
Abstract
Background:
Thoracolumbar compression fractures are common in older adults. Percutaneous kyphoplasty (PKP) is a standard minimally invasive treatment, but 30%–50% of patients still have persistent or inadequate pain relief after the procedure.
Objective:
To investigate the predictive value and mechanism of serum microRNA-145-5p (miR-145-5p) in PKP-related postoperative pain and to support precise pain assessment and intervention.
Method:
Ninety-five patients with thoracolumbar compression fractures treated with PKP were divided into a low pain group (49 cases, VAS 0–3) and a high pain group (46 cases, VAS 4–10) based on 1-month postoperative VAS scores. Fasting venous blood was collected preoperatively and 1 month postoperatively. Serum miR-145-5p and erythroblastic oncogene B4 (ErbB4) levels were measured by qPCR. An LPS-induced inflammatory model was established in RSC96 cells, and their target relationship and effects on inflammation were assessed via cell transfection, enzyme-linked immunosorbent assay (ELISA), and a dual-luciferase reporter gene assay. Logistic regression identified influencing factors, and ROC analysis evaluated the predictive value of miR-145-5p.
Results:
The high pain group had higher preoperative VAS scores, lower bone density T-scores, lower miR-145-5p levels and higher ErbB4 levels. miR-145-5p targets the 3’UTR of ErbB4, inhibiting inflammation by regulating ErbB4. Preoperative VAS score, bone density T-score, and miR-145-5p level were independent predictors of moderate-to-severe postoperative pain. Preoperative miR-145-5p had predictive value.
Conclusion:
Preoperative serum miR-145-5p is a potential biomarker for assessing PKP-related postoperative pain, aiding precise intervention.
Keywords
Introduction
Osteoporotic vertebral compression fractures (OVCFs) represent the most prevalent form of fragility fractures and are a defining clinical manifestation of osteoporosis.1,2 With the global aging population, the incidence of osteoporotic fractures, including vertebral compression fractures (VCFs), has risen substantially. 3 Percutaneous kyphoplasty (PKP), a minimally invasive surgical technique, is commonly employed in the management of thoracolumbar vertebral compression fractures owing to its effectiveness in quickly restoring vertebral body height, providing spinal stabilization, and relieving pain. 4 However, clinical evidence indicates that a significant proportion of patients experience persistent or inadequate pain relief postoperatively, impairing recovery and increasing the burden on patients, families, and healthcare systems.5,6 The incidence of residual back pain ranges from 7.8% to 15.6%, depending on follow-up duration and pain threshold definitions. 7 Currently, postoperative pain assessment after PKP primarily relies on subjective tools such as the visual analog scale (VAS) and numerical rating scale (NRS), which are susceptible to individual variability in perception, emotional state, and cognitive interpretation, thereby limiting their objectivity and reliability.7–9 Therefore, identifying objective, sensitive, and quantifiable preoperative biomarkers is essential for enabling precise prediction, assessment, and targeted intervention of postoperative pain following PKP.
In recent years, the role of miRNAs in pain modulation has gained increasing attention, positioning miRNAs as promising biomarkers and therapeutic targets for pain-related disorders.10,11 For instance, miR-204 alleviates osteoarthritis pain by inhibiting the SP1–LRP1 signaling pathway and disrupting nerve-cartilage interactions, 12 while miR-194 reduces neuropathic pain and suppresses neuroinflammation through targeting FOXA1. 13 Accumulating evidence has linked circulating microRNAs to various painful disorders, such as knee pain and migraine. For instance, serum miR-145-5p and miR-26a-5p are upregulated in migraine patients, suggesting their potential role as pain-related biomarkers. 14 In the context of postoperative pain, studies on total knee arthroplasty have identified preoperative circulating microRNAs (including hsa-miR-146a-5p, miR-145-5p, and miR-130b-3p) as potential predictive biomarkers for postoperative pain outcomes. 15 These findings support the feasibility of using circulating microRNAs to predict postoperative pain in orthopedic procedures, providing a foundation for our study on miR-145-5p in PKP-related pain. Studies have shown that miR-145-5p is dysregulated in bone diseases such as osteoporosis and osteoarthritis and contributes to disease onset and progression.16,17 However, no study has yet to establish a clear association between serum miR-145-5p levels and postoperative pain following PKP for thoracolumbar compression fractures, or elucidated its underlying molecular mechanisms.
ErbB4, an essential component of the epidermal growth factor receptor (EGFR/ErbB) family, is crucially involved in nervous system function.18,19 Dysregulated ErbB4 activation has been strongly associated with heightened inflammatory reactions and the progression of neuropathic pain. 20 In pain-associated conditions, increased ErbB4 expression in the spinal dorsal horn has been linked to thermal hyperalgesia in both inflammatory and neuropathic pain models, 21 whereas its upregulation in the dorsal root ganglion (DRG) plays a role in the development of inflammatory pain. 22 Notably, activation of ErbB4 in parvalbumin-positive (PV) interneurons within the spinal cord reduces glycine levels, thereby modulating mechanical allodynia. 23 Beyond the nervous system, ErbB4 influences bone metabolism by regulating osteoblast proliferation and differentiation as well as osteoclast activity. 23 Dysregulated bone metabolism may compromise vertebral stability, potentially exacerbating postoperative pain and impairing recovery.
Building on these findings, this study integrates clinical research with cellular experiments to examine differences in serum miR-145-5p expression among patients with varying levels of pain following PKP surgery, assess its predictive value for postoperative pain, and elucidate the molecular mechanism by which it regulates postoperative pain through targeted gene modulation and regulation of the inflammatory response. To achieve these objectives, we first conducted a retrospective clinical analysis of 95 PKP patients to identify preoperative biomarkers associated with postoperative pain severity. We then employed an LPS-induced RSC96 Schwann cell inflammatory model to validate the miR-145-5p/ErbB4 regulatory axis and its downstream effects on pro-inflammatory cytokine production. This two-tiered approach ensures that our clinical findings are grounded in mechanistic insights, thereby bridging the gap between bedside observation and bench research.
Patients and methods
Case source and grouping
This study was performed in line with the principles of the Declaration of Helsinki. This study was approved by the Ethics Committee of Nanjing Central Hospital, and all participants provided signed informed consent forms.
This study was a retrospective analysis of patients with thoracolumbar compression fractures who underwent PKP in the orthopedics department of Nanjing Central Hospital between March 2021 and July 2024. All included patients met the predefined inclusion and exclusion criteria. A total of 95 eligible patients were enrolled.
Patients were categorized into two groups based on their VAS scores 1 month postoperatively: the low pain group (VAS 0–3, n = 49) and the high pain group (VAS 4–10, n = 46). The VAS cutoff of 4 was selected to define moderate-to-severe pain, consistent with established pain severity classifications and prior PKP studies. 7 This threshold identifies patients requiring active clinical intervention and has been widely adopted in vertebral augmentation research.
Inclusion and exclusion criteria for participants
Inclusion criteria: (1) Diagnosis of thoracolumbar compression fractures confirmed by imaging modalities including X-ray and CT; (2) Fresh single-segment fractures (duration ≤2 weeks); (3) Patients meeting surgical indications for PKP without contraindications to surgery or anesthesia; (4) Provision of signed informed consent by patients and families, with the ability to participate in pain assessment and follow-up; (5) Preoperative whole-spine X-ray, CT, and MRI confirming single-segment fresh thoracolumbar compression fracture, with no evidence of adjacent (upper or lower) vertebral osteolytic lesions or compression fractures (excluding stable old fractures >6 months).
Exclusion criteria: (1) Chronic fractures (duration >2 weeks) or coexisting spinal conditions such as spinal tumors, tuberculosis, or disc herniation; (2) Patients with preoperative CT or MRI findings indicating facet fractures, articular surface injuries associated with bone marrow edema, or severe degenerative arthritis (defined as Kellgren–Lawrence grade III or IV, characterized by moderate-to-severe joint space narrowing, osteophyte formation, subchondral sclerosis, and/or bone-on-bone changes 24 ); (3) Severe dysfunction of major organs (e.g. heart, liver, kidney), coagulopathy, or active infection; (4) Preexisting chronic pain disorders (e.g. rheumatoid arthritis, postherpetic neuralgia) or long-term analgesic use; (5) History of trauma, surgery, or medication use within the past month that may influence miRNA expression; (6) Presence of psychiatric disorders or cognitive impairment that would preclude full participation in the study.
Clinical data collection
Following patient enrollment, baseline clinical data and key preoperative indicators were systematically collected and recorded using the hospital’s electronic medical record system and standardized research forms. The variables gathered comprised age, sex, body mass index (BMI), preoperative VAS score, and bone mineral density T-score. Preoperative imaging data were reviewed by two senior orthopedic physicians independently to confirm the absence of adjacent vertebral compression fractures or osteolytic lesions. In case of disagreement, a third physician participated in the consultation to reach a consensus.
Serum sample collection and processing
Blood samples were collected between 7:00 and 9:00 AM after overnight fasting to minimize circadian variation. Serum was separated by centrifugation at 3000g for 15 min at 4 °C using an Eppendorf Centrifuge 5427 R. Isolated serum was immediately aliquoted into RNase-free tubes and stored at −80 °C until analysis.
Cell culture and induction
The rat Schwann cell line (RSC96) was obtained from the Shanghai Cell Bank and cultured in high-glucose DMEM (11965092; Thermo Fisher Scientific) supplemented with 10% fetal bovine serum (A5670701; Thermo Fisher Scientific) for nutritional support, along with 100 U/mL penicillin and streptomycin (15070063; Thermo Fisher Scientific) to maintain sterility. Cells were incubated in a humidified atmosphere of 5% CO2 at 37 °C with >95% relative humidity to ensure optimal proliferation and viability.
To establish an in vitro inflammatory model, confluent RSC96 cells were stimulated with lipopolysaccharide (LPS, SMB00704; Sigma) at a final concentration of 1 μg/mL for 24 h to mimic the inflammatory microenvironment associated with pain pathogenesis. This concentration and duration were selected based on established protocols demonstrating optimal induction of inflammatory cytokine expression in RSC96 cells without significant cytotoxicity. 25
Cell transfection
RSC96 cells were seeded into six-well plates and transfected at 60%–70% confluence using Lipofectamine 3000 (L3000015; Thermo Fisher Scientific) according to the manufacturer’s instructions. The experimental groups were as follows: (1) control, (2) LPS, (3) LPS + miR-NC, (4) LPS + miR-145-5p mimic, (5) LPS + miR-mimic + ErbB4-NC, and (6) LPS + miR-mimic + ErbB4–oeRNA. Transfection efficiency was verified at 24 h post-transfection by qPCR detection of miR-145-5p expression.
qPCR
Total RNA was extracted from serum samples and cells using the MolPure® Cell/Tissue miRNA Kit (19331ES50; Yeasen). Reverse transcription was performed with the Hifair® AdvanceFast First Strand cDNA Synthesis SuperMix for qPCR (DNA digester plus, 11155ES60; Yeasen) to generate cDNA. RNA concentration and purity were assessed by a NanoDrop One spectrophotometer (Thermo Fisher Scientific), with A260/A280 ratios of 1.8–2.1 considered acceptable. The primer sequences were designed using Primer-BLAST (National Center for Biotechnology Information, USA) and synthesized by Shanghai Sangon Biotech Co., Ltd. (Supplementary Table 1). For miR-145-5p detection, U6 snRNA was used as the internal reference gene, and amplification was carried out using the Hieff® miRNA Universal qPCR SYBR Master Mix (11170ES25; Yeasen). For ErbB4 mRNA detection, GAPDH was employed as the reference gene, and reactions were performed using the Hieff® qPCR SYBR Green Master Mix (Rox Provided Separately, 11204ES50; Yeasen). The thermal cycling protocol was as follows: initial denaturation was carried out at 95 °C for 30 s, followed by 40 cycles, each consisting of denaturation at 95 °C for 5 s and annealing/extension at 60 °C for 30 s. A melting curve analysis (95 °C for 15 s, 60 °C for 1 min, 95 °C for 15 s) was performed at the end of each run to confirm amplification specificity. The relative expression levels were calculated using the 2−ΔΔCt method.
ELISA
Culture supernatants were collected from RSC96 cells in each experimental group, and the concentrations of pro-inflammatory cytokines, including tumor necrosis factor-α (TNF-α), interleukin-1β (IL-1β), and interleukin-6 (IL-6), were quantified using ELISA. 26 Commercial ELISA kits were used: TNF-α (RAB0476; Sigma–Aldrich), IL-1β (RAB0278; Sigma–Aldrich), and IL-6 (RAB0308; Sigma–Aldrich). All steps were carried out in strict accordance with the manufacturer’s guidelines.
Dual-luciferase reporter gene assay
Potential binding sites between miR-145-5p and ErbB4 were predicted using the TargetScan database. Based on these predictions, wild-type and mutant ErbB4 3′UTR reporter plasmids were constructed. RSC96 cells were transfected with Lipofectamine 3000 (L3000015; Thermo Fisher Scientific) according to the manufacturer’s protocol. After 48 h, luciferase activity was measured using a dual-luciferase assay kit (JKR23008; GENE CREATE) to validate the direct regulatory interaction between miR-145-5p and ErbB4. Renilla luciferase was used as the internal reference. Luciferase activity was measured using a GloMax® Navigator Microplate Luminometer (Promega, USA).
Statistical analysis
Data were analyzed using GraphPad Prism software. Measurement data are presented as mean ± standard deviation (
Results
Comparison of clinical characteristics across patient groups
There were no significant differences in age, gender distribution, or BMI among the groups (p > 0.05). However, with respect to preoperative pain-related indicators, the high pain group exhibited significantly higher preoperative VAS scores and significantly lower bone mineral density T values compared to the low pain group (p < 0.001; Table 1).
Clinical data statistics.

BMD: bone mineral density; BMI: body mass index; VAS: visual analog scale.
Analysis of serum miR-145-5p levels and predictive value
One day before surgery and 1 month after surgery, serum miR-145-5p levels in patients with high pain were significantly lower than those in patients with low pain (p < 0.001; Figure 1(a) and (b)). ROC demonstrated that preoperative serum miR-145-5p levels had predictive value for high pain following PKP, yielding an AUC of 0.794 (95% CI: 0.705–0.884, p < 0.001; Figure 1(c)). Bootstrap internal validation with 1000 iterations confirmed good internal validity, with an optimism-corrected AUC of 0.792 (95% BCa CI: 0.698–0.881) and minimal optimism of 0.002. The Hosmer–Lemeshow goodness-of-fit test further supported adequate model calibration (χ2 = 6.847, p = 0.553).

Serum miR-145-5p levels, predictive value, and correlation analysis: (a) serum miR-145-5p expression was significantly lower in the high pain group than in the low pain group before surgery (***p < 0.001), (b) serum miR-145-5p expression was significantly lower in the high pain group than in the low pain group 1 month after surgery (***p < 0.001), (c) the ROC curve analysis showed that preoperative serum miR-145-5p levels could predict high pain following PKP, with an AUC of 0.794 (p < 0.001), (d) preoperative serum miR-145-5p levels were negatively correlated with preoperative VAS scores (r = −0.520, p < 0.001), (e) a positive correlation was observed between preoperative serum miR-145-5p levels and bone mineral density T values (r = 0.773, p < 0.001), and (f) one month postoperatively, serum miR-145-5p levels remained negatively correlated with preoperative VAS scores (r = −0.638, p < 0.001). Relative expression was calculated by the 2−ΔΔCt method, with calibration to the mean value of the low pain group (set as 1.0). Error bars represent SD from three technical replicates.
Correlation analysis of serum miR-145-5p with VAS score and bone mineral density T value
The relative level of serum miR-145-5p 1 day before surgery was significantly negatively correlated with the preoperative VAS score (r = −0.520, 95% CI: −0.657 to −0.351, p < 0.001; Figure 1(d)). Meanwhile, it was significantly positively correlated with the bone mineral density T value (r = 0.773, 95% CI: 0.677 to −0.843, p < 0.001; Figure 1(e)). One month after surgery, the relative expression level of serum miR-145-5p remained significantly negatively correlated with the preoperative VAS score, with a stronger correlation coefficient than that observed 1 day before surgery (r = −0.638, 95% CI: −0.746 to −0.496, p < 0.001; Figure 1(f)).
Logistic regression analysis of risk factors for moderate to severe postoperative pain
Univariate logistic regression analysis revealed that elevated preoperative VAS scores were associated with an increased risk of high postoperative pain (OR = 7.713, 95% CI: 2.997–19.160, p < 0.001), as were decreased bone mineral density T values (OR = 0.084, 95% CI: 0.030–0.216, p < 0.001) and reduced serum miR-145-5p expression levels (OR = 0.282, 95% CI: 0.117–0.651, p = 0.004; Table 2).
Risk factors for postoperative pain after percutaneous kyphoplasty: univariate and multivariate logistic regression analysis.
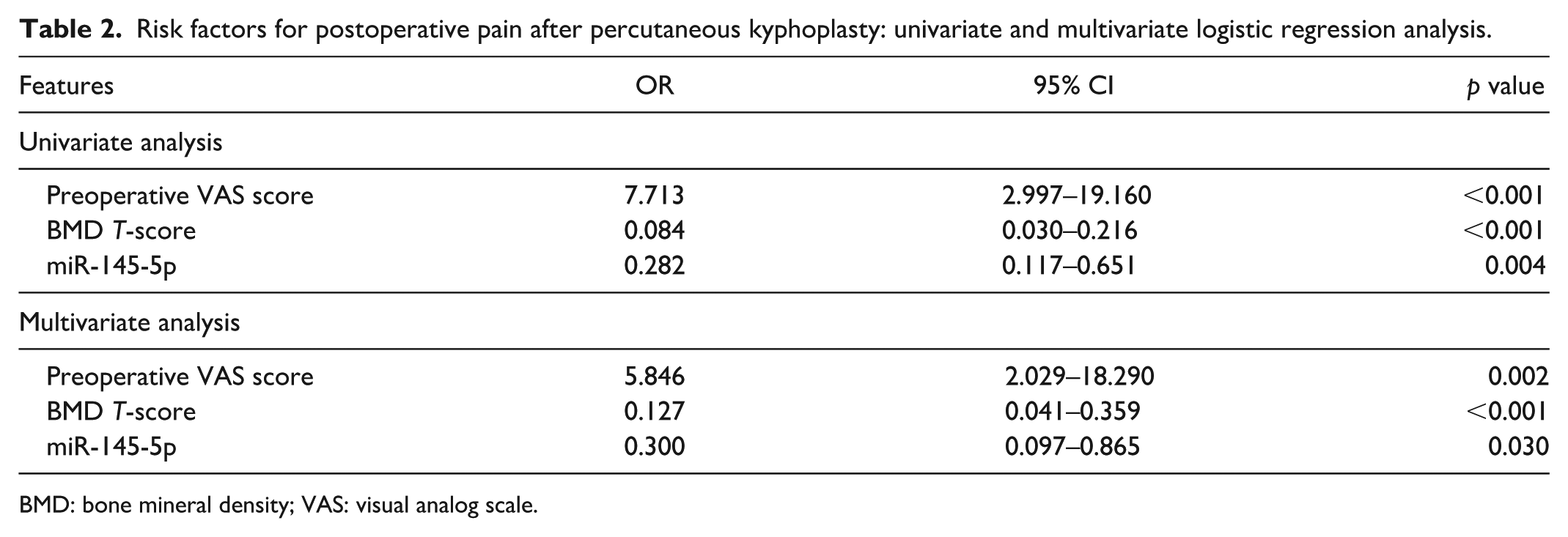
BMD: bone mineral density; VAS: visual analog scale.
Multivariate logistic regression analysis demonstrated that high preoperative VAS scores, low bone mineral density T values, and low serum miR-145-5p expression levels were independent risk factors for high postoperative pain following PKP (p < 0.05; Table 2).
ErbB4 is the target gene of miR-145-5p
The TargetScan database predicts that the binding site for miR-145-5p within the ErbB4 3′UTR is located at nucleotide positions 1021–1028 (Figure 2(a)).
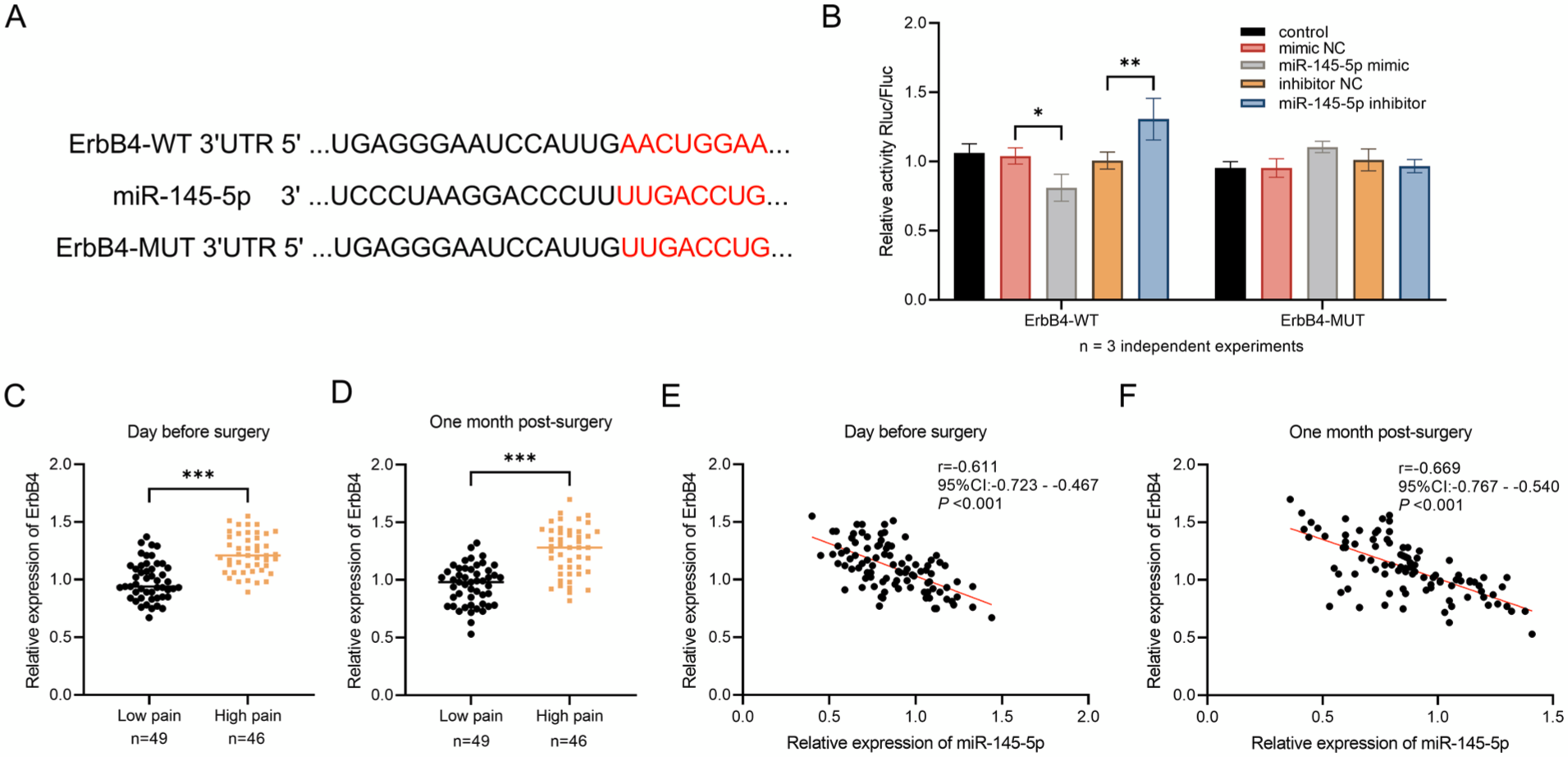
Targeting relationship between miR-145-5p and ErbB4 and clinical expression analysis: (a) TargetScan predicted a conserved binding site between miR-145-5p and the 3′-UTR of ErbB4, (b) dual-luciferase reporter assay confirmed that ErbB4 is a direct target of miR-145-5p (*p < 0.05, **p < 0.01), (c) serum ErbB4 levels were significantly higher in the high pain group than in the low pain group 1 day before surgery (***p < 0.001), (d) serum ErbB4 levels were significantly higher in the high pain group than in the low pain group 1 month after surgery (***p < 0.001), (e) a strong negative correlation was observed between serum miR-145-5p and ErbB4 levels 1 day before surgery (r = −0.611, p < 0.001), and (f) 1 month postoperatively, serum miR-145-5p and ErbB4 levels remained negatively correlated (r = −0.669, p < 0.001). Relative expression was calculated by the 2−ΔΔCt method. For the dual-luciferase assay, Firefly luciferase activity was normalized to Renilla luciferase activity. Error bars represent SD from three independent experiments.
Dual-luciferase reporter gene assay confirmed that overexpression of miR-145-5p significantly increased luciferase activity in cells transfected with the ErbB4-WT reporter plasmid, while silencing miR-145-5p decreased the activity (p < 0.05; Figure 2(b)). However, in cells transfected with the ErbB4–MUT reporter plasmid, there was no significant difference in luciferase activity (p > 0.05; Figure 2(b)). Analysis of clinical samples revealed that serum ErbB4 expression levels were significantly higher in the high pain group than in the low pain group both 1 day before surgery and 1 month after surgery (p < 0.001; Figure 2(c) and (d)). Pearson correlation analysis showed a significant negative correlation between preoperative serum miR-145-5p and ErbB4 expression levels (r = −0.611, 95% CI: −0.723 to −0.467, p < 0.001; Figure 2(e)), as well as between postoperative serum miR-145-5p and ErbB4 levels 1 month after surgery (r = −0.669, 95% CI: −0.767 to −0.540, p < 0.001; Figure 2(f)).
Regulatory effect of miR-145-5p on ErbB4 expression in RSC96 cells
Cellular experiments demonstrated that, compared with the control group, miR-145-5p expression in RSC96 cells treated with LPS was significantly downregulated (p < 0.01; Figure 3(a)), whereas ErbB4 expression was significantly upregulated (p < 0.001; Figure 3(b)). After LPS treatment, overexpression of miR-145-5p significantly increased the expression of miR-145-5p (p < 0.001; Figure 3(a)), while the expression of ErbB4 was significantly decreased (p < 0.05; Figure 3(b)). Co-overexpression of miR-145-5p and ErbB4 did not significantly change the expression of miR-145-5p (p > 0.05; Figure 3(a)), but significantly upregulated the expression of ErbB4 (p < 0.01; Figure 3(b)).
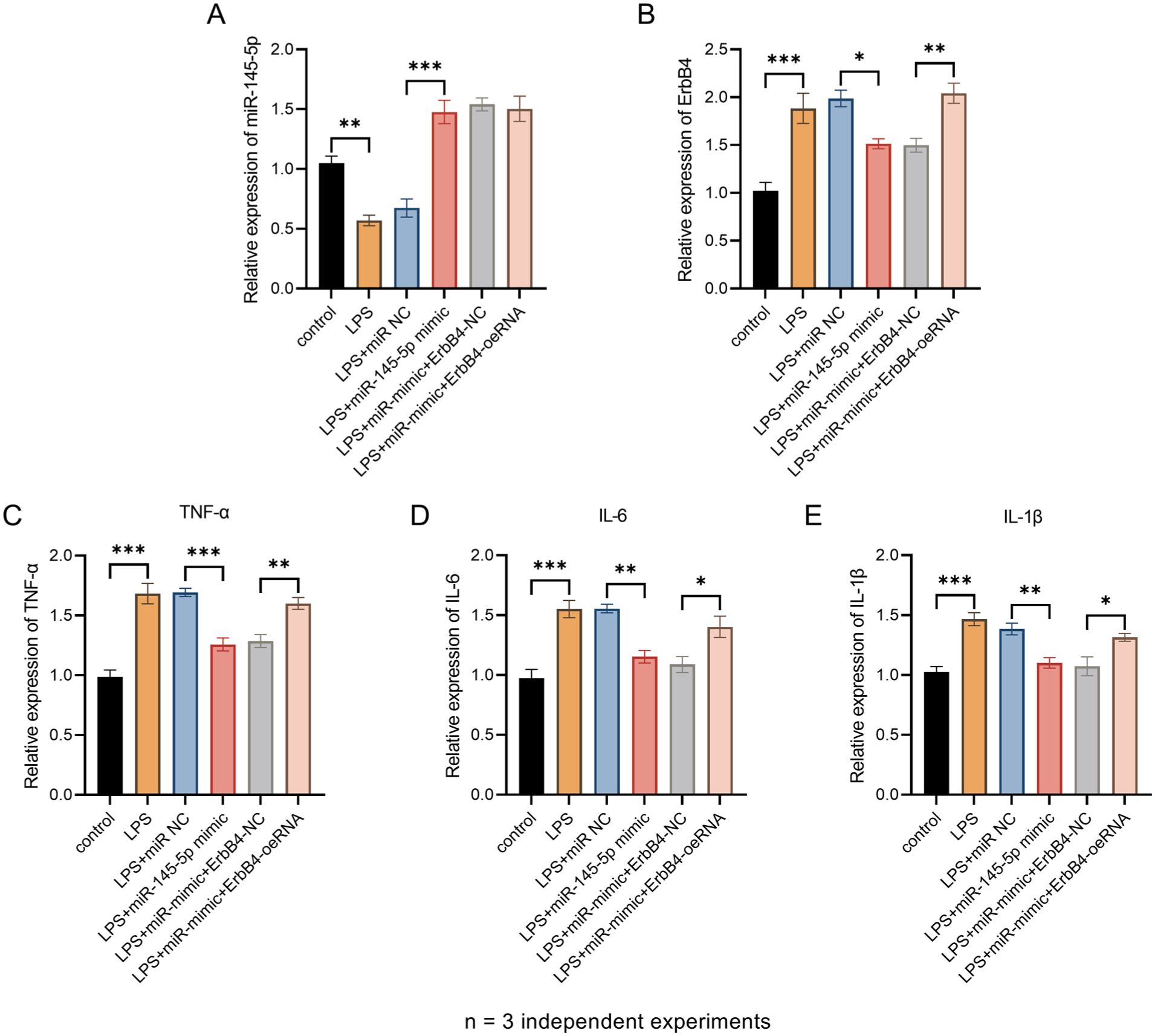
Effects of miR-145-5p on ErbB4 and inflammatory factors: (a) miR-145-5p expression was downregulated by LPS treatment, but significantly upregulated following transfection with miR-145-5p mimics. Co-transfection of miR-inhibitor and ErbB4–oeRNA did not result in a significant difference (**p < 0.01, ***p < 0.001), (b) ErbB4 expression was induced by LPS and markedly reduced by miR-145-5p overexpression. Co-transfection of miR-inhibitor and ErbB4–oeRNA led to a significant increase in expression (*p < 0.05, **p < 0.01, ***p < 0.001), (c) TNF-α expression increased upon LPS stimulation and was significantly suppressed by miR-145-5p mimics. Co-transfection of miR-inhibitor and ErbB4–oeRNA led to a significant increase in expression (**p < 0.01, ***p < 0.001), (d) IL-6 levels were elevated by LPS and decreased following miR-145-5p overexpression. Co-transfection of miR-inhibitor and ErbB4–oeRNA led to a significant increase in expression (*p < 0.05, **p < 0.01, ***p < 0.001), and (e) IL-1β expression was upregulated by LPS and downregulated by miR-145-5p mimics. Co-transfection of miR-inhibitor and ErbB4–oeRNA led to a significant increase in expression (*p < 0.05, **p < 0.01, ***p < 0.001). Relative expression was calculated by the 2−ΔΔCt method. TNF-α, IL-6, and IL-1β concentrations in cell culture supernatants were measured by ELISA and normalized to the control group (set as 1.0). Error bars represent SD from three independent experiments with triplicate wells (n = 3).
miR-145-5p inhibits LPS-induced inflammation in RSC96 cells by targeting ErbB4
The levels of TNF-α, IL-6, and IL-1βwere significantly elevated following LPS stimulation (p < 0.001; Figure 3(c)–(e)). Overexpression of miR-145-5p significantly reduced the expression of these three inflammatory cytokines (p < 0.01; Figure 3(c)–(e)). Notably, when miR-145-5p and ErbB4 were co-overexpressed, the expression of inflammatory factors was significantly reversed and the expression levels increased (p < 0.05; Figure 3(c)–(e)).
Discussion
PKP is the standard surgical treatment for this condition. 28 While it effectively restores vertebral height and improves spinal function, postoperative pain remains the most common complication. 29 It not only markedly reduces patients’ postoperative quality of life but also directly influences their satisfaction with surgical outcomes, posing a major challenge in clinical management.30,31 Multivariate analysis in this study identified a high preoperative VAS score and a low bone mineral density T-score as independent risk factors for high pain following PKP. This finding aligns with previous studies confirming that bone density is a predictor of short-term residual low back pain (SRBP) after PKP. 31 The underlying mechanism may involve osteoporosis-induced microstructural vertebral damage activating local inflammatory cascades, while elevated preoperative pain sensitivity reflects pre-existing neural sensitization. These two factors may interact to promote the chronicity of postoperative pain, increasing the complexity of pain management. Notably, prior research has demonstrated that lumbar and abdominal muscle rehabilitation training positively impacts postoperative recovery in PKP patients. 32 Such training not only improves surgical outcomes but also mitigates osteoporosis by enhancing bone metabolism, thereby optimizing prognosis in elderly patients with OVCF and offering a viable strategy for long-term postoperative pain relief. However, current clinical pain assessment relies heavily on subjective tools such as the VAS. During evaluation, nurses must interpret indirect cues—including facial expressions and limb movements, introducing potential bias due to variations in patients’ cognitive function, language ability, and emotional states (e.g. anxiety or depression). 33 This subjectivity can lead to inaccurate pain assessments, limiting the ability to reflect true pain intensity. Therefore, identifying and validating objective, sensitive biomarkers for pain prediction holds significant clinical value. Such indicators could enable early identification of high-risk patients, support evidence-based development of individualized nursing interventions (e.g. targeted analgesia and tailored rehabilitation programs), and ultimately facilitate precision pain management, further improving patient outcomes.
As a key regulator of pain-related gene expression, miRNAs have been established as critical modulators in pain pathways.34,35 For example, miR-206-3p alleviates neuropathic pain induced by chronic constriction injury through targeting HDAC4, 36 and spinal miR-34a regulates inflammatory pain by downregulating SIRT1 in complete Freund’s adjuvant-induced mouse models. 37 miR-145-5p, a miRNA widely expressed across various cell types, is involved in multiple physiological and pathological processes, including breast cancer, hypertrophic scarring, and diabetes.38–40 As previously noted, miR-145-5p has been shown to play a role in the progression of osteoporosis-related conditions. This study further reveals its significant role in postoperative pain regulation. Serum miR-145-5p levels in patients with high pain were significantly lower than those in the low pain group both 1 day before surgery and 1 month after surgery. Moreover, preoperative serum miR-145-5p levels demonstrated predictive value for high postoperative pain. Correlation analyses showed that serum miR-145-5p expression, measured preoperatively and at 1 month postoperatively, was significantly negatively correlated with preoperative VAS scores and significantly positively correlated with bone mineral density T-scores. Multivariate logistic regression analysis confirmed that low serum miR-145-5p expression is an independent risk factor for high pain following PKP. Combined with the prior finding that reduced bone mineral density and elevated preoperative VAS score are independent risk factors for postoperative pain, the association between miR-145-5p and these two variables provides important mechanistic insights into its regulatory role in postoperative pain. At the molecular level, miR-145-5p may indirectly modulate local vertebral inflammation and neuronal sensitization by targeting key genes within pain-associated signaling pathways. Consistent with our findings, Giordano et al. reported that preoperative serum miR-145-5p is a potential biomarker for chronic postoperative pain after total knee replacement, indicating that the predictive value of miR-145-5p for postoperative pain may be generalized across different orthopedic surgeries. 15 Additionally, miR-145 can alleviate chronic back pain (CBP) associated with intervertebral disc degenerative disease (IVDD). 41 These cross-disease and cross-surgical findings strengthen the credibility of miR-145-5p as a postoperative pain biomarker. Furthermore, as a minimally detectable circulating biomarker, preoperative serum miR-145-5p offers clinical utility as an objective predictor of postoperative pain severity. Measuring miR-145-5p expression before surgery enables nursing staff to identify high-risk patients earlier and supports the development of individualized intervention strategies. For instance, patients with markedly low preoperative miR-145-5p levels may benefit from enhanced perioperative pain management, such as optimized preoperative analgesia and early implementation of multimodal analgesia, combined with lumbar and abdominal muscle rehabilitation training, thereby mitigating the risk of high postoperative pain through integrated molecular and clinical approaches. Beyond its clinical utility as a biomarker, understanding the molecular mechanism by which miR-145-5p regulates pain is essential for developing targeted therapeutic strategies.
In the investigation of pain-related mechanisms, the role of ErbB4 has increasingly attracted attention. Studies using the chronic constriction injury (CCI) mouse model have demonstrated that reduced ErbB4 expression effectively prevents and reverses CCI-induced mechanical allodynia, whereas intrathecal administration of neuregulin-1 (NRG1) to activate spinal ErbB4 induces mechanical allodynia in mice with normal baseline pain sensitivity. 42 Furthermore, research on thermal nociception indicates that ErbB4 serves as a novel marker for thermosensitive spinal neurons in mice, and the NRG1–ErbB4 signaling pathway contributes to pathological pain hypersensitivity, 21 suggesting that ErbB4 plays a critical role in both mechanical and thermal aspects of pain processing. In inflammatory contexts, ErbB4 signaling promotes apoptosis of pro-inflammatory macrophages, thereby attenuating colonic inflammation, highlighting its regulatory function in immune responses. 43 Clinical serum biomarker analyses in patients with postoperative pain have revealed a significant association between pain severity and ErbB4 expression levels, indicating that ErbB4 may serve as a potential molecular indicator for assessing postoperative pain intensity. Further analysis shows a significant negative correlation between serum ErbB4 and miR-145-5p expression, providing key insight into the molecular regulatory mechanism underlying postoperative pain. In vitro experiments have clarified this regulatory axis: miR-145-5p directly targets the 3′UTR of ErbB4 mRNA, leading to translational repression and reduced ErbB4 protein expression. Co-transfection of miR-145-5p mimics and the ErbB4 overexpression vector significantly enhanced the expression levels of inflammatory factors. This mechanism elucidates how miR-145-5p alleviates inflammation and pain through direct inhibition of ErbB4 expression, and identifies a clear therapeutic target for postoperative pain management. Based on this pathway, nursing interventions can be designed around the core strategy of “inhibiting inflammatory responses,” enabling clinicians to mitigate inflammation-mediated postoperative pain via the miR-145-5p/ErbB4 axis through targeted clinical care approaches.
Although this study preliminarily revealed the potential predictive value of miR-145-5p in postoperative pain following PKP and its possible underlying mechanism, certain limitations remain. The single-center retrospective design may introduce selection bias and limit its general applicability. Future multi-center prospective validation is necessary. The sample size may be insufficient to develop a robust predictive model, and external validation in an independent cohort is needed in the future. The follow-up period was limited to 1 month after surgery, and longer-term follow-up is still required to assess the development of chronic pain. While the direct targeting relationship between miR-145-5p and ErbB4 was confirmed via dual-luciferase reporter assays, microRNAs are known to regulate disease processes through multiple target genes. Therefore, future studies should integrate bioinformatics tools such as TargetScan and miRDB to systematically identify additional potential targets of miR-145-5p in the context of post-PKP pain. In addition, the lipopolysaccharide-induced RSC96 cell inflammation model mainly simulates the inflammatory response, while post-PKP pain involves multiple mechanisms, including traumatic tissue injury, the thermal effect of polymethyl methacrylate bone cement, and mechanical nerve compression. Although this model effectively demonstrated the miR-145-5p/ErbB4/inflammatory cytokine regulatory axis, future studies should validate these findings in animal models of vertebral compression fractures and bone cement implantation to better simulate the complex pathophysiology of PKP-related pain.
In conclusion, this study confirmed that preoperative serum miR-145-5p is an independent predictor of moderate to severe pain after PKP, which enables the identification of high-risk patients who may require enhanced perioperative analgesic strategies before surgery. The miR-145-5p/ErbB4 regulatory axis represents a novel molecular mechanism underlying postoperative pain associated with PKP, where miR-145-5p directly targets ErbB4, inhibiting the production of inflammatory cytokines in Schwann cells stimulated by lipopolysaccharide. These findings collectively advance the development of precise pain management for patients with thoracolumbar compression fractures, providing practical biomarkers for clinical decision-making and offering a mechanistic basis for future therapeutic targeting of the miR-145-5p/ErbB4 pathway to alleviate inflammation-mediated postoperative pain.
Supplemental Material
sj-docx-1-mpx-10.1177_17448069261456426 – Supplemental material for Serum miR-145-5p as a predictive biomarker for postoperative pain after percutaneous kyphoplasty
Supplemental material, sj-docx-1-mpx-10.1177_17448069261456426 for Serum miR-145-5p as a predictive biomarker for postoperative pain after percutaneous kyphoplasty by Min Fang, Juan Wang, Yongliang Zhu and Hui Zhao in Molecular Pain
Footnotes
Acknowledgements
The authors have no acknowledgments.
Author contributions
MF and JW made substantial contributions to conception and design, performed all the experiment, and was a major contributor in writing the manuscript. YZ contributed to acquisition of patients and tissues specimens, analysis and interpretation of data. HZ has been involved in drafting the manuscript and revising it critically for important intellectual content. All authors read and approved the final manuscript.
Consent to participate
All participants provided signed informed consent forms.
Consent for publication
Not applicable.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
This study was performed in line with the principles of the Declaration of Helsinki. This study was approved by the Ethics Committee of Nanjing Central Hospital.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.