
Abstract
Background
Nurses’ education of patients is important for building the knowledge and skills necessary for self-management. Little is known of newly registered nurses’ preparedness to deliver patient education, or of their experiences in clinical contexts where they may encounter barriers.
Aims
The aim of this study was to explore newly registered nurses’ patient education role in an acute hospital setting.
Methods
A purposive sample of seven newly registered nurses from an NHS teaching hospital in England were interviewed to explore their understanding and experiences of educating patients. An interpretive phenomenological approach was used to analyse responses.
Results
Three superordinate themes were identified: the professional self; the ward environment; and the nurse-patient relationship. Tensions existed between the ideals newly registered nurses brought to registered practice and the practice-based realities of patient education, which was often delivered informally with limited patient involvement in collaborative goal setting. Few newly registered nurses recalled more than superficial preparation in university for the role and some were encouraged by senior colleagues to downplay the importance of patient education.
Conclusions
The patient-education aspirations of newly registered nurses need to be nurtured. Educational institutions have an important role to play as do experienced nurses, making explicit the education they routinely deliver and supporting newly registered nurses to build their own pedagogic expertise.
Keywords
Introduction
The Nursing and Midwifery Council’s (NMC’s) Standards of Proficiency require that newly registered nurses (NRNs) have the knowledge and skills to ‘work in partnership with people … to support individuals, their families and carers to manage their own care when appropriate’ (NMC, 2018: 17). NRNs are required to discuss the impact of behaviour on health, to optimise patient understanding and promote shared decision making. Implicit to these standards is an educational role that involves providing information, explaining its meaning and demonstrating its value in ways that make reasonable adjustments for an individual’s circumstances (NMC, 2018). Although preregistration curricula aim to provide the knowledge and skills required of a modern health professional, little is known of the extent to which NRNs feel prepared and confident to deliver patient education, or of their experiences of delivering education in clinical contexts where they may encounter barriers.
Background
Allan et al. (2015) contend that professional knowledge held by NRNs is re-contextualised in the move from one context (student) to another (registered nurse). New forms of disciplinary knowledge hold the key to understanding professional practice, which often involves remodelling an NRN’s learning as a student and their ideals as a registered practitioner. There is evidence that NRNs feel unprepared to work effectively in clinical practice following their university and clinical placement education (Royal College of Nursing (RCN), 2017). Although this may result from gaps in curricula or from inadequate clinical exposures, Allan et al. (2015) also refer to ‘threshold concepts’ that can only be mastered in practice. The patient education role is one threshold concept for NRNs that is under-reported in the literature (Halse et al., 2014).
In the past, patient education consisted mainly of the transfer of knowledge with health providers acting as information authority figures. However, many patients have chronic conditions for which information provision alone is not enough. They need education to learn and develop competencies and adaptive behaviours that lead to the improvement and maintenance of their health (Wittink and Oosterhaven, 2018). In this sense, patient education has shifted from a transfer of knowledge to the co-creation of knowledge by attending to people's health literacy skills.
Health literacy concerns people's knowledge, motivation and competences to access, understand, appraise and apply health information to make judgements and take decisions in everyday life concerning healthcare, disease prevention and health promotion (Wittink and Oosterhaven, 2018). Limited health literacy has been linked to poor disease management, non-adherence to treatment recommendations and increased hospitalisations (Wittenberg et al., 2018). Improving health literacy is acknowledged as a crucial element in the fight against the rising tide of chronic health conditions (Hughes, 2016).
Svavarsdóttir et al. (2016) investigated health professionals' views of the knowledge and skills needed for educating patients with a chronic health condition. Up-to-date theoretical and clinical knowledge along with advanced communication skills were considered essential for patient education, which involved establishing interpersonal relationships with patients, capturing learning needs, facilitating an effective dialogue and providing individualised education and lifestyle counselling. These pedagogic competencies describe an educational process from relationship building to the delivery of person-centred learning.
In practice, the context for patient education is an important determinant of its effectiveness. Time constraints and heavy workloads can frustrate attempts to educate patients (Ball et al., 2014; Jones et al., 2015), as can concerns among some staff for appearing critical or judgemental, thereby adversely affecting the nurse–patient relationship (Svavarsdóttir et al., 2016). Kennard (2016) has also argued that although responsibility for patient education is mostly shouldered by nurses, they are the discipline most lacking in knowledge and awareness about health literacy. Student nurses have confirmed that patient education is poorly defined and rarely discussed in practice (Halse et al., 2014). As a threshold concept for NRNs, this raises concern.
International and national policy prioritises the promotion of self-management among people with long-term conditions (LTC) (World Health Organization (WHO), 2014; NHS England, 2016). Approximately 17.5 million people have an LTC in the United Kingdom (UK) and 70% of inpatient bed days in England are used for LTC (Lacobucci, 2017). LTC such as diabetes and heart disease are illnesses that cannot currently be cured but can usually be controlled by medication, other treatments and lifestyle adjustments. Nurses’ education of patients to promote health literacy is more important than ever for building patients’ knowledge, skills and preparedness for self-management in daily life (Bergh et al., 2015). NRNs who begin their professional career in hospital settings are in a key position to provide that education. Hospital admissions can be catalysts for change and patients with chronic conditions need nurses who can capitalise on those opportunities sensitively and purposefully. This study aimed to gain a deeper understanding of NRNs’ experiences of delivering patient education in an acute hospital setting by:
describing NRNs’ feelings and attitudes towards patient education and the value they attribute to it; identifying factors that enable or hinder patient education by NRNs; exploring how well pre-registration education prepared NRNs for a patient education role.
Methods
Design, setting and sample
The research employed an exploratory design using qualitative methods and was conducted in an inner-city NHS teaching hospital in the south of England among NRNs working in general medical and surgical wards. The NRNs were first approached via email from the lead for their preceptorship programme. Inclusion criteria sought registered adult nurses with a bachelor’s degree or post-graduate diploma from a UK university, who had been qualified for between 6–12 months and had at least 3 months’ experience of working in the acute hospital sector. NRNs who worked night shifts or in critical care were not included. The researcher then contacted potential participants to provide verbal and written information about the study. This process resulted in a purposive sample of seven NRNs.
Research instrument
A semi-structured interview guide explored key themes identified in the literature and allowed participants to raise additional points relevant to their patient education role. Eight key questions considered participants’ understanding of patient education, the required skills, their experience of delivery and factors that hindered or enabled their educational role. Supplementary questions were asked by the researcher as each interview progressed. The interviews were conducted in May/June 2015, took approximately 60 minutes each, were conducted in a private room in the NHS trust’s education centre and were audio recorded with participants’ permission.
Ethical considerations
Ethical approval was granted from the NHS Trust on 2 April 2015 (C&W15/038) and from the King’s College London Psychiatry, Nursing and Midwifery Research Ethics Subcommittees on 26 January 2015 (PNM/14/15-82). Attention was paid to the power imbalance of the clinical teacher as researcher and the nurses as research participants, and to the requirement that they reflect on clinical experiences about which they may feel uncertain and/or distressed. Anonymity of the discussion and assurances that its content would not affect their statutory training were emphasised. The researcher also sought to engage with compassionate sensitivity to protect participants’ wellbeing. Details of how to access the NHS trust’s confidential counselling services were also made available, although these were not required.
Data analysis
An interpretive phenomenological approach (IPA) was adopted to analyse the data, which followed Smith et al.’s (2009) five-step process: reading and re-reading the transcripts; initial noting; developing emergent themes; searching for connections across emergent themes; and looking for patterns across participant data. IPA requires the researcher to be the primary analytical instrument whose experience is necessary for making sense of a respondent’s experiences (Smith et al., 2009). Interpretation of the data therefore relies on the researcher’s interpretative lens with findings emerging from the data but also from the relationship between the informants and researcher (Finlay, 2002). The lead researcher was known to some of the participants as a clinical teacher and had been inspired to conduct this work from observing the importance that student nurses placed on the acquisition of technical skills over less visible skills such as patient pedagogy. With a clinical background in vascular disease the researcher also holds professional expertise and an interest in the education of patients with LTC.
As the researcher had a broad understanding of the phenomena under investigation, a statement of positionality formed a reflexive starting point to guide the analysis process. Transparency of the process was assured through the use of a reflexive diary that allowed the researcher’s positionality and its impact on the research process to be acknowledged and considered. Positionality, reflexions and analyses were reviewed by a research colleague who checked for consistency of coding, thematic attributions and interpretation of the data. Any uncertainty between reviewers was resolved through discussion.
Findings
Five of the NRNs worked on medical wards, one on a surgical ward and one on a mixed medical/surgical ward. Their length of qualification ranged from 6 to 10 months. All were women who provided care to patients with a variety of common LTC including diabetes, respiratory and cardiovascular disorders. Three superordinate themes emerged from their interviews: the professional self; the ward environment; and the nurse–patient relationship. Within each, the views of NRNs reflected specific sub-themes (Figure 1).
Superordinate and sub-themes.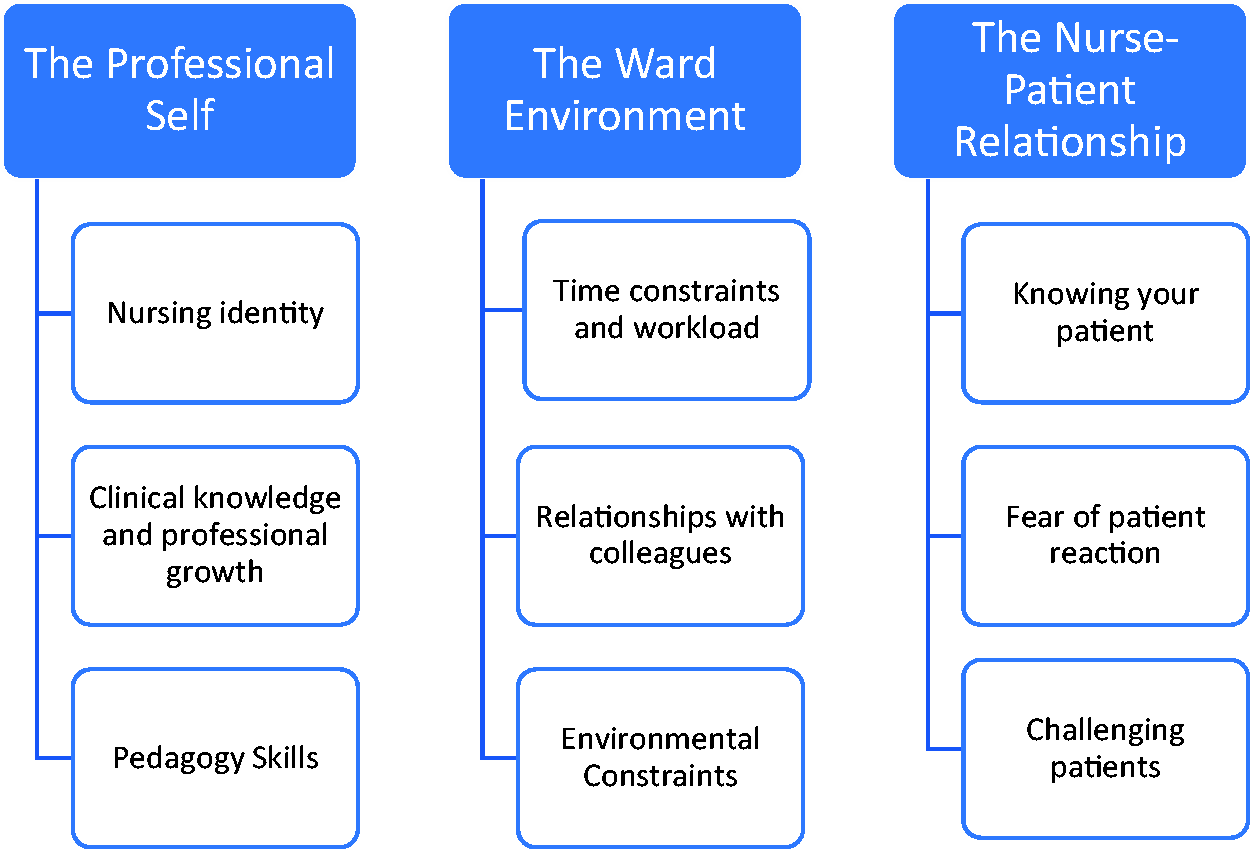
The professional self
The professional self concerns the development of a professional nursing identity. This includes the knowledge, skills and attitudes necessary for the role, which shape both a nurse’s understanding of patient education and their experience of its delivery.
Nursing identity
All NRNs believed that patient education was a foundational aspect of nursing practice. They voiced responsibility, commitment and enthusiasm for the role, and grounded these attitudes in the belief that education could benefit a patient’s overall health and wellbeing. One NRN emphasised the rights of people to be educated about their health condition and the corresponding sense of duty this placed on them. Participants also recognised their accountability for the accuracy of any information provided and emphasised the importance of honesty and a willingness to seek support from others if unsure how to respond to a patient’s request for information: ‘the important thing, I’ve found, is just acknowledging the fact that you don’t know the answer and be honest with the person, but then doing your best to find someone who does know the answer’ (participant (P) 2).
Clinical knowledge and professional growth
The patient education role highlighted an important dynamic for NRNs between the acquisition of clinical knowledge and their professional growth. Patient education required a sound knowledge base, much of which was a product of clinical experience. Although pre-registration training provided a grounding in generic nursing skills ‘the lack of training in specific areas … made it harder to give correct patient education’ (P4). Practice-based clinical knowledge, confidence as an educator and growth as a professional were part of a developmental continuum for these NRNs, who endeavoured to match their educational competence to specific patient needs. For example, they felt more able to provide education to a newly diagnosed patient than to an ‘expert patient’.
Pedagogy skills
The most common patient education activities were information giving, explaining and providing instructions, each of which reflected routine nurse-led interactions. Although the NRNs aimed to individualise patient teaching, it was often delivered informally in an unplanned way, seizing opportunities as they arose with limited patient involvement in collaborative goal setting: ‘Patient education as a principle is something that we do on purpose or inadvertently … all the time … I think that throughout a shift you will be giving patient education’ (P2) and ‘I think it’s just from experience really, it’s looking at the patient, it’s like pre-empting what you think they’re going to need’ (P3).
The non-differentiation of patient pedagogy from routine care made it difficult for participants to specify pedagogic components such as learning needs assessment, goal planning, implementation and the evaluation of learning. Psychomotor skills could be evaluated as observable behaviours, but when teaching involved the delivery of information alone, which was the most common strategy, the need to evaluate went unrecognised. However, the need for effective communication skills was widely recognised. All participants reported acting as ‘interpreters’ of information, simplifying and adapting information to a patient’s level of understanding.
Few remembered more than superficial preparation in university for their patient education role. Whilst its importance was conveyed, patient education strategies had been lacking. Neither did the NRNs recall any preparation during their practice placements. Some had found role models who demonstrated expert education skills whilst others had relied on ‘trial and error’. The NRNs believed that confidence in patient pedagogy would evolve from their clinical experience, ‘I think as you go along... by practising everyday it will just come to you’ (P1).
The ward environment
The ward environment concerns the impact of factors in clinical practice that influence the education of patients. Some acted as barriers and others as facilitators.
Time constraints and workload
Time constraints imposed by heavy workloads were commonly reported barriers to patient education. Because a patient’s understanding could be unpredictable, the NRNs considered patient education to be a time-consuming process over which they had little control. The education of patients became an ‘optional extra’ that was conditional on other work demands, ‘You don’t have time to do the smaller things and patient education sometimes ends up coming to the bottom of the pile’ (P4) and ‘Patient understanding can vary, that’s not something you have control over, so it’s kind of starting a race that you don’t know when the end [is]’ (P2).
Relationships with colleagues
All NRNs emphasised the need for inter-professional cooperation to support patient education activities, ‘If you can see that the physio’s coming in, sometimes I go in and just see how they’re mobilising the patient so that we’re all giving the same advice’ (P3).
Although senior nursing colleagues were generally viewed as supportive and encouraging, this was not always the case. One NRN was discouraged from delivering patient education, being told ‘it’s not your job, you don’t have to do it’ (P5). Others had experience of patient education not being valued by senior colleagues. These experiences frustrated the NRNs, one of whom implemented patient education strategies despite potential conflict with senior colleagues, ‘So I do it when they’re away, in a sneaky way, so they don’t have to tell me again, “You can’t do that”’ (P6).
Environmental constraints
The NRNs identified constraints to patient education imposed by the hospital environment and its routines. A lack of privacy raised concerns for patient confidentiality ‘because inside the ward it is only divided by the curtains … and whatever you say … the next-door-neighbour can hear’ (P1). The speed of patient throughput in an acute hospital setting was also a constraint. ‘Sometimes it might be a case of, oh, they’re going to be discharged, we have to sit them out in the day room … and they’re just whisked off by transport before you’ve had [a] chance’ (P3).
The NRNs were also uncertain over the extent to which they could model a patient’s home in the ward environment. There was a recognition that education should begin with an appreciation of the context in which it was to be applied. The only teaching resources available to NRNs in the ward environment were leaflets. Even then, their availability was varied and there was a general assumption that patients would be able to understand the information they contained. Some participants used the internet to obtain information both for themselves and to share with their patients.
The nurse–patient relationship
This theme is concerned with how the nurse–patient relationship influences patient education and is also affected by it.
Knowing your patient
Knowing your patient through the development of a therapeutic relationship facilitated the identification of patient concerns and an appreciation of the patient’s situation. This allowed NRNs to adjust any education according to a patient’s level of need and understanding. This involved the NRNs adopting the patient perspective, putting themselves in their shoes, and having an intuitive sense of a patient’s readiness to learn. ‘I think it’s important to know your patient because then you’ll be able to give them appropriate information in an appropriate way’ (P2) and ‘You just get a sense that … they don’t really want to change. There are other people where you sense that actually they would be open’ (P7).
Importantly, the NRNs spoke of the need to ‘be there’ for the patient who may not be ready for information about their condition. One participant described the need to remain therapeutically available in the face of initial resistance. ‘Maybe they’re not ready to learn anything but just showing that you’re ready and open if they’re ready, that that makes a big difference’ (P4).
Fear of patient reaction
Participants feared appearing critical of patients, which created an unwillingness to engage in therapeutic discussions and associated educational opportunities. The NRNs appeared to lack the advanced communication skills necessary to initiate and manage discussions on sensitive issues, particularly lifestyle choices. ‘You’re on a bariatric bed and … I’m not sure you should be drinking that and it’s how do you say that politely’ (P5) and ‘It’s difficult if it then comes across as sort of judgemental on how they currently live’ (P7).
Challenging patients
Participants identified some patients as presenting greater educational challenges than others. People with specific symptoms such as dysphasia and the cognitive decline associated with normal aging required different approaches, limiting the amount of information given at one time and providing frequent reinforcement. This could also be frustrating. ‘Every time I see them every day and I say things, the same things again and again and again so many times and so that is quite challenging’ (P6) and ‘The expressive, receptive dysphasia. It was a real shock … I just hadn’t a clue how to communicate’ (P5).
Another challenge was the ‘expert patient’ who already had significant knowledge about their condition. Although some participants experienced this as a learning opportunity for themselves, others felt vulnerable and were anxious it would affect the nurse–patient relationship. ‘It can be quite challenging sometimes because you feel undermined … and then you feel like maybe they won’t have confidence in you as a nurse’ (P4).
Discussion
Findings from this study provide insights into the experiences of delivering patient education by NRNs. There is evidence of a tension between the professional ideals participants brought to registered practice and the practice-based realities they encountered in their patient education work.
Professional ideals
All NRNs expressed a firm belief that patient education was integral to their role and responsibilities. This stands in contrast to the work of Bergh et al. (2014), who noted ambiguity among some nurses who viewed patient education as conditional on other work demands. However, the mean length of qualified practice for participants in the Bergh et al. (2014) study was 9 years, whereas in the present study the maximum length of qualified practice was just 10 months. One interpretation is that the NRNs were striving for a professional ideal that had been assimilated as conditional by more experienced staff.
Although the NRNs could not articulate patient pedagogy processes, they did emphasise specific components. The importance of sound clinical knowledge and effective communication skills was widely recognised, as reported by others (Svavarsdóttir et al., 2016). Some NRNs emphasised the need to adjust any education according to a patient’s level of need and understanding and to remain therapeutically available for patients who may be reluctant to receive information. These nuanced understandings of person-centred education are encouraging but were not explicitly positioned in a theoretical appreciation of patient pedagogy or health literacy, subjects that the NRNs did not raise as important. Instead, the NRNs tended toward a view of patient education as an implicit part of nurse-led care processes. The inseparability of pedagogy from care is found in other work that describes patient education as routine and ‘invisible’ (Bergh et al., 2014).
The NRN’s confidence to deliver patient education was dependent on the acquisition of clinical knowledge through experience. In turn, this was closely linked to a sense of developing professionalism. These are important markers for clinical competence and of understandable significance to the NRNs who were establishing themselves as new registrants. However, they leave little room for educational theory. Clinical knowledge and experience alone were the NRNs’ anticipated requirements for pedagogic competence. Preregistration education had not equipped them with an evidence-based understanding of patient pedagogy or the tools and techniques available to ensure nurses communicate effectively and meet patients’ health-literacy needs. The patient education role was to be mastered tacitly, through trial and error in clinical practice.
Practice-based realities
Not all information exchange results in a pedagogical dialogue as learning needs can be ignored and understanding assumed. This risk was evident in the responses of some NRNs who, despite professional aspirations, believed learning needs could be pre-empted without any assessment or evaluation to support their underlying assumptions. More generally, patient teaching was often delivered informally in an unplanned way, disconnected from learning theory, seizing opportunities as they arose and with limited patient involvement in collaborative goal setting or appreciation for their health-literacy needs. These characteristics of the nurse’s patient education role are not particular to NRNs and have been reported among experienced nurses (Bergh et al., 2014).
Participants turned to senior colleagues for patient education support, which was not always forthcoming. That NRNs sought explicit opportunities and guidance for patient education in contexts where more experienced staff might implicitly and informally incorporate it into their work, or actively discourage it, are important findings. Encouraging awareness of patient pedagogy among experienced staff, including recognition of the theoretical knowledge and practical skills they possess, would provide a valuable resource to NRNs. It has been recommended that nurses more clearly articulate their patient education role (Kennard, 2016; Bergh et al., 2015) and this study adds weight to that need.
Service systems and the nurse–patient relationship presented other barriers to patient education. Systemic workload pressures have been reported elsewhere as major barriers to successful implementation of patient education (Ball et al., 2014; Jones et al., 2015). The NRNs’ experiences also confirmed that lack of privacy and patient confidentiality in acute hospital settings can restrict a nurse’s willingness to deliver patient education (Bergh et al., 2014; Svavarsdóttir et al., 2016). An interesting finding is the association between a patient’s level of understanding and pressures on an NRN’s time. Because the former was uncertain before initiating a piece of education the latter was also uncertain, which generated anxiety for the NRN in the face of other competing demands. Such tensions are likely to be a constant source of pressure in acute hospital environments where system-oriented goals outweigh the sensitivities of person-centred learning. NRNs’ levels of anxiety may reduce as they gain experience and a repertoire of educational skills. However, there is a risk that anxieties are managed by relegating patient education to a conditional, optional extra; a perspective that some NRNs had been encouraged to adopt by more senior colleagues.
One NRN implemented their own patient education strategies to avoid conflict with senior colleagues. This conflict-resolution strategy has been reported among nurses (Iglesias and Vallejo, 2012) but has not previously been reported among NRNs with respect to patient education. These findings echo Allan et al.’s (2015) notion of a ‘threshold concept’ as the NRN’s knowledge and professional identify becomes re-worked or re-contextualised to practice within the service constraints and opportunities they encounter. The passion and commitment expressed by the NRNs towards patient education is admirable but also vulnerable to the realities of registered practice. That it was sometimes delivered in clandestine ways to avoid reprimands from senior colleagues is understandable, but also raises concern for the quality of any education by junior staff in contexts where the intervention is not valued by senior colleagues.
Study limitations
This is the first study of its type to explore the patient education experiences of NRNs in an acute hospital setting in the UK. However, the use of an idiographic methodology and a small sample drawn from a single site limit the transferability of its results. Additionally, six of the participants attended the same university and all were female. Different results would be anticipated from different samples, particularly in terms of the adequacy of their pre-registration education. The voluntary nature of participation may also have led to some selection bias if those involved had a specific interest in patient education. Nevertheless, many of the findings resonate with other published work and reveal important insights worthy of further research and practice development.
Conclusions
It is encouraging that the participants of this study felt enthusiasm, along with a degree of trepidation, for their patient education role. However, enthusiasm for teaching does not automatically translate into a teaching skill. Preregistration education needs to equip nursing students with the necessary tools to assess patient health literacy and to understand their own patient teaching role. Findings from this study indicate opportunities for improvement as when transitioning into professional practice, patient education became a threshold concept that was difficult to negotiate. It is also important that the patient education aspirations of NRNs such as these are protected and nurtured. They are needed in hospital contexts that increasingly manage the acute complications of chronic conditions and where opportunities can be capitalised on to support the health literacy of patients through person-centred education. Educational institutions have an important role to play but so too do experienced nurses, making explicit the education they deliver routinely in their work, building the evidence base and articulating the case on which NRNs can build their pedagogic expertise.
Key points for policy, practice and/or research
Nurses’ education of patients is more important than ever for building patients’ knowledge, skills and preparedness for self-management in daily life. Preregistration university and placement education does not always appear to equip NRNs with an evidence-based understanding of patient pedagogy, which can generate significant anxieties in practice. Encouraging awareness of patient pedagogy among experienced staff, including recognition of the theoretical knowledge and practical skills they possess and deliver routinely in their work, would provide a valuable resource to NRNs. Making patient pedagogy more explicit in the clinical environment provides the opportunity to match nursing experience with patient need, thereby nurturing pedagogic competence in the workforce and managing associated anxieties.
Footnotes
Declaration of conflicting interests
The author(s) declare no potential conflicts of interest with respect to the authorship and/or publication of this article.
Ethics
Ethical approval was granted from the NHS Trust on 2 April 2015 (C&W15/038) and from the King’s College London Psychiatry, Nursing and Midwifery Research Ethics Subcommittees on 26 January 2015 (PNM/14/15-82).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.