
Abstract
Background:
Pain and anxiety during arteriovenous fistula (AVF) puncture are crucial factors affecting haemodialysis (HD) patients’ quality of life.
Aim:
The aim of this study is to assess the effect of virtual reality (VR) distraction on pain, anxiety, satisfaction and haemodynamics during AVF puncture.
Methods:
This randomised controlled trial study was conducted in a Haemodialysis unit at Mansoura University Hospital. Ninety-six patients were randomly divided into the intervention (n = 48) and control (n = 48) groups. Six minutes prior to the puncture, patients in the intervention group used VR glasses to experience a 360° ‘Relax River VR tour’, whereas patients in the control group received no intervention.
Results:
Following the intervention, pain, anxiety, systolic blood pressure and heart rate were significantly lower, and satisfaction scores were significantly higher in the intervention group than in the control group (p < 0.05).
Conclusion:
VR distraction may help alleviate pain, anxiety and increase satisfaction. It may be considered a safe and cost-effective non-pharmacological therapy for HD patients undergoing AVF puncture.
Introduction
Chronic kidney disease (CKD) impacts over 10% of the global population (Hill et al., 2016). The burden is even greater in the developing countries (Younes et al., 2022). For instance, in Egypt, there are approximately 74 new cases of end-stage renal disease (ESRD) per million annually, with a total of 264 dialysis patients per million (Barsoum, 2006). The most common renal replacement therapy for CKD patients is haemodialysis (HD). In individuals undergoing HD, the arteriovenous fistula (AVF) is considered as the gold standard of vascular access (Schmidli et al., 2018). However, patients undergoing HD experience pain, anxiety and stress due to large-gauge needle punctures necessary to ensure efficient AVF flow (Ibrahim et al., 2022).
AVF puncture pain is a common concern, with varying degrees of intensity (Figueiredo et al., 2008). A study conducted among HD patients reported moderate-to-severe pain in 78% of participants
Various forms of distraction during AVF puncture have been employed in numerous studies, such as self-soothing music (Shabandokht-Zarmi et al. 2017), with research indicating that both auditory and visual distractions effectively reduced puncture pain, but visual distraction was found to be more effective (Aghbolagh et al., 2020). VR distraction is a non-pharmacological method that combines multiple senses, such as audio, visual and kinaesthetic, to provide social and emotional distraction from a stressful situation (Aminabadi et al., 2012).
Virtual reality (VR) is now easily accessible through smartphones. According to the gate control theory, patients’ attention is diverted, and their perception of anxiety and pain is diminished when they view VR images (Guo et al., 2015). Numerous studies have confirmed that VR is effective in reducing pain and anxiety in diverse medical procedures, such as fine-needle aspiration biopsy (Karaman and Taşdemir, 2021), dressing changes (Ding et al., 2019) and burn treatment (Li et al., 2017). Additionally, VR has been shown to reduce pain and improve patients’ satisfaction during intravenous insertion (Basak et al., 2020) and helps hypertensive patients manage their blood pressure and heart rate (HR) during dental extraction (Qin et al., 2022).
VR has become a well-accepted analgesic and sedative strategy as it is effective, feasible, portable and has no adverse effects during HD (Hernandez et al., 2021; Pourmand et al., 2018). To the best of our knowledge, no previous studies has investigated the effectiveness of VR distraction on pain, anxiety, satisfaction and haemodynamic parameters following AVF cannulation in patients undergoing HD. Therefore, the aim of the current study is to evaluate the effect of VR distraction on pain, anxiety, satisfaction and haemodynamics among HD patients during an AVF puncture.
Methods
Design, participants and setting
The current randomised, controlled, single-blind study was conducted at the haemodialysis unit in Mansoura University Hospital, Egypt, from June to November 2022. The unit is composed of a large hall with 30 haemodialysis machines, provides peritoneal dialysis as well and serves three shifts per day.
The sample size was calculated based on a previous study by Ibrahim, Badawi and Alameri (2022), with a mean and standard deviation of pain scores for AVF cannulation being 4.42 ± 2.97. Initially, a minimum of 44 patients per group was calculated (α = 0.05, power = 0.80), then increased by 10% to account for potential dropouts. From 140 dialysis patients, 96 patients met the inclusion criteria. Protocol violations resulted in the exclusion of one patient in the VR group and two patients in the control group (Figure 1). The study included patients aged 18–60, receiving HD three times per week for at least 1 month, with healthy and functional AVF access. Exclusions encompassed patients with psychiatric, panic or anxiety disorders; dysfunctional AVF; vertigo; vision; perception or hearing problems; or those who took analgesics 3 hours prior to HD.
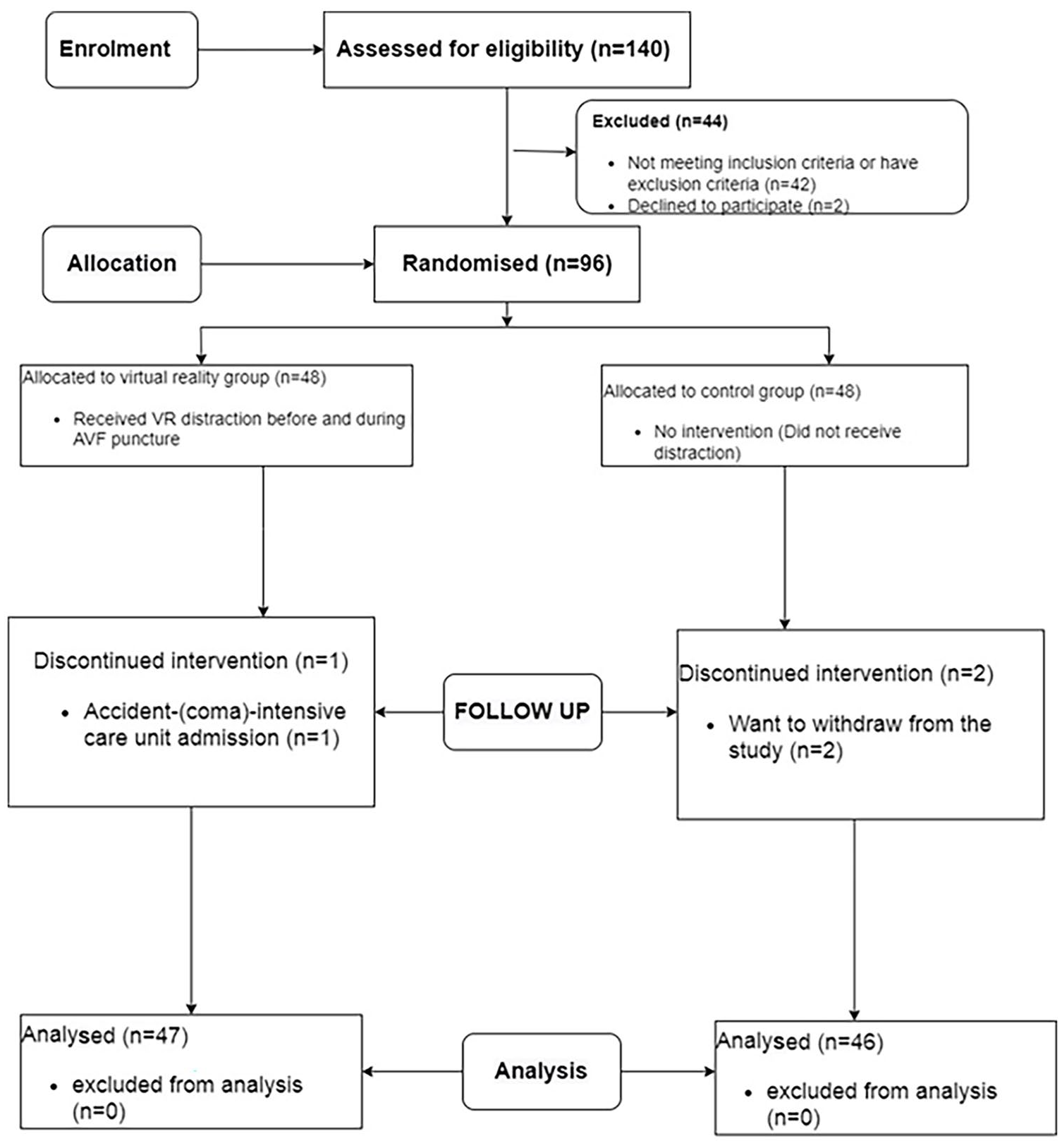
Consort flow diagram.
Randomisation and blinding
Block randomisation, with a block of size six, was used to randomly assign 96 patients into two groups: VR (n = 48) and control (n = 48). The allocation sequence was generated by an independent researcher using free online software (https://www.sealedenvelope.com/simple-randomiser/v1/lists), concealed in opaque envelopes, sealed, numbered, signed and kept blinded to the researchers until intervention procedures. The first enrolled patient was assigned with the number one envelope, which was then opened. Based on the letter inside the envelope, the patient was allocated to either the VR or control groups.
Interventions
The subjects in the intervention group viewed a 360° ‘Relax River VR tour’ using VR glasses during the puncture, starting 6 minutes prior to the procedure (Figure 2). The tour involves riding a boat on a wonderful river with rich nature and mountain scenery, discovering creatures, listening to natural sounds and relaxing to music. It is available at Google play and accessed at https://play.google.com/store/apps/details?id=com.sfera.relaxrivercb&hl=en&gl=US. The river tour was based on previous studies that used nature VR tours as a method of distraction (Karaman and Taşdemir, 2021; Menekli et al., 2022).

An HD patient using VR during an AVF puncture.
VR BOX Version 2.0 glasses (manufactured by Shinelife Company, India) used in this study is compatible with smartphones ranging from 3.5 inches to 6.0 inches, offering auditory and visual experiences for the participants. The sight distance was precisely adjusted for each patient, and their comfort was considered. Additionally, the headphones were connected to the same smartphone to allow participants to hear the sounds.
During the second dialysis session, which marked the inaugural intervention session, the fistula was punctured while the participants in the intervention group were immersed in the VR scene. The puncture procedure, performed by nursing staff, lasted approximately 2 minutes and was conducted without anaesthesia in all patients. Conversely, subjects in the control group did not receive any intervention for pain or anxiety management. They underwent the routine AVF puncture technique, which included hand hygiene, wearing personal protective equipment, disinfecting the puncture site with povidone iodine, needle insertion (rope ladder technique) and needle securement, while the procedure was observed as it unfolded. The chosen duration of 6 minutes for the VR distraction aligns with previous research employing diverse forms of distraction during AVF puncture (Aghbolagh et al., 2020; Shabandokht-Zarmi et al., 2017).
Measurements
Five tools were utilised in our study to evaluate outcomes, including:
Patient assessment sheet. The researcher designed this form after reviewing the literature to capture ‘socio-demographic characteristics’ (age, gender, educational level, social status, income level, occupation and residence) and medical characteristics (nephropathy aetiology, fistula age, type, site and duration of dialysis).
State-trait anxiety inventory (STAI). This tool was utilised to evaluate levels of state and trait anxiety (Spielberger et al., 1983). It was translated and validated in Arabic by Bahammam (2016) and demonstrated high reliability (Cronbach’s α: 0.989). It consists of two subscales, each comprising 20 items: The State Anxiety Subscale (STAI-S) asks patients about their feelings at a particular time, whereas the Trait Anxiety Subscale (STAI-T) asks about their feelings generally. Scores for each subscale range between 20 and 80, with higher scores indicating elevated levels of anxiety. In our study, Cronbach’s α was 0.934 for the state part and 0.932 for the trait subscale.
The Pain Visual Analogue Scale (VAS) is a reliable instrument for measuring acute pain (Kahl and Cleland, 2005). It consists of an unscaled 10-cm-long straight line with two endpoints: ‘No pain’ at one end and ‘worst possible pain’ at the other. Patients were instructed to indicate their pain level by marking the line at the point that best described their pain intensity. The measurement was then determined by calculating the distance in centimetres between the ‘no pain’ point and the patient’s mark. VAS scores within the range of ⩽3.4 were described as mild, scores between 3.5 and 7.4 were categorised as moderate and scores of ⩾7.5 were classified as severe (Boonstra et al., 2014).
Satisfaction VAS. This tool was employed to assess satisfaction. Patients were instructed to rate their satisfaction with the procedure on a 10-cm-long unscaled straight line with ‘0’ representing unsatisfied and ‘10’ indicating very satisfied (Şahin and Eşer, 2018).
Haemodynamics.
Data were collected by research assistants who were blinded to both groups and did not observe the puncture or distraction technique and were blinded to both groups throughout the study. Patients were provided with information about VAS and STAI use. Subsequently, face-to-face interviews were conducted with the patients to complete these assessment tools. Haemodynamic measurements were obtained using the Biolight M69 monitor.
During the initial HD session (prior to intervention), demographic and medical data were collected, and pre-procedural anxiety was assessed. Following the puncture, pain intensity was measured within 1 minute (Shabandokht-Zarmi et al., 2017). Immediately afterward, post-procedural state anxiety, haemodynamics and satisfaction level were assessed. At the second HD session (after intervention), a pain score, a post-procedural state anxiety score, patient satisfaction and haemodynamics were evaluated.
Statistical analysis
The data were analysed using the IBM SPSS 27 software. The Shapiro–Wilke test was used to assess normality, revealing that all variables exhibited a normal distribution except for age. Descriptive statistics were presented as mean, SD, frequency and percentage. For inferential statistics, paired t-test and independent t-test were employed for normally distributed data, whereas the Mann–Whitney U-test was utilised for non-normally distributed data. Fisher’s exact test and chi-squared test were applied for categorial data analysis. Effect size for significant t-test as estimated using Cohen’s d or Glass’s delta tests, with effect size classified as small (d = 0.2), medium (d = 0.5) and large (d ⩾ 0.8) based on equality of variance (Cohen, 1988). Effect size for significant chi-squared test were estimated using Cramer’s V and Phi tests, with effect size classified as small (0.1), medium (0.3) and large (⩾0.5) (Polit and Beck, 2016). There were no missing data in the analysis.
Results
The study found no statistically significant differences between groups with regard to socio-demographic characteristics, medical characteristics and trait anxiety (p > 0.05; Table 1).
The comparison of HD patients’ demographic, medical and pre-procedural anxiety scores in both groups (N = 93).
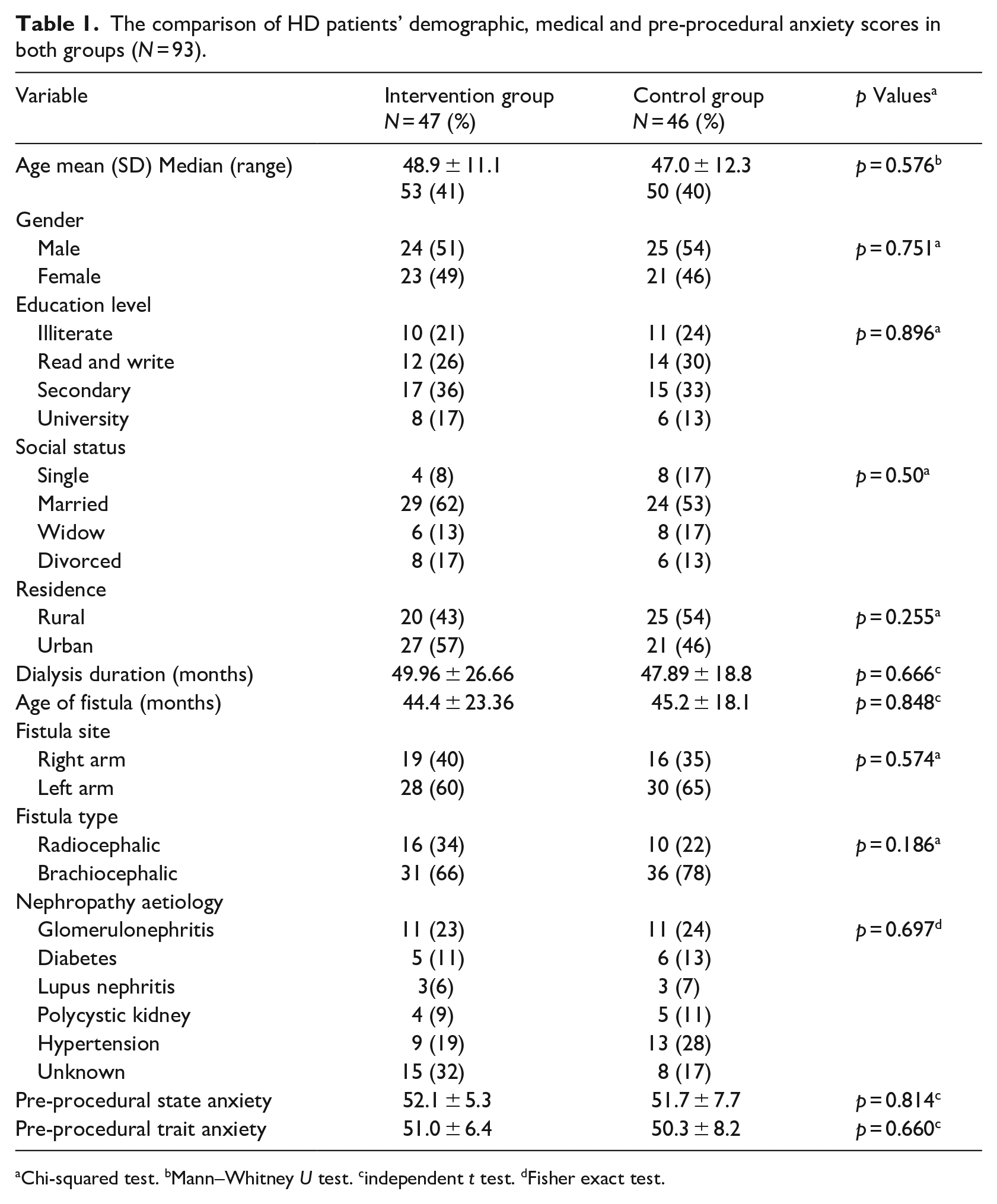
Chi-squared test. bMann–Whitney U test. cindependent t test. dFisher exact test.
Following the intervention, there was a significant reduction in pain levels in the VR group compared to the control group (p ⩽ 0.001). The effect size of the difference in pain scores between both groups was −1.87, indicating a large effect size (Table 2). State anxiety revealed a significant reduction in the VR group compared to those in the control group (p = 0.003), with an effect size of −0.629, indicating a medium effect size (Table 3). Furthermore, patients in the intervention group had significantly higher mean satisfaction scores compared to those in the control group, with a small effect size (0.438; Table 3).
Comparison of pain scores before and after VR intervention in both groups (N = 93).
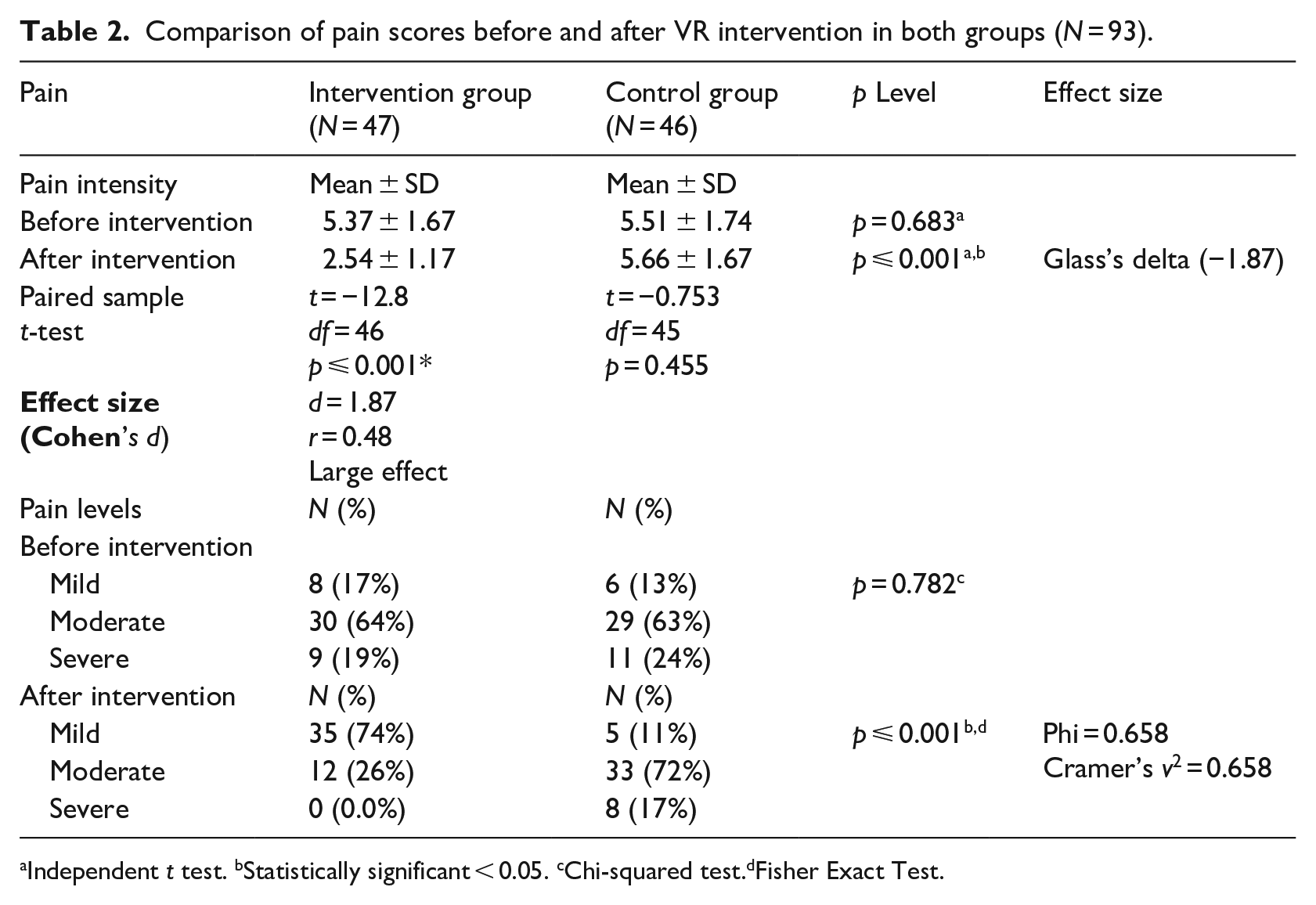
Independent t test. bStatistically significant < 0.05. cChi-squared test.dFisher Exact Test.
Comparison of post-procedural state anxiety and satisfaction scores before and after VR intervention in both groups (N = 93).
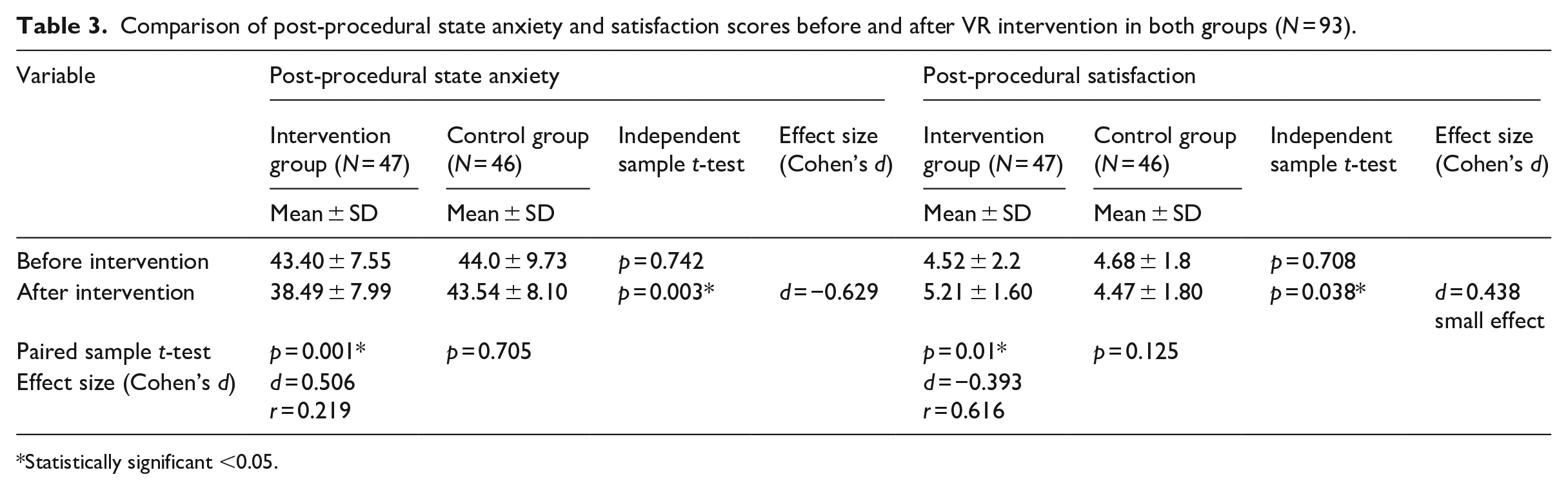
Statistically significant <0.05.
In terms of haemodynamics following the intervention, the systolic blood pressure (SBP) and heart rate (HR) in the intervention group were substantially lower than those in the control group, with both groups exhibiting a small effect size (p = 0.037, d = −0.438 and p = 0.044, d = −0.424, respectively) (Table 4).
Comparison of haemodynamics before and after VR intervention in both groups (N = 93).
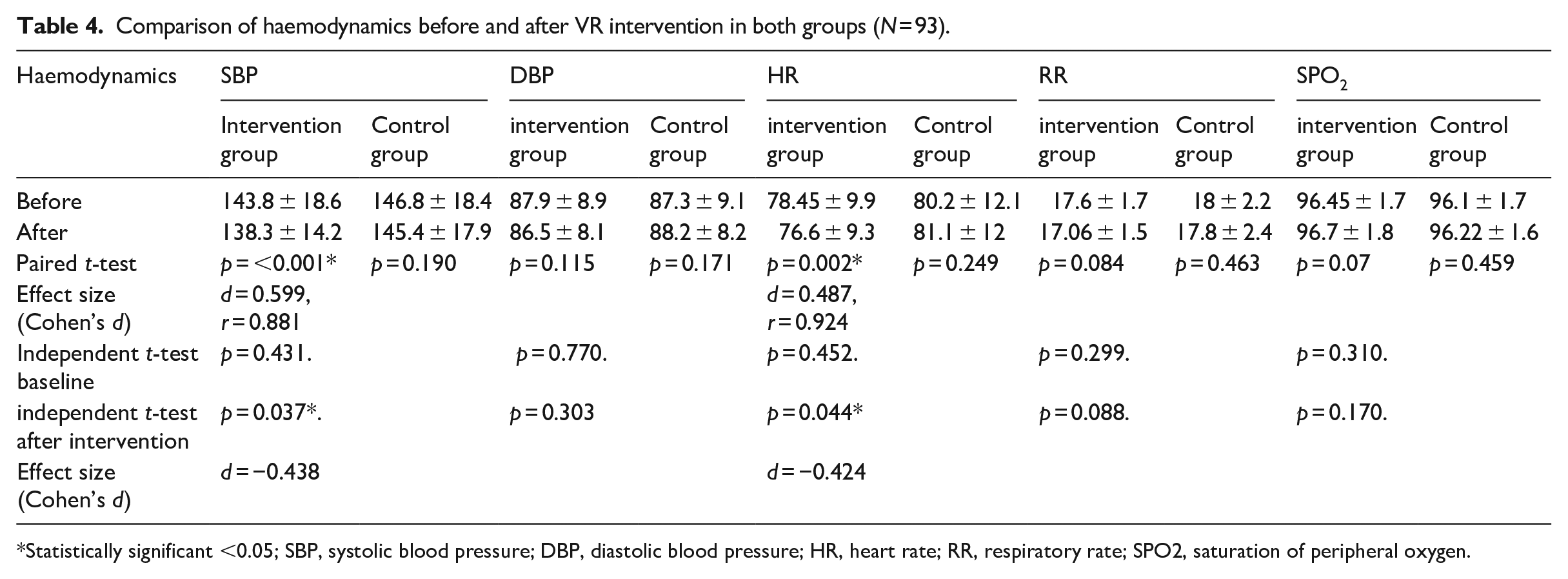
Statistically significant <0.05; SBP, systolic blood pressure; DBP, diastolic blood pressure; HR, heart rate; RR, respiratory rate; SPO2, saturation of peripheral oxygen.
Regarding patient satisfaction, it has a moderately negative correlation with pain scores (r = −0.472, p < 0.001) and a slight negative correlation with anxiety scores (r = −0.298, p = 0.042; Table 5).
Pearson correlation coefficients between anxiety, pain and satisfaction scores after VR intervention in the intervention group (N = 47).
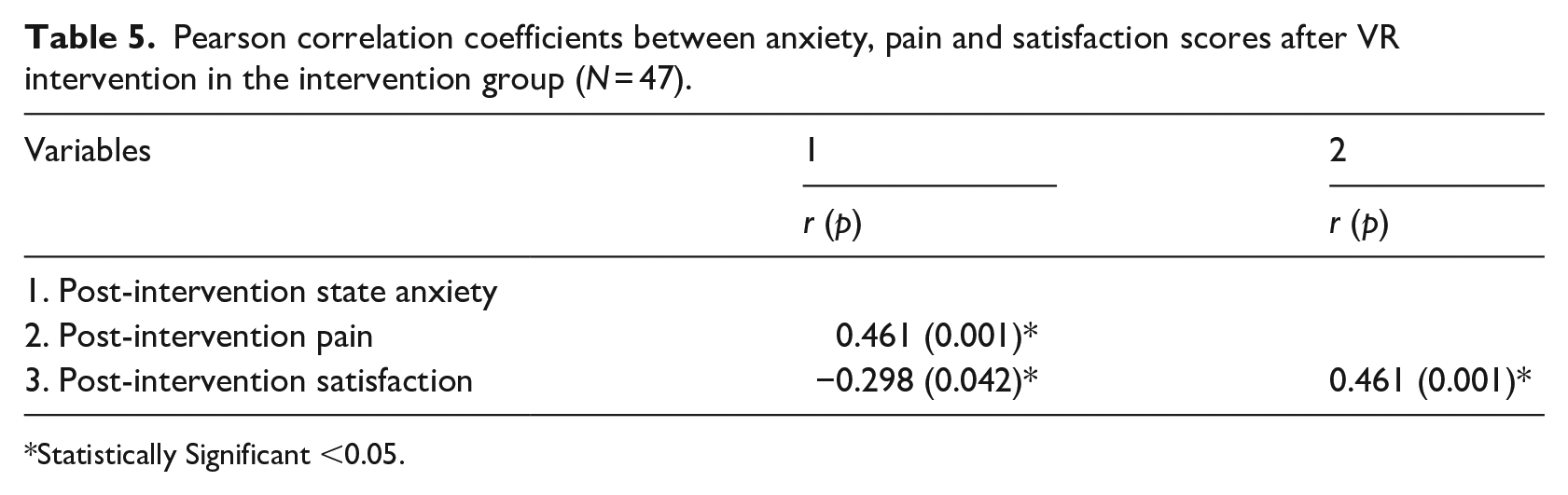
Statistically Significant <0.05.
Discussion
Before the intervention, most patients in our study had moderate pain, one-fifth had severe pain and 13–17% had mild pain, aligning with the findings of Ibrahim et al. (2022). Post-intervention, the VR group had significantly lower pain scores compared to the control group. Although no previous study used VR during AVF puncture, its effectiveness was studied in different procedures. For instance, VR distraction was effective in reducing canulation pain among adults and paediatrics (Basak et al., 2020; Gao et al., 2023), as well as during fine-needle breast biopsy (Karaman and Taşdemir, 2021) and among oncology patients undergoing port catheter implantation (Menekli et al., 2022). In contrast, a study on children reported that VR distraction was not effective in reducing pain, anxiety and vital signs during intravenous insertion (Yıldırım and Gerçeker, 2023), potentially due to the differences in pain and fear constructs between children and adults (Piskorz and Czub, 2018). Another study reported no effect of VR on pain during a cystoscopy (Walker et al., 2014). This finding may be because patients reported not being fully immersed in the VR environment, and this is supported by Guo et al. (2015), who reported a statistically significant correlation between pain level and sense of involvement in the virtual environment. Moreover, it is noteworthy that our study included male patients, and the interpretation of pain may be influenced by social and cultural factors in both males and females (Figueiredo et al., 2008; Innis et al., 2004).
In our study, VR distraction significantly reduced post-procedural state anxiety with a medium-negative effect. As reported by Ugras et al. (2022), VR showed a medium effect in reducing preoperative anxiety. Other studies reported a large effect of VR on anxiety among septorhinoplasty patients (Baytar and Bollucuoğlu, 2021), breast-biopsy patients (Karaman and Taşdemir, 2021) and oncology patients (Menekli et al., 2022). Additionally, studies among adults during dental procedure (Lahti et al., 2020), endovenous radiofrequency ablation procedures (Brewer et al., 2021) and among children during venipuncture (Gao et al., 2023) reported the effectiveness of VR in alleviating anxiety.
Conversely, VR did not reduce preoperative anxiety, according to a study conducted among women undergoing caesarean sections (Noben et al., 2019). This result may be attributable to the fact that the VR video in this study was an informative experience about the surgery and not a relaxing or distracting one. Another study on male patients during cystoscopy demonstrated a non-statistically significant effect in the VR group (Walker et al., 2014). This result may be because the VR distraction effect on anxiety differs by gender, as reported by Lahti et al. (2020). Further studies are required to determine whether the use of VR during dialysis hours has a large effect on anxiety.
According to our study findings, VR distraction reduced pain and improved patient satisfaction. A negative correlation was found between patient satisfaction and pain scores, which is consistent with the literature suggesting that effective acute pain management is linked to increased patient satisfaction (Glowacki, 2015). Similarly, Basak et al. (2020) reported high satisfaction scores among patients who received VR during peripheral cannulation. Studies involving patients undergoing knee arthroscopy (Sahin and Basak, 2020) and endovenous radiofrequency ablation (Brewer et al., 2021) also reported improved satisfaction with VR usage. Additionally, our research revealed a small effect size, suggesting that various factors, including culture and religious considerations, may influence individual’s tolerance to higher pain levels, thus reducing the mean difference between groups (Daly Quinlan-Colwell, 2009).
In terms of haemodynamics, we observed a significant reduction SBP, and HR with a small effect size, whereas DBP, RR and SPO2 showed no statistically significant reduction. This indicates that VR may increase parasympathetic activity, thereby altering physiological reactions. Hsieh and Li (2022) reported a significant reduction in HR among HD patients during the first week but no effect during the second or third week, suggesting that using the same VR video for extended periods could influence results. Additionally, Ugras et al. (2022) reported a small effect on SBP and HR in the VR group. Baytar and Bollucuolu (2021) found no effect on respiration or O2 saturation with VR. Another study reported a statistically significant decrease in SBP and HR among healthy volunteers experiencing a forest VR experience, with no significant effect on DBP (Yu et al., 2018). Conversely, a study conducted among children reported a significant increase in HR in the VR group (Felemban et al., 2021), possibly due to VR goggles isolating them from the real world and increasing anticipation of an unpleasant stimulus, thereby raising their heart rate (Slifer et al., 2002).
Limitations
This study has several limitations that warrant consideration. Firstly, there is a scarcity of comparable studies, with the majority of research focusing on paediatric populations. Secondly, our study was conducted exclusively with adult participants from a single haemodialysis unit, which limits the generalisability of our study. Thirdly, the intervention was applied only once, and we did not assess any potential delayed pain management effects. Moreover, we did not investigate patient’s viewing preferences or utilise objective physiological pain measurements, such as salivary cortisol concentration, which could have provided additional insights into the effectiveness of VR distraction.
Conclusion and recommendations
This study showed that VR distraction effectively reduced haemodialysis patients’ pain and anxiety, while also positively impacting physiological parameters such as SBP and HR. Additionally, patient satisfaction was significantly improved with the use of VR distraction. Based on our findings, we recommend the integration of VR distraction as a safe and cost-effective non-pharmacological therapy for patients undergoing AVF puncture during HD procedures.
However, further studies are warranted to evaluate the applicability and effectiveness of VR distraction techniques across diverse age groups and in the context of various needle-related procedures. Future research endeavour may explore the effects of repeated sessions utilising both similar and different landscapes on the physical and psychological outcomes of HD patients. Additionally, comparative studies between VR and other distraction techniques, as well as examining their combined effects, could offer valuable insights into optimising pain management strategies for this patient population.
Key points for policy, practice and/or research
This research encourages policymakers to consider the broader integration of VR in health care settings to enhance the quality of patient care.
This approach encourages nurses to proactively integrate VR distraction into their clinical practice to enhance the overall experience for haemodialysis patients.
This research suggests further research studies of the applications for VR distraction in critical care settings.
Footnotes
Acknowledgements
We thank all patients, nursing staff in the HD Department, and assistant researchers.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval and consent to participate
The ethics committee at Mansoura University approved the current study (no. P. 0239), and official permission was obtained from the hospital. Informed written consent was obtained from all subjects enrolled in this study. The confidentiality of patients’ data was guaranteed, participation was voluntary and patients had the right to withdraw without penalty and at no cost. The study procedures adhered to the ethical principles of the Declaration of Helsinki. Separate consent for photography was obtained.