
Abstract
Background
Clinical academics are health professionals who provide direct patient care alongside engaging in health research. Despite the generally agreed consensus that such roles enhance evidence-based care, availability and uptake has been sporadic in non-medical professions. With no data readily available regarding general practice nurses undertaking clinical academic roles, there is a need to understand the barriers and enabling factors that impact general practice nurses considering or pursuing a clinical academic career.
Aims
This review aims to address the question ‘What are the barriers and enablers relevant to general practice nurses in the UK pursuing clinical academic careers?’ by providing an overview of the relevant existing literature and drawing out the implications for policy and practice.
Methods
Literature published in the past 10 years was systematically searched. Using agreed inclusion criteria, papers were first screened on titles and abstracts, with papers included at this stage reviewed as full texts.
Results
Thirteen papers met the criteria for inclusion. The extraction and synthesis of findings allowed for the development of three themes: roles and responsibilities; embarking on a clinical academic career; and organisational research culture.
Conclusions
Findings suggest that infrastructure developments are required across higher education institutions and general practice organisations to bring about a cultural change to equip and empower general practice nurses to consider and pursue clinical academic careers.
Keywords
Introduction
In the UK, clinical academics in nursing, midwifery and allied health professions – or non-medical clinical academics – are health professionals who are engaged concurrently in clinical practice and academia (Council of Deans of Health, 2012, 2018). Such posts allow practitioners to provide direct care and clinical expertise alongside initiating and leading the health research agenda to improve patient outcomes and contribute to teaching the next generation of health professionals (Health Education England, 2015a).
Despite the generally agreed consensus that such roles are essential for high-quality evidence-based care, the availability and uptake of these roles has been sporadic (Carrick-Sen et al., 2016). The proportion of clinical academic roles in the UK for non-medical professionals is less than 0.1% of the workforce, compared with 4.6% of the medical workforce (Baltruks and Callaghan, 2018; Medical Schools Council, 2017). Moreover, it is reported that within non-medical professionals – that is, nursing, midwifery and allied health professions – nurses and midwives are less likely than allied health colleagues to pursue clinical academic careers (Trusson et al., 2019).
Defining nursing research roles
Effective exploration of research roles undertaken by nurses requires understanding of the varied nature of such positions within the profession. The Royal College of Nursing (RCN) broadly categorises nursing research careers as either university-based nursing professors or clinical research nurses (CRNs) (Royal College of Nursing (RCN), 2020). However, this approach is arguably limited due to lacking acknowledgement of nurses employed in academia who do not hold professorial posts. As such, it is beneficial to draw distinction between the role of a CRN and a nurse researcher, with the latter understood as follows: Currently, most nurse researchers are lecturers who are leading research projects as part of their academic job, or carrying out a research study within their current clinical role as part of an academic qualification. (Jones, 2015: 13) Typical functions of clinical research nurse and nurse researcher roles. Source: Adapted from Jones (2015), National Institute for Health Research (NIHR) (2019) and Deave (2005).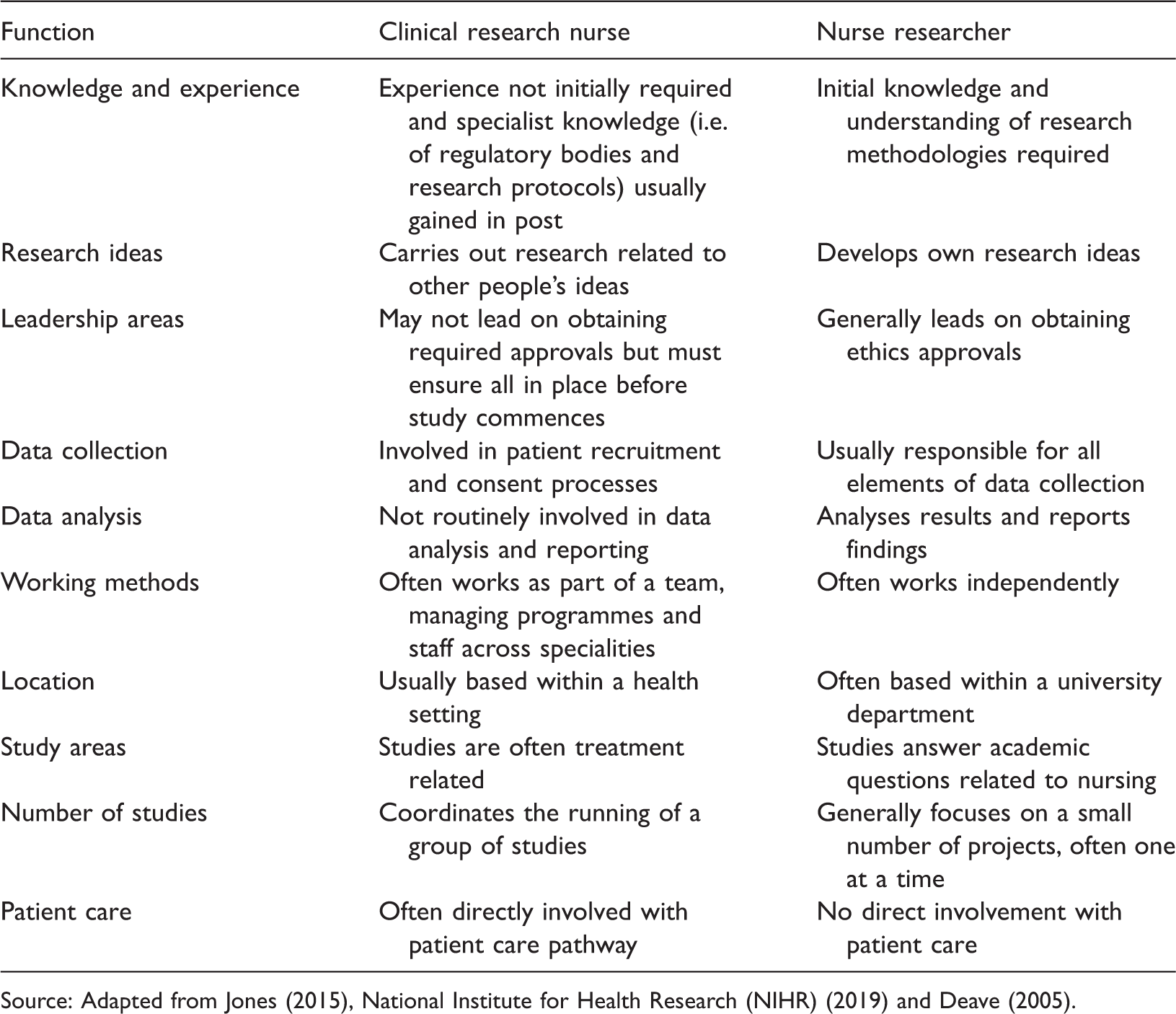
General practice nursing
There are few data on the uptake or availability of research roles for general practice nurses (GPNs), although a recent action plan for general practice nursing reports an intention to increase access to clinical academic careers for nurses working in general practice (NHS England, 2017). The career framework for GPNs published by Health Education England advocates advanced practice at level 8 (Health Education England, 2015b) but does not specifically mention clinical academic roles. There is, however, clear criteria throughout the levels pertaining to the GPN contribution to evidence, research and development.
Based on the low uptake of such roles and experiences across other specialities, there is a need to understand the barriers and enabling factors that will impact on the NHS England (2017) initiative to increase access to clinical academic careers for GPNs. The purpose of this rapid evidence assessment (REA) is to review the existing literature on clinical academic careers for GPNs. All study designs were eligible for inclusion, including quantitative, qualitative and mixed-method papers, along with reviews and editorials. The systematic searching of available literature, combined with the application of strict inclusion criteria, allowed reviewers to produce a list of 13 papers relevant to the research question. From these 13 papers, reviewers were able to extract and synthesise findings in order to develop a number of key themes relevant to the field of clinical academic careers for GPNs. The paper details the processes undertaken in relation to selecting papers for inclusion, along with the methods of data extraction and analysis. Summaries are provided for the 13 included papers for contextual and transparency purposes. The REA concludes with a discussion of the key findings.
This REA addresses the question: ‘What are the barriers and enablers relevant to general practice nurses in the UK pursuing clinical academic careers?’ As such, the REA aims to provide an overview of the existing literature on clinical academic careers relevant to GPNs in the UK, drawing out the implications for those pursuing such career pathways.
Methods
REA methodology
REAs allow for the systematic identification of literature on a particular topic. Utilising simplified components of the systematic review process allows for the creation of new ideas in a timely manner while maintaining necessary levels of methodological rigour (Tricco et al., 2015). Findings are presented in the form of a narrative synthesis, combined in order to ‘tell the story’ (Visram et al., 2016) and form new insights into the topic.
Search strategy
Literature searches were conducted using the following search terms: [(‘general practice’ OR ‘practice’ OR ‘GP’ OR ‘G.P.’) AND nurs* AND (academic OR research*) AND career]. The following electronic databases were searched in February 2019 for records published within the past 10 years. The databases searched were Cumulative Index of Nursing and Allied Health Literature (CINAHL); PubMed; Scopus; Web of Science. Hand-searching of relevant websites was also carried out (Royal College of Nursing (https://www.rcn.org.uk/); Nursing and Midwifery Council (https://www.nmc.org.uk/); Health Education England (https://www.hee.nhs.uk/); Department of Health and Social Care (https://www.gov.uk/government/organisations/department-of-health-and-social-care).
The inclusion criteria for papers were: any study/review/discussion design; published in English from 2009 onwards; related to UK nurses engaging in research activities or pursuing clinical academic careers. The REA excludes books, book reviews, conference proceedings, academic posters and dissertations/theses.
The first author conducted the initial search for papers and carried out the initial screening on titles and abstracts using the above inclusion criteria. The second and third authors reviewed a random 10% sample and disagreements were resolved by consensus. The second screening – full text screen – was completed by all authors using the same inclusion criteria, with disagreements again resolved by consensus. Papers included from the second stage were then analysed for inclusion in the narrative analysis.
Analysis and synthesis
Papers included in the REA were subject to a thematic analysis (Braun and Clarke, 2006). This process involved coding the included papers by line/paragraph (level 1 findings). Codes were then grouped into descriptive categories on the basis of similarity in meaning (level 2 findings), with these categories then subject to a meta-synthesis in order to produce a single comprehensive set of synthesised findings (level 3 findings). This process was undertaken independently by the first and second authors and findings quality assured and explored by means of discussion with the third author.
Findings
Figure 1 summarises the papers identified from searching, along with those included and excluded during the first and second screenings.
Rapid evidence assessment (REA) process from literature search to inclusion (adapted from the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram (Moher et al., 2009)).
Characteristics of papers included in the rapid evidence assessment.

The 13 papers included in the study used a variety of terms to refer to nurses who engage in research activities. In line with the terminology outlined at the beginning of the REA, the following three terms are used in this section: ‘clinical research nurse’ (CRN) relating to those involved in clinical trials; ‘nurse researcher’ relating to those undertaking small-scale independent research alongside teaching responsibilities or clinical practice; and ‘clinical academic’ relating to those undertaking a dual role as a nurse and an academic, often based within a university. It is relevant to note that only two of the included papers explicitly refer to general practice nursing (Boase et al., 2012; Jolin, 2010).
Papers that met the inclusion criteria for the REA were subjected to a process of thematic analysis which revealed three main themes: (a) role and responsibilities; (b) embarking on a clinical academic career; and (c) organisational research culture.
Role and responsibilities
Over half the included papers stated that nurse involvement in research improves healthcare practice and patient outcomes (Boase et al., 2012; Boulton and Hopewell, 2016; Bowrey and Thompson, 2014; Clark et al., 2016; Kunhunny and Salmon, 2017; Nicholson, 2016; Rose and Tuffrey-Wijne, 2017). However, the varied nature of nursing research posts results in unclear role definitions, which as a result can be confusing and problematic in terms of workload allocation and specific responsibilities (Boulton and Hopewell, 2016). Exploration of this topic within the included literature largely focuses on the responsibilities of CRN roles, with discussion of GPN research roles limited to involvement in clinical trial organisation, delivery and patient recruitment (Boase et al., 2012; Jolin, 2010).
CRN roles are reported to be particularly varied and incorporate a large number of duties; for example, people and financial management, professional networking, administering drugs, collecting samples and writing reports (Bowrey and Thompson, 2014; Fawcett and McCulloch, 2014; Kunhunny and Salmon, 2017). In addition to adding a ‘patient experience’ element to studies not typically present in medical research (Fawcett and McCulloch, 2014), it is also suggested that effective practice in a CRN role requires a level of autonomy different to that in clinical nursing roles (Kunhunny and Salmon, 2017).
For nurses involved in clinical trials, whether as a GPN or CRN, it is suggested that a specific skillset is required. These skills include effective administrative skills such as record keeping and data entry (Jolin, 2010; Kunhunny and Salmon, 2017), knowledge of the research process and associated legislation and guidelines (Fawcett and McCulloch, 2014), along with critical thinking and problem-solving skills (Kunhunny and Salmon, 2017). Brady (2017) reported that some of the skills needed by nurses pursuing a clinical academic career are naturally developed through general clinical practice.
Role challenges
Across the varied research roles undertaken by nurses, a number of challenges are consistently reported. For example, nurses are reported to experience competing loyalties between clinical and research agendas (Boase et al., 2012; Murphy, 2014), along with conflicts between continuity of research or clinical care when performing a combined role (Bowrey and Thompson, 2014; Kunhunny and Salmon, 2017). These issues may be exacerbated by time constraints, highlighting a need for protected time for specific duties (Boase et al., 2012; Coombs et al., 2012; Kunhunny and Salmon, 2017). Jolin (2010) provided an example of this by emphasising the importance of nurses involved in research devoting time to ensuring clinical skills remain up to date.
Boase et al. (2012) discussed challenges faced by GPNs working on clinical trials: recruiting patients is time-consuming; clinical trials often result in a larger workload than anticipated, resulting in feelings of being overwhelmed; unfamiliar language/jargon; insufficient training; and following a trial protocol, which can feel unnatural or difficult with patients with whom a relationship already exists.
Feelings of isolation experienced by nurses involved in research were reported in several papers; for example, by those working in a smaller research study due to no longer being a member of a larger clinical team (Bowrey and Thompson, 2014), by those working remotely from a central research team (i.e. a GPN involved in a clinical trial) (Boase et al., 2012), and more generally due to the ambiguity of nursing research roles and the feelings of exclusion this can incur (Kunhunny and Salmon, 2017). It was also reported that nurses may experience resentment from non-research colleagues (Boase et al., 2012; Kunhunny and Salmon, 2017).
Embarking on a clinical academic career
There is a poor awareness of research roles and careers among the nursing community (Jones-Berry, 2016) and research is often not seen as a viable career path by many nurses (Brady, 2017). It is reported that moving from patient care into a CRN post can be daunting (Brady, 2017), and many nurses experience a ‘crisis of confidence’ that prevents them pursuing a research-related nursing post (Murphy, 2014), including a clinical academic career (Jones-Berry, 2016). In addition, newly or recently qualified nurses reportedly do not feel a research career is available due to a perceived pressure to gain clinical experience before embarking on a clinical academic career (Fawcett and McCulloch, 2014). As such, nurses are significantly less likely to undertake postgraduate study and consequently are underrepresented as clinical academics compared with other non-medical professions (Clark et al., 2016; Jones-Berry, 2016). It is also suggested that the availability of formalised dual research and clinical roles is low (Rose and Tuffrey-Wijne, 2017).
Nurses considering a clinical academic career are advised to identify local research networks and familiarise themselves with local and national guidance on clinical academic careers (Clark et al., 2016; Nicholson, 2016). Nicholson (2016) also suggested that nurses wishing to enter research roles should consider undertaking the following activities: shadow research-active colleagues; explore postgraduate study options (e.g. a MRes degree); publish articles (e.g. undergraduate dissertation); and seek out specific training courses to address areas for development. Nurses are also encouraged to explore research nurse job descriptions and person specifications to identify transferable skills as well as areas for development (Brady, 2017; Nicholson, 2016). Rose and Tuffrey-Wijne (2017) also stated that nurses should explore secondment opportunities to gain first-hand experience of engaging in research activities.
Organisational research culture
It is reported that there are difficulties recruiting nurses to research roles, particularly given the general shortage of nurses in the UK (Boulton and Hopewell, 2016; Bowrey and Thompson, 2014; Brady, 2017). As a result research posts open to nurses are often filled by clinical trial practitioners (Brady, 2017). This issue is heightened by the lack of research training offered to nurses during undergraduate training (Jones-Berry, 2016), resulting in student nurses not being inspired to pursue a clinical academic career (Kunhunny and Salmon, 2017).
Understanding of the value of nurses involved in research is reportedly poor (Coombs et al., 2012), particularly among NHS management (Kunhunny and Salmon, 2017; Murphy, 2014). This is accompanied by a lack of research leadership for nurses (Murphy, 2014) and a general absence of research competencies featuring in the nurses’ professional development planning (Boase et al., 2012). As a result, nurses find themselves in a culture in which expectations that they should undertake research are low (Murphy, 2014).
Several of the included papers state that effectively undertaking research requires the support of the whole clinical team (Bowrey and Thompson, 2014; Jolin, 2010), particularly given the benefits for general practice in terms of profile-raising and funding (Boase et al., 2012; Kunhunny and Salmon, 2017). Some GPNs who undertake research duties with no additional pay felt this was unfair (Boase et al., 2012). It is suggested that health organisations require infrastructures that allows for protected research time (Murphy, 2014), along with mentors or ‘buddies’ for staff new to research (Murphy, 2014; Nicholson, 2016).
Discussion
The purpose of this REA was to review the barriers and enablers relevant to GPNs in the UK pursuing a clinical academic career. The literature related specifically to GPN engagement with research is limited, with only two of the included papers specifically discussing this (Boase et al., 2012; Jolin, 2010). These two papers focus on GPN engagement in specific research activities and as a result no paper included in the study pertains to GPNs undertaking clinical academic careers. However, despite the dearth of research specific to this topic, themes derived from the identified literature are pertinent to the exploration of clinical academic careers for GPNs.
Findings suggest that the involvement of nurses in research has a number of benefits, such as improved healthcare and patient outcomes (Boase et al., 2012; Boulton and Hopewell, 2017; Bowrey and Thompson, 2014; Clark et al., 2016; Kunhunny and Salmon, 2017; Nicholson, 2016; Rose and Tuffrey-Wijne, 2017). Despite this, the value of nurses pursuing clinical academic careers is not widely understood (Coombs et al., 2012; Kunhunny and Salmon, 2017; Murphy, 2014), which perhaps offers an explanation as to why nurses do not view research as a feasible career path (Brady, 2017). The underrepresentation of nurses as clinical academics compared with other non-medical professions may also be due to lower levels of postgraduate study by nursing professionals (Clark et al., 2016; Jones-Berry, 2016) and a general lack of research training during undergraduate studies (Jones-Berry, 2016; Kunhunny and Salmon, 2017). This is particularly relevant to general practice nursing; the profession has an aging workforce (Ipsos MORI, 2017) and GPNs approaching retirement are perhaps less likely to embark on a career change by undertaking the research training or experience necessary for clinical academic posts.
In addition to these challenges to embarking on a clinical academic career, the literature also highlights some of the difficulties experienced by nurses while performing research roles. The most significant challenge is reported to be competing agendas between research activity and clinical duties (Boase et al., 2012; Bowrey and Thompson, 2014; Kunhunny and Salmon, 2017; Murphy, 2014), which is likely to be exacerbated by the unclear role definitions discussed by Boulton and Hopewell (2017). Given that many GPNs feel their profession is often misunderstood (Glaze, 2019), moving into a role with comparable challenges is unlikely to appeal. Moreover, opportunities to pursue clinical academic roles may be potentially more limited for GPNs, with unique barriers and facilitators due to the independent contractual status of GP practices.
Nurses undertaking research, whether as a CRN or nurse researcher, are reported to require a specific skillset in addition to clinical knowledge and experience; for example, effective administrative skills (Jolin, 2010; Kunhunny and Salmon, 2017) and knowledge of research processes (Fawcett and McCulloch, 2014). As discussed, nurses receive limited research training while completing pre-registration courses (Jones-Berry, 2016; Kunhunny and Salmon, 2017). This lack of exposure denies nurses the opportunity to develop necessary research skills and knowledge, which in turn may prevent individuals from considering research, specifically clinical academic roles, as a viable career path.
Collectively, these factors are likely to foster the culture discussed in the literature – that is, one in which expectations of research activity by nurses are low. Consequently, many nurses do not consider research a realistic or attainable career path, despite many of the skills required to pursue a clinical academic career being naturally developed through clinical practice (Brady, 2017). However, the value and transferability of these skills is likely to remain largely unacknowledged as nurses are rarely encouraged during the early stages of their career to consider such a career pathway. Similarly, the options given by Clark et al. (2016) and Nicholson (2016) for nurses wishing to improve their knowledge of research and explore clinical academic careers – for example, liaising with local research networks and shadowing research-active colleagues – are unlikely to be of interest without an organisational cultural shift. Such a change would encourage and inspire nurses from the point of pre-registration training and through ongoing continued professional development to consider a research-related career and potentially increase the number of nurses, including GPNs, pursuing a clinical academic career.
Implications
There are a number of implications arising from this REA. Findings suggest a cultural change is required within universities and NHS organisations to empower nurses to develop research skills, knowledge and experience. Embedding a ‘research culture’ during pre-registration training would enhance awareness of a potential career pathway that at present is generally not considered by much of the profession. In line with this, it would be advantageous for organisations that employ nurses to incorporate the option of research activities into continued professional development to allow for exploring the nature of research posts, particularly the unique and dual nature of clinical academic roles. Moreover, a commitment to promoting the value of clinical academic careers actively for GPNs, from relevant stakeholders such as the Royal College of Nursing and the Queen’s Nursing Institute, may encourage organisations to support nurses to explore and pursue such career pathways. The development of a ‘typical’ role profile for GPN clinical academics would also serve to promote this area of practice. It is also recommended that further research is undertaken on the topic of GPN clinical academic careers as a means to understand the barriers and facilitators unique to this specific area of nursing practice in the UK.
Limitations
The limited timeframe associated with REAs does not allow exhaustive searching, increasing the likelihood of publication and selection bias (Ganann et al., 2010). Included studies were not subject to critical appraisal; all papers that met the inclusion criteria were included.
However, transparency was ensured by a clear search strategy and as a result provides a robust overview of the literature available on this topic. The limited number of papers related to GPN engagement in research is attributed a general lack of exploration of this topic in UK-based academic literature.
It is also pertinent to add that no papers included in this review were published after the release of ‘General practice – developing confidence, capability and capacity: a ten point action plan for general practice nursing’ (NHS England, 2017). This document is the driver for renewed commitment to the development of clinical academic roles specifically for GPNs and should facilitate focus on addressing the current barriers.
Conclusions
This REA sought to explore the barriers and enablers relevant to GPNs pursuing clinical academic careers. Despite no papers identified by the literature search being specific to GPN clinical academic careers, findings generated by the thematic analysis of included papers provided useful and relevant information to begin exploring this seemingly unexplored topic. Findings indicate the existing literature regarding nurse engagement with research in general is limited, perhaps due to the small number of nurses performing such roles. Possible reasons for the limited uptake of clinical academic posts are discussed, with the cumulative effect of these factors likely to result in the continued underrepresentation of GPNs and the wider nursing profession in the clinical academic workforce. To address this, a cultural shift and a change in attitudes and understanding is required across higher education institutions and NHS organisations, with further research necessary to explore and facilitate this.
Key points for policy, practice and/or research
The value of general practice nurses pursuing clinical academic careers is not widely understood. Opportunities for pre/post-registration nurses to build research skills and knowledge are limited. Nurses undertake less postgraduate study compared with allied health professionals and report a lack of research training during undergraduate studies. General practice nurses would benefit from the incorporation of research activities into ongoing continued professional development.
Footnotes
Acknowledgements
The author(s) would like to thank NHS Birmingham and Solihull Clinical Commissioning Group for supporting the completion of this review.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethics
Ethics approval is not required as this was a desk-based study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by NHS England (Ref No. PNF2872). This programme of work was undertaken as part of a commission from the NHSE/I GPN 10 Point Plan programme action 8 which looks at the development of clinical academic careers.