
Abstract
Pain and symptom management is the most important area of paediatric palliative care, but clinicians often receive little training in this area. Our research evaluated the effectiveness of pain and symptom management training among paediatric professionals. A quasi-experimental pretest–posttest study was used. Fifty-three paediatric nurses and 18 paediatricians participated in this study for a response rate of 80%. Results showed significant main effects of training on confidence levels (p < 0.001), and attitude scores (p < 0.001) among paediatric clinicians in a variety of areas, with no differences in scores between paediatricians and nurses. This suggests that education can effectively increase paediatric clinicians’ confidence in and attitudes towards providing pain and symptom management for children with severe illness. Further training is needed to promote interdisciplinary healthcare team work to improve the effectiveness of pain and symptom management.
Background
Paediatric palliative care is an approach which focuses on improving the quality of life for severely ill children and their families, through the prevention and relief of suffering through early identification and assessment, and the treatment of pain and other distressing symptoms, physical, psychosocial and spiritual (American Academy of Pediatrics, 2013; World Health Organization, 2010). The management of pain and symptoms is essential in paediatric palliative care and is closely related to the quality of life of patients and their families (World Health Organization, 2010). Although providing appropriate pain and symptom management for dying children is a key responsibility of healthcare providers, misconceptions and the insufficient management of paediatric pain and symptoms has been repeatedly documented (Czarnecki et al., 2014; Drake et al., 2003; McCallum et al., 2000; Peng et al., 2012). In order to assess and relieve pain and treat symptoms effectively, paediatric professionals require specific knowledge and the appropriate skills, attitudes, and confidence in providing such care (Drake et al., 2003; Peng et al., 2012; Williams-Reade et al., 2015).
One common obstacle to adequate paediatric pain and symptom management is a lack of professional knowledge and skills among clinicians (Galloway and Yaster, 2000; Jacobs et al., 2009). The evidence is clear that paediatric clinicians’ inadequate education may result in insufficient confidence to provide pain and symptom management, and an unwillingness to provide the interventions of pain and symptom management for children (Ekim et al., 2013). Research in Taiwan, where little paediatric palliative care training is available, is consistent with this finding (Peng et al., 2013), confirming that neonatal clinicians seem to lack confidence in pain and symptom management (Lee et al., 2016).
Previous researchers have recommended that paediatric clinicians learn to assess and manage these distressing symptoms in a more appropriate manner (Meyer et al., 2006). A recent study found that pain and symptoms management was the area of paediatric palliative care that was most deficient among paediatric clinicians in Taiwan (Lee et al., 2016). Another study found that many paediatric nurses lacked adequate knowledge regarding pain management for children, identifying an urgent need for further education in this area (Babgi et al., 2008; Downing et al., 2015). Nevertheless, in Taiwan only rudimentary training in pain and symptom management for paediatric palliative care is provided to paediatric clinicians (Peng et al., 2013). This study evaluates the effectiveness of paediatric palliative care pain and symptom management training for paediatricians and nurses in Taiwan.
Purpose
This study evaluated the impact of training on paediatric professionals’ confidence, and on attitudes related to the provision of pain and symptom management for children with life-limiting or life-threatening conditions.
Research methods
A quasi-experimental pretest–posttest design was used to assess the research purposes of this study.
Research intervention
Training curriculum (5 hours).
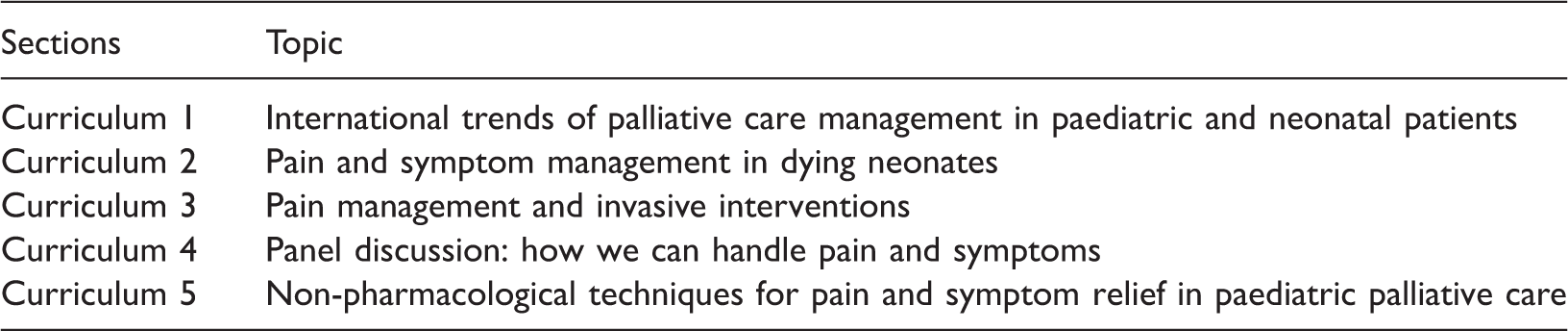
In this research, paediatricians and nurses were invited to participate in the training together because they are significant in the multidisciplinary pain management teamwork for providing a quality of care (Odell and Logan, 2013).
Because the native language of the lecturers was English, translation was provided for the lecturers and participants, and all materials were translated from English into Chinese. The curriculum included pharmacological treatments and non-pharmacological techniques for pain and symptom relief in paediatric palliative care. Various educational strategies were used, including didactic lectures, case study discussions, role-play and video viewings. Table 1 presents details of the curriculum.
Research participants and setting
This study took place at the Department of Pediatrics of the Taichung Veterans General Hospital in Taichung City in Taiwan. Participants were recruited via convenience sampling; paediatricians and paediatric nurses who were currently working in paediatric wards and who completed the entire training programme were invited to participate in this study. Institutional review board approval was obtained from the participating hospital and a consent form was obtained from each participant before data were collected.
Research instrument
A research questionnaire was administered before and after the training to survey participants’ confidence levels and attitudes regarding the provision of pain management to dying children.
The questionnaire consisted of seven questions related to demographic information, three questions in a six-item Likert format regarding confidence in the provision of pain and symptom management, and eight questions in a five-item Likert format pertaining to attitudes towards the provision of pain and symptom management to ill children. Confidence levels were coded as follows: 1 = never; 2 = rarely; 3 = sometimes; 4 = often; 5 = always; 6 = unsure. Attitude levels were coded as: 1 = strongly disagree; 2 = somewhat disagree; 3 = unsure; 4 = somewhat agree; and 5 = strongly agree.
This questionnaire was adapted from previous studies and other literature, the three questions evaluating clinicians’ confidence were mainly derived from the questionnaire, Comfort Level Caring for Dying Infants (CLCDI), by Babgi et al. (2008) and the eight questions concerning attitudes were derived from the Neonatal Palliative Care Attitude Scale (Kain et al., 2009) and another previous study (Burns et al., 2001). The content validity index (CVI) was developed by seven experts, four clinical experts and three paediatric scholars in the field of end-of-life care for children. The attitude towards caring for dying children (CVI = 0.84) and the confidence in caring for dying children (CVI = 0.89) sub-constructs revealed high content validity. An overall content validity index (CVI = 0.85) was used to determine the validity of the structured questionnaire. Some of the questions were originally prepared in English and subsequently translated into traditional Chinese for the benefit of the research subjects, who were Taiwanese. The translation accuracy was checked by a forward–backward translation procedure. Reliability testing was conducted by applying the questionnaire to five nurses and five physicians using test–retest Cronbach’s α (0.8) to determine the reliability of the results.
Statistical analysis
Data management and statistical analysis were performed using SPSS version 16.0 (SPSS Inc., Chicago, IL, USA). The demographic data were described by number and frequency. To consider the inherent subject dependency due to repeated measurements, the generalised estimating equation (GEE) method’s multiple linear regression model was used to determine the effect of the training programme on pretest and posttest of attitudes and levels of confidence after adjusting for the effects of confounding variables. Statistical significance was defined as p < 0.05.
Research results
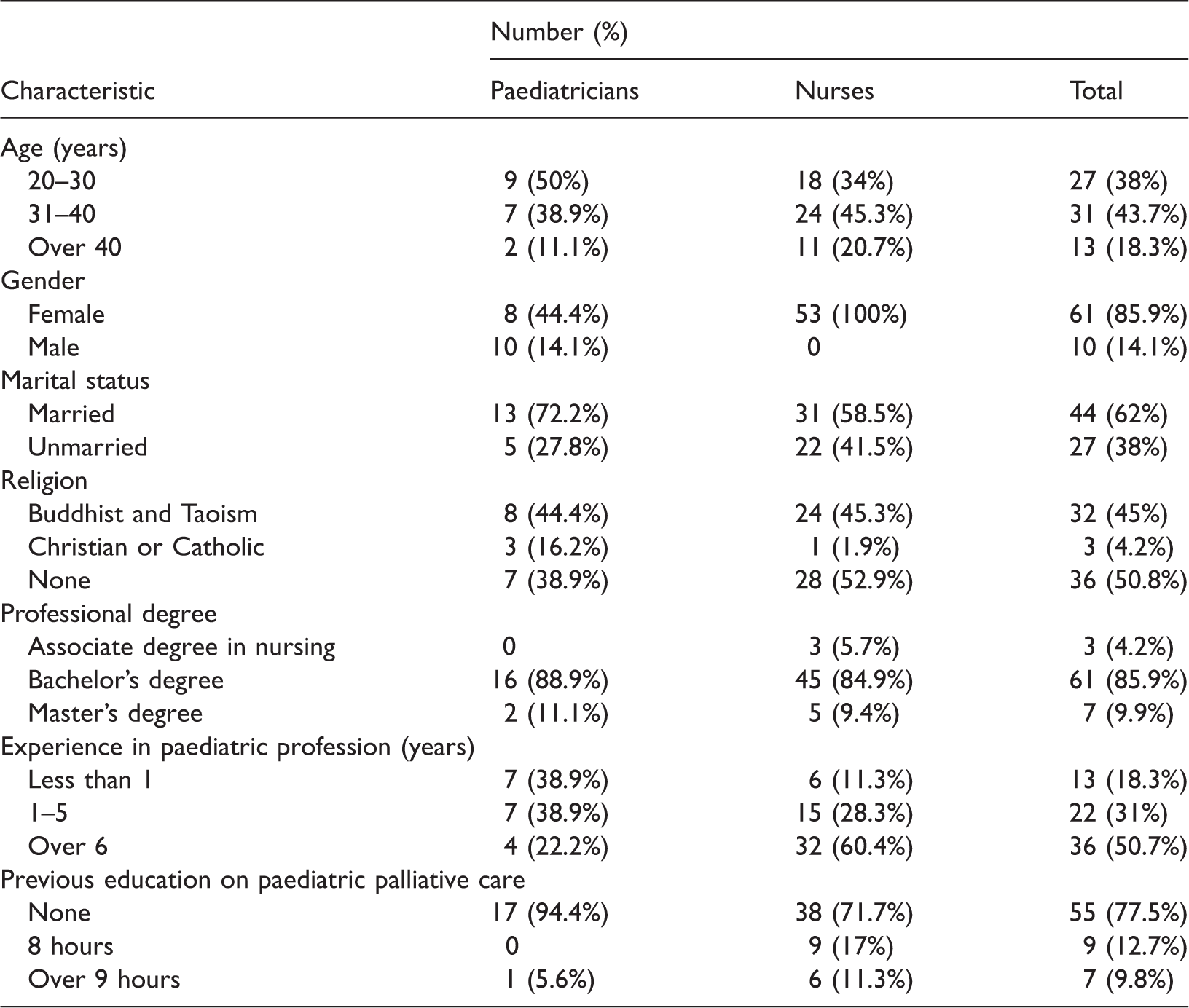
Demographic data (N = 71, physicians 18, nurses 53).
Comparison of the confidence scores pretest and posttest (N = 71, physicians 18, nurses 53).

Dependent variable: total score of confidence.
Model: (intercept); baseline score of confidence, occupations, time.
Time 1 = baseline (pretest); time 2 = posttest.
Group 1 = paediatricians; group 2 = nurses.
Comparing the attitude scores between pretest and posttest.

Dependent variable: total score of attitude.
Model: (intercept); total score of attitude, time.
Time 1 = baseline (pretest); Time 2 = posttest.
Group 1 = paediatricians; group 2 = nurses.
Distribution of changes in confidence levels (N = 71, physicians 18, nurses 53).
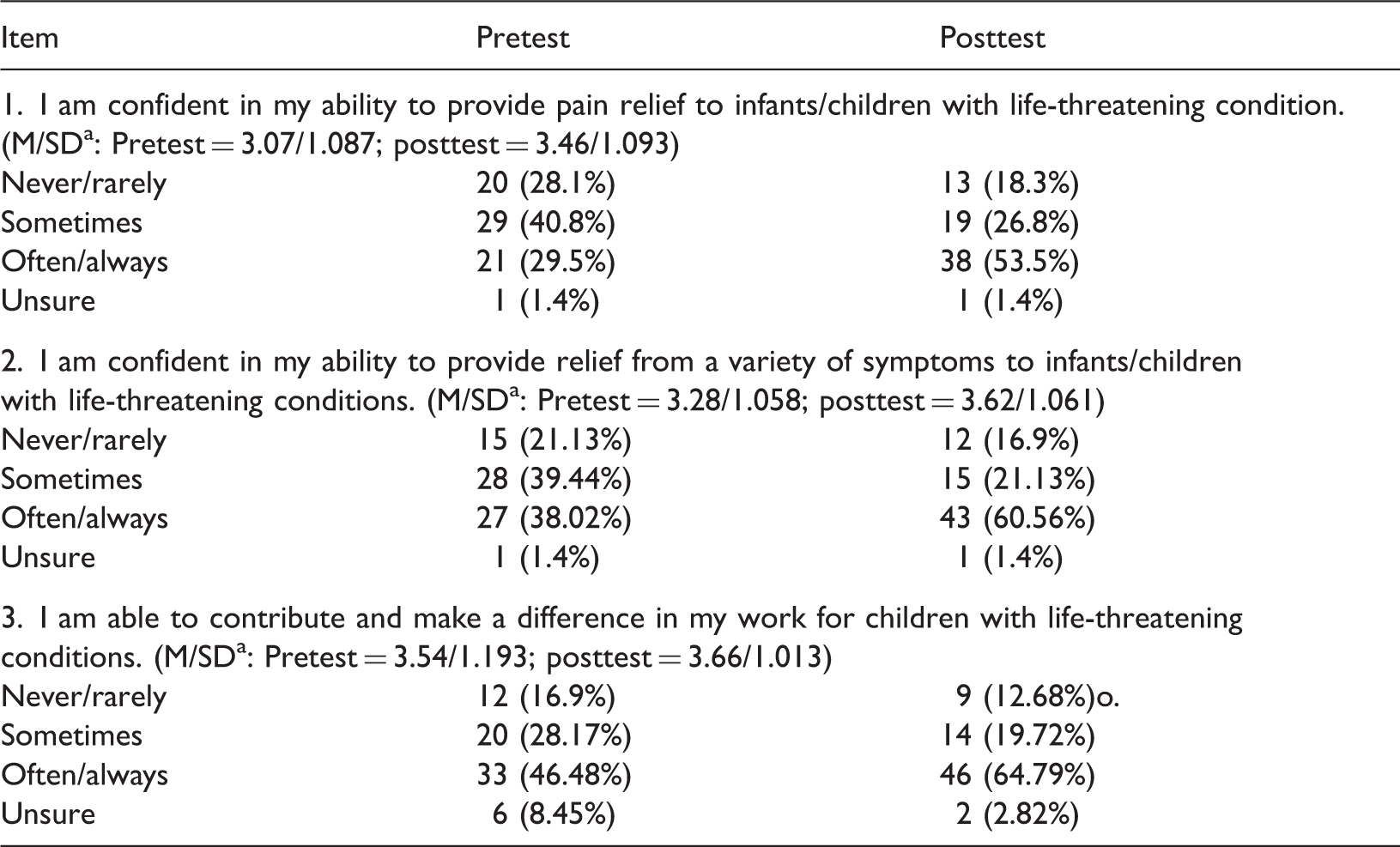
Code 1–2 = never/rarely; code 3 = sometimes; code 4–5 = often/always; code 6 = unsure.
Analysis of changes in attitudes (N = 71, physicians 18, nurses 53).

Code 1 = strongly disagree; code 2 = somewhat disagree; code 3 = unsure; code 4 = somewhat agree; code 5 = strongly agree.
Median/standard deviation.
Discussion
This research, in which most participants reported having received minimal or no previous training in paediatric palliative care, is consistent with a previous study (Lee et al., 2016). Clinicians’ insufficient education and resulting lack of knowledge may cause them to lack the confidence and willingness to provide pain/symptom management for dying children, forming a barrier to effective pain management in practice (Czarnecki et al., 2014; Ekim and Ocake, 2013).
Discussion of results
Overall, paediatric clinicians showed significant improvements in confidence and attitudes regarding pain and symptom management for infants or children with life-threatening conditions. These training outcomes were consistent with previous studies (Baker et al., 2007; Habich et al., 2012; McCabe et al., 2007; Michelson et al., 2009).
The research findings demonstrated that education can increase the confidence of paediatric clinicians regarding the provision of pain and symptom management for children with life-threatening conditions. After training, participants stated that they more often assessed dying children’s pain and distressed symptoms and discussed possible interventions with colleagues, revealing an increased willingness to cooperate across disciplines with other healthcare providers, as has been recommended by other researchers and professionals (Czarnecki et al., 2014; Grégoire and Frager, 2006; Habich et al., 2012). In a previous study, paediatric nurses cited physicians’ prescription patterns as a barrier to effective pain management (Lee et al., 2016), but since our research demonstrated that trained physicians and nurses may share similar attitudes and confidence levels regarding pain and symptom management, we propose that joint training sessions may be a good opportunity to promote a coordinated, unified approach to pain/symptom management within the healthcare team. The American Academy of Pediatrics (2000) and researchers (Wager et al., 2013) also recommended multimodal, interactive and integrative approaches to paediatric pain and symptom management. Therefore, education in interprofessional collaboration is critically required to provide successful paediatric pain and symptom management (Watt-Watson et al., 2012). Further studies are needed to survey the outcomes of interprofessional education regarding paediatric pain and symptom management (Wager, et al., 2013; Watt-Watson, et al., 2012).
In addition, after training, a majority of the respondents strongly/somewhat agreed that narcotic pain medication should be suggested to terminally ill children for the relief of physiological suffering. Although most participants would suggest narcotic medicines and explain their respiratory depressing effects to patients and families, the attitudes of some participants after training switched from agreement to somewhat/strong disagreement. This may indicate that paediatric clinicians harbour fears of the adverse effects of analgesic medications, including respiratory depression and addiction. Compounding this problem, for paediatric clinicians in Taiwan, discussing death and pain medication with patients or parents may be the most difficult issue in paediatric palliative care practice (Galloway and Yaster, 2000; Williams-Reade, et al., 2015).
Limitations
As this course was the first ever instance of pain and symptom management in paediatric palliative care training for paediatric clinicians in Taiwan, the five-hour course was insufficient to cover the topic adequately. Further training in clinical skills may be needed. The sample size was possibly too small to detect significant differences accurately between the attitudinal changes of paediatricians and nurses. In addition, clinicians’ attitudes and confidence levels were self-reported; there were no observations of behaviour to measure resulting changes in patient care. It would be informative to survey the patients’ responses after receiving pain/symptom management from clinicians after training. Further studies should include qualitative research data to determine which confidence levels and attitudes were most improved as a result of training and to reveal which paediatric patients benefit most from interventions.
Conclusion
Pain and symptom management is a vital part of paediatric palliative care. Paediatricians and paediatric nurses in this research after receiving training reported increased levels of confidence and improved attitudes towards providing pain and symptom management for children with severe illness. Future training for paediatric clinicians is needed, with a clear focus on emphasising the importance of the role of opioid therapy for dying children and providing information on pain assessment and management strategies. In addition, education in paediatric palliative care should focus content on effective ways to communicate with dying children and their families regarding pain management strategies, and should promote interdisciplinary healthcare teamwork to improve the effectiveness of pain and symptom management.
Key points for policy, practice and/or research
Providing adequate pain relief and symptom control in paediatric palliative care is a challenging area for paediatric clinicians. The evidence is clear that paediatric clinicians’ inadequate education may result in insufficient confidence to provide pain, symptom management, and an unwillingness to provide the interventions of pain and symptom management for children. Education in paediatric palliative care should promote interdisciplinary healthcare teamwork to improve the effectiveness of pain and symptom management.
Footnotes
Acknowledgements
The authors would like to acknowledge the lecturers of education: Ms Kathy Perko, Ms Joetta DeSwarte Wallace and Dr Dominic Wilkinson.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.