
Abstract
Background
Ostomates have several physical, psychological and social health problems. These problems negatively impact the ostomates' quality of life.
Aims
This study aims to identify Jordanian ostomates' health problems and their self-care ability to manage their ostomies.
Methods
This is a cross-sectional study. A convenience sampling method was used to recruit 168 Jordanian patients with intestinal ostomies. A self-report questionnaire was used to collect the data.
Results
On average, the participants’ physiological ostomy-related problem scores were 8.76 ± 2.37 (out of 13 problems) and the total score of self-care ability to manage their ostomies was 16.56 ± 2.62 (out of 24). About 22% of the participants had ‘moderately severe’ to ‘severe’ depression (nine-item Patient Health Questionnaire score ≥15) and 33.9% had ‘moderate’ to ‘severe’ anxiety (seven-item General Anxiety Disorder questionnaire score ≥10). About half of the participants had exposure to teaching and/or training about ostomy care. About 85% of participants were willing to attend health education and training programmes about ostomy care. There was a significant correlation between high ostomates’ self-care ability to manage their ostomies and a low number of physiological health problems (r = −0.67, p = 0.04), a low depression (Patient Health Questionnaire 9) score (r = −0.54, p = 0.039) and a low anxiety (seven-item General Anxiety Disorder questionnaire) score (r = −0.71, p < 0.027).
Conclusions
Health teaching and training about intestinal ostomy management, psychosocial support, follow-up assessment and treatment for ostomy-related problems are recommended for all ostomates.
Keywords
Introduction
Worldwide, colorectal cancer is the third most common cancer type among men and second most common among women. In 2017, its incidence was about 1.8 million cases with about 896,000 deaths worldwide and a higher mortality rate in developing countries. Colorectal cancer cases increased by 5% between 2007 and 2017 globally (Global Burden of Disease Cancer Collaboration, 2019). In Jordan, colorectal cancer is the second most common type of cancer in both genders, accounting for about 11% of all new diagnosed cancer cases among Jordanians. In 2013, malignant tumors were the second leading cause of all deaths (16.4%) in Jordan. Colorectal cancer alone accounted for 2% of all deaths in Jordan (Ministry of Health Jordan, 2013).
Intestinal ostomy is a surgical procedure that creates an opening between the intestine and the surface of the patients' body to excrete waste products. In 2012, about 1.2 million patients with colorectal cancer in the United States had an intestinal ostomy (United Ostomy Associations of America, 2017). Worldwide, insertion of an intestinal ostomy is increasing by about 3% each year (United Ostomy Associations of America, 2017).
Despite the importance of intestinal ostomy procedures for the survival of patients, ostomates face several physiological and psychosocial health problems, including severe gas and odour from the ostomy, pouch leakage, skin irritation, altered body image and depression or anxiety. Ostomies also negatively impact ostomates' occupational health, daily life activities and quality of life (QOL) (Ayaz-Alkaya, 2019; Silva et al., 2017; Vonk-Klaassen et al., 2016). Moreover, Muslim ostomates, who carry out their ablutions and prayers five times a day, face several difficulties in practicing their worship and spiritual activities (Karadag and Baykara, 2009; Iqbal et al., 2016).
The majority of patients with intestinal ostomies, particularly those with a permanent ostomy, have several undiagnosed and untreated ostomy-related problems. Moreover, those ostomates are at high risk of developing acute and chronic physical disorders, serious psychological disorders such as depression and anxiety and threatening life events (Ayaz-Alkaya, 2019; Recalla et al., 2013; Silva et al., 2017; Vonk-Klaassen et al., 2016; Rossella et al., 2018). Furthermore, some ostomates live in areas with a lack of medical resources, healthcare facilities and a shortage of qualified ostomy care specialists. Also, many ostomates do not seek healthcare services until their ostomy-related problems are significantly worsened (Vonk-Klaassen et al., 2016; Agarwal and Ehrlich, 2010). The literature shows a significant positive impact of improving ostomates' knowledge and self-care abilities and competencies in taking care for their ostomies to reduce ostomy health-related problems and complications (Ayaz-Alkaya, 2019; Hendren et al., 2015; Mohamed et al., 2017; Recalla et al., 2013). Therefore, providing perioparative teaching and conducting periodic continuing health education and training programmes about ostomy care are very important and recommended for all ostomates to improve the ostomates' knowledge and skill to manage their ostomies and to prevent ostomy-related problems and complications (Cheng et al., 2013; Elshatarat, 2020; Mohamed et al., 2017; Recalla et al., 2013).
The literature shows the importance of involving the ostomates and their families in the nursing care plan, which requires cooperation between healthcare providers, including nurses and physicians, the ostomates and their close family members (Gemmill et al., 2011; Silva et al., 2017; WOCN, 2010). Nurses provide direct care, spend several hours with the ostomates and are considered the backbone of the healthcare system. Literature also showed that nurses can play a major role in assessing and managing ostomy-related problems and provide health education and training on ostomy care for ostomates and their families (Gemmill et al., 2011; United Ostomy Associations of America, 2017; WOCN, 2010; Zhang et al., 2013). However, the literature also shows a lack of nurses' knowledge and competence about ostomy care and low self-confidence in their abilities and readiness to provide health education and training about ostomy care to ostomates (Berti-Hearn and Elliott, 2018; Cheng et al., 2013; Cross et al., 2014; Elshatarat, 2020). Therefore, it is very important to provide continuous health education and training programmes on ostomy care to nurses to ensure the successful implementation of nurses' activities to achieve the delivery of care plans to ostomates. Also, adopting international clinical guidelines in healthcare settings is recommended to improve health professionals' knowledge about recommended ostomy care and to ensure treatment care plans are implemented based on evidence-based practice and updated scientific research (Elshatarat, 2020; Gemmill et al., 2011; Hendren et al., 2015; Subih and O'Neill, 2012; WOCN, 2010).
Study significance and objectives
Once discharged from hospital after the insertion of the intestinal ostomy, ostomates have to take care of their ostomy themselves or with help from their families. Community health nurses have a major role in educating ostomates about ostomy care. To carry out their roles and organise strategies involving the patients and their families in this treatment plan, it is very important nurses are aware of the physiological and psychological ostomy-related problems and assess patients' self-care ability to take care of their ostomy (Ayaz-Alkaya, 2019; Vonk-Klaassen et al., 2016; WOCN, 2010). Also, reviewing national and international published studies related to the assessment of ostomates may help nurses and other health professionals establish a plan and make decisions regarding care (Ontario, 2009; Silva et al., 2017; United Ostomy Associations of America, 2017; Vonk-Klaassen et al., 2016; WOCN, 2010).
A database search on the published studies of the assessment and the management of ostomy-related problems in Jordan revealed no publications on ostomates' health problems and their experience in taking care of their ostomies in Jordan and in other Arab countries. Therefore, the current study investigated Jordanian ostomates' ostomy health-related problems (including physiological and psychological) and their self-abilities and practice in managing their ostomies.
The specific objectives of this study are to determine: (a) the participants' ostomy-related problems (including physiological and psychological); (b) the participants' exposure to previous education and training about ostomy care; (c) the participants' abilities to take care of their ostomies themselves; (d) the correlation between the participants' ostomy-related problems and their self-care abilities for their ostomies; and (e) the relationship between participants' demographics and clinical data and their self-care abilities for their ostomies.
Methodology
Research design
A cross-sectional design was conducted to address the aims of the current study.
Research sample and setting
A convenience sampling method was used to recruit 168 ostomates from two private hospitals in Amman, Jordan. These hospitals have a full range of medical and surgical care, particularly for intestinal ostomy insertion and management.
The inclusion criteria of the current study were adult patients (≥18 years old) who had intestinal ostomies for at least 12 months, were admitted to hospital to receive healthcare for their ostomies or other health disorders and were Arabic language speakers. The exclusion criteria were medically unstable patients and those who had mental or psychiatric disorders.
GPower software program (version 3) was used to estimate the effective sample size. The researchers used the power of 0.80, significant p value of 0.05 and moderate effect size of 0.30. A minimum of 129 subjects was enough to achieve the satisfied power analysis. The researchers invited 200 eligible participants to participate in this research. In total, 18 participants refused to participate and 14 questionnaires were removed because the participants did not answer all the questions.
Data collection procedure and ethical considerations
Institutional Review Board approval was obtained at Al-Ghad International Colleges for Applied Medical Sciences to conduct this current study. Before data collection, ethical approval was obtained from the general medical managers and the directors of nursing at the selected hospitals. The researchers obtained the names of eligible participants from the head nurses at the selected settings. A written consent form was signed by all patients who decided to participate in the study. The participants were informed that taking part was voluntary and their personal data were confidential and anonymous.
The data were collected by interviewing the participants in their room or in a private room at the selected setting. Patients who preferred to answer independently were given a questionnaire and asked to return the completed questionnaire to the researchers or drop it in a closed box in the head nurse's office at the selected setting.
Instruments
The researchers used a structured self-report questionnaire to address the study objectives. The demographic data were obtained from the participants. The researcher used participants' medical records to identify their clinical data, including type of stoma, location of ostomy and reason for ostomy insertion.
To identify physiological ostomy-related problems, the participants were asked: ‘during 2 weeks before the current hospitalisation, did you complain about any of the following health problems?’ The researchers listed 13 ostomy-related problems (e.g. fatigue, abdominal pain, abdominal gases, diarrhoea, etc.). Then the participants were asked to answer 1 = yes if they have the problem or 0 = no if they did not have the problem. This subscale was adopted from the City of Hope quality of life-ostomy questionnaire (Grant et al., 2004), particularly the physical wellbeing subscale, and was modified according to this study's objectives. The validity and reliability of this subscale was documented (Grant et al., 2004).
The nine-item Patient Health Questionnaire (PHQ-9) was adopted from a previous study to screen participants for major depression (Kroenke and Spitzer, 2002). The researchers used the Arabic version of PHQ-9 in this study. The validity and reliability of the original version and Arabic version of PHQ-9 were documented (Kroenke and Spitzer, 2002; Kroenke et al., 2010). The participants' responses on this scale were 0 = not at all, 1 = several days, 2 = more than 50% of days and 3 = nearly every day. The total score for PHQ-9 ranges from 0 (no depression) to 27 (severe depression) (Kroenke and Spitzer, 2002; Kroenke et al., 2010).
To assess the participants' general anxiety disorders, the Arabic version of the seven-item General Anxiety Disorder (GAD-7) questionnaire was used (Spitzer et al., 2006). The validity and reliability of the original English version and the Arabic version of GAD-7 were also documented (Kroenke et al., 2010; Spitzer et al., 2006). The patients' responses for GAD-7 were similar to their responses for PHQ-9. The total score of GAD-7 ranges from 0 (no anxiety) to 21 (severe anxiety) (Kroenke et al., 2010; Spitzer et al., 2006).
To address the second objective of this study, participants were asked to report if they had been exposed to previous theoretical education or clinical training programmes about ostomy care during the last 12 months. Moreover, all the participants were asked to report their willingness to participate in education and training programmes about ostomy care in the future. Those who received teaching and training about ostomy care were asked to report the source (including nurses and physicians) and the strategy (e.g. handout, online or multimedia materials) for these teaching and training programmes. These questions about participants' exposure to health education and training programmes about ostomy care were adopted from previous studies (Ran et al., 2016; da Silva et al., 2014).
A structured scale containing eight items was used to rate the participants’ self-care ability and practice in changing and irrigating the ostomy pouch, taking care of the peristomal skin and wearing clothes over the ostomy. The participants’ responses were 3 = ‘I am totally independent in ostomy care’, 2 = ‘I am partially independent in ostomy care’ and 1 = ‘I am totally dependent on someone else in ostomy care (e.g. family members)’. To identify the total score of participants’ self-care ability, all of these eight items were summed. The highest participants’ total score indicates the highest independence level of participants’ self-care ability to manage their ostomy. This scale was adopted from the previous study (Cheng et al., 2013). The validity and reliability of this scale was documented previously (Cheng et al., 2013).
Data analysis
SPSS software (version 21) was used for statistical data analysis. Frequencies and descriptive statistics were used to describe the participants' data. T-test analysis was carried out to determine the relationship between the participants' self-care abilities in managing their ostomies and participants' demographics and clinical data. Two separate analysis of variance (ANOVA) tests were run to identify the relationship between the participants' self-care abilities to manage their ostomies and the sources of education and training programmes about ostomy care and teaching strategies for improving their self-care abilities. Pearson's correlation test was carried out to identify the association between the participants' ostomy-related problems (physiological and psychological) and their self-care abilities in managing their ostomies. A p value <0.05 was pre-set as a significant relationship.
Results
Demographics and clinical data.
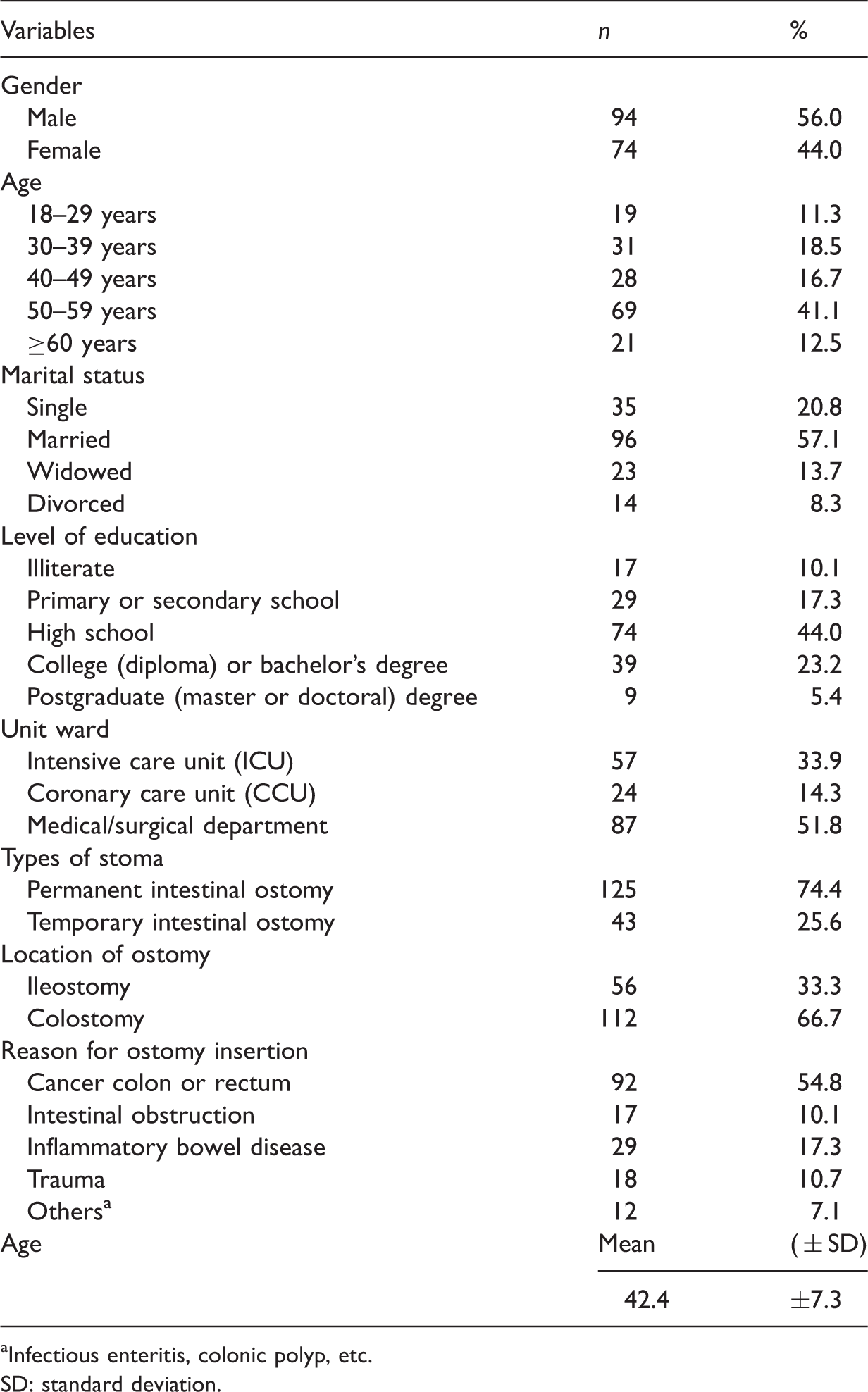
Infectious enteritis, colonic polyp, etc.
SD: standard deviation.
Physiological and psychological ostomy health-related problems.

Participants were able to select more than one choice, resulting in a total percentage >100.
Total score ranges from 0 (no problem) to 13 physiological ostomy-related health problems.
GAD-7: seven-item General Anxiety Disorder questionnaire; SD: standard deviation.
Participants' exposure to health education and training programmes about ostomy care.
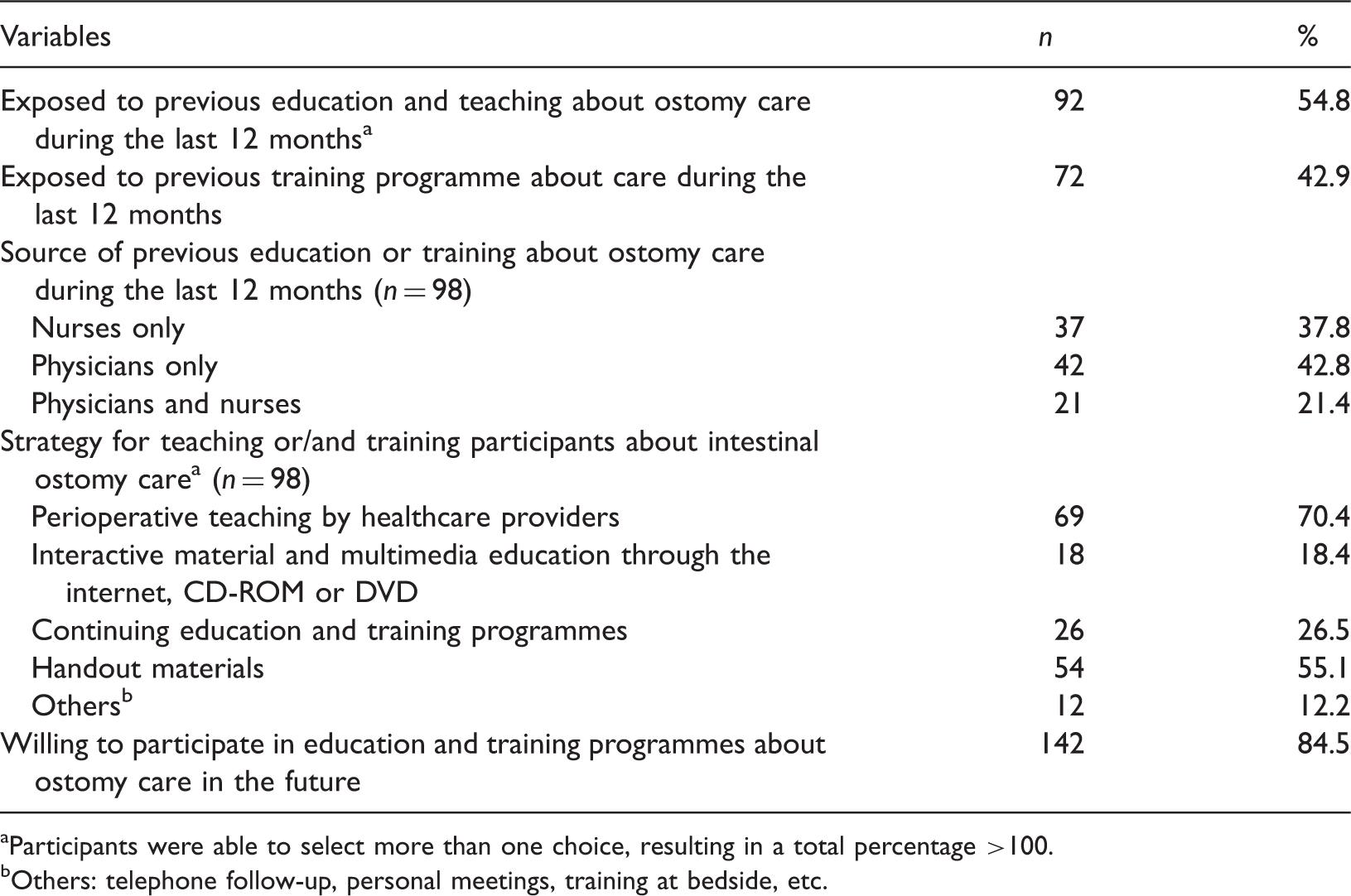
Participants were able to select more than one choice, resulting in a total percentage >100.
Others: telephone follow-up, personal meetings, training at bedside, etc.
Participants' self-care ability and practice in managing their intestinal ostomies.
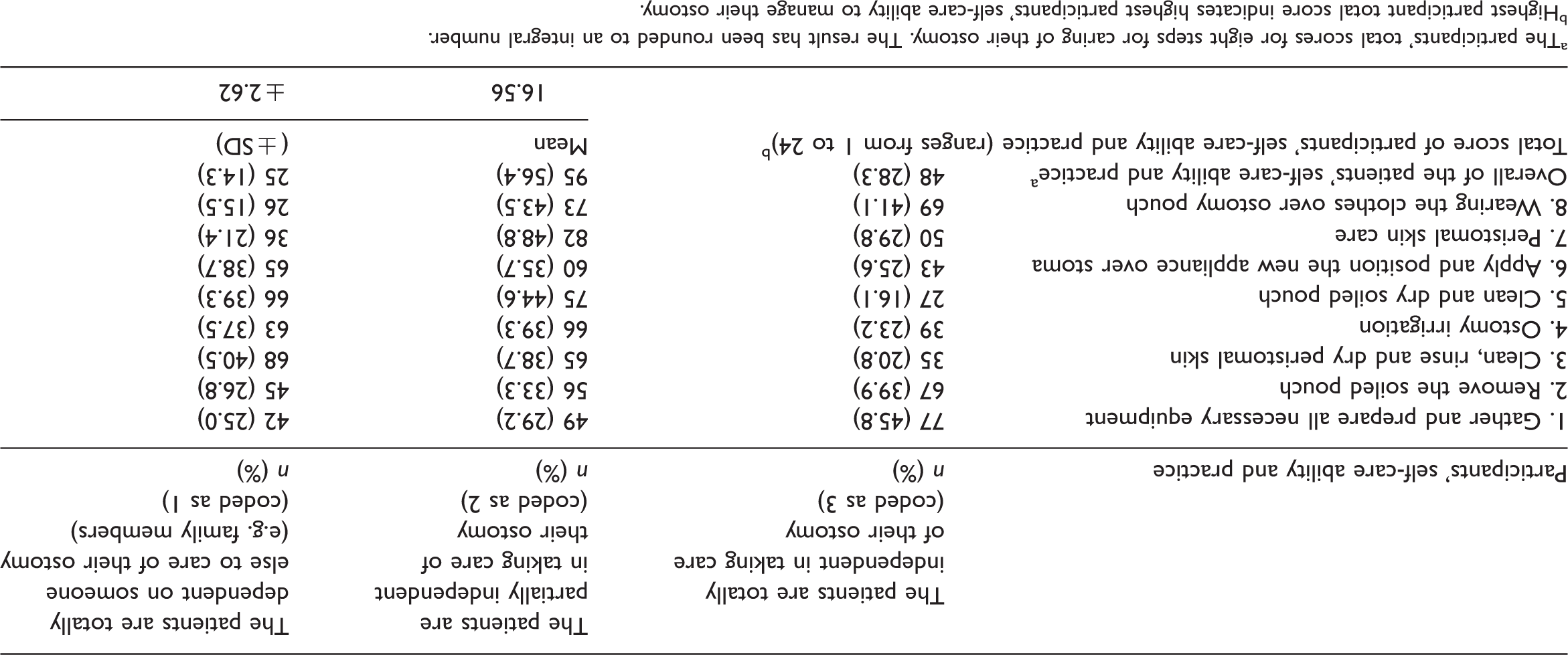
The participants' total scores for eight steps for caring of their ostomy. The result has been rounded to an integral number.
Highest participant total score indicates highest participants' self-care ability to manage their ostomy.
Pearson's correlation analysis (results are not shown in the tables) shows the participants who had high ability to take care for their intestinal ostomies themselves were significantly associated with having less physiological ostomy-related problems (r = −0.67, p = 0.035), low depression (PHQ-9) score (r = −0.54, p = 0.039) and a low anxiety (GAD-7) score (r = −0.71, p < 0.027).
The relationship between participants' demographics and clinical data and their self-care ability for their intestinal ostomies.
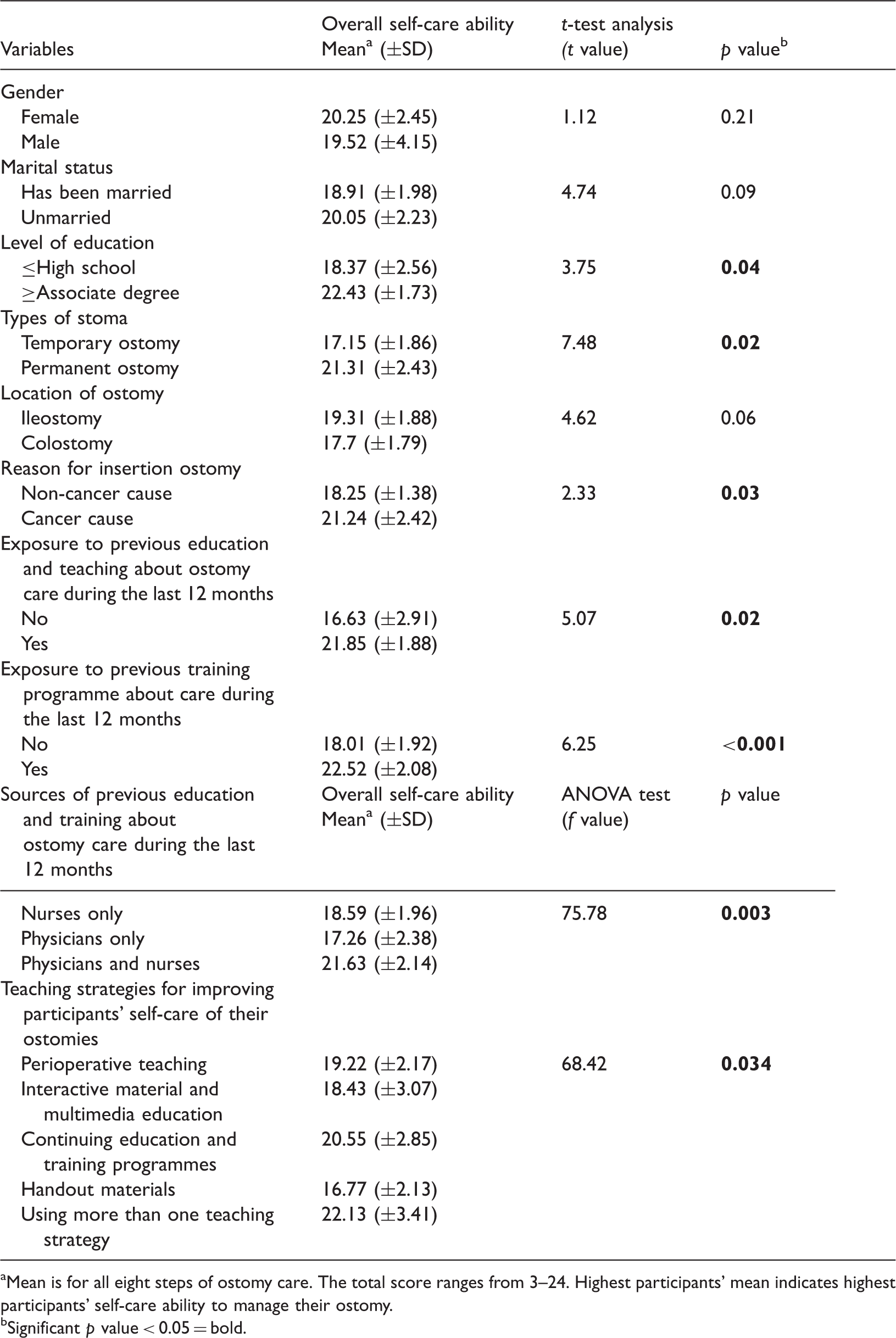
Mean is for all eight steps of ostomy care. The total score ranges from 3–24. Highest participants' mean indicates highest participants' self-care ability to manage their ostomy.
Significant p value < 0.05 = bold.
Discussion
This is the first study in Arab countries to investigate the association between Jordanian ostomates' health problems and self-care ability to manage their ostomies. Therefore, the current study offers important data to develop clinical guidelines for improving healthcare for intestinal ostomies and managing ostomy-related problems. Also, they will be baseline data for future research on the improvement of intestinal ostomy care.
Unfortunately, almost all of the participants (97.4%) had at least one physiological ostomy-related problem during the 2 weeks before hospitalisation. About half of participants had four or more physiological health problems, including abdominal pain, severe odour and gas. Similarly, several previous studies documented that these physiological problems were very common (United Ostomy Associations of America, 2017; Vonk-Klaassen et al., 2016). The overall clinical complication rate after intestinal ostomy insertion ranges between 21% and 70 % (Shabbir and Britton, 2010). Unfortunately, a large number of ostomates with these physiological health problems remain untreated for several years and they do not seek healthcare services unless these health problems are raised with them or become more complicated (Vonk-Klaassen et al., 2016; Agarwal and Ehrlich, 2010).
In this study, 22% of the participants had ‘moderately severe’ to ‘severe’ depression (PQH-9 ≥15). Also, 33.9% had ‘moderate’ to ‘severe’ anxiety (GAD-7 ≥10). These results were similar or higher than the prevalence of depression and anxiety among ostomates in the previous study (Jayarajah et al., 2016; Rafiei et al., 2017; Ayaz-Alkaya, 2019). Several studies documented a high rate of psychosocial problems among ostomates. Between 16% and 26% of ostomates experienced psychological symptoms immediately in the postoperative period. The majority of these psychosocial problems were related to poor body image and psychosocial adaptation, anxiety and depression (Ayaz-Alkaya, 2019; Jayarajah et al., 2016; Rossella et al., 2018; Silva et al., 2017). Living with an intestinal ostomy requires being attached to an ostomy bag all day, which negatively affects all aspects of ostomates’ QOL. These daily-life changes may be irreversible, depending on the ostomate's clinical condition, health professionals’ support, family members’ support and the use of coping strategies and rehabilitation programmes (Ayaz-Alkaya, 2019; Silva et al., 2017). Therefore, patients who undergo intestinal ostomy insertion surgery should be instructed about the benefits, negative consequences and complications of the surgery. It is also recommended that ostomates and family members are involved in decision making in the ostomy care process, treatment plans and clinical situations (Silva et al., 2017). Literature showed that early identification of psychological symptoms and using valid and reliable screening scales (e.g. PHQ-9 and GAD-7) in healthcare settings are an effective approach for prevention and management of psychological ostomy-related problems. Also, continuous follow-up, screening and monitoring for psychological ostomy-related problems for all ostomates during pre- and post-hospitalisation are strongly recommended (Ayaz-Alkaya, 2019; Jayarajah et al., 2016; Kroenke and Spitzer, 2002; Silva et al., 2017). Those who have psychological problems should be provided psychosocial support and referred to mental care specialists to receive treatment (Ayaz-Alkaya, 2019; Silva et al., 2017). For example, patients who have moderate depression (PHQ-9 score 10–14) should be considered for a treatment plan that involves health professionals’ psychological support, counselling, follow-up and/or pharmacotherapy. Also, patients who have ‘moderately severe’ (PHQ-9 score 15–19) to ‘severe’ (PHQ-9 score 20–27) depression should be considered for active treatment or immediate treatment, respectively, which involves referring the client to mental health specialists for initiation of pharmacotherapy and/or psychotherapy (Kroenke and Spitzer, 2002; Kroenke et al., 2010).
Lack of patients' exposure to education and training programmes about ostomy care is not limited to this study, it was also documented in previous studies (Nieves et al., 2017; Hendren et al., 2015; Ran et al., 2016). An interesting result of the current study shows the majority of participants are willing to attend education and training programmes about ostomy care in the future to improve their knowledge, self-abilities and skills to manage their intestinal ostomies. These results also are consistent with the previous studies (Cheng et al., 2013; Hu et al., 2014; Ran et al., 2016). Therefore, assertive strategies and policies should be implemented to ensure all ostomates receive postoperative teaching and training sessions before they are discharged from hospital (Hendren et al., 2015; Grant et al., 2013; Gemmill et al., 2011). Furthermore, conducting continuous health education and training programmes about ostomy are recommended for all those interested in participating in such programmes to enhance their knowledge and skills to manage their ostomies (Cheng et al., 2013; Grant et al., 2013; Ran et al., 2016).
In this study, only about 37% of participants received education on ostomy care from the nurses. Moreover, many of the participants said they were unsatisfied with the nurses' knowledge and skills in providing them teaching and training about ostomy care. Also, they felt these health education and training sessions were not adequately useful to improve their knowledge and skills about ostomy care. Similarly, the literature showed a deficit of nurses' knowledge and competencies about ostomy management and low self-efficacy in their ability to educate the ostomates about ostomy care (Berry et al., 2007; Berti-Hearn and Elliott, 2018; Cross et al., 2014; Gemmill et al., 2011; Hendren et al., 2015).
Educating ostomates about ostomy care and providing psychosocial support is one of the most important nursing roles for managing physiological and psychological health problems among ostomates (Gemmill et al., 2011; Hendren et al., 2015; WOCN, 2010; Zhang et al., 2013). To carry out these important roles and responsibilities, nurses should have enough knowledge and competence in ostomy care and how to provide ostomates with health education and training about caring for their intestinal ostomies. Literature shows that nurses who were exposed to education and specialised in ostomy care can effectively impact the prevention and management of ostomates' health problems and complications (Gemmill et al., 2011; Hendren et al., 2015; Ontario, 2009; WOCN, 2010; Zhang et al., 2013). Therefore, nurse educators and ostomy nurse specialists (if available) in healthcare settings, including hospitals, should collaborate to provide continuous health education and training programmes for bedside nurses to improve their knowledge and skills about intestinal ostomy care (Hendren et al., 2015; Grant et al., 2013; Gemmill et al., 2011). Also, bedside nurses should be exposed to continuous health education and training programmes that focus on improving their self-confidence and skills in providing teaching and psychosocial support for ostomates and their families.
Unfortunately, there are few certified wound-ostomy nurse specialists and enterostomal therapists in Jordan. So, bedside registered nurses in Jordan have complete responsibility for intestinal ostomy care during the pre- and post-operative phases (Subih and O'Neill, 2012). Bedside nurses are responsible for carrying out health assessments and nursing care for ostomates such as preparing the patient for surgery, routine assessment and management of health problems in the pre- and post-operative phases, and providing teaching and training for ostomates about assessment and management of ostomy-related problems. Therefore, it is essential to improve the curricula of undergraduate nursing programmes in all nursing schools in Jordan to focus on pre- and post-operative care for intestinal ostomies and nursing roles in providing counselling and psychosocial support for ostomates (Subih and O'Neill, 2012). Also, hospitals in Jordan should conduct continuing health education programmes for staff nurses to enhance their knowledge and skills about the updated evidence-based practice for caring for intestinal ostomies. Furthermore, the Ministry of Higher Education in Jordan should establish post-graduate professional programmes in ostomy and wound care specialty in Jordanian universities.
The results of this study showed that only one-quarter of the participants were independent when taking care of their ostomies (all steps) and half of the participants had some assistance from relatives to take care of their ostomies. These results were similar to the previous Chinese study (Cheng et al., 2013). The literature showed that the ostomates with a higher level of knowledge and self-confidence about ostomy care had higher independent self-care abilities and skills to take care of their ostomy and better QOL (including physical and psychological wellbeing) (Cheng et al., 2013; Hu et al., 2014; Mohamed et al., 2017; Simmons et al., 2007). Also, Pearson's correlation results in this study and the results of previous studies showed the association between improving patients' self-care ability to manage their ostomies and reduced ostomy-related health problems and further complications and decreased severity of depression and anxiety (Ayaz-Alkaya, 2019; Cheng et al., 2013; Ran et al., 2016; Recalla et al., 2013; Silva et al., 2017). Therefore, perioperative teaching and training before hospital discharge, continuous health education programmes and follow-up care are recommended for all ostomates to improve their knowledge and self-confidence in their ability to take care of their ostomy, reduce their ostomy-related problems and positively enhance their QOL (Mohamed et al., 2017; Hendren et al., 2015; Grant et al., 2013; Alansari et al., 2018; Berry et al., 2007).
In this study, the participants with permanent ostomy and colorectal cancer who were exposed to education and/or training programmes were more likely to be independent when taking care of their intestinal ostomies. The participants with permanent ostomy and colorectal cancer in this and other studies were more exposed to health education and training due to several visits to healthcare facilities (Mohamed et al., 2017; Nieves et al., 2017; Vonk-Klaassen et al., 2016). Similarly, the previous literature showed that recurrent exposure to teaching and training about ostomy care has significant improvement in patients' knowledge and self-care ability to manage their ostomies (Mohamed et al., 2017; Hendren et al., 2015; Grant et al., 2013; Alansari et al., 2018). Providing perioperative teaching and conducting continuous health education for ostomates after discharge from hospital (including teaching the ostomates in an outpatient setting, patients' home or by telephone follow-up) were significantly associated with improving ostomates' independent self-care abilities and skills in managing their ostomy, reducing ostomy-related problems and complications, enhancing their psychosocial adjustment with the inserted ostomy and promoting their QOL (including physical and psychological wellbeing) (Hendren et al., 2015; Grant et al., 2013; Zhang et al., 2013; Karadağ et al., 2003).
The results of this study show the significant effect of the collaboration of nurses and physicians in teaching and training ostomates about ostomy care and in using more than one teaching strategy to improve participants' self-care abilities to manage their ostomies. Similarly, the literature documented the importance of cooperation between physicians and nurses, specifically the ostomy nurse specialists if available, in providing education and training programmes (Hendren et al., 2015; Grant et al., 2013; Berry et al., 2007; Haugen et al., 2006). Therefore, ostomates' treatment plans in hospital and development of perioperative teaching for ostomates should be carried out through the cooperation of multidisciplinary staff including nurses, physicians and social workers.
The results of this study show the positive effect of using more than one teaching strategy for improving ostomates' ability to take care of their ostomy themselves, particularly through the provision of perioperative teaching and continuous education and training programmes. Similarly, previous studies recommend cooperating with healthcare providers to provide health education and training programmes using all available teaching strategies and resources, such as distributing written and multimedia educational materials, provide perioperative teaching for ostomates and utilising broadcast media and online resources (e.g. websites and social media) to promote their knowledge and self-care abilities and skills to take care of their ostomy (Mohamed et al., 2017; Hendren et al., 2015; Grant et al., 2013; Zhang et al., 2013; Berry et al., 2007).
Study limitations
Using a cross-sectional design does not help identify the cause and effect of the relationship between the variables and cannot assess participants' health problems and self-care abilities and practices to take care of their ostomy over a period of time. Moreover, the use of a convenience sampling method in this study may have resulted in selection bias of the sample beyond the researchers' control. Also, recruiting a sample only from the capital city of Jordan (Amman) affects the generalisation of results to the Jordanian population.
Conclusion
Patients with intestinal ostomies have several physical and psychosocial health problems and negative changes in their daily life activities. Moreover, intestinal ostomy-related problems have a negative impact on ostomates' QOL. The literature showed that physical and psychological wellbeing is negatively affected by a lack of knowledge and self-care ability and skill in ostomy care. Therefore, all ostomates are required to undergo perioperative teaching and continuous health education and training about ostomy management to improve their knowledge and self-care abilities. They are also in need of psychosocial support from their relatives and healthcare professionals. Furthermore, professional follow-up and counselling for ostomates are very important in preventing further ostomy-related problems and complications. The results of this study may be helpful in developing clinical guidelines for the care of ostomates. Also, this study will offer baseline information for further experimental and clinical research about the management of intestinal ostomies.
Key points for policy, practice and/or research
The results show a negative correlation between participants' ostomy-related problems and their self-care abilities to manage their ostomies. The majority of participants intended to participate in continuous health education and training programs about ostomy care. All ostomates should be required to obtain health teaching and training about the assessment and the management of their intestinal ostomy, psychosocial support, and counselling regarding ostomy care to prevent further ostomy-related problems, and improve their self-care abilities. Jordanian hospitals are recommended to develop continuous health educational programs for the bedside nurse to enhance their experience about ostomy care.
Footnotes
Acknowledgements
This publication was supported by the Deanship of Scientific Research at Prince Sattam Bin Abdulaziz University, Al-Kharj, Saudi Arabia. The authors extend their thanks to Dr Omar A Al-Smadi for English editing of this paper. The authors also thank all the participants in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics
Official Institutional Review Board approval was obtained at Al-Ghad International Colleges for Applied Medical Sciences to conduct this current study. Before data collection, ethical approval was obtained from the general medical managers and the directors of nursing at the selected hospitals.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was supported by the Deanship of Scientific Research at Prince Sattam Bin Abdulaziz University, Al-Kharj, Saudi Arabia.