
Abstract
Background
Physical and psychological concerns associated with a breast cancer diagnosis continue long after treatment. Macmillan Cancer Support developed an electronic Holistic Needs Assessment (eHNA) to help identify these concerns and allow a healthcare professional to address these as part of The Recovery Package.
Aims
The study aim was to understand the women’s experiences of having breast cancer, and of completing Macmillan’s eHNA as part of their care.
Methods
A qualitative approach was adopted. Semi-structured interviews were undertaken with 15 women, 12–18 months following surgical treatment for invasive breast cancer. Thematic analysis identified key themes.
Results
Four main themes were identified in relation to experiences of the eHNA, experiences of breast cancer, coping with breast cancer and the psychological effects of surviving. Perceptions towards the eHNA varied; some women viewed the eHNA as a research tool for hospital use rather than a beneficial aspect of their care. Several participants felt unable to raise their psychological concerns on the eHNA.
Conclusions
Although experiences differ, psychological issues remain a key factor for women with breast cancer, lasting long after treatment. The eHNA is not currently used to its potential or recognised by women as a tool to support their care. Further research is needed into how the eHNA can be used effectively to capture psychological concerns and determine best approaches to implementation of the tool to support individualised care.
Introduction
Breast cancer is the most common cancer found in females worldwide (World Health Organization, 2017). However, campaigns towards early detection and screening mean that survival rates are increasing, with 86% now surviving beyond 5 years (Cancer Research UK, 2014). It is estimated that there are 691,000 individuals living with or beyond breast cancer in the UK alone (Breast Cancer Care, 2017a).
Despite the prevalence and high survival rates associated with breast cancer, returning to life routines following treatment can be difficult, and a focus has therefore been placed on supporting women in adjusting to a ‘new normal’ (National Cancer Institute, 2014). The rapid diagnosis process begins with numerous tests, followed by treatments within weeks, which can include chemotherapy, radiotherapy and surgery that may drastically alter body image (Falk Dahl et al., 2010). Following this, the individual may be disease free, but can continue to suffer from long-term physical and psychological effects, including persistent breast pain, lymphoedema and fear of recurrence (Ewertz and Jensen, 2011; Ganz et al., 2011). As a result, there is increasing emphasis on supporting cancer survivors in developing coping strategies aimed at improving their quality of life (Kim et al., 2010).
The issue of supporting those living with and beyond cancer received national recognition initially through the development of the National Cancer Survivorship Initiative (NCSI), and the subsequent Cancer Strategy for England 2015–2020 (Independent Cancer Taskforce, 2015). The Cancer Strategy includes a recommendation that ‘The Recovery Package’ is offered to every individual living with or beyond cancer. The package incorporates a series of supportive interventions to provide support to each individual through their cancer pathway, including Holistic Needs Assessment (HNA) and care planning, Treatment Summary, Cancer Care Review and a Health and Wellbeing Event (NCSI, 2013). It has been reported that use of The Recovery Package has a direct impact on nursing practice through the potential for reductions in service demand and promoting a culture of holistic, well-integrated care (Macmillan Cancer Support, 2017). Similarly, the National Health Service (NHS) Five Year Forward View emphasised the importance of promoting integrated care, to facilitate more effective and personalised care processes (NHS, 2014).
HNA and care planning has been described as ‘the heart’ of The Recovery Package, promoting self-management among patients and providing a clearer pathway for healthcare professionals to plan care (Doyle and Henry, 2014). HNAs are assessment tools listing numerous physical, emotional, social and other concerns that an individual living with or beyond cancer may face. The tool allows the individual to rate their concerns for severity, and an adjoining care plan is created together with a healthcare professional to allow the concerns to be addressed through actions such as giving advice and referral on to additional services, or signposting (Macmillan Cancer Support, 2017). Although there are various forms of HNA in use, for example ‘Distress Thermometer’ (National Comprehensive Cancer Network (NCCN), 2016) and ‘Sheffield Profile for Assessment and Referral to Care (SPARC)’ (Bradford District NHS Care Trust, 2013), the HNA tool referred to in the current study was Macmillan’s electronic version of the HNA (eHNA). This is completed on an electronic tablet, and was selected since it has been widely piloted and adopted in the UK and its unique approach of utilising technology allows data to be compared electronically and stored in a way that is easily accessible (Macmillan Cancer Support, 2017). The eHNA tool is used to identify concerns in domains of physical, psychological, social, spiritual and practical issues, and results in completion of a corresponding care plan (Macmillan Cancer Support, 2017).
The eHNA has significant potential to play a key role in promoting self-management to those living with or beyond cancer, and this is beneficial to the individuals, nursing staff and healthcare services more generally through reduction in budgetary issues, staffing issues and service demand (The Health Foundation, 2011). These benefits may be obtained through using an individualised approach and offering follow-up to those who need it, which may in turn reduce hospital readmissions and free up resources through self-management and increased productivity – which is a significant proportion of expenditure on the NHS cancer budget to date (NCSI, 2013). However, there has been minimal research conducted into patient experiences of the tool and there is limited understanding as to its role in assisting with the recognition of, and response to, patient concerns.
Aims
The study aimed to discuss and gain an understanding of participants’ experiences of completing Macmillan’s eHNA as part of their routine aftercare.
A further aim was to understand participants’ experiences of having breast cancer, through diagnosis, treatment and in the period beyond this.
Methods
Ethical approval
Approval was obtained from the NHS Research Ethics Committee (REC) (Reference 17/EM/0046, 24/02/2017) and the Health Research Authority (HRA) (10/03/2017). Local governance approvals were sought from Research and Innovation (R&I) (Reference 17ON008, 10/04/2017) at the NHS Trust from which participants were recruited. Written and verbal consent were taken from all participants. All procedures performed in studies involving human participants were conducted in accordance with the ethical standards of the institution and the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Sampling and recruitment
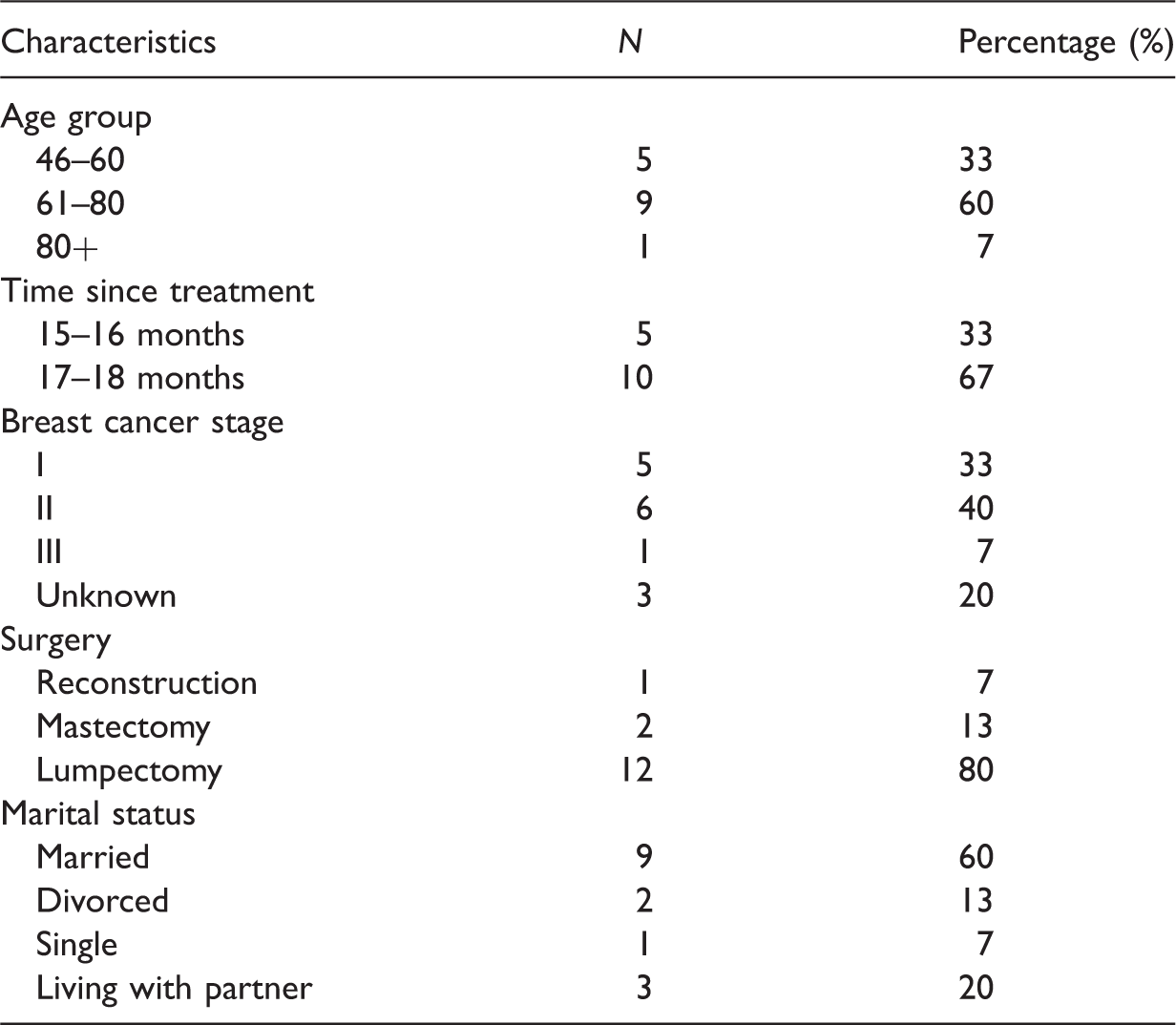
Women treated surgically for invasive breast cancer 12–18 months previously were recruited using purposive sampling from the 1-year post-treatment follow-up clinic appointment lists at a single UK NHS Trust. Eligibility criteria included those aged 18+ and were not restricted regarding stage of breast cancer or type of surgery. Those with known metastatic cancer or ductal carcinoma in situ (DCIS) or who were receiving conservative treatment were not eligible to participate, nor were those with severe cognitive impairments from whom it would have been difficult to obtain informed consent. Letters containing information about the study were sent by the usual care provider to 42 eligible women. Of these, 22 expressed interest in the study, and the first 15 were invited to interview. The remaining 7 were contacted to inform them the study was full and were thanked for their interest. There are no set recommendations for sample size in qualitative research; however, sizes of 6–12, 5–25 and 12–20 have been suggested in previous research (Baker and Edwards, 2012; Guest et al., 2006). Maximum sample size for the study was also restricted by study-time constraints and ethical approvals.
Participant details.
Data collection
A qualitative approach was adopted, and data were collected through semi-structured interviews. Participants were offered the choice to be interviewed either in their homes or in hospital. Eight (54%) opted for home and seven (46%) opted for the hospital. The hospital venue was a private consultation room at the same venue where patients received their diagnosis and post-treatment follow-up appointments. Data collection took place between May 2017 and June 2017, and interviews ranged in length from 25 minutes to 1 hour 11 minutes (mean = 42.5 min, SD = 15.37). All interviews were digitally recorded with consent and transcribed for use in analysis. The interview guide contained 14 questions targeting different time points in their cancer journeys to provide an overview of their story from diagnosis through to the present day, and their experience and opinions of the eHNA.
Data analysis
The concepts of thematic analysis were adopted to analyse the data, due to flexibility of the approach and its widespread use in health research (Braun and Clarke, 2014). The advantages of this method include its simplicity and freedom from a specific philosophical position (Braun and Clarke, 2006). However, Braun and Clarke (2006) also highlight limitations of this flexibility and simplicity, such as this not providing the ability to make claims about factors such as language use when drawing conclusions. Transcripts were initially read several times in order to become immersed in the data, then codes were assigned to each line of transcript, which were later sorted into themes and subthemes. NVivo 11 software was utilised for the process of managing and coding data.
Results
Themes and subthemes.
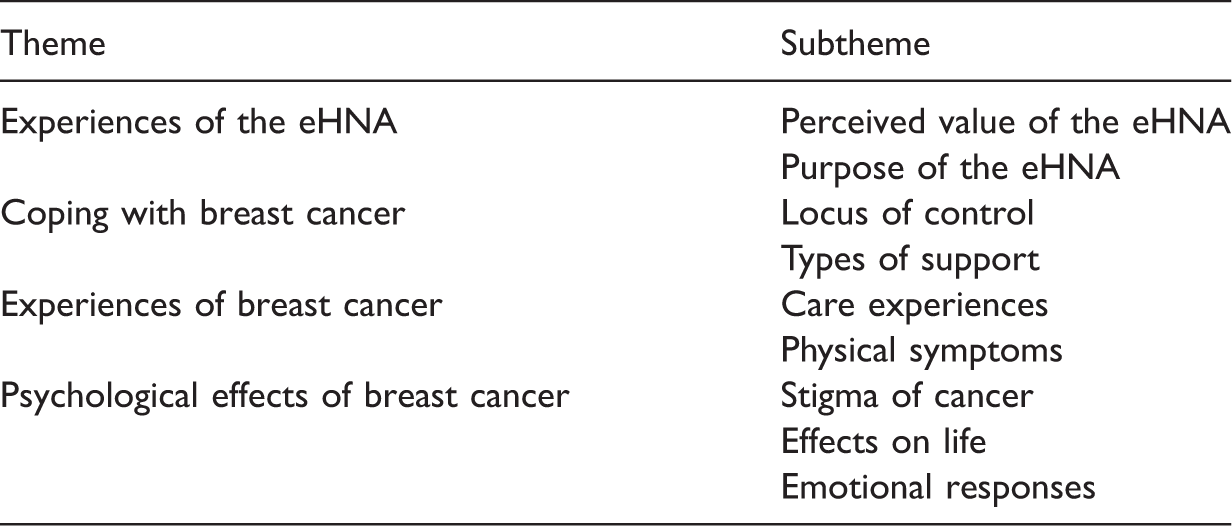
Theme 1: Experiences of the eHNA
The eHNA had been completed by all participants (self-reported and verified by the usual care provider). However, three women could not recall completing it, and therefore their opinions could not be included.
Perceived value of the eHNA
Opinions of the value of the eHNA varied between participants, with two stating that they found the eHNA helpful and several others feeling as though it was not useful to them: In my case I thought it was a waste of time. (Participant 13) I didn’t find it helpful at all to be honest. (Participant 3) So I suppose … maybe just felt like add on … it’s just something that you need to do … so whether or how meaningful it was I don’t know. (Participant 11) I would say, just before perhaps you go for your mammogram … that’s the time when people are thinking about things a little bit more and it’s a bit fresher in your mind. (Participant 6) We’d only paid for so much parking as well, so my head was like … we’re gonna get fined. (Participant 3) There was no pressure to do it, but when you’re in hospital and you’ve got a nurse with you, you’re taking their time up and they could be doing other things. (Participant 6) He doesn’t want me going in there saying I’m fearful for the future, I’m worried about my children, I’m worried about moving house … I mean what could he do really?. (Participant 1) Maybe a part of you also is almost like … well if I put all of this … will they call me back in?. (Participant 11) You can cope with sadness and loneliness … but you can’t cope with pain if there’s something there, that’s why I put the pain down. (Participant 14)
Purpose of the eHNA
Perceptions of the purpose of completing the assessment were explored. Several participants viewed this assessment as being solely for the benefit of the hospital, as opposed to it being a tool to help patients: It was never portrayed to me to be a tool to help me. (Participant 4) I thought it was for research … I didn’t think it was for me particularly. (Participant 12) You feel as if it’s for someone else and not for. (Participant 6)
Theme 2: Coping with breast cancer
Locus of control
Most participants indicated an acceptance of their breast cancer diagnosis. Their acceptance sometimes aligned with a view that superstition had played a part in both their survival and being diagnosed in the first place: It’s the guilt, yeah, because you just think well I’m lucky, there are people who are gonna be there who aren’t so lucky, let them have the time. (Participant 6) Sometimes I think, did I sort of cheat something … is something gonna come along?. (Participant 11) I think it through in my head … and at the end of the day come to the conclusion that if it does come back … there’s nothing I can control. (Participant 3).
Types of support
A final subtheme within coping was the type of support received. Participants referred to support from experts and healthcare professionals, family and peers, religion, organised support groups and other patients who had survived cancer: Everything I wanted to know was there, and I know that nurse I could ask anytime, I could ring her, that special nurse I had. (Participant 12) You’re not ever gonna see them ever again … and you can confide, because you know that they will completely perhaps understand what you’re saying cause you’re going through it, whereas friends and relatives that haven’t been through that, perhaps don’t understand your … your emotions and your thinking. (Participant 6) I mean my husband was there all the time so … he was just a brick basically. (Participant 15)
Theme 3: Experiences of breast cancer
Care experiences
Overall, participants were extremely positive about the care they received through diagnosis, treatment and subsequent follow-up appointments. However, there was a focus placed on the need for individualisation: I just wanted somebody to look at me as a person, and listen to me. (Participant 14) Somebody just to sit down with you and just explain, and just be nice about it … they're just so cold. (Participant 10)
Physical symptoms
Each participant discussed the physical symptoms they had experienced and appeared to be more forthcoming in divulging this information than when discussing the emotional aspects of cancer diagnosis and care. The physical symptoms presenting post-treatment varied in their degree of severity and at what stage in their cancer journey these were an issue, with some participants still frequently experiencing these 1-year post-treatment. Common issues included breast pain, hot flushes, generalised aches and pains, fatigue and sleep disturbances. Additionally, these physical symptoms often caused participants to worry about the origin of their symptoms, since the cause was unknown to them: I think it worries everybody doesn’t it … you think every little ache and pain you’ve got, oh what’s that … is it bone cancer?. (Participant 8).
Theme 4: Psychological effects of breast cancer
Stigma of cancer
Analysis of the interviews demonstrated that participants perceived a certain level of stigma in having a diagnosis of ‘cancer’: I don’t know whether it’s because he was frightened of the word cancer as well. (Participant 14) I think you notice more how many people are dying with cancer, everything seems to be people dying with cancer. (Participant 3).
Effects on life
It was reported by participants that surviving breast cancer had impacted on their lives in various ways, including changes in their perspective and behaviour: I think you realise that so many years you’ve been saying, oh I can’t wait for the kids to grow, can’t wait to retire … and we’re not enjoying the moment. (Participant 6). I think it’s a lot of grief and loss … friends and family expect you to be the same person … and you’re not. (Participant 7) I mean apart from going to bed early … I wouldn’t say much had changed. (Participant 2) It didn’t interfere, not with anything. (Participant 12)
Emotional responses
Several negative emotions were evident in this sample. These included anger, fear, denial, body image issues, embarrassment, guilt and isolation, although fear was the most commonly reported concern: You don’t know whether it’s gone anywhere else … throughout the whole period, your mind is your worst enemy. (Participant 6) It feels like you’ve gone through a war and you’re left with the battle scars, and you’re just stood in that field and you’re the only one alive. (Participant 7) As far as the cancer, that was done and dusted when it was done, you know … but no, no, I don’t go to bed at night and think oh has it come back, nothing like that. (Participant 9)
Alternatively, some participants commented on their positive emotional responses. For example, all women indicated a desire to move forward with their lives and referred to their ability to remain positive: I’m always quite a positive person and I look forward rather than back. (Participant 4) I didn’t want pity, I didn’t want sympathy, I was getting myself right, and I wanted to carry on looking on the positive side of it. (Participant 14)
Discussion
With regard to participant experiences of the eHNA, this study showed that distress was sometimes not reported by participants at the time of completion. This lack of reporting was due to fear of repercussions, or a concern that healthcare professionals were too busy, or women perceived that they would be unable to deal with the issues raised. This is comparable to findings of a prior study evaluating patient experiences of the ‘distress thermometer’ – an alternative form of HNA (Biddle et al., 2016). Although some women have very few concerns to report, others find it easier to talk about physical issues than psychological concerns. Raising psychological issues may be associated with perceived stigma related to having mental health conditions, and this has previously been found to deter patients from discussing psychological issues (Lynch et al., 2011; Rose et al., 2018). Furthermore, it is possible that the absence of a pre-existing relationship between clinician and patient may cause patients to feel less relaxed and result in staff feeling unable to probe for personal information (Biddle et al., 2016; Gamlen and Arber, 2013). Some participants did not understand the purpose of the eHNA or did not feel that it added value to their experience. Although no other research into this topic appears to have considered patient understanding of the purpose of the eHNA, this research challenges the findings of other studies, in which patients have indicated positive value in having completed the assessment (Ipsos MORI, 2015; Kuczkowska et al., 2015). This is likely to be related to the way in which the eHNA was introduced in the encounter or may perhaps be influenced by some of the additional barriers around the environment, such as patients’ perception of their appointment being time-pressured, or their view that it was being completed at the wrong time in their pathway. These perceptions may engender women’s perceptions of the tool being a tick-box exercise. This view is supported by Snowden et al. (2012), who found that the process of delivering HNA is likely to be unsuccessful if the initial impressions patients have of it are negative.
Coping strategies among survivors of cancer have previously been found to include distractions, acceptance, emotional support and religious support (Deimling et al., 2006; Lauver et al., 2007). Psychological wellbeing of cancer survivors is particularly important, since in our study, participants frequently used acceptance and emotional support to cope, whereas religion and denial were reported less frequently.
Overall, all of the women in this study reported being happy with the care they received. Nevertheless, lack of individualisation in care was highlighted as an important problem and a similar finding has been reported elsewhere (Suhonen et al., 2012); this perception of depersonalisation may affect patient experiences of the eHNA delivery. Similarly, a systematic review looking at cancer survivor care plans found that despite awareness of the need for individualisation among healthcare professionals, barriers such as lack of time make this difficult to achieve (Keesing et al., 2015).
With regard to the physical side effects of treatment noted by participants, the most commonly reported factors were fatigue, hot flushes, lymphoedema, breast pain, arm dysfunction and general aches and pains. This is comparable with prior research around the side effects of breast cancer treatment (Breast Cancer Care, 2017b; Fu and Rosedale, 2009; Levangie et al., 2011) and the reported side effects of hormone therapy drugs (Macmillan Cancer Support, 2016).
The psychological impacts of breast cancer are well established. Difficulty concentrating and body image have been identified as top concerns among those living with or beyond cancer (Lauver et al., 2007). Although none of the participants interviewed in the current study raised difficulty in concentrating as an issue, more than half of them reported concerns related to their body image, and all of the participants reported that they had experienced a fear of recurrence at some point during their treatment or beyond, which varied in its degree of severity. The after-effect of fear is commonly reported in the literature (Brennan et al., 2011). Risk factors for psychological distress in breast cancer patients include being younger, having limited access to social support and predisposing mental health conditions (Ganz, 2008). Although all of the participants in our study reported accessing some form of social support, the younger women tended to report more psychological effects following diagnosis and treatment than older participants. However, it is worth noting that several participants reported that there was very minimal disruption to their lives following cancer and stated that they had no issue readjusting and no lasting psychological effects. This is congruent with the published evidence, in which approximately one-third of patients have reported no distress at all in their first year following treatment (Henselmans et al., 2010).
Limitations
The study was conducted at a single site where the eHNA was offered 1-year post-treatment and so data may not reflect the views of those in other geographical locations. The interviews required participants to recall thoughts and feelings from up to 18 months ago, and as such, data may be subject to memory recall bias. Indeed, some participants found recall of the eHNA challenging or failed to recall completing it. This was a small, self-selected sample and it is possible that those who agreed to be interviewed were particularly positive in outlook – the views of women who did not take part in this study are unknown. The sample included only White British participants reporting good social support networks, and the views of other sociodemographic groups are not known.
A further consideration with this study is the potential impact of the researcher on the findings. Participants were aware of the researcher’s dual role of researcher and nurse. This could have influenced the information disclosed, and how women perceived the interview and how their responses would be interpreted. Every attempt was made to reduce this risk by informing participants prior to participation that the interviewer was there in a solely research capacity and that their participation or non-participation would not affect their clinical care in any way.
Conclusions
This study contributes to a limited but emerging evidence base around the experiences of the eHNA in women who are living with or beyond breast cancer. The overall aim of this research was to increase understanding of women’s experiences of the eHNA and provide insight into the experiences of those living with and beyond a breast cancer diagnosis.
The issues faced may continue long after treatment and subsequently affect quality of life from both a physical and psychological perspective. These findings enhance our understanding of the patient journey, and of women’s experiences of completing an essential element of The Recovery Package (eHNA), which contributes to the Cancer Strategy aims to improve cancer aftercare (Independent Cancer Taskforce, 2015). There is a need for increased individualisation in the care provided, and the provision of tailored support that aims to address women’s concerns holistically. There is a need for better communication between healthcare professionals and patients to ensure that the purpose and value of the eHNA is fully understood in order for this tool to be used to its maximum potential in individualised patient care.
Further research is needed around patients’ willingness to report psychological concerns, and how this communication might be better facilitated by nursing staff, in order that the benefits of the tool can be maximised. Obtaining a nurse’s perspective would be beneficial in understanding how the eHNA is delivered and implemented into routine practice and the factors affecting this. It would also be useful to ascertain the views of women with breast cancer who are being treated and undertaking the eHNA at different geographical locations, to ascertain any potential variations in care and implementation, and any potential impact of these on patient perceptions and outcomes.
Key points for policy, practice and/or research
Holistic care is an essential element of ensuring that those living with or beyond breast cancer feel well supported throughout their journey. There is a need for care to be individualised and patient centred. The way the eHNA is implemented in practice may influence the success and usefulness of this tool in identifying and addressing patient concerns. Research is needed to better understand patient communication around psychological concerns, and how the nurses can use HNA tools to better facilitate communication and care planning.
Footnotes
Acknowledgements
The authors would like to thank the participants who opted to take part in the study, and the Breast Care Nurses at the NHS Trust who facilitated the process of recruitment to the study. Lydia Briggs would additionally like to thank the NIHR for funding the MA qualification.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Approval was obtained from the NHS Research Ethics Committee (REC) (Reference 17/EM/0046, 24/02/2017) and the Health Research Authority (HRA) (10/03/2017). Local governance approvals were sought from Research and Innovation (R&I) (Reference 17ON008, 10/04/2017) at the NHS Trust from which participants were recruited. Written and verbal consent were taken from all participants. All procedures performed in studies involving human participants were conducted in accordance with the ethical standards of the institution and the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This project was undertaken as part of a Master’s in Research Methods, for which the Lydia Briggs was funded by the National Institute of Health Research (NIHR). The research itself received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.