
Abstract
This paper describes the leadership and management competencies of head nurses and directors of nursing in social and health care. In the nursing profession, studies have tended to describe the role of the nurse manager, or to provide lists of competencies, talents and traits which can be found in successful managers. However, nursing managers’ leadership and management competencies lack any depth of research knowledge. Data were gathered by electronic questionnaire. Respondents (n = 1025) were head nurses and directors of nursing. The data were statistically analysed. Both groups evaluated their leadership and management competencies to be quite good and their general competence to be better than their special competence. Overall, directors of nursing rated their general competence and special competence better than head nurses. However, the head nurses had a stronger expertise in general competence areas, professional competence and credibility, and also in the special competence areas of substance knowledge than the directors of nursing. While the overall leadership and management competencies were good for both groups, each has identified areas which can be further developed.
Keywords
Introduction
Management in social and health care is currently undergoing many changes and reforms, both internal and external. This involves the reform of service structures, business processes and management (Cathcart et al., 2010; Fennimore and Wolf, 2011). The success of these reforms requires competent management (Groves, 2011). Therefore, management research information relating to social and health care is both timely and important (Buffington et al., 2012).
Additional to changes and reforms, both leadership and management practices and the role of the leader are affected by the rapid retirement of the baby boomer generation, and this will decrease the number of available leaders. Also, difficult economic conditions may force businesses to reduce costs by downsizing human resources at all levels within an organisation (Chavez, 2011; Groves, 2011). Changes in the organisation’s management, staff and services are reflected in nursing management, and introduce the need for new management competencies (Cathcart et al., 2010; Fennimore and Wolf, 2011; Germain and Cummings, 2010). Nurse managers are expected to have both leadership and management competencies, as well as substance knowledge. This also entails a knowledge of the operating management mechanisms of the system in which leaders function, as well as an ability to adapt to change. In addition, managers need skills in human resource management, finance and strategy. Management competencies relating to values and ethical issues are also seen to be increasingly important. Nurse managers must perform expertly in relation to regional, sub-regional and national targets, and also lead other experts within their group or organisation (McCallin and Frankson, 2010; Thomson and Hall, 2011; Wood, 2011).
This paper considers social and health care management from the perspective of nursing leadership and management competencies, and in relation to nurse managers (head nurses and directors of nursing) who work in different parts of Finnish municipal social and health care systems. The title ‘head nurse’ is used for nursing managers on a unit and ward level, and the title ‘Director of Nursing’ is used for middle and senior nursing managers on a clinic level. This paper describes their leadership and management competencies (general and special) from a self-assessment perspective, and explains their associated factors. In addition, their special competence is further discussed in relation to four competence areas: substance knowledge, human resources (HR) management, operational management, and research and development (Kantanen et al., 2011).
Background
Management is a set of processes that keeps an organisation functioning, and involves planning, budgeting, staffing, clarifying jobs, measuring performance and problem-solving when processes do not go according to plan (Jasper and Crossan, 2012; Pillay, 2011). Leadership, on the other hand, is about aligning people to a vision, and the leadership competence becomes visible in their buy-in, communication, motivation and inspiration (Andrews et al., 2012; Casida and Parker, 2011). While leadership and management are distinct concepts, there is a natural overlap between the skills that nurse managers are required to have. The concept of ‘leadership and management competencies’ identifies the knowledge, skills and attributes that a manager needs in order to be an expert in her/his field. It refers to the capabilities needed to work and function effectively in society, and to the management of the necessary knowledge, skills, values, motivations, attitudes and their associated levels of ability (Kantanen et al., 2011; Kantanen et al., 2017).
The concept of ‘leadership and management competencies’ has rarely featured in nursing research. In general, studies in nursing have investigated either leadership professional competence or management professional competence (Casida and Parker, 2011; Cummings et al., 2010; Hutchinson and Purcell, 2010; Jasper and Crossan, 2012; McCallin and Frankson, 2010; Supamanee et al., 2011; Thomson and Hall, 2011; Westphal, 2012; Wood, 2011), and have looked at inter alia, HR management, change and performance management, and leadership behaviours, standards and requirements (Azaare and Gross, 2011; Fealy et al., 2011; Macphee and Suryaprakash, 2012; Patton et al., 2013; Supamanee et al., 2011). Furthermore, several studies have described the role of the nurse manager as lists of competencies, talents and traits which can be found in successful nurse managers (Casida and Parker, 2011; Cummings et al., 2010; Hutchinson and Purcell, 2010; Jasper and Crossan, 2012; McCallin and Frankson, 2010; Supamanee et al., 2011; Thomson and Hall, 2011; Westphal, 2012; Wood, 2011). However, these lists fail to capture the experience-based judgement and practical knowledge that affect the leadership and management competencies required in the nurse manager’s pivotal organisational role (Cathcart et al., 2010). These lists cannot describe nursing managers’ leadership and management competencies as a whole, and research is lacking in how these competencies may be improved. Because skilled know-how is always context specific, nurse managers should self-assess their skills in any particular situation (Benner et al., 2010). For this reason, this paper looks to describe nurse managers’ self-assessed leadership and management competencies.
In our study, nurse managers’ leadership and management competency areas are investigated from the viewpoint of general and special competencies. For nurse managers the special competence area is structured using four categories: substance knowledge, HR management, operational management, and research and development (Kantanen et al., 2011).
Aim
The aim of this study was to explore the leadership and management competencies of head nurses and directors of nursing, and to study their associated factors.
Method
Participants and data collection
The survey was conducted in Finnish specialised and primary health care organisations, and also in the Finnish social care sector. The initial goal was to reach all of the above organisations (N = 159), but 68 of those approached declined to participate in the survey. Either they did not respond to the request, they did not have nursing leaders or nursing executives who were about to retire, or their organisational structure was going to change. As a result, the data were collected from the nurse managers of 91 municipal social welfare and health care organisations in the spring of 2014. All of the nurse managers (N = 2986) employed in these 91 organisations were asked to participate. The inclusion criterion was that potential respondents held the role of departmental sister, head nurse, charge nurse, nursing director, senior nurse, assistant matron or a similar role in primary or specialised health care, and these are later reported as either head nurses or directors of nursing.
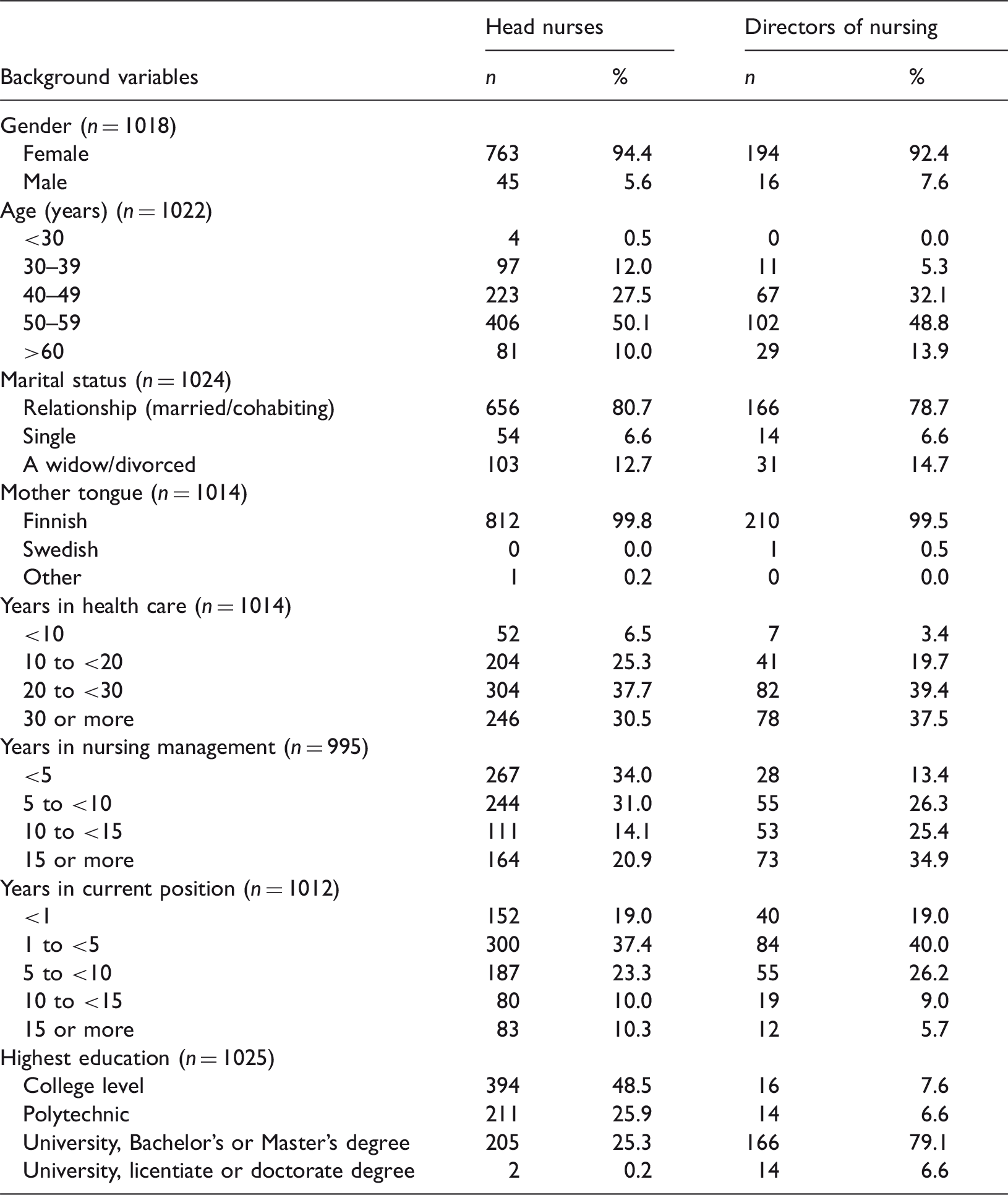
Participants’ demographic data.
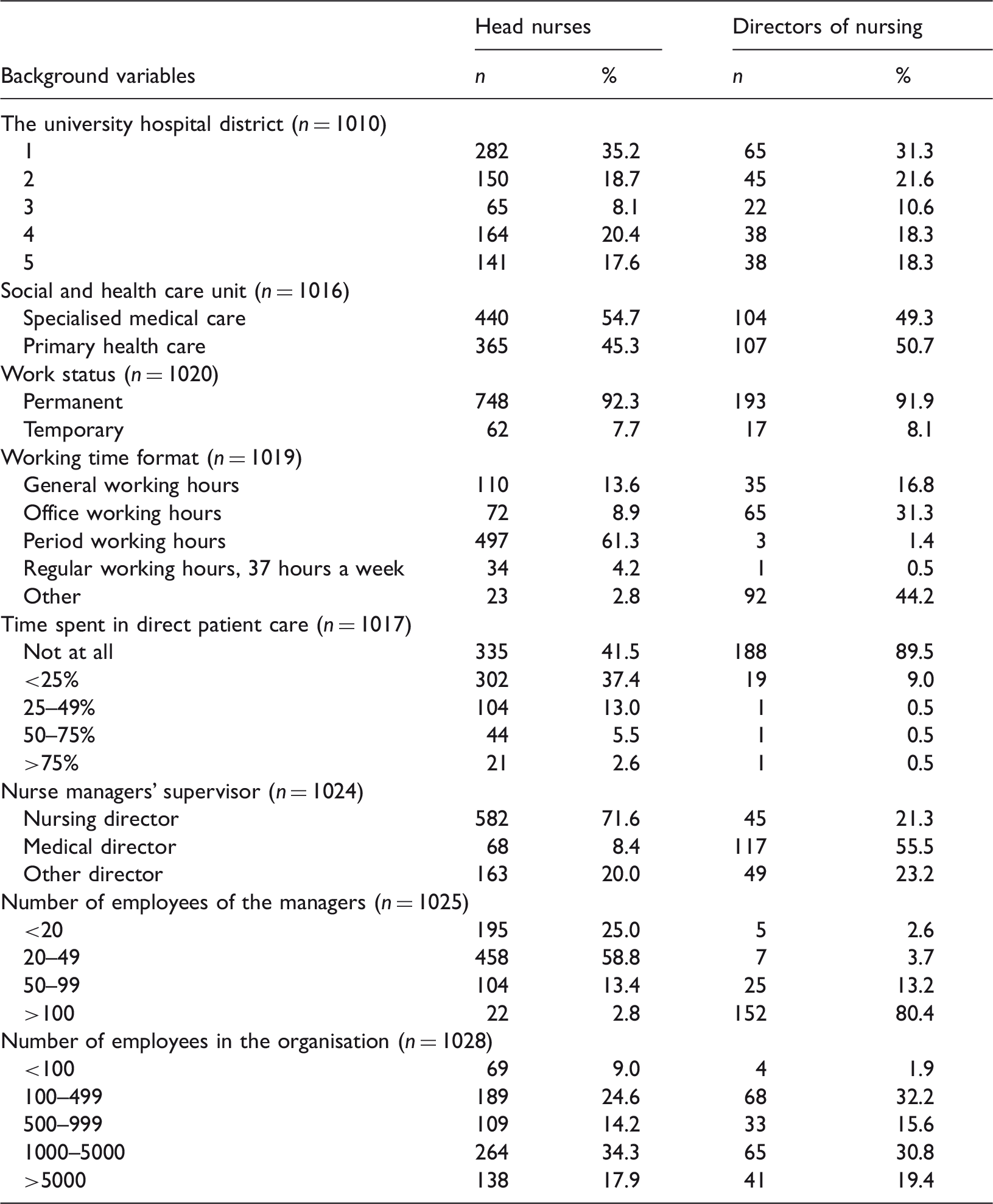
Participants’ work information.
Participants were given 1 month to respond (with two reminder letters sent), and a response rate of 34.4% (n = 1025) was achieved.
Data analysis
The data were analysed by statistical methods using SPSS 21-software. In the analysis phase, age was classified into five groups and professional experience into six groups. The data are described in terms of percentages, frequencies, means and standard deviations. Associations between variables were examined using cross-tabulation and correlation. In addition, the distributions of the variables were examined using histograms, together with measures of skewness and kurtosis. The distributions of the variables were skewed, therefore non-parametric Mann–Whitney U and Kruskal–Wallis tests were selected to be used in the analysis. The statistical significance limit was set at p < 0.05 (Burns and Grove, 2013; Hair et al., 2010). The mean values were categorised as ‘well’ (<1.5), ‘quite well’ (1.5–2.4), ‘moderate’ (2.5–3.4), ‘quite poorly’ (3.5–4.4) and ‘poorly’ (>4.5).
Ethical considerations
Research ethical considerations were taken into account at every stage of the study, and good scientific practice was followed in accordance with the guidelines provided by the World Medical Association Declaration of Helsinki (WMA, 2013). Permission to conduct the research was obtained from all of the organisations who participated. Based on Finnish national requirements, ethical approval was not needed for this type of survey research among nurses. However, the ethical considerations of study participants were upheld based on the provision of adequate information about the study, including the contact details of the researcher, the research topic description, data collection and the time spent on the research, the use, storage and further use of collected data, and the voluntarily nature of participation (WMA, 2013).
The technical functionality of the survey’s website was confirmed by constructing a simple web questionnaire and evaluating its performance. All questionnaires were filled out anonymously, and the responses could not be tracked back to the respondents. Answering the questionnaire was interpreted as the subject’s informed consent to process their supplied data. The responses were automatically saved to a password-protected database to ensure the security of the research data (Burns and Grove, 2013). The results of the study are also presented in such a way as not to identify individual respondents (WMA, 2013).
Results
The participants’ background information
Of the respondents, 79.4% (n = 814) worked as head nurses and 20.6% (n = 211) as directors of nursing. The majority were women (94.0%). The youngest respondent was 27 years old and the oldest 67 years old (mean age 52 years). The managers’ work experience in the health care sector averaged 25.7 years (SD 8.79), and their experience as managers averaged 11.2 years (SD 8.51). On average, they had worked in their current position for 6.6 years (SD 6.74). Almost half of the head nurses had a college-level education (48.5%), while directors of nursing usually had a Bachelor’s or Master’s degree (79.1%) (Table 1).
Geographically, the respondents represented all five Finnish university hospital districts, each with a population base of approximately one million people. Of the head nurses, 54.7% worked in specialised health care and 45.3% in primary health care. Similarly, 49.3% directors of nursing worked in specialised health care and 50.7% in primary health care. As a rule, head nurses and directors of nursing were in a position of permanent employment (92.3%). More than half of the respondents worked a shift system (52.5%), and half of the respondents did not undertake direct patient work (51.4%). The majority (71.6%) of the head nurses had a nursing manager as their own upper-level manager, but more than half (55.5%) of directors of nursing had a medical doctor as their own manager. Around two-thirds (69.3%) of nurse managers had fewer than 50 subordinates (Table 2).
Leadership and management competencies
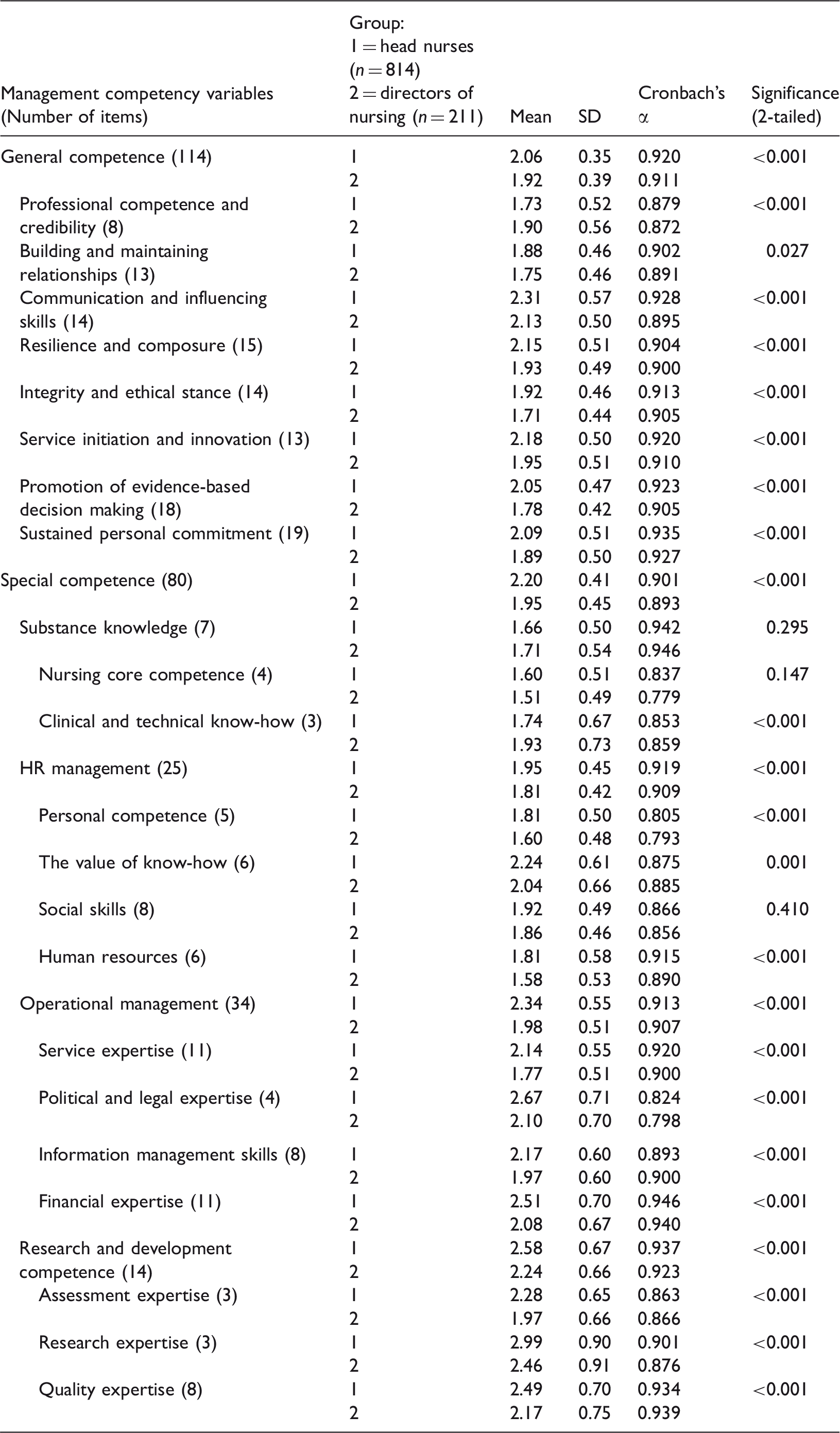
Head nurses and directors of nursing considered their own leadership and management competencies to be quite good (mean 2.11, SD 0.42 vs mean 1.93, SD 0.40). Of the studied competence areas, head nurses (mean 2.06, SD 0.35) and directors of nursing (mean 1.92, SD 0.39) evaluated themselves to be most competent in areas of general competence. Head nurses (mean 2.20, SD 0.41) and directors of nursing (mean 1.95, SD 0.45) tended to rate themselves as less competent in the investigated areas of special competence.
General competence
Leadership and management competencies of head nurses and directors of nursing.
Background variable association with leadership and management competencies.
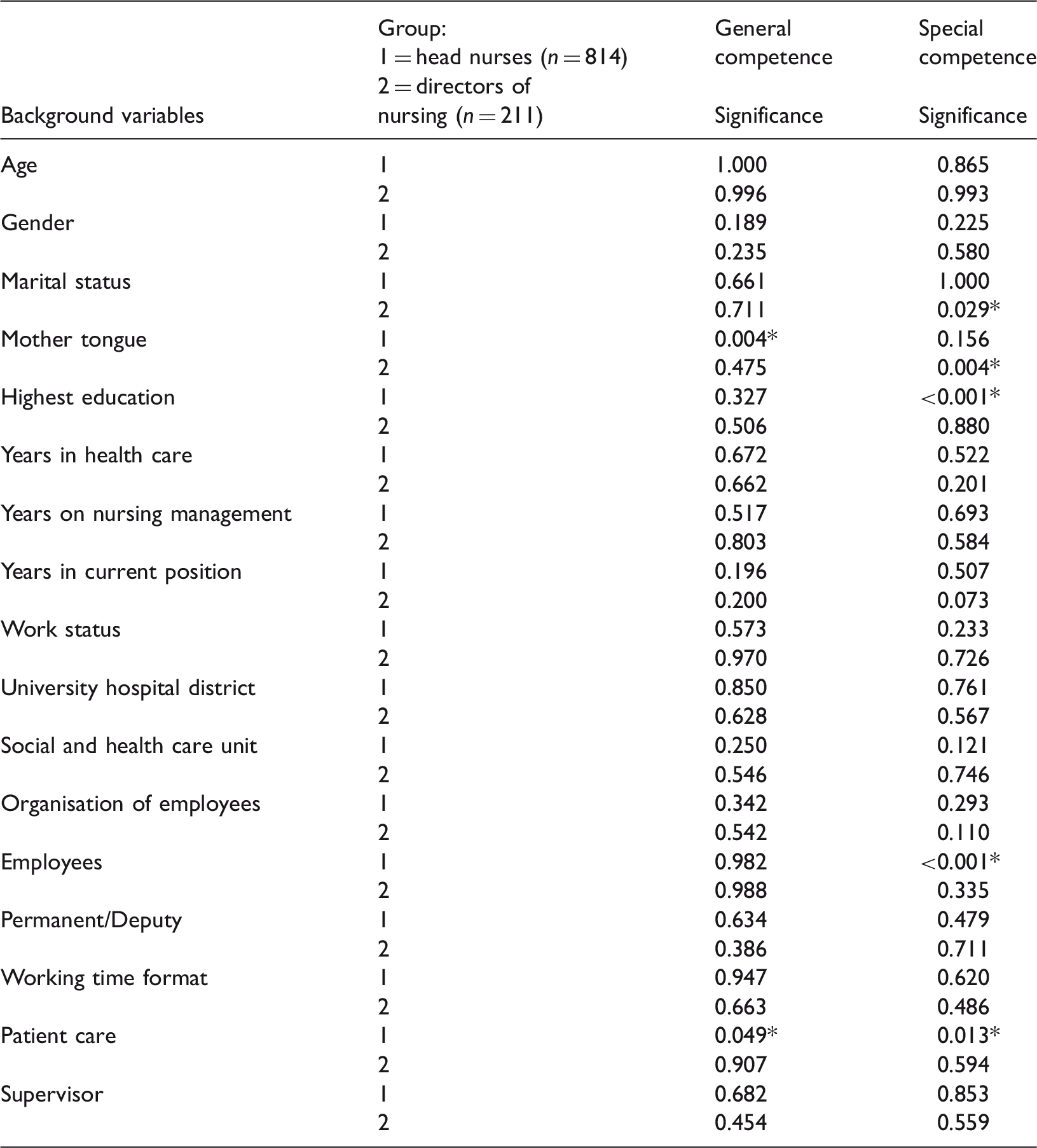
Statistically significant (sig. < 0.05).
Special competence
Head nurses (mean 2.20, SD 0.41) and directors of nursing (mean 1.95, SD 0.45) perceived their special competence to be quite good (Table 3). Head nurses (mean 1.66, SD 0.50) evaluated their substance competence better compared with directors of nursing (mean 1.71, SD 0.54). However, in other areas of special competence the directors of nursing assessed their competencies to be significantly better than the head nurses.
Marital status, mother tongue, highest education, the number of subordinates, and time spent in direct patient care had an association with how managers rated their special competence (Table 4).
Marital status (p = 0.029) and native language (p = 0.004) were statistically significantly associated with the special competence of directors of nursing. Respondents who were married or cohabiting assessed their competences better (mean 1.93, SD 0.04) than respondents who were single (mean 2.13, SD 0.13). Those respondents with Swedish as their native language rated their special competence highest (mean 1.94, SD 0.15).
The highest level of education (p ≤ 0.001), the number of subordinates (p ≤ 0.001) and the amount of time spent in direct patient care (p = 0.013) were statistically significantly associated with the head nurses’ special competence. Respondents who had completed a Bachelor’s or Master’s degree rated their competences best of all (mean 2.14, SD 0.33), and the worst ratings were seen among those who held licentiate and doctorate degrees (mean 2.35, SD 0.14). Head nurses with fewer than 20 employees assessed their competences the best (mean 2.18, SD 0.04), and those with 50–99 employees assessed their competences the worst (mean 2.23, SD 0.05). Head nurses who did not work in direct patient care rated their special competences the best (mean 2.17, SD 0.03), while those who worked 50–75% of their work time in direct patient care rated their special competences the worst (mean 2.36, SD 0.07).
Substance knowledge
Background variable association with special competence.
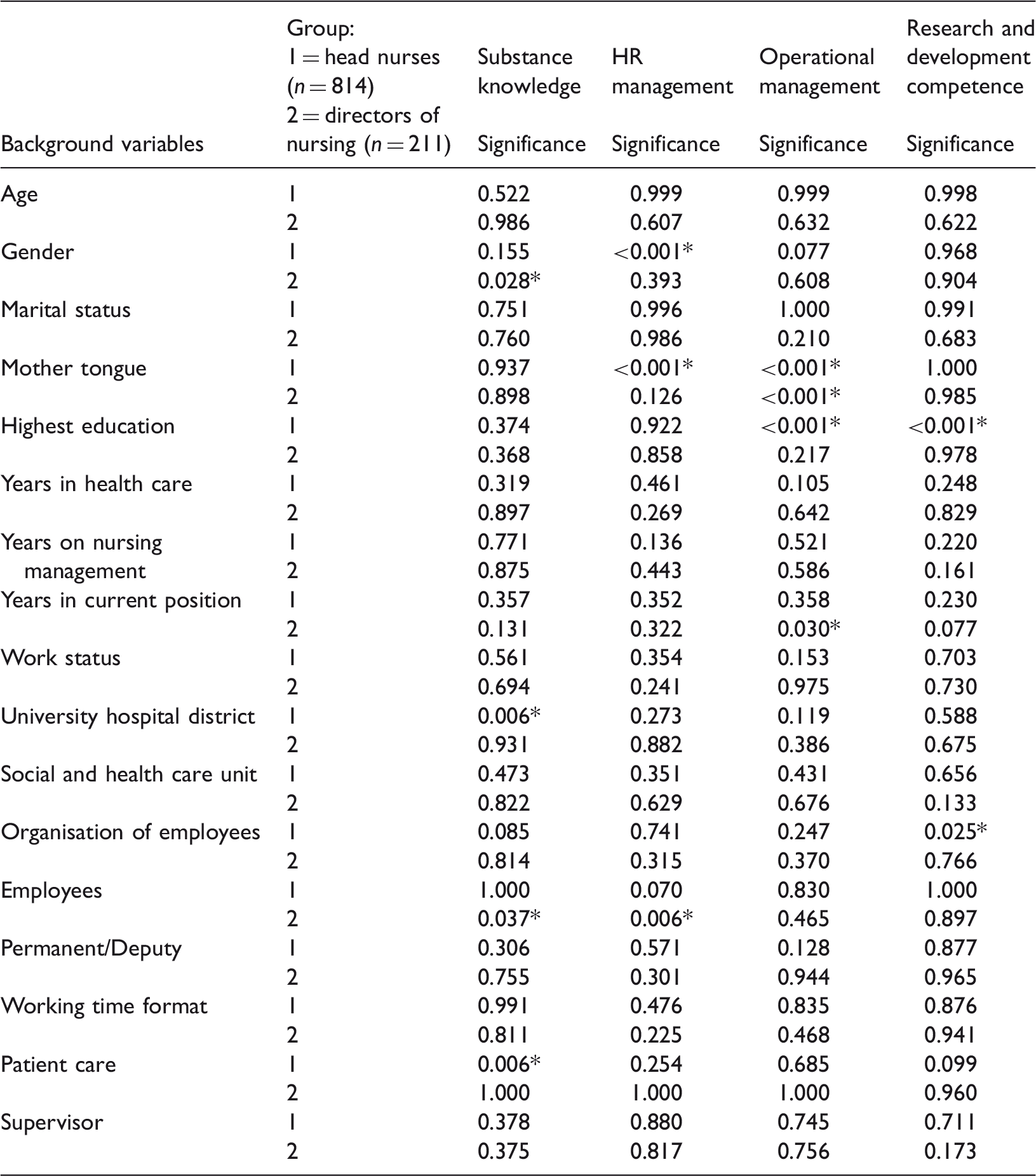
Statistically significant (sig. < 0.05).
Gender (p = 0.028) and the number of subordinates (p = 0.037) were statistically significantly associated with the substance knowledge of directors of nursing. Female respondents rated their competences better (mean 1.70, SD 0.04) than their male counterparts (mean 1.79, SD 0.16). Substance knowledge competence was seen as best with managers who had over 100 subordinates (mean 1.63, SD 0.09), and worst among managers with 20–49 subordinates (mean 1.75, SD 0.06).
The university hospital district the head nurses were from (p = 0.006) and how much they were involved in direct patient care were variables which held a statistically significant association with how head nurses evaluated their substance knowledge. The competence of head nurses was seen to be best in those who worked over 75% of their work time in direct patient care (mean 1.54, SD 0.12), and worst in those who spent 50–75% of their time in patient care (mean 1.78, SD 0.07).
HR management competence
The HR management competence (HRM) of both groups was evaluated to be quite good for both head nurses (mean 1.95, SD 0.45) and directors of nursing (mean 1.81, SD 0.42) (Table 3), but with a highly statistically significant difference (p ≤ 0.001) between the groups. Directors of nursing assessed their knowledge better than the head nurses throughout the HRM competencies, which concerned personal competence, the value of know-how, social skills and HR areas (Table 3).
Few of the background factors of head nurses and directors of nursing, such as gender, mother tongue and the number of employees they managed, were associated with how managers rated their HRM (Table 5).
The respondents’ gender (p ≤ 0.001) and mother tongue (p ≤ 0.001) were statistically significantly associated with head nurses’ HRM. Female respondents rated their competences better (mean 1.94, SD 0.02) compared with their male counterparts (mean 2.09, SD 0.08). Respondents with Finnish as their mother tongue rated their competence better (mean 1.94, SD 0.08) than those with Swedish as their mother tongue (mean 2.06, SD 0.08). Similarly, among the directors of nursing, the number of subordinates was statistically significantly associated with HRM (p = 0.006). HRM was seen to be best among those who were supervisors of more than 100 employees (mean 1.65, SD 0.06), and worst among those who supervised 20–49 employees (mean 1.88, SD 0.04).
Operational management competence
The operational management competence (OM) of both groups was evaluated to be quite good, although directors of nursing estimated their OM better (mean 1.98, SD 0.51) than head nurses (mean 2.34, SD 0.55) (p ≤ 0.001) (Table 3). This was reflected through OM as a whole, and concerned areas of service expertise, political and legal expertise, information management skills and financial expertise (Table 3).
Correlating background factors related to the respondent’s mother tongue, their highest education level and their years in their current position (Table 5). Mother tongue (p ≤ 0.001) and highest education (p = 0.001) were statistically significantly associated with the head nurses’ OM. Respondents with Finnish as their mother tongue rated their competence better (mean 2.21, SD 0.03) than those with Swedish as their mother tongue (mean 2.44, SD 0.11). Respondents who had completed a Bachelor’s or Master’s degree rated their OM best (mean 2.27, SD 0.04), and the worst ratings were seen amongst those who held licentiate and doctorate degrees (mean 2.47, SD 0.13).
Mother tongue (p ≤ 0.001) and the years spent in current position (p = 0.030) were statistically significantly associated with the OM of directors of nursing. Respondents with Finnish as their mother tongue rated their OM competence better (mean 1.98, SD 0.04) than those with Swedish as their mother tongue (mean 2.11, SD 0.19). Directors of nursing with a current position experience of 5–9 years had the best level of competence (mean 1.94, SD 0.08), contrasting with those who had less than 1 year’s experience (mean 2.13, SD 0.07) who showed the worst.
Research and development competence
Research and development competence was evaluated to be quite good by the directors of nursing (mean 2.24, SD 0.66) and moderate among head nurses (2.58, SD 0.67) (Table 3). Directors of nursing had a stronger research and development competence than head nurses. This concerned research and development as a whole and featured competencies such as assessment expertise, research experience and quality expertise (Table 3).
Two background factors were statistically significantly associated with head nurses’ research and development competence. These were their highest level of education (p ≤ 0.001) and the number of employees in the organisation (p = 0.025) (Table 5). The head nurses with a Bachelor’s or Master’s degree assessed their competence better (mean 2.51, SD 0.05) than those with a polytechnic degree (mean 2.66, SD 0.05). The competence of head nurses was seen as best among those who worked in organisations with less than 100 employees (mean 2.51, SD 0.09), and worst in organisations with 100–499 employees (mean 2.66, SD 0.05). The nursing directors’ background variables were not statistically significantly associated with their research and development competence.
Discussion
The results of this study suggest that head nurses and directors of nursing consider themselves to have quite good leadership and management competencies. However, it should be noted that competence is always context related, which is why a self-assessment by nurse managers of their skills in their own particular situation is important (Benner et al., 2010). Self-assessment gives the respondents a possibility to gain ownership of developing their leadership and management competencies. From an organisational perspective, this may help to better understand the strengths and development needs of the management, and lead to the head nurses and directors of nursing being more willing to participate in any training that is provided. A self-evaluation is not meant to identify whether the respondents are ‘better’ or ‘worse’ managers. However, as a method, self-assessment is only one of the possible evaluation means and thus has its limitations. In particular, it is possible that the respondents are either too critical, try to respond in a way that they perceive to be socially or organisationally acceptable, or simply do not recognise all of their competence areas. Thus, the results of this study should be critically considered from their methodological starting point, and should an external evaluation of different management competencies be required, then another method should be chosen.
Also, when considering the wider implications of the results, it has to be acknowledged that the research was conducted in the Finnish social and health care system. Hence there are national differences which have to be taken into account, for example the specific responsibilities of the two groups of nurse managers, which are likely to differ between countries. However, as all countries have different levels of nursing managers, and their competence areas differ accordingly (see e.g. Pillay, 2011), it is important that the topic is studied in different contexts. So although this study adds to the body of knowledge on leadership and management competence within nursing, it should be considered as a Finnish perspective on the overall discussion.
Directors of nursing rated their general and special competence better than head nurses. However, the head nurses rated their general competence areas of professional competence and credibility better than the directors of nursing. Exploring managers’ special competence, head nurses evaluated their substance knowledge better than directors of nursing. However, directors of nursing rated all of the other areas of competence better than head nurses. Both groups can be seen to have a lot of knowledge in relation to direct patient care, the management and leadership of staff, and organisational resource management. In addition, nursing managers have a good knowledge of service quality and legislation targets. They also know how to operate within set budget boundaries. These results echo those of previous studies that examine municipal sector management skills, where public sector managers consider their main management skills as controlling, leadership and organising (Pillay, 2011). The results also show that although technical competence is of importance among head nurses, human and conceptual skills have become more important for directors of nursing.
Respondents generally evaluated their substance knowledge as quite good, but their practical nursing skills differed and some of the respondents assessed their expertise in this field to be only moderate. In the nursing context, it is important to notice the difference between current skills and required skills, especially when the role of nurse leaders is changing. Although change is a universal constant for nurse leaders throughout the world, the potential for role overload or role confusion increases. McCallin and Frankson (2010) wrote that the multiple demands stemming from wide-ranging sources such as staff, colleagues, patients, families and the wider organisation were such that nurse managers felt that role expectations caused role overload. Also, in this study, in the general competence areas of resilience and composure there was evidence of mediocre or even poor knowledge, of stressful work situations which might be avoided, as well as issues of work–life balance.
It is clear that a wide variety of role requirements and ongoing reform processes press for nurse managers’ competencies to be strengthened. The results show that head nurses and directors of nursing self-rated their competence as mediocre in regard to evidence-based nursing and nursing development expertise, as well as the effectiveness of nursing and science between services. Also, nursing resource planning and financial expertise were seen to be weaker than the other areas of expertise that were evaluated. A fifth of the respondents rated their expertise in national and local social and health care quite poorly, and inevitably it comes to mind that this evaluation is affected by the fact that these areas perhaps do not get the scientific attention they deserve (Jasper and Crossan, 2012). However, there is more and more evidence that the role of nurse leaders has changed significantly over recent decades (Hutchinson and Purcell, 2010), and focus is shifting towards broader areas of responsibility (Asamani et al., 2013). This underlines the need to develop skills in different management activities (Asamani et al., 2013), as well as those to do with business, information and skills development (Jasper and Crossan, 2012).
Additional to this study, a number of previous studies have shown that a new nursing leadership must possess synthesised competencies that include substance competence and also the management of services from a business perspective. Nursing management is a discipline that combines the practice and caring aspects of nursing with the theories and methods of administration. The results of this study suggest that nursing managers have wide-ranging expertise, as well as global leadership and change management skills. They also have competencies in managing the practical aspects of their field.
Conclusions
The aim of this study was to explore the leadership and management competencies of head nurses and directors of nursing, and to explain their associated factors. The study presents an overview of the competencies, but does not explain the detailed skill mix that lies within them. However, this would be an interesting topic for further investigation, as the different skill mixes within competencies may have an effect on how head nurses and directors of nursing manage their duties. Some of the background factors, for example marital status, mother tongue and education, were statistically significant for either head nurses or directors of nursing, and either general competence or special competence. These offer an interesting starting point for further analysis and study of the complex phenomenon of the self-assessment of competence. This study of leadership and management competencies was cross-sectional, so a need exists for longitudinal research that will update and improve the depth of research information. In addition to better describing the current situation, this would also increase the awareness and visibility of nursing management and may improve its quality.
Nursing management is an important part of daily nursing practice. It is carried out in constantly changing circumstances which shape the management context, and which substantially affect the perception of the core mission of nursing leadership and management, as well as the nurse managers’ competence. Therefore it is time for a discussion about the definition of nurse managers’ leadership and management competencies, and how they may be improved. This study makes visible the leadership and management competence of the head nurses and directors of nursing as they assessed it at the time the study was conducted. It would therefore be both interesting and potentially beneficial to extend this study to see how these self-perceptions change over time. In this way, it may be possible to better understand the experience-based judgement and practical knowledge which affect nurse managers’ leadership and management competencies.
Key points for policy, practice and/or research
The results of the study highlight a need for head nurses to improve their expertise in the general competence areas of communication and influencing skills, and in service initiation and innovation. Head nurses should strengthen their special competence with regard to research, political and legal issues, finance and quality. Directors of nursing should increase their expertise in general competence areas of communication and influencing skills, and in special competence areas of research, quality and finance. This information may be used across a wide range of health care organisations and educational settings in the Finnish context.
Footnotes
Acknowledgements
Study design: KK, TS, MK; Data collection and analysis: KK, MH; Manuscript preparation: KK, TS, MK, MH.
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research has been partly funded by the Competitive State Research Financing of the Expert Responsibility area of Tampere University Hospital (grant number 9S065).