
Abstract
Using health diaries is associated with improved outcomes in patients with heart failure. However, heart failure patients’ attitudes towards using a diary have not been investigated so far. The aim of this study was to investigate heart failure patients’ attitudes towards and the factors influencing diary use. Patients who took part in an educational session to foster self-care behaviours, during which they were given a diary, were asked to participate in this explorative, cross-sectional survey study. The survey took place at least six months after the educational session. Over half of the 53 participants (52.8%) were still using the diary. Reasons for not using it were no perceived need to use it, stable vital signs, and being able to recognise symptoms of exacerbation without the diary. Users and non-users did not differ in their general attitudes towards diary use except regarding the statements ‘Keeping a diary makes no sense’ and ‘Keeping a diary helps to control the disease and the occurrence of symptoms’. Therefore, diary users may be prone to better self-care activities. Age and living situation are influencing diary use. To improve diary adherence, health care providers should stress the advantage of using a diary and the importance of diary adherence.
Introduction
To support self-care, patients with chronic conditions are often recommended to record their disease symptoms in a diary. Diaries have been used since the early decades of the 20th century and are attributed to fostering patients’ involvement in their care, and to facilitating health education and changes in patients’ behaviour (Burman, 1995). Numerous studies have investigated the benefits and effects of using a diary in patients with various conditions. Keeping a diary is associated with improved symptom recognition (Greenhalgh, 2005; Schumacher et al., 2002), symptom evaluation (Schumacher et al., 2002), memory of symptom frequency and intensity (Ferrari and Russell, 2010), medication adherence (Van Berge Henegouwen et al., 1999) and sensitising the patient to notice the disease’s exacerbation (Llor et al., 2012). In addition to assessing outcomes, Greenhalgh’s study examined experiences with and attitudes towards using a diary (Greenhalgh, 2005). In that study, patients with multiple sclerosis stated that keeping a diary helped them to develop coping strategies, to better recognise their symptoms, and to discover new symptoms they had not previously experienced. In addition, patients had the impression that the attending neurologist would benefit from the data collected in the diary. However, concerns about diary use were also expressed. One-third of the participants stated that the diary made them think more about their symptoms than they liked, and that it reminded them daily of their disease and its consequences in daily life.
In contrast to the reported benefits of diary use, in one study with children with asthma no effect of diary use on disease self-management was identified (Arga et al., 2014). Other studies using a sample of adults with chronic diseases revealed that overall compliance with diary use is low and decreases over time (Litcher-Kelly et al., 2007; Stone et al., 2002). Reasons for not using the diary are feeling too ill to keep the diary, forgetting to keep it, feeling better, and that it is inappropriate for managing the disease (Baggott et al., 2012; Greenhalgh, 2005).
Heart failure patients have been encouraged to use a diary to record weight and symptoms of exacerbation such as dyspnoea, fatigue, oedema and vital signs like blood pressure and pulse rate in numerous studies (Jaarsma et al., 2008; Köberich et al., 2015; Pearl et al., 2003). There is evidence that keeping a diary improves disease-related self-care and outcomes. Patients with heart failure who keep a diary demonstrate a high adherence rate of daily weight monitoring, are living longer, have more contacts with health care providers, report a better quality of life and stay out of hospital longer than those patients not keeping a diary (Eastwood et al., 2007; Jones et al., 2014; White et al., 2010; Wright et al., 2003). However, results of some studies suggest an overall low rate of diary users. For example, Eastwood et al. (2007) reported in their study a non-user rate of 44%. Wright et al. (2003) found a decrease in diary use over the 12-month study period, with an 18% decrease in the first six months. The reported reasons for not using a diary are numerous. However, they have been inadequately researched in patients with heart failure. Only White et al. (2010) investigated the reasons for not using a symptom diary in heart failure patients: being on vacation, partaking in holiday meals and forgetting to weigh themselves were the reasons most often stated.
As no study investigating the use of a diary in heart failure patients to date has evaluated their attitude towards diary use, this study aimed to examine the use of and attitude towards a diary of patients with heart failure three months after completing an educational programme about heart failure self-care. The following questions were the basis for this study:
Do patients use the diary three months after completing a heart failure-specific educational programme? What are their reasons for not using a diary? What is their attitude towards using a diary?
Method
Design
To evaluate patients’ attitudes towards and the use of a heart failure diary, an exploratory, cross-sectional survey was conducted between July 2012 and November 2014 at the Clinic of Cardiology of a university-affiliated hospital in southern Germany.
Study population
All patients who received a nurse-administered, hospital-based education intervention from 2011 to 2014 and finished a three-month follow-up with four consecutive telephone calls were eligible to participate in this study.
Education intervention
The procedure and content of the educational session has been described elsewhere in detail (Köberich et al., 2015). Briefly, patients identified as having heart failure received a standardised one-hour in-hospital education session aimed at fostering self-care behaviours. The educational session comprised the following topics: the physiology of the circulation and respiratory systems, pathophysiology of heart failure with particular focus on fluid retention, medication, a heart failure-specific diet and fluid restriction, signs and symptoms of worsening heart failure, when to seek help, lifestyle changes, symptom monitoring, travelling and recreational activities. To support their self-care behaviour, patients were given a diary during the educational session, and its use was explained. After discharge, patients received four telephone calls within 12 weeks to learn whether the patients were demonstrating the ability to transfer the content of the educational session to their everyday life, and they were given further instruction if necessary. This specific educational programme can improve self-care behaviours (Köberich et al., 2015).
Procedure
Patients were contacted by mail and asked to participate in this study. A cover letter with the description of the study aims, a questionnaire to collect demographic and disease-related data, and a questionnaire to assess the attitude towards and use of a heart failure diary (Heart Failure Diary Questionnaire) plus a prepaid envelope were mailed by the investigator. Voluntary consent was assumed if the questionnaires were returned to the investigator.
The study protocol was approved by the Ethics Committee of Albert-Ludwigs-University Freiburg, Freiburg, Germany (Ethics Committee No. 269/12), and the study complies with the principles outlined in the Declaration of Helsinki (Rickham, 1964).
Measurement
The Heart Failure Diary Questionnaire (HFDQ) was developed for the purpose of this study. Items in the HFDQ were derived from six interviews with patients who attended a nurse-administered, hospital-based heart failure educational intervention and from the literature (Greenhalgh, 2005; Schmincke, 2009; White et al., 2010; Wright et al., 2003).
After formulating the questions and answers, an initial draft of the questionnaire was reviewed by six clinical nurse specialists from different medical disciplines regarding the comprehensibility of the questions and answers and the logic of its structure. After reformulating some questions and restructuring the questionnaire, a second draft was pretested with six patients. Patients were asked to indicate whether they had any trouble understanding the questions or answers, or if the content could be improved. Suggestions for improving the comprehensibility and content were reviewed by the author and subsequently integrated in the questionnaire.
The HFDQ is in German and consists of nine sections assessing the use of and attitude towards a heart failure diary. Section 1 evaluates how often patients monitor themselves for symptoms of worsening heart failure. Sections 2 and 3 ask the patients whether and how often they use the diary to record the measures. Section 4 evaluates reasons for not documenting measures. Section 5 asks the patients about their perceived benefits of using the diary and how they handle it. This section consists of 10 items rated on a five-point Likert-scale (1 = I totally agree; 5 = I totally disagree). Sections 6 and 7 examine whether the patient's general practitioner or cardiologist is aware of the diary and, if so, of how they use the diary. Section 8 evaluates patients’ attitudes towards using the diary. It contains seven statements using a five-point Likert-scale (1 = I totally agree; 5 = I totally disagree). Section 9 asks about reasons for not using the diary.
In addition, patients were asked to give information about their age, gender, marital status, educational level, self-rated New York Heart Association (NYHA) status, self-rated health (five-point Likert-scale: 1 = excellent; 5 = bad), living situation, and how they perceived the quality and benefit of the education session about heart failure self-care (quality rating: 1 = very good; 6 = insufficient; benefit rating: 1 = very helpful; 4 = not helpful).
For the purpose of this study, this report is limited to the results of sections 1, 4, 5, 8 and 9 of the questionnaire.
Data analysis
The data were coded and entered into IBM SPSS Statistics, Version 19. Descriptive statistics were used to describe patients’ characteristics and their attitudes towards and use of a diary. Nominally-scaled variables are displayed as numbers and percentages, interval-scaled variables as mean values and standard deviations if normally distributed, and otherwise these are displayed as a median and interquartile range. To calculate differences between groups, the t-test or Mann–Whitney U test was used where appropriate.
To evaluate factors influencing diary use, we calculated the bivariate correlation between diary use and socioeconomic and disease-related variables. If variables correlated on a statistical level of p ≤ 0.2 they were entered into a binary multivariate regression analysis.
Overall, a p-value of ≤0.05 was deemed statistically significant.
Results
Participants
Patients’ characteristics.
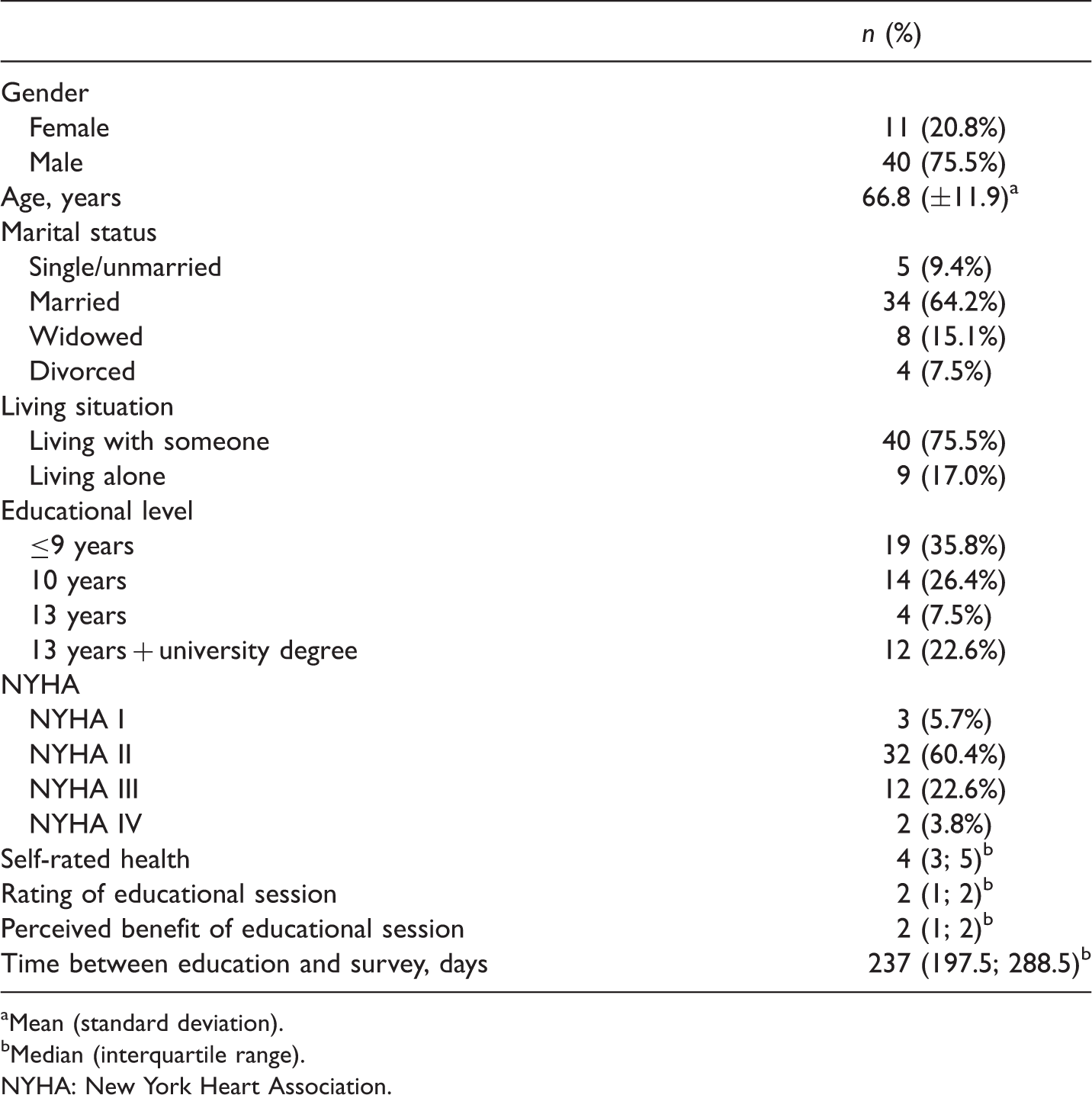
Mean (standard deviation).
Median (interquartile range).
NYHA: New York Heart Association.
Diary use
Of the 53 patients who returned the questionnaire, 28 (52.8%) stated that they are still using their heart failure diary, 22 (41.5%) did not use the diary any more and three (5.7%) did not answer this specific question. Most used their diary to record body weight (n = 21; 75.0%), blood pressure (n = 21; 75.0%), oedema (n = 16; 57.1%) and other heart failure-related symptoms (n = 18; 64.3%) on a daily basis.
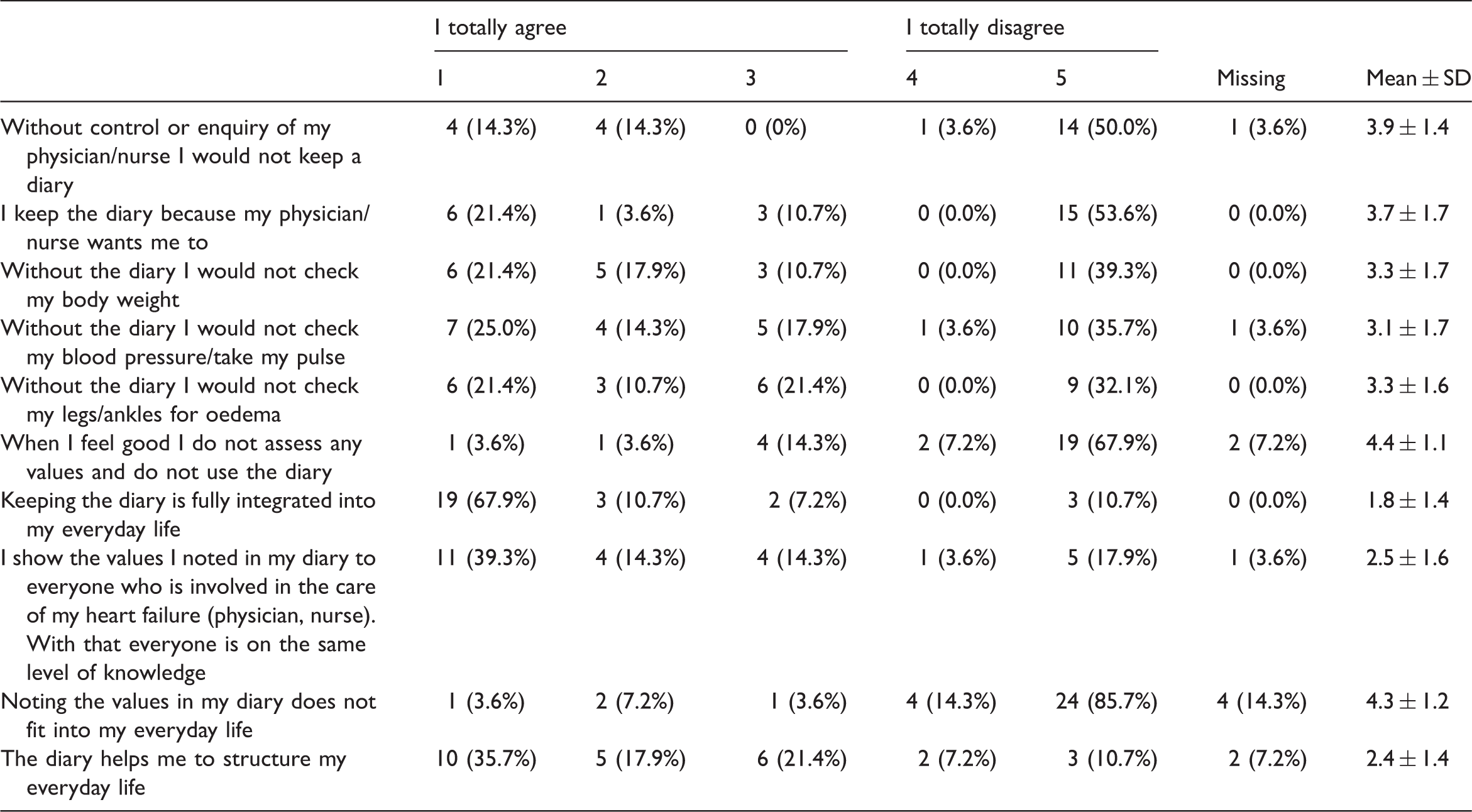
Diary users’ perceived benefits of using a diary and handling of the diary
Diary users’ perceived benefits of using a diary and handling of the diary.
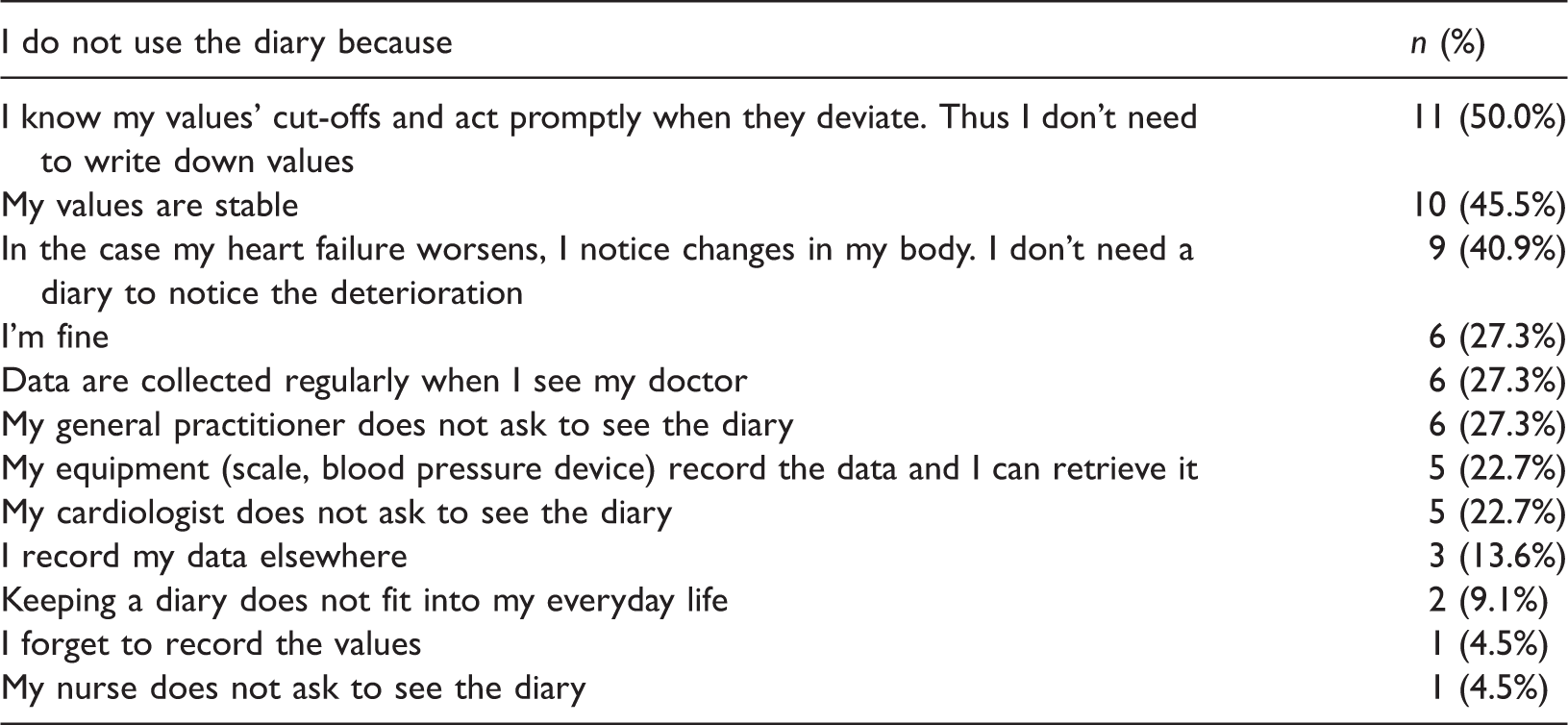
Reasons for non-use
Reasons for not using a heart failure diary.
Attitudes towards diary use of users and non-users
Attitudes towards diary use.

Mean of five-point Likert-scale (1 = fully agree; 5 = fully disagree).
Factors influencing diary use
Factors influencing diary use.

Discussion
This is the first study evaluating heart failure patients’ attitudes towards keeping a diary to routinely record their weight, blood pressure, pulse rate and oedema. Results indicate that older patients and patients living with someone are more in favour of keeping a diary than young patients and those living alone. In addition, those keeping a diary believe that doing so makes sense and helps to control the disease and emerging symptoms.
Half of the diary non-users stated that they do not use the diary because they know their threshold of critical values and if any measured variable exceeds these thresholds they will react to it. This means that they would only take action to prevent acute exacerbation when their weight has exceeded a critical point, for example. However, self-care monitoring aims to identify early signs and symptoms of exacerbation as soon as possible to prevent exacerbation. Sethares and colleagues (2015) analysed in their review numerous studies investigating factors influencing care-seeking, describing peripheral oedema, weight gain and dyspnoea as factors for a greater delay in seeking care. It is hypothesised that heart failure patients do not respond to heart failure symptoms in a timely manner due to deficient knowledge about these symptoms and how to react to them (Sethares et al., 2015). Riegel and colleagues describe this as ‘unreflective, insufficient self-care’, that is, correct self-care behaviours without knowing enough about what makes them beneficial and what to do with the results (Riegel et al., 2012). In contrast, the finding from a large retrospective study indicates that those patients with greater heart failure knowledge delayed care seeking (Nieuwenhuis et al., 2011). In that case they assumed that those patients with more knowledge initiated adequate self-care management measures (e.g. taking an extra dose of diuretics) in the case of symptoms related to fluid overload and therefore did not seek professional treatment.
As no study has ever evaluated the association between diary use, weight monitoring and delay in seeking professional treatment in heart failure patients, further large-scale studies are needed to establish evidence regarding this association.
Interestingly, 45.5% of those not using the diary stated that they do not use it because they have no signs or symptoms of heart failure. Using a diary should enable one to recognise deterioration in the disease at an early stage whether the patient has ever experienced symptoms/signs of worsening heart failure or not. Those who do not use the diary might be lulled into a false sense of security. It is possible that those patients will fail to recognise signs/symptoms of worsening heart failure (triggering rehospitalisation), especially if they have never or only once experienced disease exacerbation. It is possible that the self-care education programme did not sufficiently stress the importance of the early detection of signs/symptoms of heart failure exacerbation and how these signs/symptoms can be detected at the time with the help of a diary. In fact, Jones and colleagues found that using a diary to monitor body weight with a diary-recorded adherence rate of more than 80% is associated with fewer heart failure-related hospitalisations (Jones et al., 2014). In this study, those patients using the diary seemed to be more committed to recognising symptoms of heart failure exacerbation at an early stage than the non-diary users. The users’ attitude towards diary use is affected by believing that it helps one control the disease better and cope with signs of exacerbation. It seems that diary users are more confident regarding their self-care activities. According to Riegel et al. (2012), confidence moderates the relationship between self-care and outcomes. Therefore, it would be interesting to learn whether this positive attitude towards using a diary is associated with lower exacerbation and rehospitalisation rates. The results of a secondary data analysis study performed by Lee and colleagues indicate that early symptom recognition is able to decrease myocardial stress and systemic inflammation and therefore to delay disease progression (Lee et al., 2011).
In a study conducted by White et al. (2010) patients did not sufficiently make contact with their health care providers despite experiencing and recording weight gain. The authors concluded that health care providers should encourage the patients to use the diary data to seek help. This implies that health care providers are interested in the data patients record. Interestingly, more than 20% of the participants who used the diary stated that their general practitioner or cardiologist did not ask for the diary even though the health care providers had been informed by the clinical nurse specialist who conducted the educational session that the patient had received heart failure education and been given a diary to record weight, blood pressure, pulse rate and oedema. Perhaps health care providers also need more information about the benefit of health diaries.
Socio-economic factors influencing diary use are age and living situation. In this present study, those with higher age and those living with someone used the diary more often than those who were younger or living alone. The results of this study are in line with the results of Jones et al. (2014), who observed a statistically significant difference in age between those groups with a diary adherence rate of more than 80% and those with an adherence rate of under 80%. Although evidence of determinants of self-care in heart failure patients is mostly inconsistent (Oosterom-Calo et al., 2012), there are additional studies suggesting a positive relationship between age or living situation and self-care (Cameron et al., 2010; Holzapfel et al., 2009; Ni et al., 1999; Riegel et al., 2009; Sayers et al., 2008). The living situation reflected the amount of social support: living with someone led to greater social support. The importance of social support and the involvement of family members or caregivers in the self-care activities of heart failure patients has been acknowledged for several years and is part of ongoing research and discussion (Buck et al., 2015; Retrum et al., 2013). The association between living with someone and diary adherence might only reflect the social support the patient is experiencing. Therefore, to foster self-care activities, it seems important to engage family members and caregivers.
Conclusion
Even though the use of a symptom diary is recommended by health care providers, in this study only half of the patients kept a diary after terminating telephone follow-up as part of a nurse-led education programme to foster chronic heart failure self-care. Keeping a symptom diary is associated with higher age and with living with someone. In addition, the results of this study suggest that patients keeping a diary feel more confident to be able to control their disease with the help of the diary than patients not keeping one. This may lead to better self-care behaviours. Therefore, during educational sessions health care providers should emphasise the benefit of keeping a diary.
Limitations
This study has several limitations to consider. Due to its explorative nature and small sample, no statistically significant differences in the use of and attitudes towards diary use with appropriate statistical power could be detected. Therefore, the study results should be regarded as preliminary and as a first step towards formulating hypotheses about patients’ attitudes towards keeping a heart failure symptom diary. In addition, the sample of heart failure patients participating in this study is not representative of all patients with heart failure. This patient cohort was a convenient sample of patients educated in heart failure self-care behaviours. These patients might be more interested in maintaining a physiologically and emotionally stable condition and therefore more prone to aids like a diary than those not being educated. Furthermore, those who took part in this study might represent a cohort of diary users, which may result in overestimating the rate of diary users in this patient cohort.
As this is a cross-sectional study, the result of the regression analysis regarding influencing factors on diary use must be interpreted with caution, because cross-sectional studies can only provide a snapshot of an actual situation and results of a regression analysis may be misleading.
Furthermore, the questionnaire used was only tested for face validity. No further psychometric properties were assessed. As the items of the questionnaire were not used as single items of a scale, assessing construct validity in terms of applying exploratory and/or confirmatory factor analysis was not indicated. Test–retest reliability was not assessed as this was not the focus of the study. However, stability of item responses has to be questioned and should be the focus of further studies.
The focus of this study was to explore patients’ attitudes towards keeping a health care diary. Because of its exploratory nature a qualitative approach to answer the research question would be more appropriate. However, this quantitative approach was chosen due to its being easy to conduct and to get a first impression of heart failure patients’ attitudes towards keeping a symptom diary. Studies using a mixed-methods approach might give a deeper understanding of patients’ attitudes.
Key points for policy, practice and/or research
Using a symptom diary is influenced by age and living situation. Diary users seem to feel more confident of being able to control their disease with the help of a diary than patients not keeping one. Using a diary may foster disease self-care activities. Health care providers should emphasise the benefit of keeping a diary. Further research about reasons for not keeping a diary in chronic heart failure patients is needed.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.