates are summarized in Table 3, highlighting their distinct mechanistic profiles and clinical implications.
Comparison of injectates used in hydrodissection: mechanisms, neuromodulation, and clinical implications.

D5W: 5% dextrose; NSS: normal saline.
In contrast, conventional pharmacological therapies such as non-steroidal anti-inflammatory drugs and opioids primarily target downstream inflammatory or central pathways without addressing underlying mechanobiological dysfunction.13,14 This limitation underscores the need for mechanism-based, drug-sparing interventions that act at the level of tissue structure and mechanotransduction. Clinical guidelines increasingly support non-pharmacological approaches for chronic low back pain, reflecting this shift toward addressing upstream drivers of pain. 15
Despite these advances, several limitations remain. Heterogeneity in study design, injectate composition, and outcome measures limits direct comparison across studies, and most clinical studies lack direct molecular validation. Future research should integrate molecular biomarkers, ion channel activity, and imaging of ECM and fascial dynamics to directly link mechanotransduction with clinical outcomes. Mechanism-driven randomized trials will be essential to clarify the relative contributions of mechanical, biochemical, and osmotic effects.
This approach supports a shift from technique-based to mechanism-based intervention, where injectate selection and procedural strategy are guided by underlying tissue pathology and mechanotransductive signaling rather than a one-size-fits-all approach.
Collectively, these mechanisms provide a biologically coherent link between extracellular matrix perturbation, ion channel activation, and multilevel modulation of nociceptive signaling.
In summary, normal saline, dextrose, and sterile water represent a continuum of injectate mechanisms. Saline acts predominantly through mechanical decompression, dextrose combines mechanical and biochemical modulation, and sterile water uniquely integrates mechanical hydrodissection with osmotic activation of mechanosensitive ion channels. These integrated effects across neural, muscular, fascial, joint, and vascular systems provide a coherent mechanobiological framework for understanding and optimizing injection based therapies in chronic musculoskeletal pain.11,12,16–19,21–30,35–45,47–51,54,55
Conclusion
Ultrasound-guided mechanical needling combined with sterile water hydrodissection represents a mechanobiologically informed approach to musculoskeletal pain, integrating structural intervention with molecular-level neuromodulation. By disrupting fibrotic adhesions, restoring fascial mobility, and inducing osmotic-driven activation of mechanosensitive ion channels such as TRPV1 and PIEZO1/2, this technique targets both the physical and signaling substrates of nociception.
Current evidence supports a model in which mechanical decompression and osmotic stimulation interact to modulate peripheral nociceptive input, potentially influencing downstream central processing. These effects extend beyond analgesia, encompassing restoration of tissue dynamics, normalization of mechanotransductive signaling, and improvement in functional outcomes.
Compared with isotonic and glucose-based injectates, sterile water uniquely provides a hypotonic microenvironment capable of directly engaging ion channel–mediated pathways while preserving the mechanical benefits of hydrodissection. This dual mechanism positions sterile water as a distinct tool within a spectrum of injectate strategies.
Importantly, this framework supports a transition toward mechanism-based intervention, in which procedural and injectate selection are guided by underlying tissue pathology and mechanotransductive processes rather than empirical approaches. Such a strategy aligns with emerging paradigms in precision and regenerative pain medicine.
While further studies are required to directly validate molecular pathways and define optimal protocols, ultrasound-guided mechanical needling with sterile water hydrodissection provides a coherent and biologically plausible model that bridges tissue-level intervention with ion channel–mediated neuromodulation in chronic musculoskeletal pain.
Footnotes
Author contributions
CPCC and AS contributed equally to the drafting, integration, and development of the manuscript, including literature synthesis, data interpretation, and health-systems analysis. AS conceived the study, developed the conceptual and policy framework, led key sections of the manuscript, and provided senior scientific and clinical leadership, including critical revision for important intellectual content. All authors meet the ICMJE authorship criteria and approved the final version of the manuscript.
Consent for publication
Not applicable.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AS has developed and applied the ultrasound-guided mechanical needling with sterile water injection (SWI) technique described in this manuscript as part of routine clinical practice. AS and CPCC have authored peer-reviewed studies evaluating SWI. The authors declare no other competing interests.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Science and Technology Council of Taiwan (grant numbers NSTC114-2314-B182-021-MY2; NMRPD1Q0921-2).
Institutional review board statement
Not applicable. This study is a structured narrative review based on previously published literature and did not involve human participants, identifiable data, or experimental interventions. Patients and the public were not involved in the design, conduct, or reporting of this research.
Human and animal rights
This article does not contain any studies with human or animal subjects performed by the authors.