
Abstract
Background:
Cervical cancer screening is a powerful tool in the prevention, early detection, and diagnosis of precancers and cancer. There is mounting evidence, however, demonstrating that Queer cisgender women experience disparities in cervical cancer screening access and uptake compared to their heterosexual counterparts. To close gaps in screening, Queer women’s voices and visions must foreground recommendations aimed at remedying screening inequities.
Objectives:
This study aims to explore perceptions on an ideal cervical cancer screening exam among a racially and ethnically diverse group of Queer women.
Design:
This qualitative interview study is led in partnership with a multidisciplinary community steering committee. Our work is grounded in the Reproductive Justice Framework.
Methods:
We held in-depth interviews with 19 Queer women to understand their recommendations for improving cervical cancer screening experiences for their community. Data from these interviews were analyzed through thematic analysis.
Results:
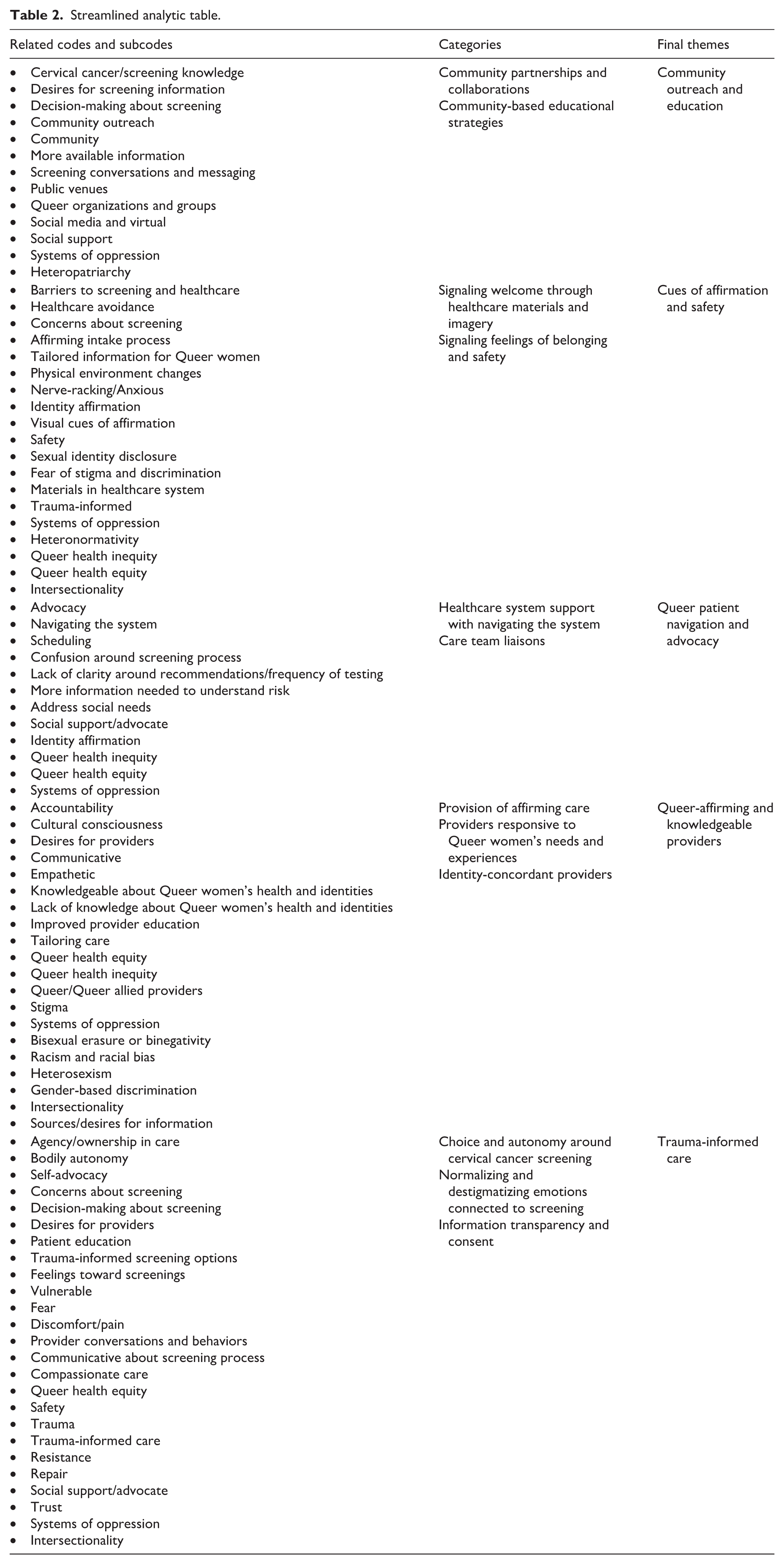
We identified five themes around creating an ideal cervical cancer screening experience among Queer women: (1) community outreach and education, (2) cues of affirmation and safety, (3) Queer patient navigation and advocacy, (4) Queer-affirming and knowledgeable providers, and (5) trauma-informed care.
Conclusion:
Engaging Queer women in developing solutions to address screening disparities is a missing link in cervical cancer prevention and the advancement of reproductive health equity. We share actionable strategies at the healthcare professional, community, and organizational levels to support healthcare systems in translating Queer women’s visions into practice. Our findings also inform medical organizations, expert panels, and health authorities on patient-defined strategies and pathways to remedying screening inequity.
Plain language summary
Cervical cancer screening helps prevent, find, and treat cervical cancer. However, Queer cisgender women have lower rates of cervical cancer screening than heterosexual women. The goal of this study is to explore perceptions of an ideal cervical cancer screening exam among a racially and ethnically diverse group of Queer women. We led interviews with Queer women to understand their recommendations for improving cervical cancer screening experiences for their community. We found five themes from these conversations, including: (1) community outreach and education, (2) cues of affirmation and safety, (3) Queer patient navigation and advocacy, (4) Queer-affirming and knowledgeable providers, and (5) trauma-informed care. We share strategies to support healthcare systems in translating Queer women’s visions into practice.
Keywords
Introduction
Cervical cancer is the third most common gynecologic cancer 1 in the United States, with 13,360 new diagnoses and 4320 deaths expected to occur by the end of 2025. 2 Routine cervical cancer screening is a powerful tool in the prevention, early detection, and diagnosis of precancers and cancer 3 and a critical part of reducing cervical cancer incidence and mortality.4,5 Yet, a growing body of literature reveals that Queer cisgender women (e.g., women who identify as bisexual, pansexual, lesbian, Queer, and otherwise non-heterosexual) experience striking disparities in cervical cancer screening access and uptake.6–12 Nearly one-third of young adult lesbian and bisexual women have not received a cervical cytology test (e.g., Pap test) in the last 3 years. 11 In a study using data from the National Health Interview Survey, sexual minority individuals had 46% lower odds of ever receiving a Pap test compared to heterosexual individuals. 8 Further, a 2024 study found a 10% lower prevalence of up-to-date screening rates among lesbian, gay, and bisexual women compared to heterosexual women. 10 These disparities are exacerbated among Queer Asian/Pacific Islander women, 13 Queer Black women, 14 and Hispanic sexual minority individuals, 8 likely owing to systemic factors such as gendered racism and heterosexism.
Barriers to cervical cancer screening among Queer women are multifaceted, including factors across the individual, interpersonal, organizational, and structural levels. For instance, individual and provider misconceptions related to Queer women’s reproductive health,15–18 non-affirming provider communication,18,19 lack of insurance coverage and cost of screening,7,20 lack of access to primary care, 10 and previous experiences of discrimination and stigma19,21,22 adversely influence screening access and uptake. While researchers have gained a better understanding of the multi-level barriers that shape screening disparities among Queer women over the last decade, research examining Queer women’s perspectives on facilitators to screening remains scarce. 23 Furthermore, Queer women’s voices and visions must foreground recommendations aimed at remedying screening inequities, yet no studies have investigated Queer women’s perceptions of what would constitute a positive, culturally conscious cervical cancer screening experience.
This study fills a notable gap in the literature by qualitatively exploring perceptions on and visions for an ideal cervical cancer screening exam among a racially and ethnically diverse group of Queer women. Through our work, we seek to impact clinical practice and healthcare delivery while contributing to broader justice-based social movements aimed at transforming the culture of healthcare systems and reducing medical stigma and discrimination toward Queer women.
Working in partnership with our community steering committee, we provide strategies, rooted in reproductive justice, for translating Queer women’s visions into action to advance screening. Moreover, this study offers foundational data for future studies examining facilitators to screening uptake.
Methods
Conceptual framework
Reproductive justice served as the primary framework guiding the development and facilitation of the study (Figure 1). Reproductive justice was coined by the Women of African Descent for Reproductive Justice in 1994, and the Southern-based organization SisterSong helped to launch Reproductive Justice as a national, multi-ethnic movement. 24 Rooted in intersectionality, a theory developed by Women of Color scholar-activists25–27 and named by civil rights law professor Kimberlé Crenshaw, 28 and human rights tenets, this framework calls on researchers to identify and examine the overlapping systems of power and domination that shape reproductive healthcare access and experiences, bodily autonomy, and the complexity of reproductive health decision-making.29,30 By centering communities who have historically been marginalized, including Queer women, and focusing on root causes of reproductive health inequity, the Reproductive Justice Framework is a change-making analytic tool that supports transformation across reproductive healthcare and efforts to improve cervical cancer screening. 31 We used the framework to guide our study design and research questions, build the interview guide, and as a lens to analyze and interpret the data.

Community steering committee
Community wisdom and leadership are a cornerstone of our work and integral to advancement toward reproductive justice. This project was led in partnership with PRISM, a community steering committee comprising five members who hold multiple identities as Queer cisgender women, transgender and non-binary individuals, Queer-allied reproductive healthcare professionals, and reproductive justice advocates. This multidisciplinary, racially/ethnically diverse group reflected the need for multi-identity and multi-issue solidarity within the Reproductive Justice Framework. 29
PRISM convenes virtually six to eight times each study year, guiding study decision-making across the project lifecycle. In line with equitable community-engagement approaches, our partnership extends beyond the simple elicitation of community member feedback. For instance, PRISM members developed interview guide questions, co-presented at national conferences, and led community-based research dissemination events. In preparing this article, PRISM members contributed to the interpretation of the data, organization of themes, and drafting and editing of the manuscript. Authentically and intentionally engaging communities is foundational in creating generative partnerships that honor community priorities and embodied knowledge.
Recruitment and participants
The reporting of this qualitative study aligns with the SRQR guidelines (Supplement 1). 32 Our work was performed in a community-based healthcare system in the South Puget Sound region of Washington State. After receiving approval from MultiCare Health System’s IRB (#2023/07/5), interview participants were recruited to the study through convenience sampling methods. These methods included posters within our healthcare clinics, emailed invitations to patients within our system whose demographics and screening history aligned with our eligibility criteria, discussions within our personal and professional networks, community outreach, social media posts within private LGBTQ+ groups, and chain referral among participants. Diversifying our recruitment channels beyond our personal networks helped to mitigate sampling bias. Those interested in participating in the study completed an online eligibility screening survey and provided written e-consent to take part in the interviews through REDCap. 33 During the e-consent portion of the survey, participants were provided with a detailed and accessible description of the purpose of the study and the voluntary nature of their participation, study procedures, risks and benefits, costs and compensation, and confidentiality procedures. The consent form included an option for interested participants to share if they would like to speak to the study lead before deciding whether to electronically sign the consent form and participate.
Eligible participants identified as Queer women (lesbian, bisexual, pansexual, femme, Queer, and otherwise non-heterosexual individuals), were 21–65 years old (aligning with the recommended age range within the American College of Obstetricians and Gynecologists (ACOG) cervical cancer screening guidelines), 34 resided in the United States, and either had not been screened for cervical cancer within the past 3–5 years or had never been screened for cervical cancer in their lifetime. Those under the age of 21 or over the age of 65 who met ACOG criteria to cease screening were excluded, as cervical cancer screening is not recommended. Among those who completed the eligibility screener and provided informed consent, 33 individuals were eligible for the study. Recruitment continued until data saturation was reached, the point at which there is sufficient data to develop a rich understanding of the study phenomenon due to the repetition of comments within participants’ narratives. 35 Our final sample included 19 participants.
Data collection
The study’s PI and first author (DW) led semi-structured interviews with participants from January to May 2024. She is a Black woman and health equity researcher who has worked alongside the LGBTQ+ community for over a decade. She also holds doctoral-level training in qualitative interviewing. Although our team shared recruitment information through personal networks, the PI had no established relationship with any participants prior to the interviews. All interviews were held virtually and recorded through our healthcare system’s HIPAA-compliant videoconferencing platform. These discussions lasted 60–90 min, and participants were compensated with $100 in appreciation for their time.
The interview guide was developed in partnership with PRISM members, drawing upon relevant literature,19,36–40 the Reproductive Justice Framework, and our personal and professional expertise to shape the questions. The study lead piloted the initial version with PRISM, and our team’s clinical lead to improve credibility and trustworthiness of the guide and made refinements based on their feedback. Our final questions explored messaging around cervical cancer; knowledge, attitudes, and beliefs about cervical cancer; screening behaviors and barriers; communication and relationships with reproductive healthcare providers; and recommendations for improving screening (Supplement 2). This article reports relevant themes related to screening recommendations. Interview recordings were transcribed verbatim using HIPAA-compliant transcribers. We replaced participants’ names with ID numbers and participant-selected pseudonyms for identity protection and the reporting of the results in this paper.
Data analysis
Two team members with training and expertise in qualitative methodologies (DW and LF) developed the codebook within Dedoose (v10.0.35, SocioCultural Research Consultants LLC) qualitative data management software. Like DW, LF had no previous relationship with study participants. The majority of the codes were developed inductively, including codes related to the cervical cancer screening process. We included a number of a priori codes (e.g., systems of oppression, resistance, body autonomy) from the Reproductive Justice Framework to ensure our analysis remained grounded within this lens (Table 1).
Deductive codes, rooted in reproductive justice.

We analyzed the data using thematic analysis, 41 a widely utilized qualitative analytic approach that is used to identify patterns within and across participants’ lived experiences, perspectives, and behaviors. 42 Before beginning the coding process, we immersed ourselves in the data by reading each transcript several times, revisiting reflective notes written during the interviews for additional context. We then independently applied inductive and deductive codes and subcodes to meaningful sections or sentences within the data. As we coded, we each created digital memos within Dedoose (v10.0.35, SocioCultural Research Consultants LLC) to track our ideas related to the excerpts and identify emerging patterns. Whenever new codes were created or alterations were made to existing codes (e.g., renaming or merging codes), we revisited our transcripts to account for these updates. All coding progressions and revisions were carefully documented within an audit trail maintained by the PI to track our decision-making processes and mitigate bias during analysis. DW and LF held regular debriefing meetings throughout this process to adjust the codebook if needed, assess the consistency of code applications, and discuss memo reflections. When discrepancies arose in our code utilization, we reviewed the excerpt(s) in question, explained our meaning-making process, and clarified our interpretations of the data until reaching a mutual understanding.
Once coding was complete, our team organized the codes into categories, merged categories into initial themes, and used an analytic map to determine relationships between these three elements. We refined initial themes at the coded excerpt level and dataset level, identifying further patterns across these two levels of data. We then finalized and defined each theme, in partnership with PRISM members (Table 2). Employing triangulation 43 throughout our coding and analysis process (e.g., involving multiple perspectives and investigators) helped enhance validity in our findings.
Streamlined analytic table.
Results
Participants ranged in age from 21 to 59 years old (Table 3). More than half of the participants were White (57%, n = 11), while 42% (n = 8) were People of Color. Around one-third of participants identified as lesbian (n = 7), 25% identified as Queer (n = 5), 21% identified as bisexual or pansexual (n = 4), and 15% used multiple labels to describe their sexual identity (n = 3). For most participants, more than 3 years had passed since their last cervical cancer screening (57%, n = 11), though more than one-quarter (31%, n = 6) had never been screened in their lifetime. Our analysis generated five themes around creating an ideal cervical cancer screening experience among Queer women, described in detail below.
Participant demographics.

Community outreach and education
Despite the desire among most individuals to better understand cervical cancer screening recommendations and the screening process, participants described an absence of readily available resources relevant to Queer women when seeking information. Participants also noted an overwhelming silence around cervical cancer within LGBTQ+ community spaces in comparison to conditions that disproportionately impact Queer men. Thus, participants called for more intentional outreach and education around cervical cancer screening within the community, as an ideal screening exam includes Queer women having culturally relevant resources that support informed and empowered decision-making. Community events, such as Pride celebrations, were mentioned as important venues for sharing such information: Every Pride, there’s always some sponsor for HIV and AIDS. I always see some type of banner for that. I feel like if we could have something out there about getting screened for HPV or cervical cancer, that would be beneficial within our own community. Because that’s how we can ensure that our people are being protected is by talking amongst one another. (Amaya Lynn, Gay and Queer, Latina/x, age 22)
Undoubtedly, outreach and education within Queer-centered spaces can help build Queer women’s trust toward screening and create opportunities for dialog around prevention as a form of community care.
Public campaigns tailored to Queer women were also discussed as a desired outreach and education strategy, especially given the role of several sexual health campaigns in increasing HIV and sexually transmitted infection (STI) testing within the LGBTQ+ community. Lane provided an example of this, saying “in the Queer community, we pay attention to campaigns. So, if you get something more outward like an advertisement, that could increase screening” (Lesbian, Gay, and Queer, Latinx, age 41). As Queer women may not have access to or participate in LGBTQ+ spaces and community groups, outreach and education strategies should also occur more broadly across the community to maximize their reach. This sentiment was shared by Karlie, who envisioned multidisciplinary collaborations between healthcare systems and institutes of higher education to provide Queer women in college more opportunities for exposure to cervical cancer screening information.
I’m currently in college, so healthcare providers need to collaborate with institutions and get people to reach out. I go to a liberal arts school where there’s a lot of Queer women. Just reach out more and not have it just be in the hospital room. (Karlie, Queer, Black, age 23)
Meeting Queer women where they are, as Karlie mentioned, could help close informational gaps around cervical cancer screening for young Queer women and facilitate pathways to timely screening.
Finally, participants spoke of wanting in-person and virtual spaces for dialog around screening to support community-building and solidarity among Queer women. Some individuals, like V, imagined healthcare providers facilitating these spaces, sharing, “providers can have meetings for Queer women to discuss screening. . .and let them know how important it is” (Lesbian, Black, age 59). Others, such as Violet, described a virtual space by and for Queer women centered on mutual aid and sharing embodied knowledge, “[I’d like] being a part of some online community if you can’t get that support from your actual healthcare provider, you can get it from a community where you can feel safe. Maybe not medical information but general advice that you might need healthcare-wise that could only come from someone that’s Queer” (Queer, Ukrainian/Nepalese, age 22). Though different in context, within both V and Violet’s comments is a vision for social support and connection; both types of spaces could create a beneficial infrastructure for answering screening questions, alleviating screening concerns and fears, and connecting Queer women to further affirming resources.
Cues of affirmation and safety
Participants discussed the importance of viewing LGBTQ+ affirming information and imagery within clinics, describing how these materials create emotional and psychological safety for Queer women. Given the historical and contemporary entrenchment of heteronormativity within the healthcare system (e.g., beliefs that privilege heterosexuality as the “norm,” leading to inaccurate and biased assumptions about Queer women’s sexual identity and reproductive needs44,45), many Queer women understandably anticipate discrimination when seeking cervical cancer screening. Tori Gable discussed how cues that indicate belonging, such as rainbow flags and brochures with health information specific to the LGBTQ+ community, help mitigate these fears and engender reassurance among Queer women.
It would be so nice to see anything saying that offices, clinics, or hospitals are supportive of the LGBTQ community, just because there is so much discrimination and hate. And a lot of people in the community feel like they’re not going to get the same quality or maybe horrible service at those places. Having a poster up, brochures, something visual when you’re in the waiting room looking around, it helps ease anxieties around that. (Tori Gable, Gay or Lesbian, Black and White, age 54)
Many participants echoed Tori Gable’s sentiments that clinic waiting rooms and lobbies shape their first impressions of the healthcare system, influencing “whether they can let their guard down a little bit” (Kyle, Queer-leaning bisexual, White, age 37). Accordingly, the absence or presence of materials and messaging reflective of Queer women’s lived experiences and needs sets the tone for the screening exam before interacting with medical staff or their provider. Participants additionally emphasized a sense of safety in clinic spaces with trans-affirming images and photos representing racial/ethnic and body diversity. Queer women are not a monolith; therefore, visual cues must reflect a multitude of identities and demonstrate support toward communities that Queer women share solidarity and affinity with.
Language and questions on intake paperwork were also described as an opportunity to signal safety for Queer women: Throughout the intake questionnaire, [I’d like] non-gendered options, questions about identity pronouns, and unassuming questions about my sexual history, goals, and concerns. That would make it clear that this is a safe space for me. (Syrena, Queer, White, age 35)
Syrena’s comment highlights how forms that encourage the sharing of sexual orientation, gender identity, and pronouns (SOGI-P data) and allow for gender-neutral, non-assumptive ways of reporting one’s sexual and reproductive health history communicate a desire to thoughtfully understand Queer women’s identities and unique health needs.
While participants’ narratives illuminate the importance of affirming and representative cues within the healthcare system, these signals alone are not enough to provide high-quality reproductive care to Queer women. Amaya Lynn (Gay and Queer, Latina/x, age 22) spoke of this saying, “if your physicians genuinely aren’t affirming, that’s a bigger issue. It’s not enough to have a Pride flag up and be like, ‘Yeah, we’re affirming here.’” Indeed, Queer-affirming materials must be part of larger justice-based efforts and actions to advance culturally responsive reproductive care for Queer women, including affirming behaviors from healthcare professionals.
Queer patient navigation and advocacy
Central to participants’ vision of an ideal screening exam was the desire for Queer-affirming patient navigators or trained community advocates (e.g., healthcare professionals or practitioners who assist in care coordination and mediation, patient education, resource linking, and emotional support46–48) to provide support throughout the screening appointment, answer questions, and serve as a liaison to their reproductive healthcare team. Though participants acknowledged that some healthcare systems have existing navigation or advocacy programs, majority are not specific to Queer women’s needs, such as addressing misperceptions around cervical cancer screening risk. Furthermore, individuals within these roles often have limited expertise relevant to Queer women’s health. Navigators and advocates who are trained in LGBTQ+ health could provide improved emotional and informational support to Queer women over those with more general health training, as described by Chelsea: Something that would be so incredibly helpful is if different clinics or providers had somebody within their office almost like an ambassador. Somebody there that if you have questions specific to those sorts of unique needs that we have, or if you have concerns around anything, somebody that would be there for the LGBTQ community to go to. I know that most places have a patient advocate, which I have tried to go through that route before. But I feel like knowing that there’s somebody there for LGBTQ+ specific topics would be helpful. It’d be really reassuring. It would make me feel more comfortable and confident talking to somebody in that sort of position versus just a normal patient advocate. (Chelsea, Pansexual, White, age 39)
A common narrative across multiple interviews was the challenge of scheduling screening appointments and navigating the healthcare system. Specifically, extensive wait times for access to care, stress from advocating for oneself during appointments, and the overwhelming nature of the healthcare system were highlighted as barriers to cervical cancer screening. While these needs are not exclusive to Queer women alone, Beatrice illuminates how access to Queer-affirming navigators or advocates could help mitigate these barriers by providing scheduling assistance, sharing an overview of the screening process, and advocating for Queer women during their exam.
In my case, I’m already struggling with my mental health. Then it’s like, this is in your hands now, make your own appointment, get on these waiting lists, we’ll see you in six months, you be vigilant and do this and that. As much as I think it is important that women are able to advocate for themselves, sometimes you just can’t, and you need other people to help you. . .welcome you into the process [of screening] and guide you. Without a roadmap, it’s just easy to get overwhelmed. (Beatrice, Lesbian, White, age 22)
Beatrice’s reflection also underlies the compounding difficulties that individuals with mental health conditions may experience when seeking and navigating healthcare. As Queer women experience mental health disparities compared to heterosexual women, owing to socio-structural factors such as anti-Queer discrimination and violence, Queer-specific navigation and advocacy programs could serve as a critical, trauma-informed resource for bridging gaps in screening, scheduling, and uptake.
Queer-affirming and knowledgeable providers
Another aspect of participants’ vision for an ideal screening appointment included more Queer-affirming providers with expertise regarding Queer women’s reproductive health. Many participants recounted receiving reproductive care from providers with inconsistent knowledge about their health and identities and experiences of intersectional heterosexism (e.g., the system of power that centers and values heterosexuality, contributing to the systemic erasure, exclusion, and discrimination against Queer communities in medical systems49,50), binegativity (e.g., negative attitudes and stereotypes about bisexual individuals, such as harmful assumptions that bisexual people are “going through a phase”
51
), and sexism enacted by providers. From these experiences, participants voiced a desire to receive cervical cancer screening from providers reflective of their intersectional identities whenever possible, such as Karlie who shared, “I would like more female providers. It would be nice if they were Queer too and People of Color” (Queer, Black, age 23). Identity-concordant providers can bring a deepened sense of understanding around Queer women’s lives, increasing feelings of comfort, affirmation, and relatability as exemplified by Violet and Jade: I would definitely pick the queer/trans provider because I just would feel more comfortable and more seen, and it would also feel more relevant. There’s an automatic connection that happens. (Violet, Queer, Ukrainian/Nepalese, age 22) Having Queer providers themselves. That is the first dream, right? When you are sharing space with people that share some kind of identity with you, it allows your nervous system to just relax in some way. (Jade, Lesbian, Mexican/Indigenous, age 34)
Expanding Queer representation and visibility within reproductive healthcare cannot be achieved without establishing more pathways to support Queer students and residents pursuing careers in medicine and incorporating an equity-based lens into recruitment, hiring, and retention policies and practices within healthcare systems. “We need more Queer visibility in hiring [in healthcare]. . .it goes back to education and graduate school and medical school. That influences who gets hired” (Polar Bear, Queer, East Asian, age 48).
Participants also wanted more intentionality around the LGBTQ+ health education offered to healthcare providers as a meaningful step toward an equitable screening exam. While multiple healthcare systems have mandatory LGBTQ+ competency training, limited forms of accountability are in place to assess whether providers thoughtfully engaged with the material, especially when training occurs asynchronously online. Therefore, though there remains a need for expanded provider education around Queer women’s health, training initiatives must be in tandem with mechanisms that can measure tangible progress toward health equity. “Having Queer- and trans-inclusive care education on how to be a better provider, even if you don’t share these identities, should be mandatory. But ideally, it can’t just be ‘okay, I did it.’ There should be somebody checking what’s actually happening after” (Jade, Lesbian, Mexican/Indigenous, age 34). Furthermore, Queer women need to be able to easily locate the providers who hold LGBTQ+ expertise when scheduling screening exams.
It would be nice if you could look up an OBGYN or a gynecological doctor who has knowledge of my community and my needs and concerns. I would rather go see somebody who is invested in understanding and knowing how to care for a Queer woman out of their own interest. I would pick that person over somebody who didn’t. But that’s not published anywhere. (Lucy Knudson, Lesbian, White, age 53)
While online databases of LGBTQ+ providers exist, their availability varies based on geographical regions, and they are not consistently updated. Additionally, individual healthcare systems do not always have LGBTQ+ specific filters for searching providers, making it challenge to discern who might specialize in Queer medicine. As Lucy Knudson shared, ensuring that Queer women can readily access information on Queer-affirming providers would help connect them to high-quality, culturally conscious cervical cancer screening.
Trauma-informed care
All participants highlighted trauma-informed care principles and strategies as integral to an ideal cervical cancer screening experience. One approach discussed was the necessity of providing Queer women with choices and options to support their empowered decision-making and encourage collaboration with their provider.
Explain if self-swabbing is an option. If I ever express reserve or reservations or fear about the pelvic exam, talk about what there might be for different trauma-informed care options. (Syrena, Queer, White, age 35) [Providers] should say “let’s have a conversation around [screening]. That doesn’t mean we have to schedule anything right away. We’ll come up with a plan that works for you.” Maybe it’s planning it on a day when you have therapy after, doing therapy just prior, or suggesting some relaxation techniques. (Tori Gable, Gay or Lesbian, Black and White, age 54)
Sharing accommodations and choices that are possible before, during, and after screening prioritizes patient-centered care and can help providers better address screening stress and anxiety. Beatrice and others added that part of respecting Queer women’s choices also means honoring body autonomy. Participants want their providers to explicitly verbalize that “your consent is the most important thing, and we can stop if you need” (Beatrice, Lesbian, White, age 22 ), instead of leaving Queer women to question whether they have a voice in the pace and completion of an exam.
Effective patient–provider communication is a critical component of a high-quality screening exam; however, communication desires and informational needs differ across patients, given their lived experiences. Amy Carr shared how Queer women’s unique reproductive health histories, emotions toward screening, and previous experiences of trauma might shape the depth and type of information desired within a screening appointment. Providers must consider these factors and avoid making assumptions by personalizing their communication with each patient.
Maybe, [providers] could ask, “do you want me to go into detail about what these things are [the speculum] and what we’re doing during the exam or would you rather me just summarize it?” I feel like maybe that would be helpful—because I know personally, I like to close my eyes. I don’t like to think about it too much, everything that’s happening. But I’m sure some other people would like to know specifics, and I could see that. (Bisexual, Latina and White, age 22)
While Amy Carr ideally desired less information and explanation throughout a screening, others like Violet were interested in “having everything laid out in terms of what’s gonna happen in detail” (Queer, Ukrainian/Nepalese, age 22). Consequently, an ideal screening exam includes trauma-informed communication approaches that uphold safety in patient–provider interactions and help providers avoid retraumatizing patients through their communication style.
Given the range of feelings that might be evoked during screening, including vulnerability, participants envisioned providers acknowledging the intimate nature of the exam to demonstrate empathy and compassion. “Maybe just even the acknowledgement of, ‘this is an intimate thing.’ Just acknowledgment of ‘yeah, we know this is invasive’” (Katelyn Queen, Lesbian, White, age 38). Establishing empathic relationships also entails normalizing and destigmatizing emotions like “fear and shame” by holding space for Queer women to transparently “feel all those feelings that might come up” (Alice, Queer, White, age 32). Access to trained peer counselors within the healthcare system (e.g., individuals with shared lived experiences who provide emotional support52,53), as described by Rashell, would be a meaningful resource for providing Queer women with additional opportunities to discuss their emotions and concerns before their appointment and debrief the exam post-appointment.
I would love to see a peer counselor pre-visit to address concerns or trauma issues to be able to help people work through that before the procedure. And then to also have that resource after, to sort through those emotions. I think that would make such a difference. Just having somebody understanding that can help you work past the clinical part. (Rashell, Lesbian, White, age 35)
Given participants’ desire for Queer navigators and advocates, peer counselors could also be included within this affirming support model.
Discussion
Though cervical cancer is preventable through routine screening, alarming disparities persist in Queer women’s access to and uptake of cervical cancer screening. Researchers and healthcare professionals must equitably involve Queer women in identifying and defining recommendations to promote screening uptake among their community to address these disparities meaningfully. In this novel qualitative study, we examined recommendations for improving cervical cancer screening engagement, the healthcare system environment, and affirming screening experiences among a racially and ethnically diverse group of Queer women. Queer women’s recommendations for an ideal experience spanned five themes, including community outreach and education around screening, cues of affirmation and safety within the healthcare system, Queer patient navigation and advocacy, Queer-affirming and knowledgeable providers, and trauma-informed care practices enacted by providers. We propose several actionable strategies to support the implementation of these recommendations and the advancement of health equity in cervical cancer prevention (Table 4).
Cervical cancer screening recommendations and implementation strategies.

Our results demonstrate a need for expanded outreach and education around cervical cancer to improve Queer women’s linkage to cervical cancer screening information and services. Leveraging Queer patient advocacy or community health worker outreach models54,55 could address Queer women’s informational needs while deepening community trust around reproductive healthcare services. Attending community events, health fairs, and cultural celebrations and building equitable partnerships with community-based organizations are two tangible strategies to support advocates and community health workers in effectively reaching Queer women. The establishment of these outreach models aligns with participants’ endorsement of in-person and virtual spaces for screening dialog among Queer women. While healthcare systems do not traditionally offer such opportunities, advocates and community health workers could facilitate these discussions in partnership with Queer-affirming community organizations, providing an innovative pathway for co-learning, community-building, and screening uptake. Online crowdsourcing, as mentioned by some participants, also has an important place in mutual learning among Queer women. 39 Given the pervasiveness of health mis/disinformation across online platforms, 56 connecting moderators of online Queer communities to reputable screening resources would improve justice-based information sharing and informed decision-making around screening.
Participants noted that displaying health materials and images specific to the LGBTQ+ community within healthcare system lobbies and waiting rooms can help signal acceptance while fostering a sense of belonging, reassurance, and comfort among Queer women attending screening appointments. Though these efforts might seem small and are more focused on micro-level shifts, 57 literature shows that LGBTQ+ individuals frequently seek signs of affirmation when entering spaces where rejection and discrimination are anticipated or frequent.58–61 Accordingly, clinical “objects,” such as posters on walls, are neither mundane nor passive as they convey messaging that elicits emotional responses (e.g., fear, uncertainty, safety). 62 Healthcare systems can create a more welcoming environment within their public and private spaces by including posters, magazines, educational materials, brochures, and pamphlets inclusive of Queer women’s health needs and experiences. By engaging with Queer women in the community through community-based participatory research, community steering committees, or community convenings, healthcare systems can better understand the materials desired by Queer women and involve them in the co-creation of culturally responsive content and messaging tailored to specific subgroups. Clinics should also work with trusted LGBTQ+ organizations on materials development and share local resources and media from such groups.
Importantly, cues of safety and affirmation also stemmed from images representing diversity beyond sexual identity. Indeed, even as healthcare systems strive to signal safety, not all spaces are safe for those who are navigating different forms of intersectional privilege and oppression. 62 The portrayal of diversity across race and ethnicity, gender, and body shape and size can contribute to the disruption of normativity in imagery and demonstrate critical consciousness in creating spaces that feel welcoming for a multitude of communities who have been historically excluded in healthcare, including Queer women with multiply marginalized identities. Participants’ commentary around desiring inclusive intake forms also has important implications for cervical cancer screening uptake, as Queer women who disclose their sexual identity to their provider have an increased likelihood receiving a Pap test.6,11 Using forms that avoid gendered, heteronormative language could help Queer women feel more comfortable communicating about their identity, reducing cervical cancer screening disparities. Moreover, intake conversations about Queer women’s sexual histories should include separate questions on their identity, partners, sexual practices, and past screening experiences to prevent conflating this information or making incorrect assumptions about patients’ cervical cancer risk. 63 Providers can reference frameworks from the National LGBT Health Education Center and the Sexuality Information and Education Council of the United States (SIECUS) 64 for language and guidance on taking an affirming sexual health history. Because safety is a core principle in trauma-informed care, implementing more Queer-affirming cues into the healthcare system can help advance healing-centered orientations to care at the clinical and organizational level. 65
Participants’ calls for more Queer-affirming and knowledgeable providers align with existing literature on culturally insensitive and discriminatory reproductive healthcare experiences among Queer women.19,39,66,67 Interestingly, there was limited discussion on training needs for front-desk staff and other healthcare professionals who are part of the cervical cancer screening care experience, despite their role in shaping early impressions of appointments before patients interact with their provider. As previous experiences of negative and discriminatory healthcare can shape decisions to delay or avoid routine care in the future, 68 it is imperative to advance LGBTQ+ clinical responsiveness and cultural consciousness among all reproductive healthcare professionals and staff who may interact with Queer women through ongoing training and education efforts. Systemic changes in organizational culture cannot be achieved from initiatives that value training completion alone, as noted by participants. Tangible shifts toward culturally responsive care must include opportunities for ongoing, in-person learning that fosters thoughtful engagement and guided discussion around unpacking intersectional power dynamics within the healthcare system, unlearning and addressing bias, and actionable strategies for promoting reproductive health equity. To mitigate time and scheduling constraints, these learning opportunities could be integrated into all staff meetings, morning huddles, and resident didactics lessons. Accountability mechanisms, such as metrics for assessing progress toward LGBTQ+ clinical responsiveness and transparent reporting around training outcomes to the community, should be established to support more meaningful changes rooted in equity.
Our findings on desires for more providers reflective of participants’ overlapping identities are consistent with literature on preferences for LGBTQ+ identity-concordance within the healthcare system.19,69 Though most studies have focused on the benefits of race and gender concordance, increasing Queer visibility and representation might be a promising approach to improving trust between Queer women and their provider, 70 increasing cervical cancer screening uptake. 71 Strategies for diversifying the healthcare workforce could include establishing more scholarship and support programs for Queer students and trainees pursing healthcare careers, connecting students and trainees to healthcare professional mentors to support their professional development and educational retention, partnering with LGBTQ+ organizations to foster community-based pathways to medicine, and implementing policies and practices that uphold equity in healthcare hiring, promotion, and retainment (e.g., benefits policies that support LGBTQ+ families, hosting Queer affinity groups). In addition, offering an LGBTQ+ provider directory and including online filters for LGBTQ+ care specialties when scheduling appointments can help Queer women locate affirming providers more readily.
Participants’ commentary on trauma-informed care underscores the importance of choice, shared decision-making, patient-centered communication, and provider humility in creating an ideal screening exam. Notably, some participants expressed a desire for the option of HPV self-collection, in place of clinician-collected HPV testing or cervical cytology (e.g., Pap tests) that necessitate a speculum exam. This approach holds great potential to increase screening rates among Queer women, especially among those who have experienced trauma.72,73 HPV self-collection can improve physical and phycological comfort by allowing patients to collect their own cervical cancer screening samples in clinical settings without undergoing a speculum examination.72,73 Our findings expand on recent research from LeBlanc and colleagues, 63 illuminating patient-centered recommendations around trauma-informed care practices that may advance screening equity. While participants’ proposed reproductive justice-based strategies and behaviors are critical to improving Queer women’s sense of safety and agency throughout a screening exam,74–76 the consistent implementation of trauma-informed care remains a challenge across healthcare systems.77,78 This is troublesome as 66% of Queer women reported seeking treatment for trauma in the 2022 National LGBTQ+ Women’s Community Survey, 79 and trauma history can adversely impact cancer screening behaviors. 80 Efforts to improve trauma-informed care implementation in reproductive healthcare require multi-level changes that consider the social-structural and historical experiences that shape Queer women’s lives. Aligning trauma-informed care principles with system policies and protocols can support more universal and sustainable trauma-informed care implementation. 78 In addition, providing healthcare professionals with protected time and resources to engage in continuing, trauma-informed care education would expand their ability to recognize the signs and impact of trauma among Queer women, integrate trauma-informed care into practice, and reflexively examine and address biases and power dynamics that hinder equitable care for Queer women.75,81 Embedding Queer-affirming peer counselors, navigators, and advocates into trauma-informed care models might further expand compassionate support for Queer women before and after their screening while mitigating provider time constraints and burnout. 82
Limitations
The majority of participants resided in the Western part of the United States, meaning recommendations might differ across geographical contexts, especially within states lacking explicit LGBTQ+ nondiscrimination protections in healthcare. 83 Furthermore, even though our study included a racially and ethnically diverse sample of participants, more than half of participants were White (57%). Future research including more Queer Women of Color is needed to more comprehensively understand how the intersections of racism, sexism, heterosexism, and additional forms of oppression shape recommendations for improving cervical cancer screening. As participants did not distinguish between healthcare settings during their discussions (e.g., primary care clinics, OBGYN clinics), further research is needed to determine how Queer women’s cervical cancer screening visions and priorities might differ across varying healthcare environments. Finally, we note that clinical workflows and healthcare system resources have implications for the implementation of our recommendations. Healthcare systems could embed these recommendations into system-wide quality improvement initiatives or align them with existing health equity or patient safety metrics to support integration into clinic workflows and optimization of processes. Furthermore, engaging healthcare system leaders and administrators and community-based organizations as thought partners is critical in the allocation of resources toward implementation efforts, especially in relation to healthcare professional training and the availability of Queer-affirming navigation, advocacy, and peer counseling services.
Conclusion
Cervical cancer screening disparities remain a pressing concern among Queer women. However, Queer women’s perspectives on factors that shape positive and culturally responsive screening exams remain understudied. Engaging Queer women in developing solutions to address screening disparities is a missing link in cervical cancer prevention and the advancement of reproductive health equity. Grounded in community engagement and reproductive justice, our findings reveal Queer women’s five visions for an ideal cervical cancer screening exam. We share actionable strategies at the healthcare professional, community, and organizational level to support healthcare systems in translating these visions into practice. Our work also provides foundational data for examining and contextualizing facilitators for screening uptake in future research. As national recommendations for promoting health equity within cervical cancer screening lack specificity for Queer women, 63 findings from this work can inform medical organizations, expert panels, and health authorities on patient-defined strategies and pathways to remedying screening inequity.
Supplemental Material
sj-pdf-1-whe-10.1177_17455057261428108 – Supplemental material for “Give me the sense that I matter:” Queer women’s recommendations for an ideal cervical cancer screening exam and pathways to screening equity
Supplemental material, sj-pdf-1-whe-10.1177_17455057261428108 for “Give me the sense that I matter:” Queer women’s recommendations for an ideal cervical cancer screening exam and pathways to screening equity by Deana M. Williams, Shawn Reilly, Tanisha Lord, Kara Ayers, Sage Kissiah-Grove, Marissa Robinson, Lyda Fong and Joseph Angel in Women's Health
Footnotes
Acknowledgements
We express deep gratitude to the participants of this study for sharing their stories.
Ethical considerations
This study was approved by the MultiCare Health System IRB (#2023/07/5).
Consent to participate
Participants provided written consent to take part in the interviews.
Consent for publication
Participants provided written consent for their de-identified data to be used in publications.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this work is funded through the Andy Hill CARE Fund, Washington’s Cancer Endowment (Grant number IDCT-06).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Anonymous transcripts are available upon reasonable request from the corresponding author, depending on permission from MultiCare Health System IRB. The data are not publicly available due to privacy restrictions.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.