
Abstract
Background
Nurses' knowledge of central venous catheter-related infection (CVC-RI) prevention guidelines is poor, indicating that nurses do not receive proper education about these guidelines.
Aim
The aim of this study was to evaluate the effectiveness of an educational course that aimed to improve nurses' knowledge about CVC-RI prevention guidelines.
Method
A sample of 131 nurses were randomly assigned to the experimental group (received an educational course) or control group (received no education). Pre-Post data were collected using a structured questionnaire that included a 23-item knowledge assessment.
Results
In the pre-test, all participants demonstrated poor knowledge, with mean scores of 8.2 (standard deviation = 3.6). After completion of the course, knowledge was significantly improved in the experimental group, whereas the control group showed no change (t(106,3) = 25.1, p = 0.00).
Conclusions
An educational course on CVC-RI prevention guidelines had an encouraging effect. Decision makers are recommended to implement such courses in their settings to improve nurses' competency.
Keywords
Introduction
The central venous catheter is an advanced intravenous infusion device (Cicolini et al., 2014) used for administering intravenous fluid, blood (Rogers et al., 2016), medication (Luckianow et al., 2016) and total parenteral nutrition (Cuerda et al., 2016), and to monitor central venous pressure (Jackson et al., 2016; Wilson, 2015). As an invasive device, the central venous catheter predisposes patients to a variety of complications such as thrombosis (Luckianow et al., 2016), embolism formation (Ferdous et al., 2015) and infection (Galy et al., 2016; Parienti et al., 2015).
Central venous catheter-related infection (CVC-RI) is bacteraemia secondary to the presence of a central venous catheter (Gahlot et al., 2014). It is a common complication associated with an increase in the cost of care (Harron et al., 2016; Shah et al., 2016), an extended hospital stay and increased mortality. CVC-RI causes 250,000 deaths per year in the United States (Brunelli et al., 2016) and increases the cost of care by US$33,000 (Harron, 2016), and hospital stay is increased by up to 3 weeks as a result of CVC-RI (Harron et al., 2016). Prevention is imperative in order to save money and prevent mortality. In Jordan, very few studies have investigated CVC-RI although one study reported an increase in the rate of CVC-RI in comparison with other countries (Al-Rawajfah et al., 2013).
The Centers for Disease Control and Prevention has published CVC-RI prevention guidelines that help to reduce the rate of CVC-RI and related complications (El Nemr et al., 2015; Ista et al., 2016). Major topics in these guidelines include education of healthcare providers, antisepsis, intravenous administration management, hand hygiene and dressing (Ling et al., 2016; Septimus and Moody, 2016).
Although the effectiveness of CVC-RI prevention guidelines was supported by the literature, studies reported that intensive care unit (ICU) nurses’ knowledge of these guidelines was still questionable (Cicolini et al., 2014; Labeau et al., 2009). Teaching nurses about CVC-RI prevention guidelines is essential in order to improve their competency and enhance quality of care, which in turn will help to prevent the occurrence of CVC-RI, cut the cost of related complications and improve treatment outcomes. Thus the purpose of this study was to evaluate the effectiveness of the CVC-RI prevention guidelines educational course presented to ICU nurses in Jordanian hospitals.
Method
Design
This study was a randomised controlled trial. Nurses were randomly assigned to either the experimental or the control group. Nurses in both groups completed pre-test and post-test questionnaires. Those in the experimental group underwent an educational course on CVC-RI prevention, whereas the control group did not.
Sample size estimation and randomisation scheme
The G*Power 3.1 (Erdfelder et al., 1996) software was used to calculate the required sample size. Based on a power of 0.8, a medium effect size of 0.5 and a significance level of 0.05, the required sample size needed to run a two-group independent-samples test was 128 participants, 64 in each group. In this study, we recruited a sample of 136 participants to compensate for the expected drop-out rate. The Research Randomizer® random number generator (Urbaniak and Plous, 2013) was used to perform randomisation. This software was available free online. The software generated two sets of 68 numbers. There were no statistically significant differences in the baseline characteristics (e.g. age, gender and years of experience) of the two groups.
Study setting and participants
The study was conducted at 10 Jordanian hospitals of different affiliations. Four hospitals were governmental, two were educational and four were private. All hospitals were located in urban areas. The ICUs within these hospitals were mostly medical surgical units with an average capacity of 10 beds. All of the participating hospitals had continuous education and infection control departments. Registered nurses, working in an ICU and having at least 1 year of experience, were considered eligible participants.
Instrument
A questionnaire was developed based on the CVC-RI prevention guidelines from the Centers for Disease Control and Prevention (O’Grady et al., 2011). The questionnaire has two parts: part 1, in which biographical details (age, gender, previous CVC-RI education and the source of that education, and years of experience) were requested; and part 2, a multiple-choice exam consisting of 23 questions. Each of these questions had four options: one correct answer, two distractors, and an ‘I don’t know’ choice. Each correct response was worth one mark, with no credit for the other responses. The instrument was evaluated for clarity, understandability, internal consistency reliability and content validity by a panel of three infection control specialists. It showed very good internal consistency reliability, with Cronbach’s alpha of 0.82. Some items were reworded on the recommendation of the panel.
Ethical permission
The study was approved by the IRB in the participating hospitals provided ethical overview and permission to access the sample. Nurses were instructed that their completion of the study questionnaire would be considered as consent to participate. They were informed that there was no direct benefit from participation in the study, although their participation would help to push science forward. Participants were allowed to withdraw from the study at any time with no penalties. Confidentiality was maintained throughout the whole study. A master code list was created that included the participants’ names and codes to match the results of the pre- and post-tests. All materials related to the study were kept in the principal investigator’s personal office with restricted access. All documents and data were discarded appropriately at the end of the study.
Data collection
The study was advertised in the participating hospitals. Nurses interested in participating registered in a registration office in each of the hospitals. Of 200 ICU nurses working in the participating hospitals, only 136 nurses agreed to participate, giving a response rate of 68%. Those who declined to participate were of different genders and educational levels. Nurses were assigned to either the experimental group (68 nurses) or the control group (68 nurses) using computer software. Three nurses from the experimental group and two from the control group withdrew, giving a final number of 131 nurses: 65 in the experimental group and 66 in the control group. On the first day of the study, a pre-test questionnaire was given to the nurses by the principal investigator. The post-test was administered to all participants after completion of the educational programme. Data collection took 2 months, from October to December 2016.
The CVC-RI prevention educational course took place in the continuous education facility in one of the participating hospitals. The course comprised 3 lecture sessions of 3 hours each. All sessions were prepared and delivered by the principal investigator. The first covered central venous catheter types, indications, insertion, complications and nurses’ role in the prevention of complications. In the second and third sessions, presentations about the updated guidelines for prevention of CVC-RI were given. The teaching strategies included video recordings, classroom presentation and class discussion.
Data analysis
SPSS version 21 was used for data analysis (IBM, 2012). Descriptive statistics were used to calculate the frequency of correct answers and the mean scores. An independent-sample t-test was used to test the difference in knowledge scores between the experimental and control groups. A paired-sample t-test was used to evaluate the change in knowledge scores from the pre-test to the post-test. The variable years of experience was categorised to ≥5 years and <5 years, and an independent-sample t-test was conducted again to find the difference in post-test scores with respect to baseline characteristics.
Results
Frequencies of correct answers in the pre-test and post-test (N = 131).
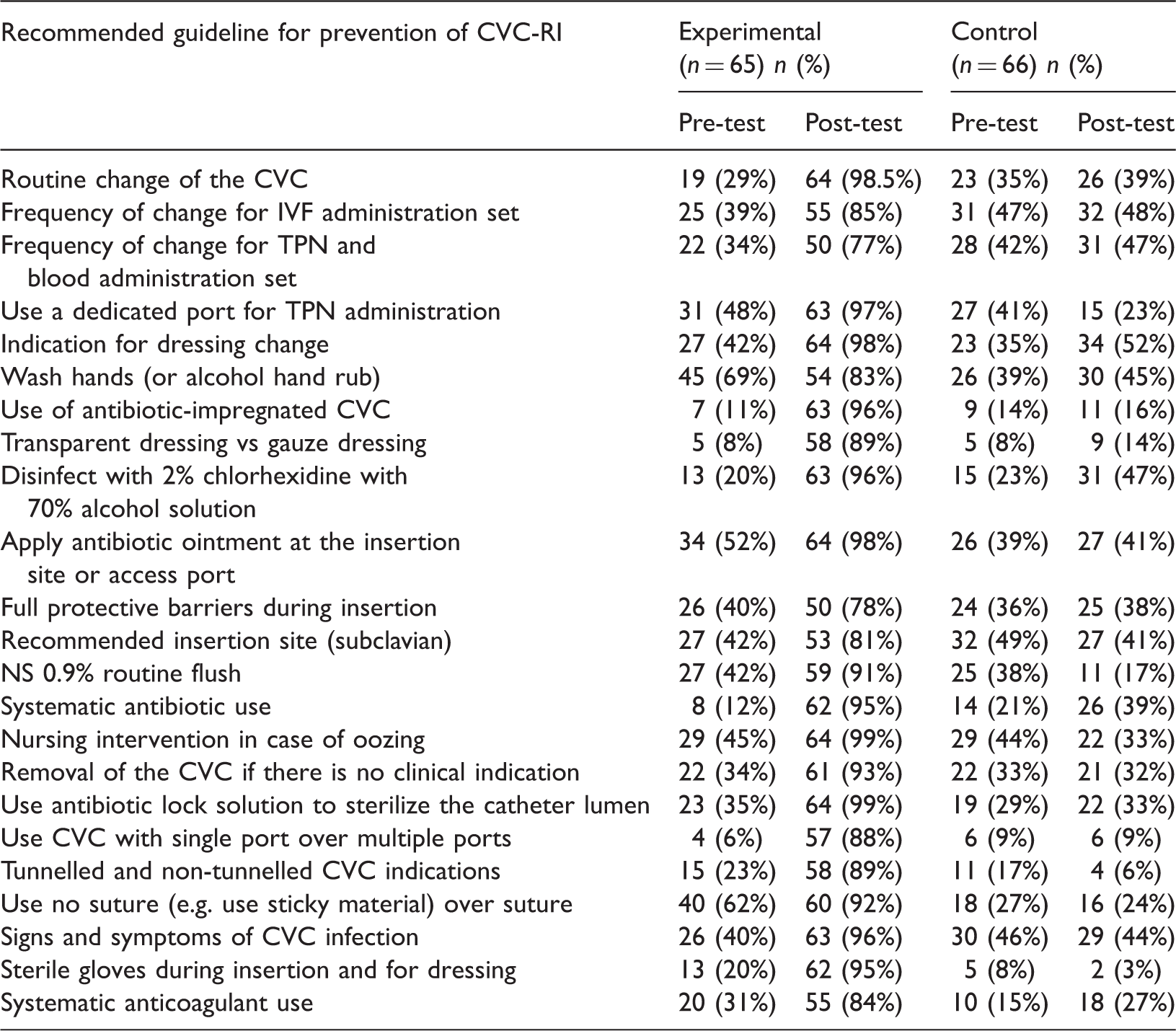
CVC: central venous catheter; TPN: total parenteral nutrition, CVC-RI: central venous catheter-related infection; IVF: intravenous fluid; NS 0.9%: normal saline.
Results of the pre-post-test knowledge scores.
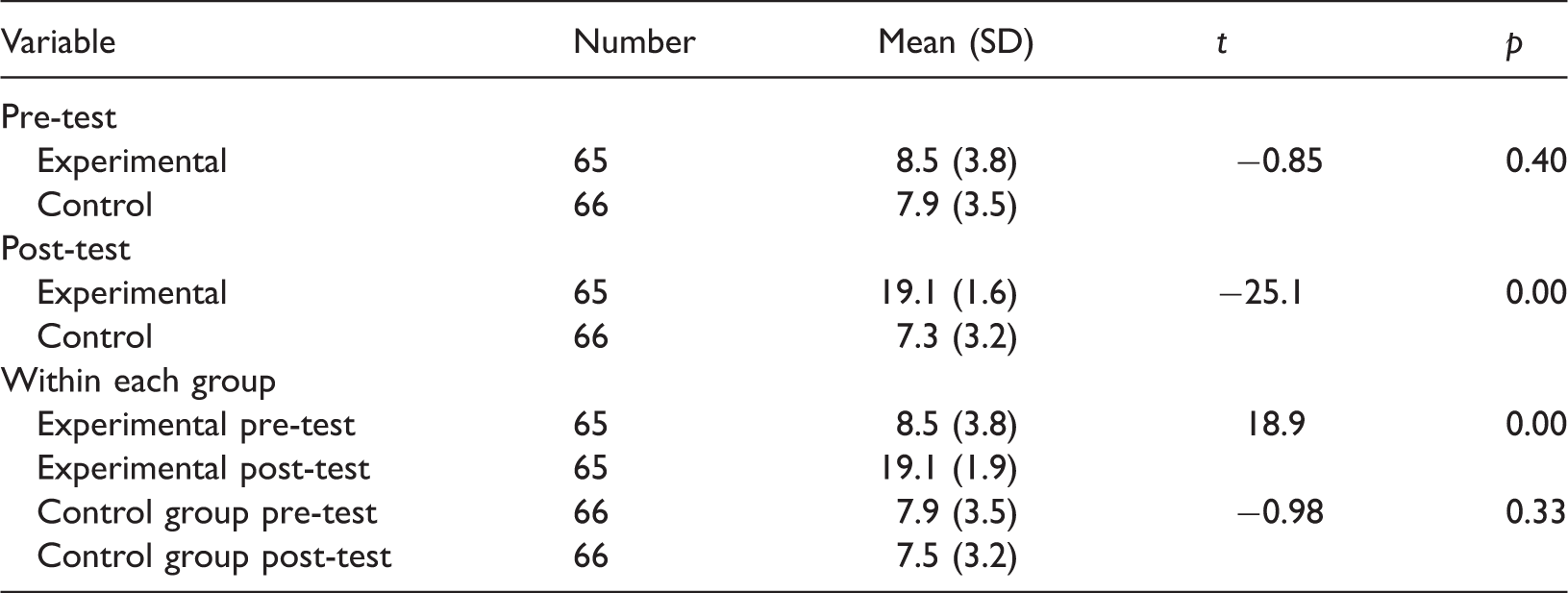
Within the control group, the participants with experience of ≥5 years showed much better improvement in their knowledge scores in the post-test (M = 21.0, SD = 1.0) in comparison with their counterparts with less experience (M = 20.1, SD = 2.5); t(32) = −2.10, p = 0.04. There was no statistically significant difference according to gender; t(63) = −0.98, p = 0.33.
Discussion
This study was a randomised controlled trial that aimed to evaluate the effectiveness of a CVC-RI prevention guidelines educational course. Nurses were randomly assigned to an experimental group that received CVC-RI prevention guidelines education or a control group receiving no education. At the pre-test stage, a significant weakness in knowledge was observed in both groups; however, the experimental group demonstrated a significant improvement in their knowledge after completion of the educational programme.
The findings revealed that ICU nurses had insufficient knowledge about CVC-RI prevention guidelines. Significant weaknesses were noticed in topics related to the recommended antiseptic solution, the use of a single-port central venous catheter over the multiple port, the use of a tunnelled versus a non-tunnelled catheter, sutureless versus suture securing, and the type of dressing material (Table 1). These findings support those of previous studies that revealed inadequate knowledge about CVC-RI prevention guidelines (Al Qadire, 2017). Although some of the nurses reported having been taught about the central venous catheter prior to the study, the majority showed poor knowledge. The reasons for this might include defects in the quality of education at the undergraduate level and a lack of post-registration education and training in hospitals. In one study, student nurses reported dissatisfaction with their infection control courses (Al-Hussami and Darawad, 2013). In two other studies, students reported some difficulties in the clinical settings that prevented learning (Harrison, 2004) and a need for non-traditional strategies to enhance their learning (Cardoso et al., 2012). Another reason for nurses’ poor knowledge might be lack of education and training within the participating hospitals. In one study, Al Qadire et al. (2017) reported that student nurses did not receive proper education and training on CVC-RI prevention, which affected their competency and compliance in the future.
The educational course in this study was successful in expanding nurses’ knowledge of CVC-RI prevention guidelines. This finding is consistent with those of many other studies that indicated the benefits of such courses in the improvement of nurses’ knowledge (Hina and McDowell, 2017; O’Neil et al., 2016). It is also congruent with the recommendations of the Centers for Disease Control and Prevention and the American Thoracic Society for continuing education and training as a basic element in CVC-RI prevention (Labeau et al., 2009; O'Neil et al., 2016).
Limitations
The current study has some limitations. Although the educational programme integrated different teaching strategies, it lacked clinical training for CVC-RI prevention guidelines. Replication of the study with clinical training is recommended in the future. Moreover, the study included only Jordanian nurses, which may limit the generalisability of findings. Future studies are recommended to include nurses of different nationalities. Finally, this study did not measure the compliance of nurses. Future studies are recommended to observe nurses during patient care in order to investigate the effect of education on compliance.
Conclusion
This study sheds light on a critical issue related to the nursing profession. Nurses showed insufficient knowledge about CVC-RI prevention guidelines; however, significant improvement was achieved through an educational course. This finding raises a red flag about the quality of education at the undergraduate level, and of postgraduate education and training. Findings from this study can be used by nursing educators and health professionals to guide their clinical practice and advance the quality of care.
Key points for policy, practice and/or research
This study provided evidence of the need to educate nurses in the critical care settings with CVC-RI prevention guidelines to prevent complications that are associated with insertion and manipulation of the central venous catheter and to improve the quality of care. Postgraduate education and training is imperative in order to improve nurses' knowledge and competence. Nursing curricula, especially at the undergraduate level, need revision and refinement. Integration of CVC-RI educational content and training is critical to improve students' knowledge and would have a significant effect on their future competence.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics
Ethical permission was obtained from the IRB in Al Albayt University, Mafraq Jordan (reference number 3/2016/2017, in 25/1/2017) and from the participating hospitals.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was funded by Al albayt University/Mafraq/Jordan).