
Abstract
Background:
Chronic kidney disease is associated with structural and functional abnormalities in the kidney caused by a range of different aetiologies.
Purpose:
The study’s purpose was to explore the lived and coping experiences of patients with kidney failure undergoing haemodialysis in three private hospitals in Malaysia.
Methods:
Applying an interpretative phenomenological analysis using a hermeneutic phenomenological design to derive common meaning from participants lived and coping experiences. In the study, data were collected using a semi-structured interview guide from 15 purposefully sampled patients with kidney failure. Data were analysed using the interpretative phenomenological analysis principles.
Results:
Patients with kidney failure reported emotional distress, life limitations, financial burdens, knowledge deficits and varying perceptions of the haemodialysis treatment. Body image changes, financial assistance, social support and hope were coping strategies used by patients with kidney failure. It was identified that patients with kidney failure used unique coping strategies such as applying perfume and using clothes to conceal the impact of haemodialysis on their bodies, which is not comprehensively discussed in published literature.
Conclusion:
Nurses who deliver care to patients with kidney failure should focus on mitigating emotional distress, increasing knowledge related to kidney failure and improving perception of the haemodialysis treatment. Delivering and providing social support are indispensable nursing roles to help patients cope with haemodialysis treatment.
Keywords
Background
Haemodialysis is the most common treatment for managing kidney failure because of the limited availability of organs for transplantation, and it has been shown to improve the patients’ longevity, functional capacity and quality of life (Shahgholian and Yousefi, 2018). Patients experience physical, psychological, economic and social complications due to haemodialysis treatment, which can negatively impact their quality of life (DePasquale et al., 2020; Han et al., 2019; Hejazi et al., 2021). The global prevalence of kidney failure was 9.1% in 2017 (Bikbov et al., 2020). In Malaysia, it is estimated that the prevalence of kidney failure was 15.48% in 2018, a 6.41% increase from the 9.07% identified in 2011 (Saminathan et al., 2020). Malaysia has a hybrid private-public financing model, with the government contributing more than 50% of the funding (National Renal Registry (NRR), 2022). Despite approximately 56.2% of patients with kidney failure seeking haemodialysis in private facilities, Malaysian-based qualitative studies have mostly been conducted in public settings (NRR, 2022).
In the transactional theory of stress and coping, the theorist emphasises that when individuals experience stressors, they evaluate the factors about the available resources to overcome the issues (Obbarius et al., 2021). Healthcare providers need to offer tailored support founded on patients’ goals, values and attitudes to prepare them psychologically for haemodialysis treatment (Angioletti et al., 2018; DePasquale et al., 2020). A vast body of international literature is available on the lived experiences of individuals receiving haemodialysis (Kim and Lee, 2023; Moreels et al., 2023; Shahgholian and Yousefi, 2018). The need to conduct this study was the limited information about how Malaysian patients with kidney failure live and cope during haemodialysis, particularly those treated in private hospitals.
Purpose
The purpose of this study was to explore the lived and coping experiences of patients with kidney failure undergoing haemodialysis in Malaysian private hospitals.
Methods
The study was conducted using an interpretative phenomenological analysis (IPA), which supported applying a qualitative methodology and hermeneutic phenomenology design. The rationale for selecting a qualitative methodology was that it enabled the researcher to understand better the study phenomenon (Aspers and Corte, 2019). The researcher adhered to the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist when reporting the content in this methodology section (Appendix A; Tong et al., 2007).
Design
The hermeneutic phenomenological paradigm was applied. The design enabled the researcher to understand the lived and coping experiences of the patients with kidney failure undergoing regular haemodialysis treatment (Husserl, 2014; van Manen, 1990). For this reason, the design enabled the researcher to interpret the participants’ interview responses and derive meaning.
Sample/participants
A non-probability purposive sampling technique was used to select participants for this study. The recruitment involved the researcher sending the inclusion-exclusion criteria to each head of the dialysis department (HOD) at the private hospitals. The HODs gave the researcher a list of 30 patients who fulfilled the criteria. Purposive sampling was used to identify participants from the provided list who could be eligible for inclusion in the study. Participants were considered eligible to part of the study if they were (a) adults; (b) diagnosed with kidney failure; (c) receiving haemodialysis for the last 1 year; (d) could speak and understand English, Malay or Mandarin; (e) had consistent dialysis access without complications such as bleeding or poor flow to prevent causing excess distress to the patients and (f) free from any hearing impairments. Conversely, patients were excluded if they experienced impaired judgment, delusions, seizures and hypoglycaemic reactions; had two or more interruptions of their regular dialysis schedule because of illness, access issues or vacation; had any other kidney replacement therapy other than haemodialysis and had known short- or long-term memory impairment per their medical records and been diagnosed with Alzheimer’s disease or similar memory loss. Out of the 30 who consented, data were collected up to the 15th participant because saturation was achieved. The sample size was consistent with that in published literature, where researchers have argued that qualitative studies conducted using a phenomenological design should have a sample size of 3–10 participants after achieving data saturation (Hennink and Kaiser, 2022; Sim et al., 2018; Vasileiou et al., 2018).
Data collection procedure
The researcher adopted Heidegger’s theoretical assumption, modified by Creswell (2007), for conducting the interview. Before the interview, the study protocol was piloted, and the contents were confirmed. The researcher conducted face-to-face interviews in a private counselling room at the haemodialysis department from January 2020 to December 2020. The researcher audio-recorded the semi-structured interviews and made field notes during the process. The interview questions were open-ended and semi-structured. There were three private hospitals involved in this research study.
The researcher collected demographic data, such as gender, ethnicity, age, age diagnosed with kidney failure and length of time in haemodialysis treatment. Data on experience and coping were collected using a semi-structured interview guide. The duration of each interview process was 45–90 minutes, and the researcher gave each participant a hard copy of the transcribed interview the next day to verify its accuracy. All participants were also given shopping vouchers as a token of appreciation for participating.
Data analysis
Four steps of interpretative phenomenological analysis (IPA) principles were used in this study since it deals with emotional and significant life-changing experiences (Smith, 2008). Firstly, the researcher read and re-read the data to gain an understanding of the transcripts. Secondly, the researcher coded and categorised the transcripts using the NVivo software to generate the preliminary themes. Thirdly, the researcher organised the themes and sub-themes based on the research questions (Appendix B). Fourthly, themes were tabulated in a summary table (Appendix C), and the process was then repeated in the subsequent interviews. The IPA data analysis principles help researchers derive common meaning from patients’ experiences to answer research questions.
Trustworthiness
To ensure study quality, credibility, consistency, transferability and confirmability were used (Lincoln and Guba, 1985; Appendix D). The COREQ checklist was used for the reporting (Tong et al., 2007). Likewise, the researchers considered their own reflexivity throughout the process, being aware and reflexively self-critical of how their possible assumptions and biases could influence the process and the results. The research study consisted of nurses with health care experience, academics and management staff with knowledge in qualitative research methods.
Ethical considerations
The study was conducted after receiving approval from the Research Ethical Committee at the university’s Faculty of Medicine and Health Sciences on 9th January 2020 (reference number: University’s acronym-2019-388). The respective administrators approved recruiting patients from the three private hospitals. Participants provided signatures on written consent forms before participating in an interview. None of the sampled participants had any cognitive impairment based on the medical record and the Montreal Cognitive Assessment tool. Participation was voluntary, and coded identifiers were used to protect confidentiality. The researcher reminded patients with kidney failure that their participation was voluntary and could stop at any time. All study materials were kept on a secure university server, and no paper records were kept.
Findings
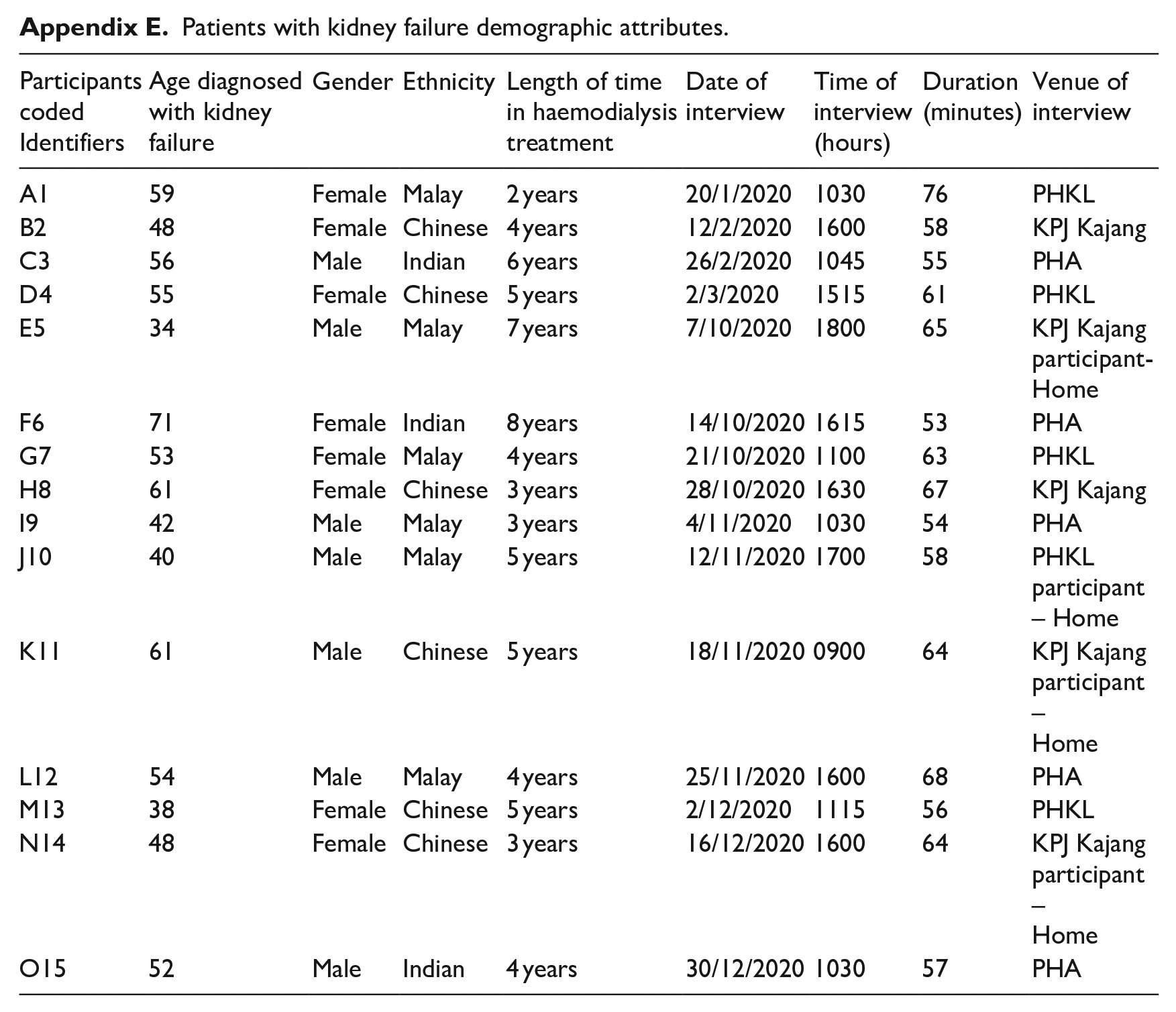
Fifteen of the sampled patients with kidney failure (eight female and seven male) were between 43 and 79 years old. All the patients were from three ethnic groups, namely Malay (n = 6), Chinese (n = 6), and Indian (n = 3). The patients were diagnosed with kidney failure between 34 and 71 years old and received haemodialysis treatment for 2–6 years. The Table in Appendix E contains a summary of patients’ demographic attributes. The study findings were categorised according to the research questions.
Research question 1: Lived experiences
The first research question was developed to understand the lived experiences of patients with kidney failure undergoing haemodialysis treatment. Five major themes were identified: emotional distress, financial burdens, limitations in life, knowledge deficit and diverse perceptions towards haemodialysis treatment (Appendix C).
Emotional distress
The 15 patients reported emotional distress as a lived experience. In essence, the emotions of shock, depression, regret and uncertainty were identified. Patients were shocked after being diagnosed with kidney failure. For instance, B2 indicated that:
the doctor told me that I would need to do dialysis treatment. I was shocked and did not accept the news.
The other feeling was depression, characterised by severe sadness, melancholy and sorrow. For example, I9’s response was:
I was extremely sad when the doctor told me that the biopsy results indicated that my kidneys were not functioning and that I would need to have dialysis. I locked myself in the room alone for about three months.
In addition, the patients expressed regret because of engaging in actions that they perceived resulted in kidney failure. The patients expressed regret about drinking carbonated drinks, eating salty snacks, consuming unprescribed or traditional medication, eating microwaved canned and frozen foods, and ineffective adherence to antihypertensive drugs. D4 indicated that:
I regret taking the painkiller medications that led to my kidney failure. I would take four Panadol tablets in 6 hours, and I had never consulted a doctor. I did it for over 10 years if I had any mild fever or discomfort. B2 stated that ‘I was regretful having carbonated drinks and salty snacks as my main meal every day’.
The other feeling was uncertainty about their futures, especially with the limited possibilities of receiving a kidney transplant. In addition, the patients indicated a possibility of dying at any time. K11 posited that:
I was afraid to accept the news when the doctor first told me, as I have my own family. I thought I could not plan my future when on dialysis treatment because I could die at any time.
Limitations in life
All 15 patients reported experiencing limitations in life-related to physical movement, foods, or drinks to consume, and the ability to perform family responsibilities, increasing their dependency. Illustratively, A1 indicated that:
I enjoyed travelling overseas before I was sick. Now, I cannot because I cannot walk for long and need to book dialysis treatment six months ahead. If I travel locally, I will need to book dialysis at least three months in advance.
In terms of restricted foods and diet, G7 indicated that:
I must keep track of the amount of fluid consumed. I can consume fluids up to 1000 mL daily.
Financial burdens
Twelve patients experienced financial burdens because of the haemodialysis expenses and hidden costs that destabilised their family’s fiscal capacity, exacerbated among individuals who lost their jobs. For example, F6 posited that:
The cost of dialysis is expensive. It is burdensome for my family because of the extra expenses it puts on me for my dialysis treatment.
Knowledge deficit on kidney failure
Ten respondents indicated a lack of knowledge about kidney failure, specifically the disease’s signs, symptoms and treatment technique. The deficiency in knowledge caused the patients to reject their diagnosis. For instance, A1 indicated that:
The doctor told me I had a kidney problem and needed dialysis. I did not know anything about this disease.
Diverse perceptions toward haemodialysis treatment
The patients had positive and negative feelings about the haemodialysis treatment. They indicated that they positively perceived the machine because it was important in supporting their survival, which made adhering crucial. For example, D4 posited that:
I enjoy dialysis because the treatment process helps me live in a place between happiness and dependence. The dependency provides me with an opportunity to connect with my family members.
Notably, the negative perception associated with the haemodialysis machine was provided by I9, who explained that:
The treatment has become repetitive and time-consuming. The dialysis treatment makes me tired and unfit to perform any activity.
Research question 2: Coping experiences
The second research question was explored to understand how patients with kidney failure cope with regular haemodialysis treatment in private hospitals. The major themes of body image changes, financial assistance, hope and social support were identified. Accordingly, the identified themes are discussed below.
Body image changes
Patients explained about the body image changes they used to cope with being on haemodialysis. The strategies included applying makeup, spraying perfume, and using clothes to conceal the impact of haemodialysis on their bodies. N14 said that:
Since starting dialysis treatment, I have become more self-conscious about my appearance, especially my hand with the fistula. When I was on long-term dialysis treatment, it affected my appearance, especially on my fistula hand. The scary purple vein that runs through the hand with the fistula is very clear, so I use make-up to conceal it. The smell can sometimes be too much for me, and I lose my confidence because of it. I will wear long sleeves over my hands when I am outside. I spray perfume on myself to hide the smell.
Financial assistance
Two patients indicated that they receive financial assistance with their medical bills. For example, M13 indicated that:
The nurses connected me with a referral group, where I was able to learn more about seeking financial aid from non-profit private organisations.
Hope
The patients reported being hopeful about receiving a kidney transplant, having their health restored and regaining their freedom. An example is C3 who stated that:
It might take a while, but I keep fighting. I am waiting for my turn to have a kidney transplant one day. Another respondent N14 expressed: I hope to return to my previous life before dialysis treatment, when I was no longer dependent on dialysis to prolong my life or needed to have fluids and diet restrictions. I hope to live a normal life again.
Social support
Ten patients indicated that they receive social support from family members, friends, healthcare providers, religious leaders, volunteers and employers/superiors. An example of supportive family members was provided by F6, who indicated that:
I am glad that I have a supportive family. My daughter is very supportive of me. I do not ask her what I need, but she is aware.
An example of response on supportive health care personnel was by F6, who posited:
The nice and friendly staff here treat me very well. The nurses here are concerned about me.
A response related to the supervisors’ support was made by E5, who indicated that:
I can still manage my work as I have my supportive superior and colleagues helping me if I am absent. They are willing to share my workload.
On spirituality, B2 said:
I always pray to God as I believe God is my shelter and will look after me. I go to church and seek strength from God.
Discussion
The findings of the patients’ experiences with kidney failure are congruent with those published in the literature. DePasquale et al. (2020) and Hejazi et al. (2021) acknowledged that being diagnosed with kidney failure is associated with psychological illnesses such as depression. The patients in this study reported that after being diagnosed with kidney failure, they were shocked, depressed and extremely sad.
Ahmad and Al Nazly (2015) and Tadesse et al. (2021) identified that patients with kidney failure receiving haemodialysis reflected the experience of a horrible nature because of requiring lifelong treatment, recurrent expenditure, limited social life and restricted diet and fluids intake. The researchers support the identified themes of limitations in life, diverse perceptions about haemodialysis, and financial burdens. In this study, the patients reported that haemodialysis was expensive and burdensome for them and their families. The disease had limited their physical movements, such as travelling and capacity to consume certain foods and drinks. The patients reported experiencing a knowledge deficit about kidney failure and haemodialysis, a concept that has not been adequately assessed in published literature. A notable diverse perception about haemodialysis was identified in a participant’s response which indicated that although the treatment resulted in dependency, it provided an opportunity to connect with their family members.
According to the transaction theory of stress and coping, coping influences physical and mental wellness and social functioning (Obbarius et al., 2021). Tadesse et al. (2021) acknowledged body-related changes such as swelling and abnormal distortion as a problem, but the researchers did not report how patients cope with the issues. The study generated new knowledge by identifying that patients in the three Malaysian hospitals cope with haemodialysis symptoms by performing body changes, specifically applying perfume, wearing clothes and using make-up, strategies that had not been discussed in the published literature.
The patients reported having supportive family members, healthcare professionals, work supervisors, religious leaders and spouses as coping strategies. The results are consistent with the published literature, where researchers have acknowledged family members and healthcare professionals as a source of support for patients undergoing haemodialysis (Han et al., 2019; Mbeje and Mtshali, 2021). Social support from work colleagues/employers is a unique source of solace for patients in haemodialysis that has not been reported in the published literature. A possible explanation for this new knowledge contribution is that some of the study participants were still employed despite having chronic kidney disease, which differs from the norm.
The patients indicated coping with their fiscal burdens through financial assistance and social support. Financial assistance is provided by non-governmental organisations, a concept supported in published literature (Han et al., 2019; Shahgholian and Yousefi, 2018). Consistent with the theory of self-regulation and the self-response concept that patients can positively or negatively respond to challenges such as haemodialysis treatment, the perception of hope was identified among the interviewed patients (Ma et al., 2022). Tavassoli et al. (2019) acknowledged that being hopeful about receiving a kidney transplant is a common concept among kidney failure patients.
Limitations
The limitations in this study are associated with the qualitative methodology’s bias and trustworthiness. Specifically, participants in this qualitative study were recruited from three private hospitals within the same area in Malaysia. As such, the recruited sample could hinder the results’ transferability because the respondents were likely to receive specialised care. In addition, only participants receiving haemodialysis for at least 1 year were involved in the study, limiting the findings’ applicability to patients just beginning their treatment. Another limitation is using semi-structured, in-depth qualitative interviews as the only data source. As a result, the participants’ responses may have been influenced by their situations and how they observe the experiences, which affects the findings’ trustworthiness. The other limitation is that this study was conducted by one researcher, which increased the probability of bias. Specifically, researcher bias could have occurred because the interpretation of the findings was based on one person’s perception, meaning their preconceptions about the topic could have affected the results.
The conducted qualitative study has a small sample size, which reached saturation after 15 samples, since it emphasises in-depth study. Although more participants may have been interviewed, the number represents Malaysian haemodialysis patients with kidney failure. The focus of the study was exploring Malaysian haemodialysis patients lived and coping experiences rather than generalising. Semi-structured, in-depth qualitative interviews were used as the significant data source, meaning the findings were influenced by participants’ experiences and views. Despite these limitations, the rich, detailed descriptions used in this research can enable patients, family members, health providers and researchers of kidney failure to understand the lived and coping experiences of kidney failure patients receiving haemodialysis in Malaysia.
Conclusion
The findings in this study suggest that patients with kidney failure experience emotional distress, life limitations, financial burdens, knowledge deficits and varying perceptions of the haemodialysis machine. However, applying coping approaches such as body image changes, hope, financial assistance and social support facilitates overcoming the problems. As such, nurses have a role in improving both the patients’ experiences and supporting their coping capabilities.
Specifically, the findings provide nurses with an understanding that patients diagnosed with kidney failure are at risk of experiencing emotional distress, particularly those in advanced stages of haemodialysis treatment. Hence, nurses should focus on mitigating emotional distress, increasing their knowledge of kidney failure-related information, and improving the perception of haemodialysis treatment among kidney failure patients. Applying shared decision-making approaches, where the patients’ families are involved and promoting social support, are indispensable nursing roles to help the patients cope with haemodialysis treatment. The implications for patients with kidney failure and its related challenges are manageable through body image changes, seeking financial assistance, being hopeful, receiving quality treatment and accepting social support.
Key points for policy, practice and/or research
Patients with kidney failure experience emotional distress, life limitations, financial burdens, limited knowledge and different perceptions of the haemodialysis machine.
Experiences such as body image changes, hope, financial assistance and social support help patients cope with kidney failure and haemodialysis treatment.
Nurses who deliver care to patients with kidney failure should apply evidence-based interventions focused on mitigating emotional distress, increasing knowledge of kidney failure and improving perceptions of the haemodialysis treatment.
The nurses’ focus should be engaged in shared decision-making to promote social support and help the patients cope with haemodialysis treatment.
Unique coping experiences, specifically applying perfume and using clothes to conceal the impact of haemodialysis on their bodies, were identified as lacking in the published literature, creating a need for more research on the concepts.
Supplemental Material
sj-pdf-1-jrn-10.1177_17449871241235627 – Supplemental material for Exploring the lived and coping experiences of patients with kidney failure undergoing haemodialysis in Malaysian private hospitals
Supplemental material, sj-pdf-1-jrn-10.1177_17449871241235627 for Exploring the lived and coping experiences of patients with kidney failure undergoing haemodialysis in Malaysian private hospitals by Tan Woei Ling, Lee Khuan, Anisah Baharom and Mohd Mursyid Arshad in Journal of Research in Nursing
Supplemental Material
sj-pdf-2-jrn-10.1177_17449871241235627 – Supplemental material for Exploring the lived and coping experiences of patients with kidney failure undergoing haemodialysis in Malaysian private hospitals
Supplemental material, sj-pdf-2-jrn-10.1177_17449871241235627 for Exploring the lived and coping experiences of patients with kidney failure undergoing haemodialysis in Malaysian private hospitals by Tan Woei Ling, Lee Khuan, Anisah Baharom and Mohd Mursyid Arshad in Journal of Research in Nursing
Supplemental Material
sj-pdf-3-jrn-10.1177_17449871241235627 – Supplemental material for Exploring the lived and coping experiences of patients with kidney failure undergoing haemodialysis in Malaysian private hospitals
Supplemental material, sj-pdf-3-jrn-10.1177_17449871241235627 for Exploring the lived and coping experiences of patients with kidney failure undergoing haemodialysis in Malaysian private hospitals by Tan Woei Ling, Lee Khuan, Anisah Baharom and Mohd Mursyid Arshad in Journal of Research in Nursing
Footnotes
Appendices
Quality criteria (Lincoln and Guba, 1985).
| Criteria | Procedure |
|---|---|
| Credibility | Verbatim transcripts of interviews. Search the text for textual evidence to support findings. |
| Dependability | Detailed description of participants’ characteristics and their inclusion and selection criteria. Detailed description of all the stages of the research process, the results and decisions taken during research, justifying their rationale. |
| Transferability | Each individual’s perceptions are unique, and the meanings behind them are shared. |
| Confirmability | Separate and pairwise analysis of the data. The interpretive (narratives) results have been compared with all the participants (15 patients). |
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was conducted after receiving approval from the Research Ethical Committee at the university’s Faculty of Medicine and Health Sciences on 9th January 2020 (reference number: University’s acronym-2019-388).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.