
Abstract
Background
Research active hospitals have better patient outcomes and improvements in healthcare are associated with greater staff engagement in research. However, barriers to research activity include inadequate knowledge/training and perceptions that research is a specialist activity. Nursing is an academic discipline but the infrastructure supporting nursing research worldwide is variable and sustaining clinical academic careers remains challenging. The National Institute of Health Research 70@70 Senior Nurse Research Leader programme provides dedicated time to increase clinical academic opportunities and foster a research culture across England; we describe initiatives developed by one National Institute of Health Research 70@70 leader to increase clinical staff engagement in research.
Aim
The purpose of this work was to develop initiatives to facilitate clinical research opportunities and bridge the gap between clinical care and research.
Methods
New strategies were developed in one health service to increase clinical staff engagement in research activity. This included: (a) Chief Nurse Research Fellows: clinical staff undertaking bespoke research training to identify local clinical research priorities, (b) an exemplar nurse-led Embedding Research In Care unit to pioneer innovation, evaluation and research participation supported by a research facilitator and (c) a Clinical Academic Network for nursing, midwifery and allied healthcare professionals to aid collaborative working.
Results
The first cohort of Chief Nurse Research Fellows have successfully completed a bespoke training programme and, with mentoring, developed projects to tackle clinical problems. The Embedding Research In Care unit initiative was configured and the first Embedding Research In Care unit has been awarded. A Clinical Academic Network group of 25+ nurses, midwives and allied health professionals was established and provides peer support and mentoring.
Conclusions
This multi-faceted approach has successfully supported research training/engagement, enabled career development and identified nurses/midwives with potential to undertake clinical academic careers. A range of strategies, such as those described in this paper, are required to successfully bridge the gap between clinical care and research and provide additional opportunities for clinical staff to become engaged in a research active career.
Keywords
Introduction
Nursing has been an academic discipline for decades but the infrastructure for nursing research in many countries is still limited and nurses often have difficulties developing or sustaining careers in nursing research due to lack of career opportunities (Hafsteinsdóttir et al., 2017) and limited understanding of clinical-academic roles (Carrick-Sen et al., 2019). The need to strengthen the infrastructure for nursing research and develop supportive leadership and mentor programmes for nurses to enable research activity and ensure optimal evidence-based, high-quality care for patients has been recognised (de Lange 2019) along with the need for peer support (Al-Nawafleh et al., 2013). However, access to such provision is variable and institutional or organisational barriers may directly or indirectly impact on the development of research productivity (Al-Nawafleh et al., 2013). Organisational barriers may prevent academic nursing from functioning as a true partner in healthcare with clinical academics frequently located in higher educational institutes rather than healthcare settings, with missed opportunity for partnership despite a desire to develop relationships and dynamic visions for academic nursing (American Association of Colleges of Nursing (AACN), 2016). Insufficient resources are a further barrier to supporting significantly enhanced roles for academic nursing (AACN, 2016, Albert et al., 2019). Additional barriers often cited include funding and clinical/research time constraints with key drivers for success comprising strong and strategic clinical academic leadership and effective partnership working (Henshall, 2021).
There is a positive association between engagement in research by healthcare organisations and improvements in healthcare performance (Boaz et al., 2015) and a significant association between clinical research activity, academic output and reduced patient mortality (Bennett et al., 2012; Ozdemir et al., 2015). The relationship between nursing education and research with quality patient outcomes is clearly recognised (Henderson and Winch, 2008), with academic-clinical collaborations promoting a culture that challenges the status quo (Albert et al., 2019). Combining clinical practice and academic work facilitates the integration of research findings for high-quality patient care, however establishing clinical academic careers for nurses remains a challenge (van Oostveen et al., 2017). For clinical academic research to flourish the development of staff who understand the importance of research and innovation and the role of an embedded research culture is key (Olive et al., 2020). Culture change is required with evidence of leadership that promotes and enables a combination of research, teaching and clinical practice with infrastructure to support clinical academic career pathways for nurses (van Oostveen et al., 2017). Research active clinical environments have been developed by linking experienced researchers with healthcare professionals within clinical settings (Holzhauser et al., 2008); however sustainability of such partnerships relies on shared goals, contributions and resources (Albert et al., 2019).
There is growing evidence for the impact of mentoring in aiding career development and supporting nurses to provide optimal evidence-based, high-quality care for patients (de Lange et al., 2019; Hafsteinsdóttir et al., 2020). Mentoring has positively influenced research productivity, career development, leadership skills, work culture and collaboration, and is essential in supporting ongoing research activity (Hafsteinsdóttir et al., 2017). The Dutch Leadership Mentoring in Nursing Research programme is one example, developed specifically to increase the cadre of nurse scientists, strengthen nursing research within universities, and improve the career development of postdoctoral nurses (Hafsteinsdóttir et al., 2020). Research mentor programmes have demonstrated increased confidence amongst participants for research leadership roles and pursuit of research and quality assurance projects (Fry and Dombkins, 2017). Building researcher skills within the clinical workforce will better support quality healthcare and the examination of everyday practice. Opportunities for building research networks and role modelling the value and importance of research to practice and quality improvement is key to developing a research culture with clinical leadership and research networks that strengthen workforce capacity (Fry and Dombkins, 2017).
Chief Nurse Fellowships have previously developed the foundational clinical and academic skills of frontline junior clinical staff, through bespoke development programmes, improvement projects and clinical/academic mentorship (Bramley et al., 2018). Similar schemes outside the UK provide examples of fellows completing programmes where they are supported to develop leadership skills, develop independent research and establish research collaborations (Hafsteinsdóttir et al., 2020). Such fellowships were used as models for the Chief Nurse Research Fellows (CNRFs) described below.
Practice Development Units (PDUs) are examples of nurse-led centres for pioneering, evaluating and disseminating innovative practice and facilitating the professional development of healthcare staff (Gerrish, 2001). PDUs have been associated with having a positive influence on multidisciplinary team working, evidence-based practice and improving opportunities for professional development (Bray et al., 2009). They establish cross-organisational structures and processes that facilitate the integration of clinical knowledge and research methods, to enhance clinical practice (Henderson and Winch, 2008). A number of factors have been recognised to influence the success of PDUs in particular: the role of the clinical leader, the motivation and commitment of the team members, financial resources and the nature of support from managers and medical staff (Gerrish, 2001). The importance of embedding processes and outcomes for practice development in corporate strategy is emphasised (McCormack et al., 2013). Progress is dependent on all those involved and sharing common goals in the implementation of evidence-based healthcare (Wright, 2001). The principles of these models have been used as a framework for the development of the nurse-led ‘Embedding Research In Care’ (ERIC) units described below.
The National Institute of Health Research (NIHR) 70@70 programme was set up in 2019 with the aim of strengthening the research voice and influence of nurses and midwives in health and social care settings. Seventy senior nurse/midwife research leaders from across England were appointed to lead local research engagement, strengthen nurse/midwife contribution to research delivery and facilitate clinical academic pathways. The appointment of MS as one of the NIHR 70@70 cohort provided dedicated time, 2 days per week for 3 years, to realise the aim of developing a range of initiatives to strengthen the nursing voice in research and bridge the gap between research and clinical care.
Method
A vision for nursing, midwifery and allied healthcare professional (NMAHP) research was developed which involved a multi-faceted approach with a range of strategies designed to bridge the gap between research and clinical care. Based on the success of Chief Nurse Fellows and PDUs elsewhere we adapted these models with a primary focus of increasing research awareness and research activity within clinical care.
Chief Nurse Research Fellows (CNRFs)
The Royal Devon and Exeter NHS Foundation Trust professional development plan considers the spectrum of care from core to advanced practice, striving for excellence with safety and compassion alongside continuous improvement. The purpose of the plan is to ensure a workforce that is fit for the future, responds flexibly to change and maximises service excellence. One area within the plan specifically aims to increase awareness through learning opportunities including research and the establishment of chief nurse fellow roles. We met with the Royal Devon and Exeter NHS Foundation Trust’s Chief Nurse and other senior nurse leaders to discuss the vision of developing CNRF roles within the Trust. External funding was secured to support secondments to the roles for 1 day per week for 6 months and the opportunities advertised via the Trust Intranet. Applicants were asked to send in expressions of interest and interviews were conducted by MS, RE and the Chief Nurse. A bespoke training plan was developed to include sessions on: research methodology, local research studies, R&D governance, research ethics, patient and public involvement and engagement (PPIE), the role of the Clinical Research Network and Clinical Research Facility, the Research Design Service, literature searching, funding opportunities, designing programmes of research and other NMAHPs from across the region at various stages of a clinical academic career providing details of their research journey. Links to the organisation’s clinical research nurses were provided with planned opportunities to shadow research study recruitment and delivery. In addition access to online research training and participation at regional research events was provided. The CNRFs were guided to network and establish links with clinical academics elsewhere who were conducting research within a similar area of interest. Individual guidance was given to help the CNRFs develop projects in their own areas around a specific clinical problem, which they had identified. The CNRFs had the opportunity to present their projects to the local Patient and Public Involvement (PPI) group and gain feedback which enabled them to amend and improve their projects. The Trust's communication team was involved in promoting the initiative and uploading updates and vlogs on the hospital Intranet to raise awareness.
Embedding Research In Care (ERIC) unit
An iterative consultation process was developed and meetings held with a range of senior staff members across the organisation (Figure 1). Initial discussions were held with the Chief Nurse and Deputy Chief Nurse who were enthusiastic about the initiative and suggested strategies for engaging and gaining ideas from other staff members. The vision for developing ERIC units was then conveyed to the Joint Professional Forum: a multi-disciplinary group of lead nurses, midwives, allied healthcare professionals and the Head of Professional Development. Ideas and contributions were collated and discussed with the matrons within the organisation, the Clinical Academic Network (see below) and clinical research teams. Consensus was reached with the aim for the ERIC to become a centre for pioneering, evaluating, disseminating innovative research practice and facilitating staff development using a framework for change. The vision would encourage all staff within the department to become engaged with research and increase research activity, identifying local clinical problems, which could be developed into potential research projects. The vision would integrate research within clinical care, ensure the clinical staff were knowledgeable about local research studies and enable more patients to access research thereby improving patient experience. Consultation process to develop Embedding Research In Care (ERIC) unit model. Allied Health Professional (AHP).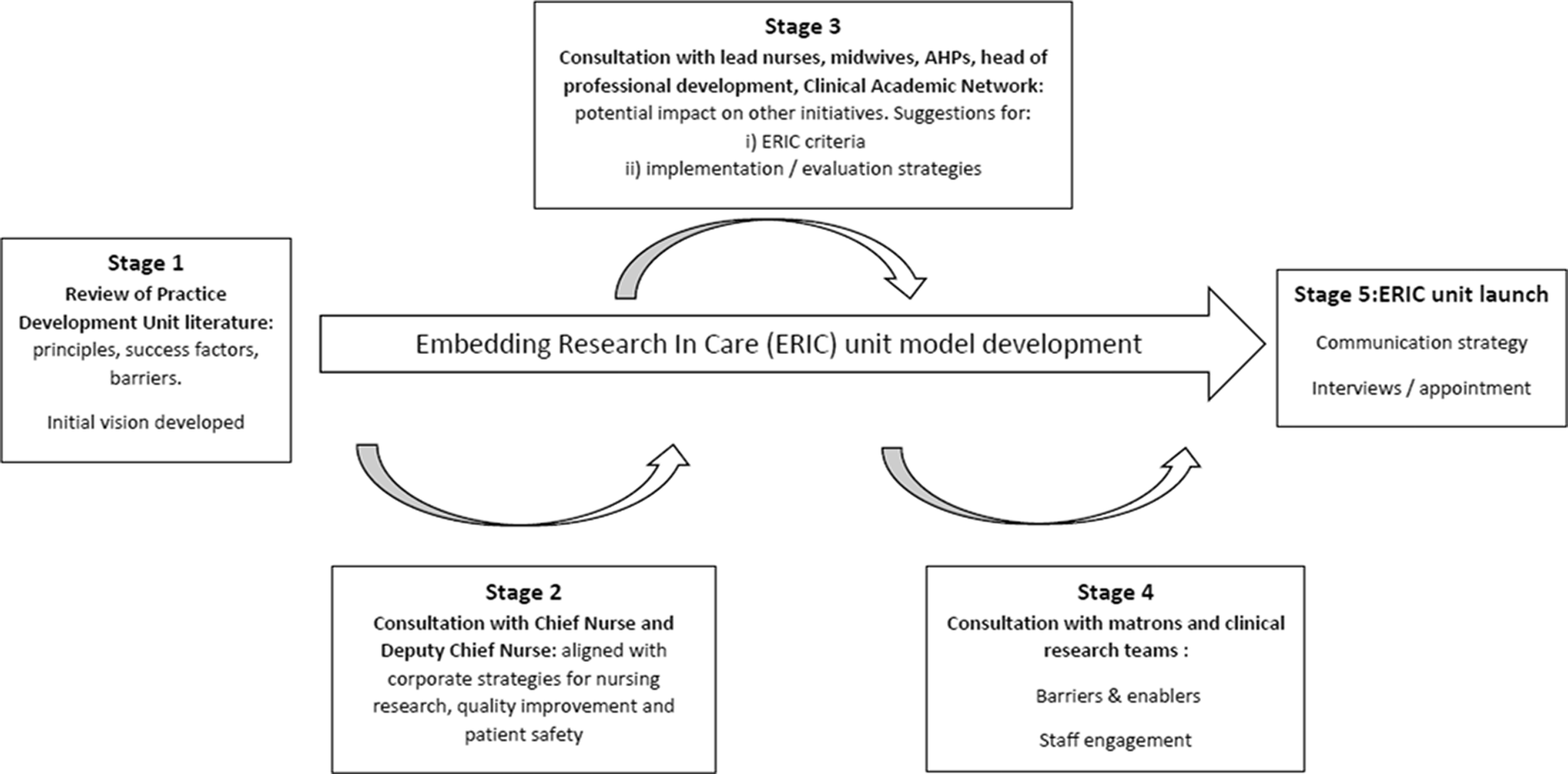
This new initiative was communicated widely via the organisation's Intranet and teams interested in obtaining more information were encouraged to contact MS and attend an information session. This meeting was convened to discuss the initiative with interested departments across the organisation. Applications were encouraged to indicate: why they wanted their area to become an ERIC unit, what research currently takes place on their unit, how this could increase by becoming an ERIC unit, the anticipated role of clinical leaders within the unit, motivation and commitment of staff team and support from managers/medical staff. Interviews were held with MS, RE, HQ and the Chief Nurse, and teams applying were encouraged to ensure a wide attendance of staff from varying disciplines from their departments.
Research Facilitator
A new role of a Research Facilitator has been developed to provide support, research expertise and guidance to the ERIC unit 1 day per week for 12 months initially. A job description has been agreed, expressions of interest requested and interviews conducted by MS and RE. This post provides a new, exciting possibility for an experienced clinical research nurse to develop skills and increase research engagement within a clinical team. External funding was gained to support this new role. The Research Facilitator will be a key member of the team enabling/increasing research activity within the units by working directly with clinical staff, upskilling clinically-based nurses in research, identifying priorities for research within the units, highlighting opportunities for research training, facilitating links with the research teams, chief investigators and R&D colleagues.
The Research Facilitator will undertake a role as lead practitioner and coordinate, monitor and increase patient participation in local/national research in line with performance and monitoring metrics, promoting research opportunities for patients, inspiring nurses within the units to develop their own research and ensuring optimum delivery of clinical research and identifying clinical priorities for new research. The Research Facilitator will be line-managed by MS and will also be supported by RE and HQ.
Clinical Academic Network
A Clinical Academic Network group was set up to link NMAHPs across the Trust who were interested in or already undertaking their own research. The vision was to provide a collaborative network of individuals who could provide peer support or mentoring to each other, share experiences including developing research proposals or applying for funding. Not all those interested in a clinical academic career were working in research-active departments and the group provides a forum to increase networking opportunities and link like-minded colleagues together. The group also has the opportunity to review and comment on strategies planned or developed within the Trust to increase research activity and awareness amongst NMAHP colleagues.
Results
The development of these initiatives is complementary and part of a wider NMAHP research strategy. The interconnection of the CNRFs, ERIC units and Research Facilitator with the wider research team can be seen in Figure 2. Interconnection of the Chief Nurse Research Fellows (CNRFs), Embedding Research In Care (ERIC) units and Research Facilitator with the wider research team. NIHR: National Institute of Health Research. MDT: Multi-Disciplinary Team.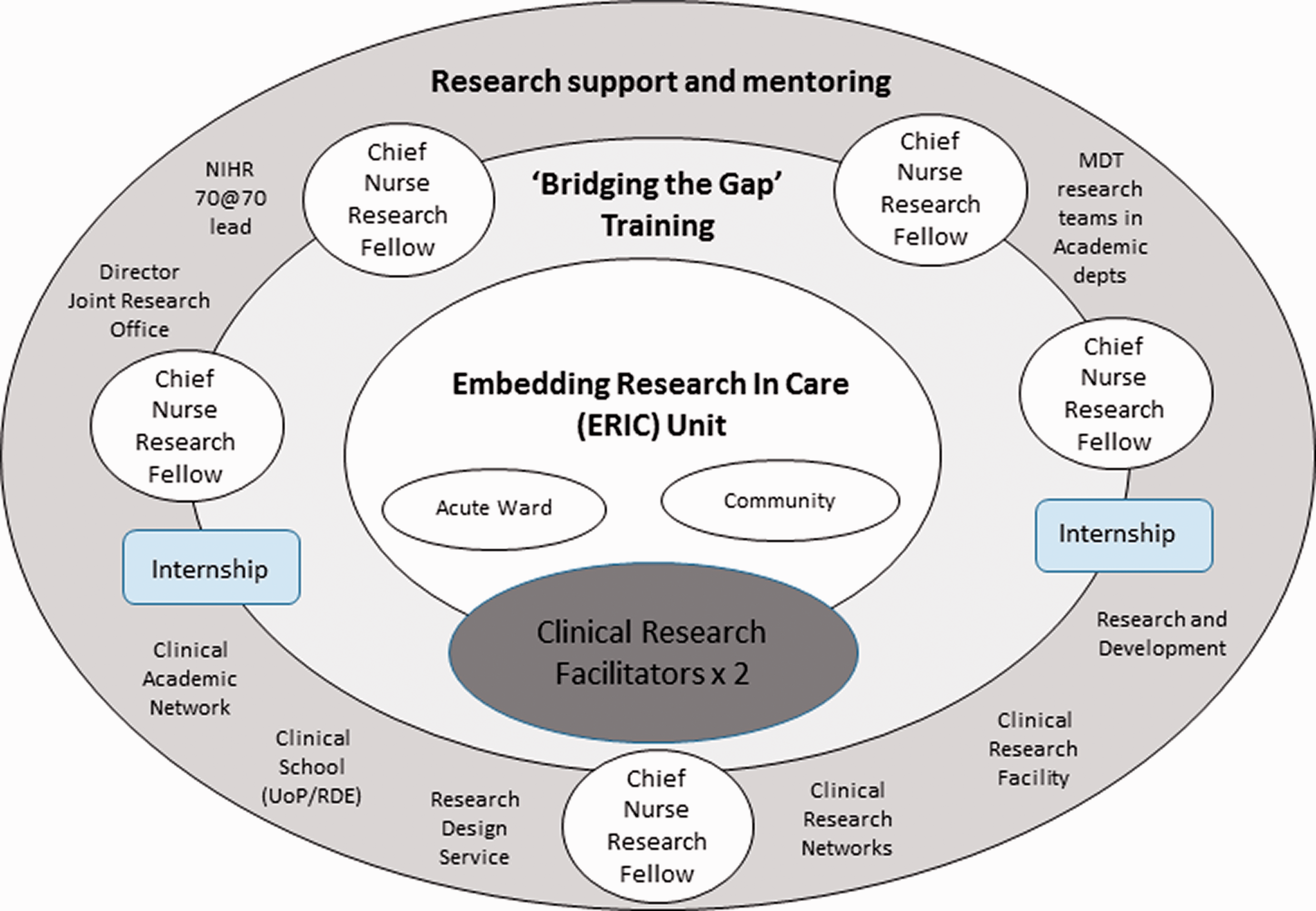
Chief Nurse Research Fellows (CNRFs)
After a Trust-wide application process, five healthcare professionals were seconded 1 day per week for 6 months as CNRFs. These included; a community physiotherapist, a community midwife and three hospital-based nurses – working in the neonatal unit, gastroenterology and stroke sections. Initial assessments of research experience were conducted using the Spider instrument (Smith et al., 2002) and reassessed at completion of the secondment. All actively engaged with the initiative and completed the six-month secondment with one gaining promotion to a new role during this period. Fellows were able to link with clinical research nurses within their own areas of interest and gain insight into research studies being conducted within the organisation. They contributed to Trust communications highlighting their activity within the secondment through vlogs. Projects developed included: Use of virtual reality as an aid to increase activity in people with type 2 diabetes Evaluation of telephone triage within midwifery services Evaluation of the use of pain assessments during procedures with neonates within the clinical environment Establishing patients with inflammatory bowel disease perspectives of teleheath Identifying nurses perceptions of their role within rehabilitation of patients within the stroke unit
Developing the projects required gaining new skills in a number of areas including: literature searching and questionnaire design as well as making new links with colleagues in the audit departments, governance leads and pitching their proposals to a local PPI group. The projects undertaken may lead to changes in local practice or the development of future funding applications.
Initial assessment of research experience and knowledge was undertaken as a self-assessment by each CNRF using the Spider instrument (Smith et al., 2002) and repeated at the end of the six-month secondment (Figure 3). Mean scores increased from 1.76 (no experience/little experience) at baseline to 3.2 (some experience) at 6 months. Spider scores before and after the six-month fellowship.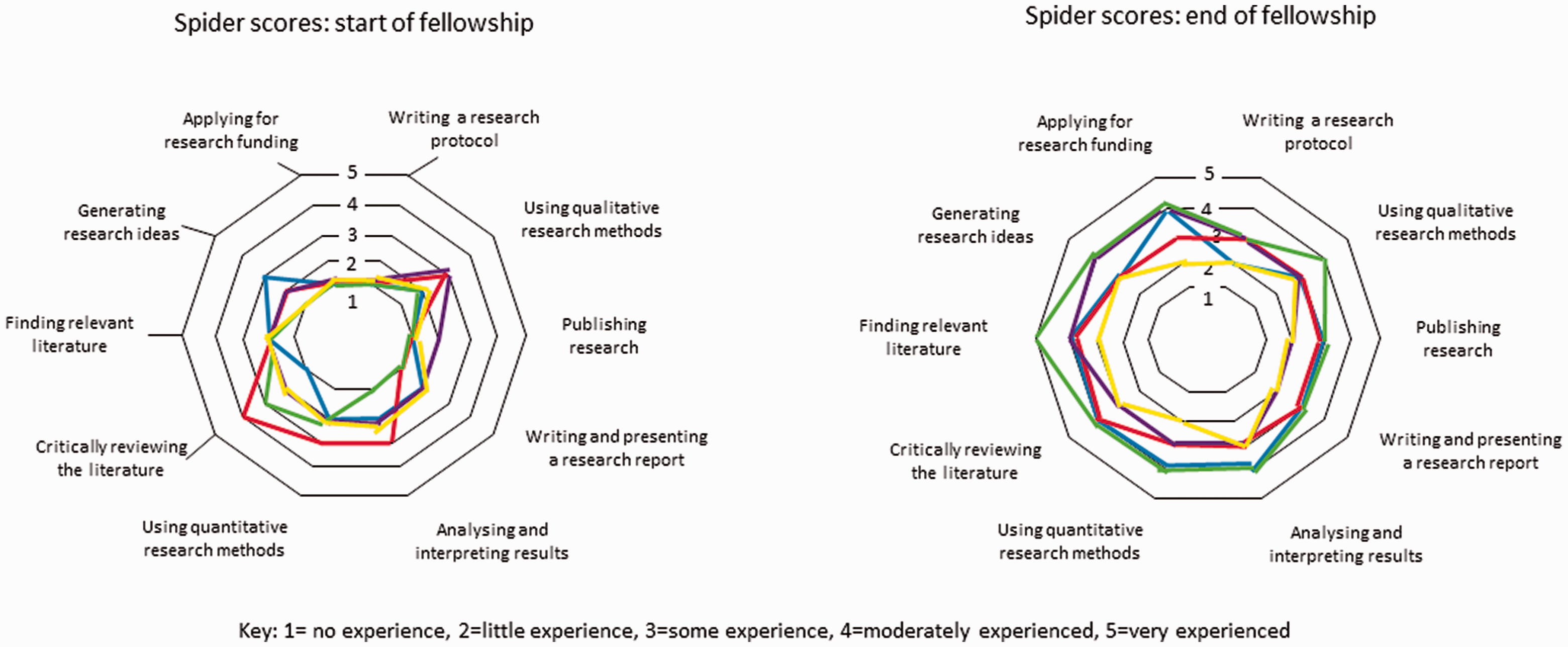
Formal qualitative evaluation from the CNRFs regarding the initiative indicated the training component increased their knowledge of research: ‘The CRNF role has had a huge impact on my development, I have learnt a vast amount’ (CNRF1). The mentoring provided was perceived to be positive and influential in terms of the CNRFs' future aspirations: ‘The mentoring from MS and RE has been encouraging. They have inspired me to pursue a career in research’ (CNRF2). Some of the CNRFs were motivated to progress to become clinical academics in the future and gained confidence in how to achieve this through the secondment: ‘It has cemented my vision further in becoming a clinical researcher... this programme has sparked further enthusiasm to take the next step... I feel clearer on what to do next and who I can ask for support’ (CNRF3). Others were keen to influence clinical practice through research: ‘It has given me a drive and passion to try and implement change through research within my profession’ (CNRF1) or seek ongoing funding to undertake further research: ‘I have been inspired by both the programme mentors and other speakers to seek further funding to develop my research portfolio’ (CNRF2)
While developing their projects during the secondment, accessibility to a local PPI group was considered particularly helpful: ‘The PPI group work was a great learning opportunity to further understand research and… really helped me to focus my research idea’ (CNRF2). The CNRFs believed the projects they had developed would have a positive impact which would benefit patients: ‘I feel excited about the progression of my project and can see it making a real difference for the patients I care for’ (CNRF4). They considered the projects would also increase staff contentment: ‘The research idea I have focused on will hopefully improve not only patient care but also midwifery and patient satisfaction’ (CNRF1). The CNRFs were able to meet other clinical academics through the programme and were encouraged to network with others with similar research interests which proved valuable: ‘Having the opportunity to network with other professionals in research around the UK has given me a huge insight into different pathways into the research’ (CNRF1) and inspiring: ‘I had some fantastic conversations with others also interested in neonatal pain, nationally and internationally’ (CNRF4). Networking also led to the possibility of ‘one to one’ virtual meetings with research leaders across the UK: ‘I was able to connect with research enthusiasts... I had a 1:1 session with the head of the UK Stroke Forum... [and an] Asst Prof. of Oxford University, who pioneered the Oxford Cognitive Screen tool’ (CNRF4).
Working alongside the other CNRFs was considered beneficial, collaborative and supportive: ‘It has been a great experience to work alongside others with the same passion for research, we have been able to encourage each other and offer advice and feedback’ (CNRF1). ‘It has been so valuable working alongside the other CNRF’s; listening to their experiences has helped me develop my own ideas and project’ (CNRF4).
The CNRFs believed the secondment would have an ongoing impact: ‘I feel this is not the end and I will continue to implement research into my practice more and more’ (CNRF1). During the course of the 6 months, additional positive outcomes included one of the CNRFs gaining promotion and another securing a new job within one of the organisation's most research-active academic departments.
Following completion of their secondment the CNRFs will join the Clinical Academic Network to network and collaborate with other NMAHPs within the organisation who are interested in and currently conducting independent research. The CNRFs will continue to be supported as required in terms of furthering their clinical academic careers by MS in her role as NIHR 70@70 Senior Nurse Research Leader and RE in her role as Director of the Clinical School.
Embedding Research In Care unit
Through the consultation process, a 12-month plan for the exemplar nurse-led ERIC unit was developed with four key phases: Phase 1: integration, promotion and assessment – where the Research Facilitator would be integrated into the ERIC team, assess staff experience in research (using the Spider Instrument (Smith et al., 2002), promote local research opportunities and aid recruitment to local and national studies. Baseline data would also be collected relating to research activity within the previous 12 months including the number of studies open to recruitment, number of participants recruited and number of NMAHP principal investigators. Phase 2: training and identification of research priorities – with training opportunities offered, both online and in-house, for ERIC unit staff and opportunity to identify clinical challenges/research priorities using a consensus process. Phase 3: data analysis and project development – use of readily accessible datasets, development of proposals relating to clinical priorities. Phase 4: evaluation, dissemination and ‘talent spotting’ – including evaluation of research activity and grant applications submitted. ‘Talent spotting’ of NMAHPS to pursue clinical academic careers e.g. CNRF roles, internships, Pre-doctoral Clinical Academic Fellowship (PCAF) or fellowships. Evaluation would include: research training accessed, repeat collection and comparison of baseline data at start and at 12 months and impact on staff within the ERIC units: assessed through focus groups including staff retention/satisfaction.
Five departments within the Trust expressed an interest in becoming an ERIC unit. The Respiratory Department was awarded the Trust’s first ERIC unit status following a successful interview attended by members of their multidisciplinary team. They wanted to become an ERIC unit as they recognised the importance of clinical research to improve patient care, were keen to support staff development and believed becoming an ERIC unit would support and accelerate their research ambitions.
The Respiratory ERIC unit recognises the importance of a whole-department approach to the development of research. The team are motivated by improving patient care and are committed to bringing on the next generation of researchers, with a focus on developing an environment in which NMAHP researchers can grow, develop and thrive. A monthly ERIC unit leadership meeting will oversee the strategic direction of the Department, with a clear emphasis on the development of the ERIC unit which will in turn be guided by a steering committee, meeting quarterly. As a healthcare organisation with acute and community services the respiratory team's desire to include multi-disciplinary staff across services and throughout the patient pathway was an exciting opportunity to foster collaborative research for the benefit of their patients.
Research Facilitator
Following a competitive interview process an experienced senior research nurse from the Exeter NIHR Clinical Research Facility was seconded to the role of Research Facilitator 1 day a week for 12 months initially. This staff member has extensive experience in clinical research (10+ years) and is enthusiastic about the possibility of working with the ERIC unit team to increase research activity/knowledge and embed research into clinical care at all levels.
Clinical Academic Network
The Clinical Academic Network has supported the CNRFs by sharing their experiences of developing a research career, research projects and funding applications through presentations to the group. They have also been involved in discussions around developing and evaluating the ERIC unit initiative and sharing awareness of these initiatives with their colleagues.
Individuals within the Clinical Academic Network group have had success in gaining personal academic research awards with: 1 × NIHR doctoral fellowship (clinical scientist), 1 × clinical doctoral research fellowship (occupational therapist), 2 × internships (dietitian and physiotherapist). A nurse within the group has applied for a pre-doctoral clinical academic fellowship and is waiting to hear if she has been successful. Applications for internships are also in progress.
Discussion
This paper highlights recent initiatives developed within one health service in South-West England through the NIHR 70@70 Senior Nurse Research Leader programme. Our approach has strengthened the research voice of nurses in the NHS, embedded research into clinical care, provided new opportunities for nurses and midwives and identified research priorities within clinical care.
These initiatives have significance to nursing practice and the role of nursing in providing evidence-based care. Nurse training and job descriptions include research or evidence-based care as an essential element yet active engagement with clinical research is often limited. Both the CNRF and ERIC unit initiatives provide opportunities for real engagement and commitment to ensuring research is a core component and integrated with clinical care and staff at all levels. We agree with de Lange et al. (2019), Bramley et al. (2018), Hafsteinsdóttir et al. (2017), Fry and Dombkins (2017) and others that mentoring, leadership and role modelling are key elements required to successfully ensure the integration of research into nursing practice and this support has been central to our initiatives.
The UK policy framework for health and social care research indicates that ‘a research culture should be fostered… by encouraging an awareness of health and social care research, research ethics and public involvement’ and enable staff to develop skills in research methods (Section 9.3b page 15). The policy also specifies that employers should encourage a high-quality research culture (NHS Health Research Authority, 2020). Our initiatives involved high-level agreement from the Trust's Chief Nurse and senior staff from the outset and have increased awareness of research and the importance of PPI amongst the CNRFs. The consultation process regarding the development and instigation of the ERIC unit initiative was key to engaging a wide range of clinical staff to ensure the strategy was acceptable, practical and recognised as a meaningful approach to embedding research in clinical care. The Chief Nursing Officer (CNO) for England national strategy for supporting, developing and embedding research 2020–2022 is currently being developed (NHS, 2020). The strategy runs alongside a commitment to ensure that the important contribution of nursing academia is fully recognised and supported as being integral to successful transformation. The CNO’s strategy will ensure that nursing research and evidence helps drive policy and underpin system transformation (NHS, 2020). The initiatives described in this paper align with the CNO’s strategy to develop and embed research and welcome the recognition of the importance of clinical academics.
The limitations of this paper include the fact that we only report the first cohort of CNRFs and the setting up of the first ERIC unit. The impact of the CNRFs' increased awareness of research on their colleagues was not formally assessed, given the impact of COVID-19 on how staff groups were operating, but this will be considered for future cohorts. However we have received expressions of interest to join future cohorts from staff within the CNRFs' own clinical areas which indicates transmission and increased enthusiasm as a consequence of the CNRF secondments. Unfortunately the commencement of the ERIC unit, originally planned for autumn 2020, was delayed by the COVID-19 pandemic, when it was deemed inappropriate to start a new initiative within a clinical area at a time of significant impact on clinical services. The original training programme planned for the CNRFs included a range of ‘shadowing’ opportunities with senior research staff and colleagues involved in research in a variety of research roles, this aspect of the training programme was adapted to ensure social distancing with remote learning and virtual meetings.. We are hopeful that future CNRFs will be able to engage in more ‘face-to-face’ opportunities and work alongside our team of clinical research nurses to gain greater experience in research delivery. We have secured commitment to fund five new CNRFs for the next financial year. However, the fact that multiple applications are required and we have not yet been able to secure long-term funding underlines the difficulties faced by nurses in forging clinical academic careers. We are supportive of initiatives to address this and recognise the role of strategic leaders in working together to identify which initiatives increase research capability and support the growth of clinical academics.
Conclusion
The introduction of CNRFs, developing and initiating an ERIC unit and setting up a Clinical Academic Network are examples of three initiatives developed through protected time within the NIHR 70@70 Senior Nurse Research Leader scheme to facilitate clinical research opportunities and successfully bridge the gap between clinical care and research. To ensure the success of these initiatives ongoing commitment to fully fund and evaluate such programmes is crucial and will enable their effectiveness and value for money to be demonstrated. We report this work in the early stages and will be expanding the initiatives with an ongoing rolling programme of training and appointment of new cohorts of CNRFs, with the second cohort commenced in June 2021. We will also expand and develop more ERIC units across the Trust in both acute and community settings with the ongoing support of research facilitators. We envisage the ERIC units as incubators for future NMAHP researchers developing clinical academic careers and as magnets for research innovation.
Key points for policy, practice and/or research
Dedicated time through the NIHR 70@70 Senior Nurse Research Leader scheme has enabled the development of a range of initiatives to embed research into clinical care. Our multi-faceted approach supports research training and enables career development, providing new opportunities for clinical staff to become engaged in research. Mentoring of staff, visible clinical academic role models and strategic leadership are crucial to ensure successful engagement and integration of research into nursing practice. Embedding research in usual care is essential if research is not to be seen and treated as a niche activity. These initiatives align with the CNO for England’s strategy for supporting, developing and embedding research.
Footnotes
Acknowledgements
MS is an NIHR 70@70 Senior Nurse Research Leader and also supported by the NIHR Exeter Clinical Research Facility which is a partnership between the University of Exeter Medical School College of Medicine and Health, and Royal Devon and Exeter NHS Foundation Trust. The views expressed in this article are those of the author(s) and not necessarily those of the NIHR, or the Department of Health and Social Care. MS acknowledges the support of the national network of NIHR 70@70 Senior Nurse/Midwife Research Leaders through discussions of the initiatives described.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics
Ethical approval was not required as this work describes a range of service developments rather than research.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this paper: This work was co-funded by the NIHR 70@70 programme (MS), the UK South West Clinical Research Network Research Innovation Fund and the Burdett Trust Fund for Nurses.