
Abstract
Research results hold value for many stakeholders, including researchers, patient populations, advocacy organisations and community groups. The aim of this study is to describe our research team’s systematic process in designing a dissemination strategy for a completed research study. We organised a dissemination event to feed the results of our study to participants and stakeholders and collect feedback regarding our study. We applied the Agency for Healthcare Research and Quality’s dissemination framework to guide the development of the event and collected participant feedback during the event. We describe our dissemination strategy along with attendees’ feedback and suggestions for our research as an example of a way to design a patient- and community-focused dissemination. We explain the details of our dissemination strategy, including (a) our process of reporting a large research study into a stakeholder event, (b) stakeholder feedback collected at the event and (c) the translation of feedback into our research team’s studies. We also describe challenges encountered during the dissemination process and ways to handle issues such as logistics, funding and staff. This analysis provides key insights and practical advice for researchers looking for innovative ways to disseminate their findings within the lay and scientific communities.
Keywords
Introduction
The research dissemination process is a crucial aspect of any study, especially research that directly involves the community (Chen et al., 2010). The knowledge produced through systematic investigations (a) informs the development of knowledge within the scientific field, (b) ensures that the study’s methods, analysis and conclusions are open to scientific and public scrutiny and (c) guarantees that those with a vested interest in the research understand and find benefit from the study’s findings. The Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) statement sets guidelines for ethical ways of disseminating research, stating that dissemination ‘honors the altruistic motivations of patient-subjects’, that participants are ‘entitled to know the results of the research their enrollment made possible’, and that dissemination is ‘consistent with the duty to share new knowledge’ (Mann, 2005). While peer-reviewed journals, professional conferences and professional communities remain excellent mechanisms by which to deliver results to the scientific community, researchers should capitalise on the opportunity to bolster their professional objectives by distributing research results widely to all stakeholders (Chambers and Azrin, 2013).
As nurse researchers, we must acknowledge the value of our research across multiple audiences (Timmins, 2015). We must strive to appreciate the potential impacts of our research for study participants, patient populations, community organisations and policy organisations alike. Our scientific research may be valuable in ways not originally intended by our scientific question, and the dissemination process and planning of future research is an ideal time in which to engage these stakeholders (Anderson et al., 2014).
Our research team recently experienced such a crossroads at the end of a national, cross-sectional study among adult females with a history of cancer. Our parent study aimed to develop a measure of patient self-advocacy to assess their ability to get their needs met in the face of challenge. We believe that this concept is crucial in the current climate of ongoing health inequities (Adler et al., 2016; Lyratzopoulos et al., 2013), increasingly complex medical care (Collins et al., 2009; Reyna et al., 2015) and vested interests in promoting patient engagement in their healthcare decisions (Frank et al., 2015). We decided to disseminate the results of our study not only to our participants, but to wider community audiences who had vested interests in discussing our results and imaging potential future steps. In this way, we could both share our results and build community with like-minded individuals and community partners interested in addressing the need for patient self-advocacy.
The purpose of our one-time dissemination strategy and activities was to inform, empower and engage a multitude of groups interested in improving the health of women with cancer. This analysis is meant to give practical and translational guidance to researchers who are interested in disseminating their research in novel ways, and to stakeholders who are interested in partnering with researchers in the scientific process.
Methodology
Parent study
We sought to disseminate our mixed-mode, cross-sectional survey study testing the psychometric properties of a new measure of self-advocacy among female cancer survivors (Hagan et al., 2016a; Hagan et al., 2016b). The Self-Advocacy Study took 3½ years to complete and was based on qualitative pilot work describing how patients define and enact self-advocacy (Hagan and Donovan, 2013). We recruited women locally from the western Pennsylvania area as well as nationally through cancer-related advocacy groups to complete a battery of paper or online questionnaires about their health history, cancer- and treatment-related symptoms, beliefs about their health, and personality traits. Inclusion criteria for this parent study included being female, having a previous diagnosis of an invasive type of cancer, and being able to read and write in English. Participants (N = 347) were recruited nationally and locally from two patient research and tumour registries, cancer clinics and seven advocacy organisations. This study received human subjects approval from the University of Pittsburgh Institutional Review Board.
While we did not design this study using community-based participatory research principles, we collected input from women with cancer, advocacy organisations and other stakeholders at all stages of the Self-Advocacy Study. We wanted to know stakeholders’ preferences and attitudes about patient self-advocacy, the design and implementation of the study and potential uses of a self-advocacy scale we were developing. We met with leaders from the patient registries, cancer clinics and advocacy organisations to discuss the study and potential collaborations before, during and after the study. As a measure of trust-building and collaboration, we promised each of our recruitment sites that we would share the results of the study with them and their membership at the end of the study. Most organisations requested receiving the results of the study for education of their stakeholders and organisation.
Dissemination event
As we completed the Self-Advocacy Study, our research team began to consider possible strategies to efficiently and fruitfully disseminate our results to multiple groups of lay and scientific stakeholders. Despite our study being a one-time survey study, we grew close to our participants during the course of the process as we heard their stories of advocating for their healthcare and personal needs. Even though we conducted qualitative pilot work exploring patient experiences of self-advocacy, we recognised that this study was exposing patients’ additional concerns. We concluded that patients and our stakeholders required a larger forum in which to discuss patient self-advocacy. We wanted to provide space to discuss the challenges to having patients speak up for their values and preferences and brainstorm ways to build self-advocacy skills in vulnerable patient populations.
Our main dissemination event consisted of a large one-day dissemination meeting and discussion in August 2015. We invited participants from the parent study, individuals from our recruitment sites, and community members who would be interested in promoting patient self-advocacy. At this event we presented the findings of our research study, encouraged stakeholders to discuss the findings with each other, and together developed strategies for future research studies. We did not intend for this event to be a formal research study, but did want to capitalise on the opportunity to receive feedback from multiple stakeholders and collectively discuss future steps for our research team’s long-term programme of research.
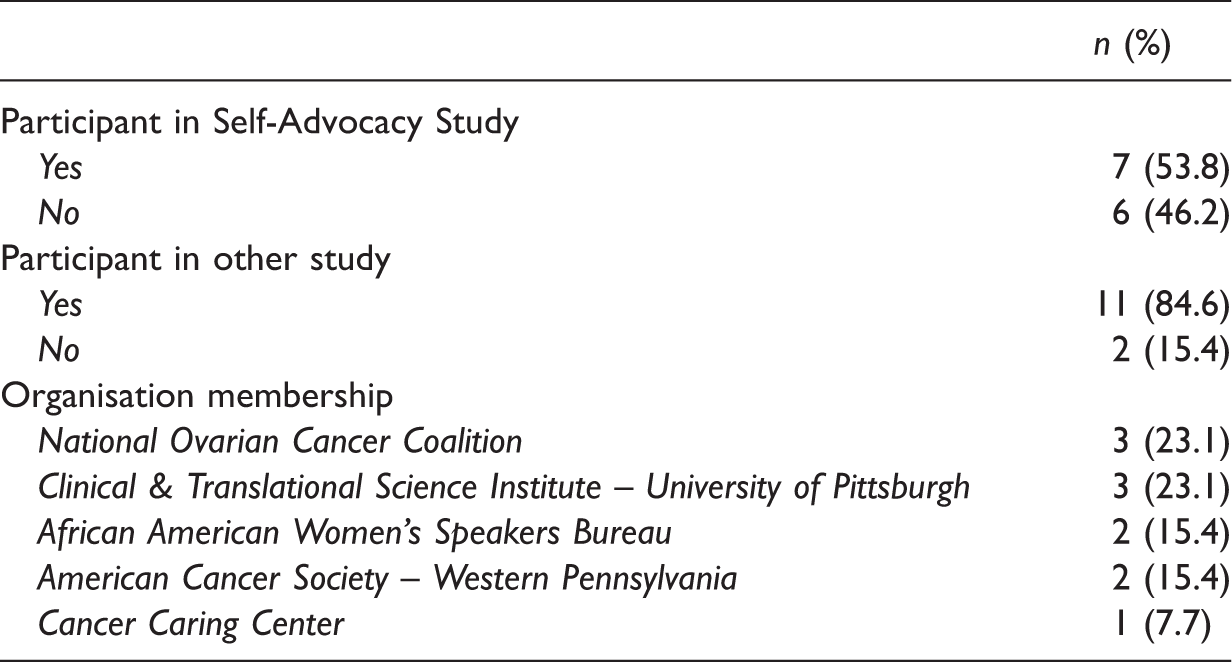
Dissemination event attendees (n = 13).
The event lasted an hour and a half and consisted of lunch, a brief presentation describing the Self-Advocacy Study’s purpose and results, and a testimonial from a woman with ovarian cancer describing her experience of self-advocacy. This testimony was intended to provide a real-life description of the clinical problem and reinforce the need for research to improve self-advocacy among women with cancer.
While describing the study, we shared a brief overview of the final self-advocacy scale and its items. Rather than discuss the validity and reliability statistics supporting the psychometric strength of the instrument, we discussed the meaning of the scale (what each sub-dimension meant and how the scale could be used). We focused on data that was relevant to our audience in order to provide context and the results of the study to them. We encouraged questions from the audience and received many thoughtful comments throughout the presentation.
Next, attendees broke up into small groups to discuss the Self-Advocacy Study’s findings and future study directions. They were instructed that their feedback would be used by the research team in their making of patient education and future research studies. Therefore attendees were encouraged to talk openly and freely, and assured that all perspectives were equally valuable. We wrote the questions below to elicit feedback on study results and brainstorm future research and patient support:
From what the study found out about self-advocacy, do you think the researchers are missing any critical parts of how patients advocate for themselves? From what the study found out about self-advocacy, what do you think is the best way to help teach women how to advocate for themselves? How would you specifically try to do this?
After the small group discussions, the entire group reconvened to share findings and discuss future research priorities. Research team members facilitated the conversation within each small group, took notes to document the discussion, and kept a log of suggestions. The same research team members recorded notes from the large group discussion.
Dissemination framework
We searched for dissemination frameworks that would provide us with a structured method for disseminating research into the community and collecting feedback from stakeholders. The Agency for Healthcare Research and Quality (AHRQ) created the dissemination planning tool (Figure 1) in an effort to support researchers in effectively disseminating their research. We selected this framework because its first step reflected our research study’s status (e.g. research findings) and the framework’s specific, targeted steps for creating a robust dissemination plan including identifying and defining (a) research findings and products, (b) end users, (c) dissemination partners, (d) communication, (e) evaluation and (f) dissemination work plan (Carpenter et al., 2013). This framework is intended to serve as a tool for researchers to market the unique aspects of their research to those multiple end users.
Agency for Healthcare Research and Quality’s dissemination planning tool.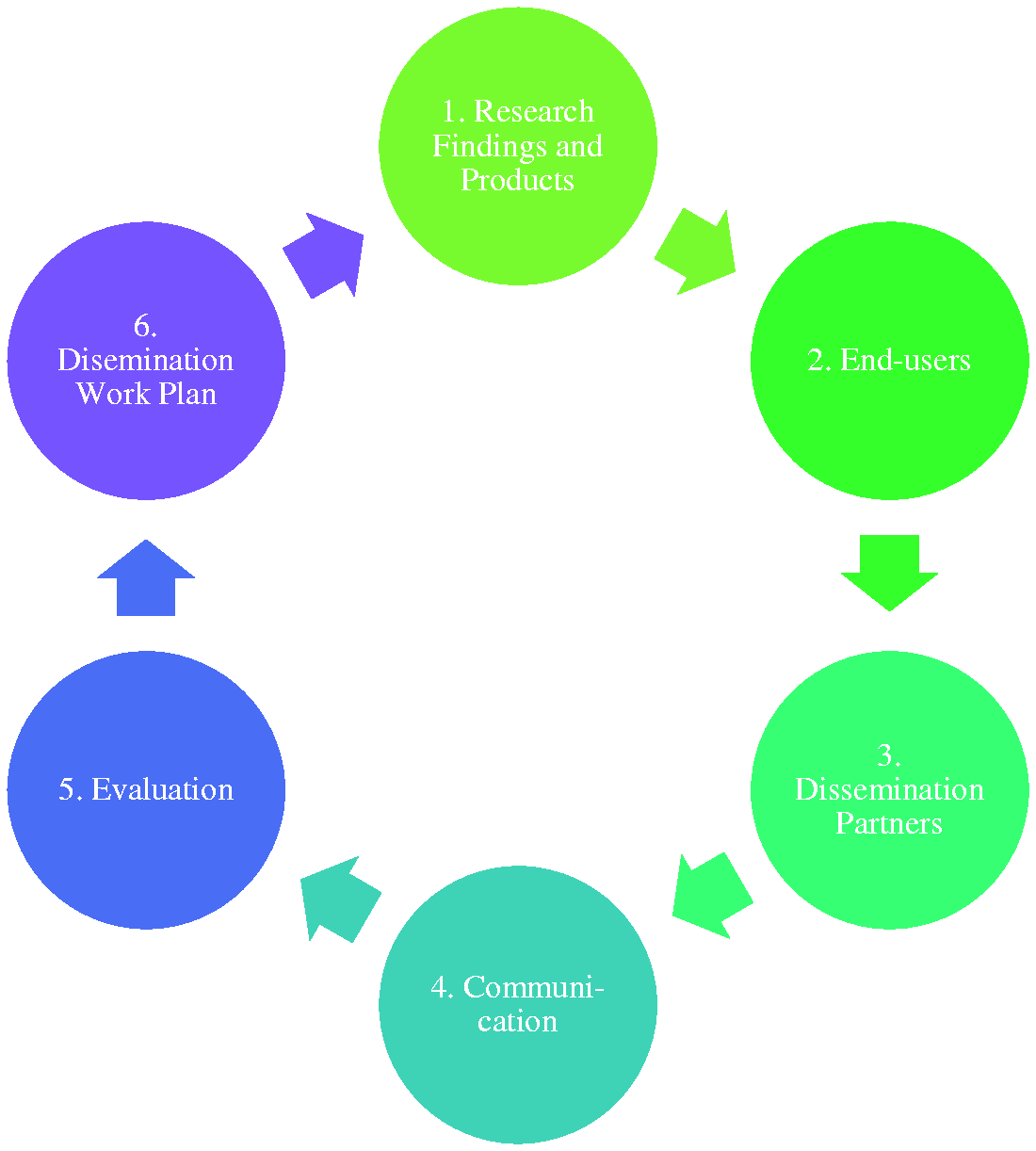
In this paper, we describe our application of the AHRQ framework to the Self-Advocacy Study’s dissemination plan. Using the steps of the framework, we will expound on our planning and implementation of the dissemination event, and then describe the results of this event especially as they pertain to involving patients and community stakeholders in our research programme.
Results
Dissemination strategy results
We describe the results of our dissemination strategy as they relate to the AHRQ dissemination framework.
Research findings and products
We designed our dissemination strategy to involve our partners in our dissemination process by presenting them with the results of our Self-Advocacy Study at our dissemination event and asking for their advice during this event. We purposefully chose not to make assumptions about how stakeholders would interpret our research findings. Rather, we specifically wanted their guidance on how the study results should be used to both inform future studies and develop patient education teaching self-advocacy skills to individuals with cancer.
Developing research products for dissemination required a shift in viewpoint among the research team. The scientific findings of our study were related to the psychometric properties of our new self-advocacy scale, and we are currently reporting these results in scientific journals and at scientific conferences. Study participants and recruitment sites were aware of these aims of the study, but we presumed these groups and other non-scientific stakeholders would likely not be interested in our scale’s psychometric results. Therefore, we altered our dissemination focus and rethought our findings from the perspective of these stakeholders to present our most interesting and useful results for discussion at the dissemination event.
End users
Dissemination methods and results by end user.

Dissemination partners.
Patient education materials to train cancer survivors to self-advocate are currently being developed and will be delivered to appropriate end users once the materials are finalised.
Dissemination partners
Given our diverse end users, we decided to streamline the dissemination process by having at least one event in August 2015 that we could invite study participants, recruitment site leaders and all interested stakeholders to attend. The University of Pittsburgh Clinical and Translational Science Institute (CTSI) was a major contributor, both as one of our most successful recruitment partners through their Research Participant Registry and as a source of funding for our dissemination process.
Communication
Since we had such a wide range of end users, we wanted the communication of our dissemination strategy to appeal to multiple groups. We communicated our dissemination event using paper and email brochures and included a description of the event emphasising that most of the time would be discussing the study results. We also included a brief two-page bulletin describing the study and highlighting our results. To encourage others who may be interested in the study and topic to attend, we asked all of our partners to share the invitation on their respective networks. Because our research study was national but our event was held locally, we invited interested parties to attend the dissemination event using video-conference and/or to privately share their thoughts about the study and ideas about potential next steps with the research team.
Evaluation
Immediately after the dissemination event, we asked attendees to complete an evaluation and offer additional suggestions to our research team. These forms were primarily a programmatic evaluation of the event and an additional opportunity for feedback; we did not originally intend to design these forms as qualitative questionnaires for research purposes. We also received feedback from other patients and stakeholders who were not able to attend the event, but who had received our bulletins and presentation slides.
Dissemination work plan
Based on the evaluation feedback we received at the dissemination event, our research team developed a work plan after highlighting ways in which we could integrate the results of the research study with the results from the dissemination event to inform our next steps in this programme of research regarding patient self-advocacy. The plan consisted of (1) creating patient education materials to train patients to self-advocate and (2) designing a patient-centred intervention also to train patients to self-advocate.
Table 2 describes the products and modes of dissemination for each end user along with the research team’s special considerations for each. This table demonstrates how the same products can be shared across end users.
Feedback
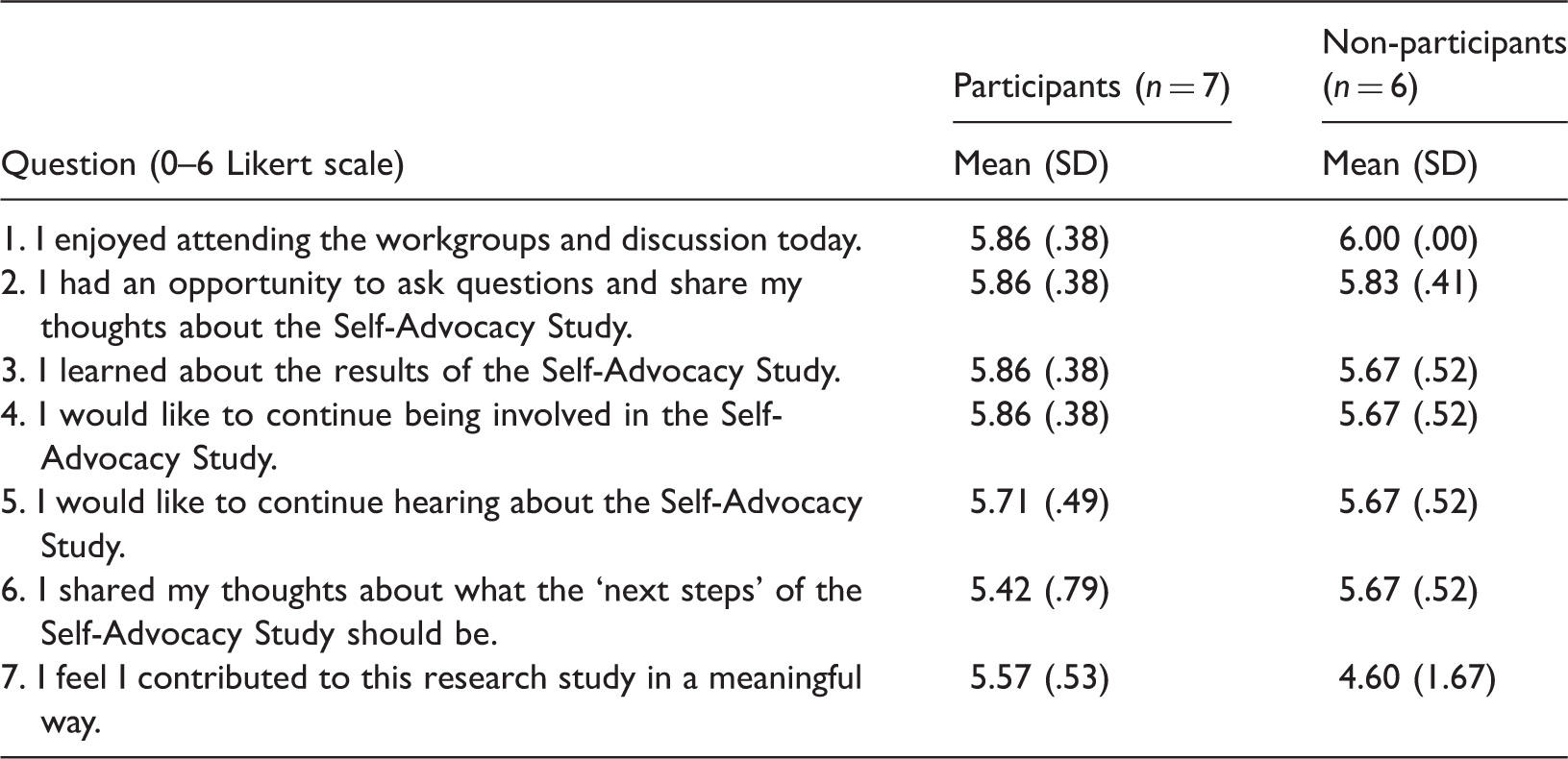
Evaluations from dissemination event.
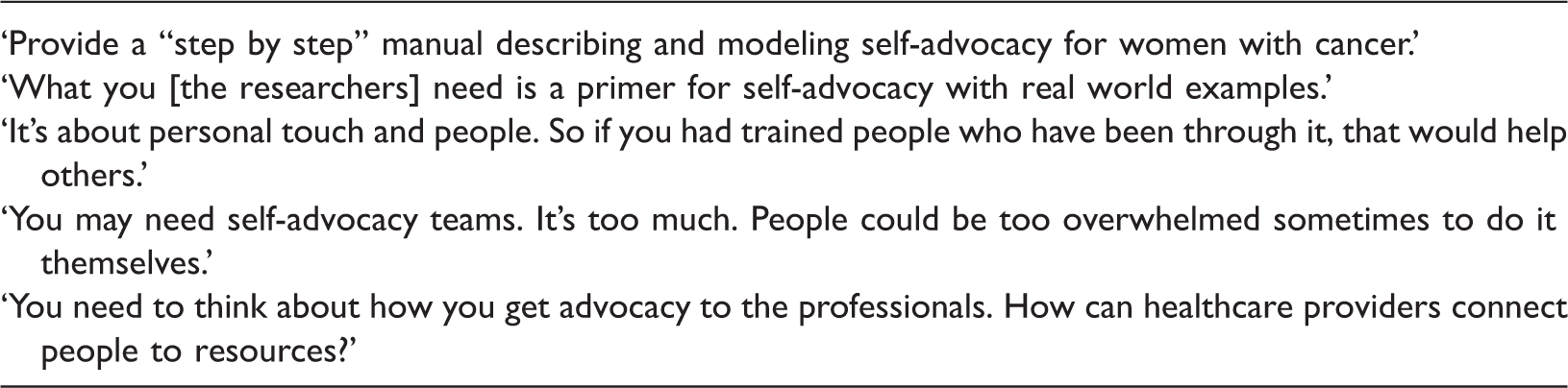
Advice from participants on how to support self-advocacy among women with cancer.
Development of patient education materials and planning for future research studies
The feedback we received during the dissemination event provided keen, direct guidance suggesting we develop patient education materials to help patients self-advocate. For example, attendees were adamant about the role of social support as foundational to women being able to advocate for themselves. Therefore, our patient education (and research interventions) must address how a woman can effectively use her available support systems. One attendee who was a study participant gave an exemplary metaphor when she described the interplay between self-advocacy and social support: ‘It’s like Uber – you are in charge of where you are going, but you don’t always have to drive.’ This metaphor is invaluable for our research team as we move our research into designing interventions. Based on what these stakeholders suggested for our self-advocacy patient education, we developed a website (www.empowercancerpatients.com) that will engage individuals with cancer in sharing their stories of self-advocacy, offer hints for others who are struggling to self-advocate, and show our results from previous studies regarding patient self-advocacy. We will continue to use this website to provide a space for individuals affected by cancer looking for connection and strength together.
Feedback from the dissemination event provided us with critical perspectives for our future research. Specific recommendations included the ideal timing and location of future interventions and specific types of information that would be appealing to women who struggle to self-advocate. One attendee urged us to design research with clear, explicit instructions: ‘What you [the researchers] need is a primer for self-advocacy with real world examples.’ Attendees also recommended having self-advocacy interventions include their healthcare providers and community resources outside of the hospital system. One woman described the difficulties of self-advocating with a rare cancer, and ended up informing other attendees about her type of cancer and the lack of available resources. Based on this feedback, we are currently designing and pilot testing a self-advocacy training intervention that uses common situations patients in our previous discussions have described in order to demonstrate how and when they can advocate for their needs and priorities.
Our study team learned several key lessons relevant to anyone attempting to organise a patient- and community-centred research dissemination event.
Practical concerns
Key challenges and lessons learned during our dissemination included the following:
Facilitators of our dissemination plan included:
Discussion
This simple, one-time dissemination strategy represents an alternative to only disseminating research for the scientific community. For non-researchers, involvement in a dissemination strategy like the one described in this paper provides a feedback mechanism via which to understand and critique research intended to benefit end users like themselves. For researchers, having patients and stakeholders interested and involved in one’s research offers several tangible benefits in addition to ensuring that the end users have received the results of the research.
Research participants want and expect trustworthy, timely information about the studies to which they consent to participate (Ondenge et al., 2015). As a cross-sectional survey study, the Self-Advocacy Study offered a limited, inflexible platform for sharing ideas and concerns. Therefore, our participants and stakeholders appreciated the outlet that the dissemination event provided to raise concerns or offer suggestions about how to improve the lives of women with cancer. We received positive feedback from attendees, indicating their appreciation for being included in the research endeavour and enjoyment of the event. We recommend other research groups use the AHRQ dissemination planning tool to methodically consider their dissemination process and how this process can be used to spur inventive, patient- and community-stakeholder-centred projects. If robustly designed, such dissemination events can succeed at both improving patient engagement and making research more relevant to all stakeholders (Domecq et al., 2014).
Innovative partnerships between academia and community stakeholders have demonstrated the creative potential of having multiple perspectives and talents brought together (Roy et al., 2014). By viewing research as a sustained programme rather than punctuated episodes, such partners can provide tangible resources (e.g. space, staff, volunteers and connections) and dedicated attentiveness (e.g. future collaborations) unmatched within the constraints of academia. Our partners during the Self-Advocacy Study assisted in organising this dissemination event and actively discussed future research priorities. We will continue to nurture these partnerships for the purpose of collectively working to benefit this patient population.
Above all, dissemination processes can build trust among researchers, patients and community stakeholders. In an era with growing public scrutiny of the research process (Gauchat, 2012), such partnerships are critical. By ensuring all parties understand the others’ priorities and activities, a more unified effort can be orchestrated to address critical healthcare problems (Gradinger et al., 2013). This may lead to sustainable academic–community partnerships that can facilitate a healthy, ongoing collaboration of developing shared research questions, scientific investigations and result dissemination (Carney et al., 2011). Even though our dissemination event was limited in time and space, it convened a group of stakeholders together to succinctly and efficiently provide study results and request stakeholder input.
Limitations to this study include the low participant turn-out rate among research participants and the low response rate for evaluation forms among attendees of the dissemination event. While we spent considerable time working with study participants and recruitment sites advertising the event and addressing possible obstacles to attendance (e.g. having the event webcast, offering lunch, validating parking, etc.), we were limited by the availability of study participants (recruited from around the country) to hold the event at a time and location that may not have been convenient for all individuals, especially those who had ongoing health issues. Finding creative ways to involve individuals with health limitations and limited travel abilities will ensure all stakeholders are able to contribute during these dissemination events. Moreover, our research assistants attempted to collect evaluation forms from each attendee, but many attendees left the event prior to the research assistant being able to remind attendees to complete the form. In future studies, we would suggest holding multiple events at times and locations that are not cumbersome to the patient population being served. We would also conduct a formal pre-post study to evaluate specific aspects of the dissemination event that impacted stakeholders.
Conclusion
Publication of research findings within scientific journals is adequate but not innovative. Finding novel ways to share findings can serve the interests of researchers, academics and participants. While we do not believe that our dissemination of the Self-Advocacy Study was overly elaborate, the method by which we approached and conducted our dissemination can be used by other researchers and community stakeholders interested in making mutually beneficial research partnerships.
Key points for policy, practice and/or research
Dissemination of study results can mutually benefit the patient and community stakeholders as well as investigators of research studies. Applying frameworks of research dissemination can assist researchers in developing a strategic, community-based approach to sharing study results and generating imaginative, patient-focused approaches to advancing scientific discovery. Building collaborations with community stakeholders through honest, open dissemination of study results and discussions of future research steps establishes trust between the lay and scientific communities. Creative means of sharing and building research programmes can stimulate novel forms of patient education, approaches to intervention research and forms of stakeholder involvement in research.
Footnotes
Acknowledgements
The authors would be remiss not to acknowledge the tremendous support received from the University of Pittsburgh’s Clinical and Translational Science Institute who advised the researchers throughout every stage of this project. The community stakeholders were essential to this study as well, including the Urban League of Greater Pittsburgh, the Cancer Caring Center, Our Clubhouse, the LiveWell programme at the University of Pittsburgh Cancer Institute, the African American Women’s Speakers Bureau and the National Ovarian Cancer Coalition of Pittsburgh. Above all, the patients and cancer survivors who participated in this study and offered their voices continue to demonstrate to us how best we can make our voices heard.
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by NIH/NINR (grant number F31NR014066) and the University of Pittsburgh Clinical and Translational Science Institute (grant number UL1TR000005).