
Abstract
Background
Disrespectful care violates women’s rights, delays care-seeking and contributes to preventable adverse birth outcomes. Although Respectful Maternity Care (RMC) is a key strategy for improving maternal and neonatal health, evidence on factors affecting its implementation in least-developed countries remains poorly synthesised.
Objective
To assess the barriers and facilitators of RMC in low-income countries.
Design
Systematic review synthesising evidence from qualitative and mixed-methods studies was conducted.
Data sources and methods
A systematic search was conducted across major databases, including Scopus, Web of Science, PubMed, CINAHL, and Embase. Eligibility criteria were defined using the SPIDER framework. Studies published between 2015 and 2025 were included. Methodological quality was assessed using JBI SUMARI for qualitative studies and the QATSDD tool for mixed-methods studies. SPIDER framework was applied to support eligibility criteria. The review followed PRISMA guidelines. The data were synthesised using thematic analysis and applied to the Socio-Ecological Model.
Results
Forty-eight studies conducted in least-developed countries were analysed, consisting of 36 qualitative studies and 12 mixed-methods studies. Barriers and facilitators to RMC were identified at individual (knowledge, attitude, skills), interpersonal, organizational (resources, infrastructures), policy (guidelines, education), and socio-cultural level (norms, cultures).
Conclusion
Strengthening RMC is crucial for reducing maternal and neonatal mortality. The review highlights the need for supportive policies, improved infrastructure, and targeted provider training. Future research should develop and validate context-specific RMC principles and indicators to strengthen providers’ understanding and skills for practice in least-developed countries.
Registration
The protocol was registered with PROSPERO (CRD42023443998).
Plain language summary
This review examined what facilitates and what challenges respectful maternity care (RMC) in least-developed countries. After analysing 48 studies, the review found that barriers and facilitators exist at multiple levels, including individual knowledge and attitudes, relationships between care providers and patients, health facility resources, national policies, and wider cultural norms. Strengthening RMC is essential to reduce maternal and newborn deaths. The review highlights the need for better policies, improved health system infrastructure, and targeted training for healthcare providers. It also recommends developing RMC guidelines and measures tailored to the local context.
Introduction
Despite global improvements, adverse childbirth experiences and preventable maternal deaths remain concentrated in low-resource settings. 1 In 2023, the global maternal mortality ratio (MMR) was 223 per 100,000 live births, with 60% of these deaths occurring in low-income countries (LICs), particularly in Sub-Saharan Africa. 2 These rates exceed the Sustainable Development Goal target of fewer than 70 deaths per 100,000 live births by 2030, requiring a much faster annual decline than currently observed. 3 Respectful Maternity Care (RMC) is recognised as a key strategy for improving maternal health outcomes and reducing mistreatment, and is strongly endorsed by the World Health Organization (WHO). 4
WHO defines RMC as the care that safeguards a woman’s dignity, privacy, and confidentiality, ensures protection from harm and mistreatment, and facilitates informed choice and continuous support during the perinatal period. 4 This person-centred care should be provided for all women, gender-diverse people, neonates, and families. 5 RMC has also been found to be a significant indicator of maternal and newborn health improvement.4,6 However, the global provision of RMC remains inadequate, with around 54% of women experiencing mistreatment during childbirth. 7 This indicates that mistreatment of women during childbirth is a global concern affecting healthcare systems. 8
Most incidents of mistreatment occur in LICs, where limited resources, awareness, and insufficient data hinder the advancement of RMC. 9 Recent studies conducted in LICs regions shows that women often face insensitive, harsh, disrespectful, or abusive treatment during childbirth.10,11 Evidence from Sub-Saharan and Eastern African countries indicates that nearly half of women giving birth in healthcare facilities experienced mistreatment.12,13 A study conducted in four low resource countries found that 41.6% of women (n = 2,016) observed during labour and childbirth in healthcare facilities experienced physical or verbal abuse and discrimination based on personal attributes. 14 This study also reported that often procedures like caesarean sections, episiotomies, and induction of labour were performed without consent. 14
Mistreatment harms women psychologically, physically, erodes trust and communication, normalises poor treatment, limits informed decision-making, and is linked to poor obstetric outcomes.15–17 Such mistreatments undermine women’s relationships with their newborns, families and future contact with health care services.14,18 These negative experiences often lead to reduced engagement, compromised decision-making autonomy, and ongoing feelings of disrespect. 19
Understanding the factors that contribute to women’s negative experiences is essential for advancing RMC. 5 WHO categorises factors influencing RMC into policy-related, sociocultural, organizational, and individual drivers. 5 These factors can be further understood using frameworks such as the Socio-Ecological Model (SEM), which examines how personal, social, and environmental influences interact to shape practice. 20 The model highlights multiple levels of determinants, intrapersonal, interpersonal, institutional, and broader environmental or societal factors and suggests that changes can promote positive experiences. 20 Successful implementation of RMC in LICs requires a clear understanding of the drivers of RMC, as perceived by both the women receiving care and the healthcare providers delivering it. 21 Although a substantial body of research addresses this topic, the drivers of RMC in least-developed countries have not been comprehensively synthesised.
Review aim
This systematic review aims to synthesise primary studies to answer the question, “What factors facilitate or impede RMC implementation in least-developed countries from the perspectives of women and healthcare providers?”
Methods
The reporting of this study conforms to the PRISMA guidelines. 22 This systematic review followed the JBI approach for qualitative systematic review. 23 The protocol was submitted to the PROSPERO database (International Prospective Register of Systematic Reviews) with the registration number (CRD42023443998).
Theoretical framework
We applied SEM to assess barriers and facilitators of RMC in LICs. 20 The SEM provides a structured approach for examining individual, interpersonal, organizational, and community factors across diverse settings.20,24 This model has been used by WHO in their compendium of RMC, which assessed factors affecting RMC; in a systematic review on the barriers and facilitators to maternal healthcare in East Africa 25 ; a study on negative childbirth experiences of Dutch women 26 and studies that explored women’s and care providers’ perspectives on mistreatment during childbirth.27,28
Although other frameworks such as the Theoretical Domains Framework (TDF)
29
and Normalisation Process Theory (NPT)
30
could be used to explore drivers of RMC, they have limitations. TDF focuses on individual behaviours but lacks a systems-level perspective,
29
while NPT examines social processes but does not fully address external policies, organizational structures, and cultural factors.
30
Therefore, in this review, the SEM is the most suitable framework compared to other theoretical models. The detail is presented in Figure 1. Socio-ecological model to study drivers of RMC in least-developed countries.
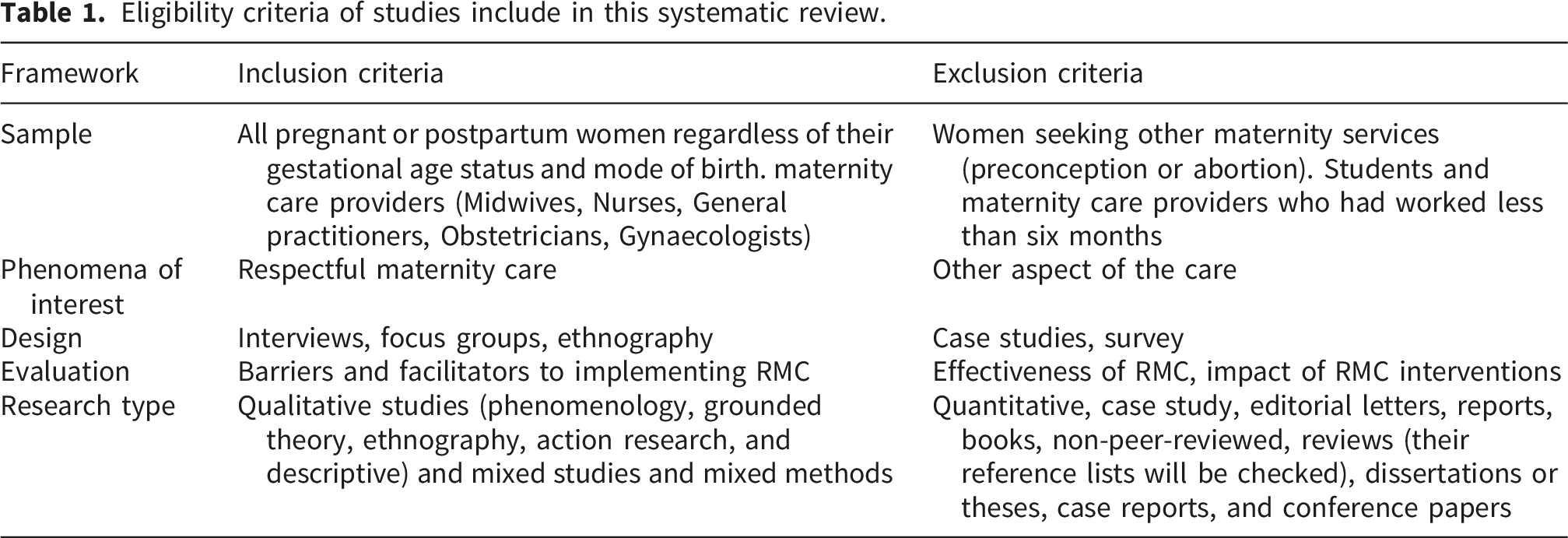
Eligibility criteria
Eligibility criteria of studies include in this systematic review.
Search strategy
The search strategy comprised specific headings, MeSH, keywords, and free text search terms, with truncation and wild cards to enhance sensitivity across each database. The strategy involved searching for primary articles based on the eligibility criteria. Initially, a preliminary search was conducted on PubMed to locate relevant publications. Scopus, CINAHL, Embase, PubMed, and Web of Science were systematically searched. To identify additional relevant studies, we also manually reviewed the reference lists of included papers. An example of the search strategy using the keywords found in the titles, abstracts, MeSH, and index terms of pertinent publications is available in the supplementary files (Supplemental file S1). The reference list of each study selected for critical appraisal was examined for additional relevant research.
Study selection
All identified citations were first uploaded to EndNote and then imported into Covidence, where duplicates were removed. 33 Subsequently, two independent reviewers screened titles and abstracts to determine whether they met the eligibility criteria. Potentially relevant articles were retrieved, and full text articles were imported into the Covidence system. 33 Two independent reviewers carefully evaluated the complete text of chosen citations against the inclusion criteria. Any conflicts or discrepancies between the two primary reviewers were resolved through discussion with a third reviewer. A Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) flow diagram (see Supplemental file S2) was used to illustrate the search results in the final report, including a comprehensive description of their findings. 22
Assessment of methodological quality
The standardised critical appraisal instruments from JBI SUMARI were employed to evaluate the methodological validity of the qualitative studies. 34 The overall score was assessed on a scale of ten, with the range of 8-10 being deemed as high quality, 4-7 as fair, and 0-3 as low quality (Supplemental file S3). The Quality Assessment Tool for Studies with Diverse Designs (QATSDD) 35 was utilised for quality assessment of mixed method studies. This tool was selected due to its good inter-rater reliability (k = 71.5%) and ability to highlight the methodological strengths and weaknesses of studies. 35 The QATSDD offers a range of scores, where 0 to 14 indicates a low-quality study, 15 to 28 indicates a moderate or fair quality study, and 29 to 42 indicates a high-quality study 36 (Supplemental file S3). In instances where additional information was required for clarity, the authors of the paper were contacted. Discussion between reviewers enabled consensus.
Data extraction
The standardised JBI data extraction tool 34 was used by two independent reviewers. Extracted data included the title, authors, country, and publication year of each study. Information on the population, study method, sample size, context, setting, and culture were also collected. Additionally, data on enabling or facilitating factors, impediments or barriers were extracted. Qualitative data themes or subthemes with corresponding illustrations were assigned a credibility level.
Data synthesis
Data were synthesised using the SEM as a framework. 24 Subthemes were first developed by grouping findings with similar meanings, and these subthemes were then organised into broader themes. 37 Each theme was mapped onto the appropriate domain of the SEM (individual, interpersonal, institutional, health system, and sociocultural). 24 Supporting the SEM, this review used Bohren et al.’s (2015) evidence-based framework to define key aspects of RMC. 38 The Bohren et al. framework identifies seven interconnected domains of mistreatment during facility-based childbirth: physical abuse, verbal abuse, sexual abuse, stigma and discrimination, failure to meet professional standards of care, poor rapport between women and providers, and health system conditions and constraints. 38 This structured approach ensured consistency and accuracy in interpretation, strengthening the quality and reliability of review findings.
Results
Search results and study characteristics
The search retrieved 12,058 articles from the following databases: Scopus (n = 2,514), PubMed (n = 2,910), Web of Science (n = 2,821), CINAHL (n = 2,401) and Embase (n = 1,405). Seven references were sourced through citation search (n = 7). After identifying and removing duplicates (n = 6,927), a total of 5,131 titles and abstracts were screened, leading to the exclusion of 4,916 irrelevant studies. Consequently, 215 studies were selected for full-text analysis. Forty eight studies satisfied the inclusion criteria, comprising 36 qualitative studies,27,28,39–72 and 12 mixed methods studies.73–84 The detail is presented in Figure 2. PRISMA flow chart of the article selection for barriers, and facilitators of respectful maternity care in low-income countries, 2025.
The review included studies from Ethiopia (n = 20), Tanzania (n = 9), Afghanistan (n = 3), Malawi (n = 4), Zambia (n = 2), Madagascar (n = 1), Mali (n = 1), Mozambique (n = 1), Rwanda (n = 1), Uganda (n = 1), Zimbabwe (n = 1), Guinea (n = 1), Myanmar (n = 1), Zambia and Mali (n = 1) and Zambia and Tanzania (n = 1). A summary of findings is presented in Supplemental file S4.
Quality appraisal results
Overall, most studies demonstrated moderate to good quality. Nine mixed-methods studies and twelve qualitative studies were rated as high quality. The review team used an inclusive appraisal approach to capture strengths and limitations, enhancing the reliability of findings. Detailed scoring for each JBI SUMARI and QATSDD domain was provided in Supplementary File S3.
Barriers and facilitators of RMC implementation in low-income countries
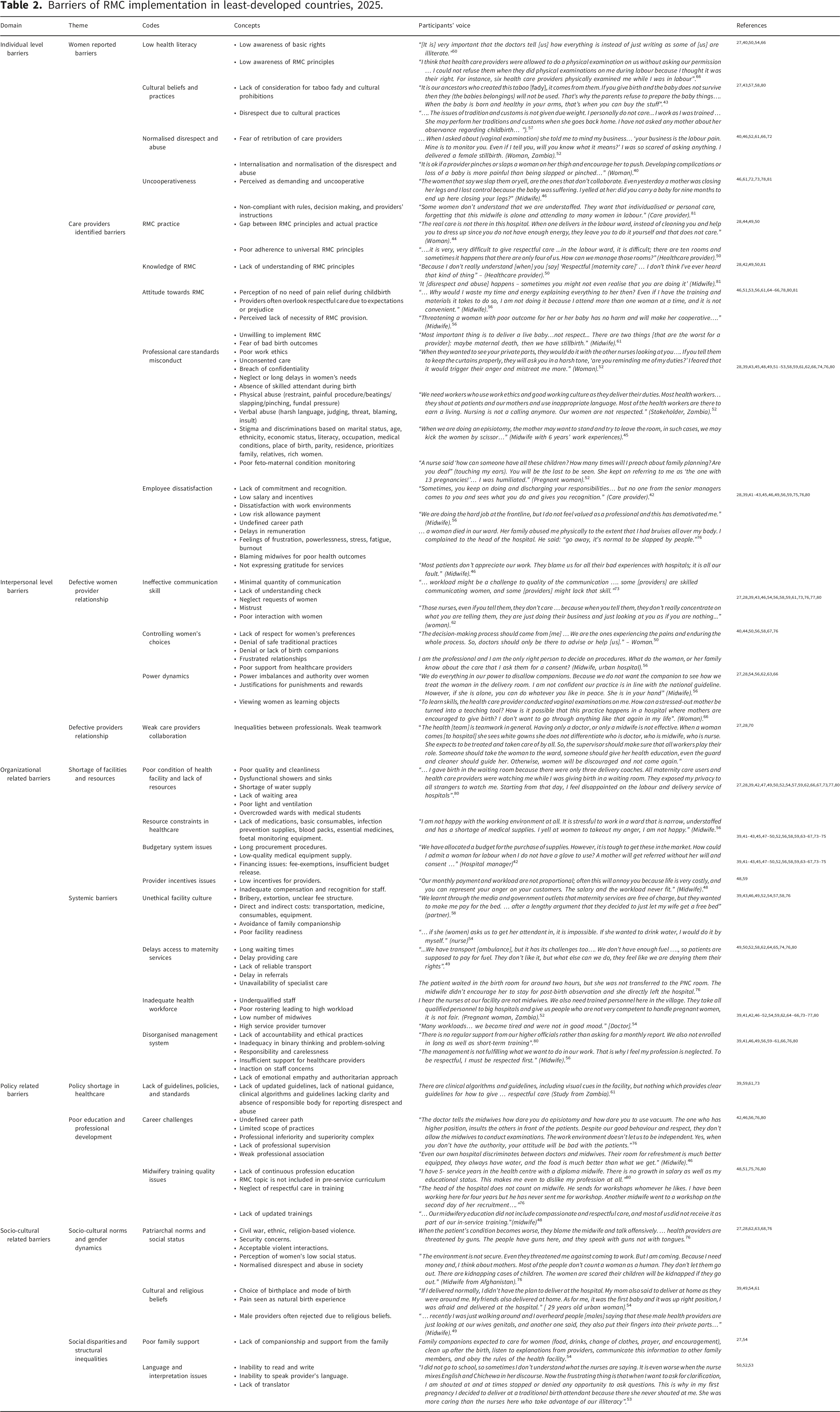
Barriers of RMC implementation in least-developed countries, 2025.
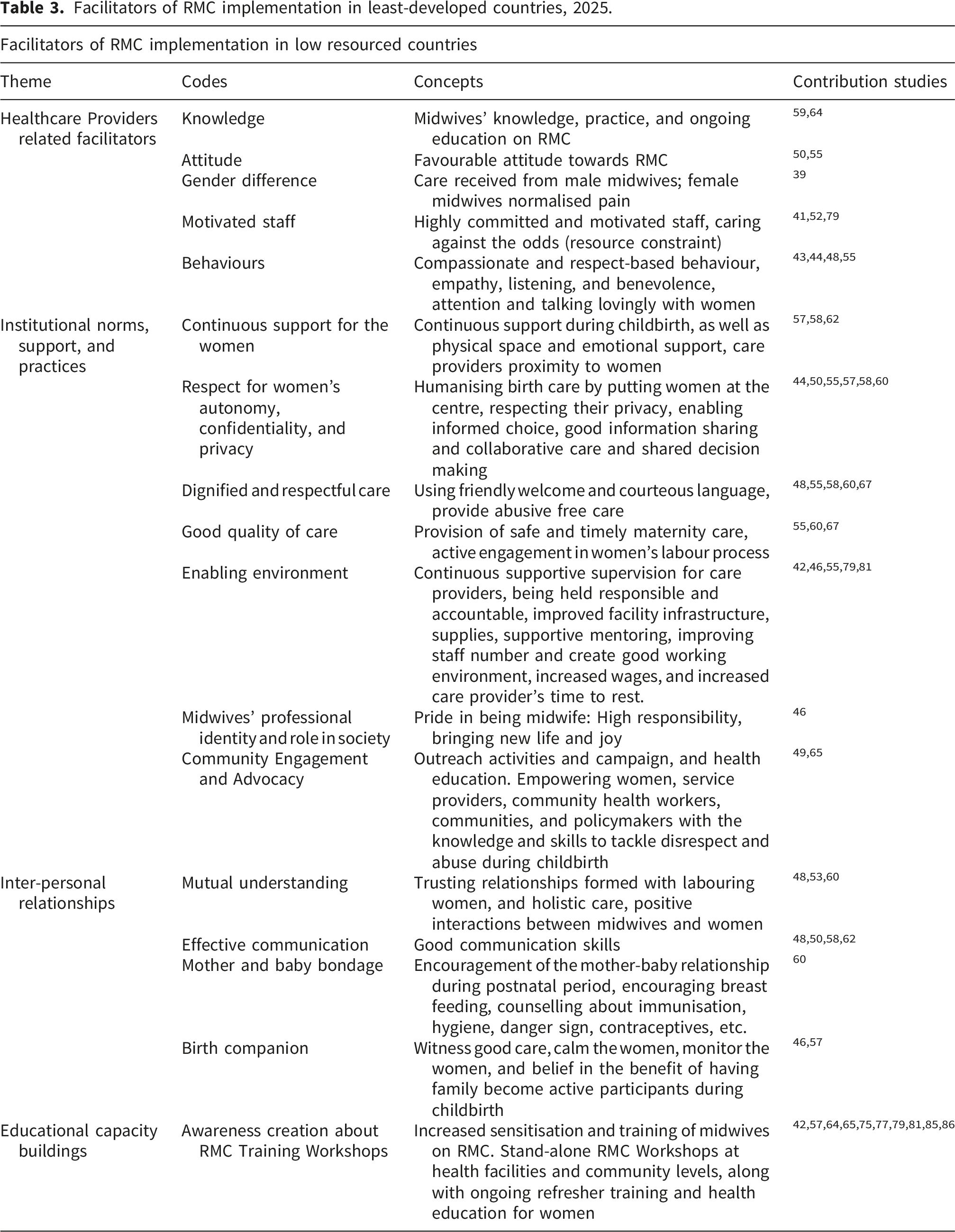
Facilitators of RMC implementation in least-developed countries, 2025.
Individual barriers
Women-identified barriers
Women’s limited health literacy and lack of awareness of their rights contributed to mistreatment.40,50,54,66,75 Lack of consideration for their culture and traditions by staff exposed many women to disrespect.43,57,80 Many women internalised and accepted mistreatment as normal,40,66 while others reported feeling pressured into remaining silent.40,52
Most women faced discrimination based on their socio-economic status and ethnic background.39,45,46,51–53,61,76 There were reports of painful vaginal examinations, no informed consent, confidentiality breaches, neglect, and delays during care.45,48,58,59,80 Most women reported a lack of emotional support from their care providers.43,49,58,76 Many mothers also report verbal abuses.51,53,58,59,74,80 Care providers’ favouritism and bias toward wealthier or socially connected clients undermined respectful care to less fortunate women.39,52,66 Women reported punishment from care providers for improper clothing, not carrying their birthing materials/documents, and late arrival.62,63
Healthcare providers-identified barriers
Unfavourable attitudes,46,51,53,56,61,64–66,78,80,81 limited knowledge,42,49,50,81 and inadequate skills among staff were self-reported barriers of RMC.44,49,50 Healthcare professionals were observed using force, including physical restraint, fundal pressure, 45 and other forms of physical violence during labour.59,80 Many care providers mistreated women due to frustration, stress, fatigue, and burnout.39,41–43,45,46,49,56,75,80 Disrespect toward midwives by some family members and blaming them for adverse birth outcomes hindered their ability to provide respectful care.39,46 Care providers reported that women’s ‘uncooperative’, ‘disobedient’, and ‘aggressive’ behaviours were barriers to delivering RMC.45,46,54,61,72,73
Individual facilitators
Good understanding, attitudes and motivation
In some settings, improving midwives’ knowledge and practices, and providing ongoing education served as key facilitators of RMC.59,64 Care providers with favourable attitudes toward RMC were more likely to implement it effectively.50,55 Strong staff commitment and motivation facilitated improvements in RMC.41,52,79 Compassion, kindness, and empathy were key provider behaviours that facilitated RMC.43,44,48,55 Prioritising women’s needs, respecting their privacy, supporting informed choices, and fostering collaborative care all facilitated RMC.44,50,55,57,58,60 Using friendly, courteous language and providing abuse-free care were positive factors that enhanced RMC.48,55,58,60,67
Interpersonal barriers
Poor women-provider communication
Inadequate communication skills among care providers39,58,59,73,76,77,80 and poor interactions with women hindered the provision of RMC.27,28,43,46,54,59,61 Women were often excluded from care decisions,58,67,76 leading to distrust.44,50 Language barriers and the lack of available translators further contributed to misunderstandings and increased the risk of mistreatment.52,53
Weak healthcare team collaboration
Perceived professional hierarchies, with doctors ranked above midwives and nurses, hindered RMC quality. 42 RMC implementation was also hindered by disorganised management, lack of accountability, and unethical practices.39,41,60 Poor supervision, ignored staff concerns, and authoritarian management styles exacerbated mistreatment.41,46,49,59,66,76
Interpersonal facilitators
Good interpersonal relationships
Positive care provider/s-woman interactions, trust, and holistic care facilitated RMC implementation.48,53,60 Effective communication between care providers and women enhanced understanding and cooperation.48,50,58,62 Encouragement and support of the mother-baby relationship during the immediate postnatal period also facilitated RMC. 60
Organizational-level barriers
Poor facilities and shortage of resources
Healthcare facilities in low-resource countries often lacked essential medications, consumables, privacy screens, bed linen, infection control supplies, blood packs, and fetal monitoring equipment.39,41–43,45,47–50,52,56,58,59,63–67,73–75 Generally the low standard of facility construction, limited space or overcrowding, lack of water and sanitation, as well as inadequate lighting and ventilation were recognised barriers.39,42,47,49,50,52,54,57,59,62,66,67,73,77,80 Lengthy procurement processes, low-quality equipment, and inadequate financing 42 were reported. Low pay, poor incentives, and staff shortages contributed to disrespectful care.42,48,59
Systemic barriers
RMC was diminished in cultures where disrespect and abuse are normalised, bribery was evident, healthcare costs for patients were high, and family companionship during labour and birth was restricted.39,43,46,49,52,54,57,58,76 High workloads and long shifts further hindered RMC.39,41,42,46,48–52,54,59,62,64–66,73–77,80 For women, long waiting times, deficient electronic systems/record keeping, transport and referral delays, and limited access to services and specialists, contributed to poor RMC.49,50,52,62,64,65,74,80
Organizational level facilitators
Good institutional norms, support, and practices
Facilitators of RMC included safe, effective, and timely care, as well as high-quality service.55,60,67 Other facilitators included managerial support, better infrastructure, mentoring, staff development, higher wages, and staff-friendly rostering.42,46,55,79,81 Allowing companionship during childbirth was found to significantly enhance RMC implementation.46,57
Policy level barriers
Lack of guidelines and policies
Policy-related barriers to RMC included poor adherence to existing policies, unclear RMC core principles and indicators, outdated evidence and clinical algorithms, lack of national guidance, and the absence of a designated entity or process for reporting mistreatment.39,59,61,73 Lack of standardised measurement methods and varying guideline interpretations among care providers further hindered effective implementation.44,49
Poor education and professional development
In several settings, midwives reported limited access to, and insufficient ongoing professional development and training.39,49,61,65,73,75 Other barriers included the omission of RMC from pre-service training, lack of updated evidence-based resources, and weak professional associations.51,75,76
Policy level facilitators
Capacity building and professional motivation
RMC implementation was strengthened through capacity-building initiatives, including training and health professional education.42,57,64,65,75,77,79,81,85,86 Additionally, professional pride in being a midwife was believed to support the provision of respectful care. 46
Societal-related barriers and facilitators
Socio-cultural related barriers
Societal acceptance of disrespect, intimate partner violence, and civil conflict create environments that limit RMC implementation.40,76 Unmet societal expectations regarding birth practices and traditional customs can further inhibit RMC.49,62 Cultural norms that reduce women’s autonomy and social status limit their ability to make decisions about birthplace, mode of birth, and companionship during childbirth.54,62,63,68
Socio-cultural related facilitators
Health promotion education that empowers women and communities facilitates respectful care.49,65 Continuous support from companions during childbirth, along with emotional support from family, also enabled RMC in several settings.57,58,62
Discussion
The Socio-Ecological Model (SEM) provides a structured framework for analysing the barriers and facilitators of RMC across multiple levels.20,24 In this review, drivers of RMC were identified at the individual, interpersonal, organizational, policy, and socio-cultural levels. The synthesis of these drivers was guided by the Bohren et al. (2015) framework. 38 Consistent with the SEM, Bohren et al. (2015) highlighted that poor RMC arises from both individual behaviours and broader systemic factors. 38 According to the socio-ecological framework challenges such as inadequate provider knowledge, limited resources and institutional support, and cultural norms cannot be addressed in isolation.20,38
The application of the SEM in this review enabled a more comprehensive understanding of drivers of RMC that may otherwise have been overlooked. At the individual level, many women in LICs demonstrated limited health literacy and poor awareness of their rights to respectful care.40,50,54,66 This aligns with a study in Southeast Nigeria, which found that most women have low awareness of their basic human rights and perceive healthcare providers’ disrespectful behaviours as normal. 87 Such gaps in understanding might stem from broader system-level issues, like inadequate education for women from healthcare about RMC. 70 SEM emphasises that individual behaviours are shaped by interconnected factors like interpersonal, and institutional factors. 20 For example, care providers reluctance to support women was influenced by their perceptions of labouring women as unfriendly, difficult, uncooperative, unappreciative, and aggressive.88–90 Ige et al. (2022) further noted that women’s negative reactions may partly reflect unmet expectations, indicating the reciprocal dynamic between women and care providers. 90 Through the SEM lens, these interpersonal tensions can be understood as emerging within organizational and structural environments that offer limited support, foster power imbalances, and fail to prioritise respectful care. 5
At the intrapersonal level, factors like knowledge, attitudes, skills, and intentions of care providers can influence the provision of care. 20 In this review limited knowledge, negative attitudes, and abusive practices among maternity care providers impeded RMC delivery in low-income countries. 91 This may be due to the lack of RMC in pre-service training or undergraduate education and ongoing training. 87 Midwives working in LICs often reported feelings of underappreciation, and frustration, which may contribute to displaced aggression.72,89 Similarly, studies from Nigeria and Guinea found that poor compensation and lack of recognition hindered RMC provision.72,87 These insights show that when systems fail to protect women’s rights and prioritise respectful care, both women and midwives experience heightened frustration and a sense of powerlessness. 28
In this review, the SEM indicated that interactions between women and providers, and within care teams, were shaped not only by interpersonal dynamics but also by organizational, policy and sociocultural factors.20,88 System level barriers such as high workloads, understaffing and a culture of disrespect further shaped how providers and women engaged with each other, demonstrating the cross-level influences central to the SEM.72,87 Evidence from two Brazilian public hospitals aligns with our results, indicating that poor communication by providers was a key barrier to RMC. 92 Lambert et al. (2018) also found that miscommunication between women and providers were a major challenge to delivering quality care. 93 Conversely, increased interaction between women and healthcare providers, 4 and strong inter-professional collaboration facilitated a continuum of care that supported optimal maternal and neonatal outcomes. 94
By applying SEM, institutional level factors such as resource shortages, inadequate infrastructure and poor accountability mechanisms can be interpreted as central structural determinants of RMC rather than isolated operational issues. 27 These findings align with evidence from Nigeria, which identified poor work environments, including inadequate space, stressful hospital protocols, and lack of equipment were significant obstacles to RMC. 87 In Sub-Saharan Africa structural inequalities, health system policies, and hierarchical work environments negatively influenced staff practices. 88 Another study indicated that mistreatment during childbirth was associated with weak redress mechanisms. 87 According to SEM organizational constraints can ripple downward, influencing relationships at the interpersonal level as well as providers’ behaviours and women’s experiences at the intrapersonal level. 20 Findings supported the SEM notion that institutional systems created the conditions in which respectful or disrespectful care became normalised. 28
At the policy level, national guidelines, measurement tools and professional training shape the broader context in which maternity facilities operate.38,59,95 Weak enforcement of RMC standards and outdated guidance undermine organisational capacity and create norms that enable mistreatment. 38 Strengthening midwifery education is crucial, as standardised training improves maternal and newborn outcomes and enhances women’s care experiences. 96 WHO recommends that all women and newborns receive care from fully trained and authorised midwives. 96 Countries such as Ethiopia, Burkina Faso, Cambodia, Indonesia, and Morocco have strengthened their midwifery education and reduced maternal mortality. 97 Viewed through the SEM lens, these findings indicate that policy-level factors influence education, resource availability, provider working conditions, and women’s awareness of their rights. 20 This highlights that improving RMC requires comprehensive policy reforms, updated guidelines, high-quality midwifery education, and supportive professional environments. 5
Though majority of the studies included in this review are from Ethiopia and Tanzania, the barriers and facilitators identified are mainly distributed across the least-developed countries. Evidence from WHO guidelines indicated that normalisation of disrespect and abuse, fragile health system, patriarchy, health literacy are identified as the main causes of mistreatment. 4 This normalisation culture of disrespect and abuse in low-income countries is mainly due to power-imbalance between women and care providers, which may contribute to unprofessional behaviour and low morale. 38 In line with these findings, according to Foucault’s theory, power imbalances and the medical gaze can undermine the relationship between health care providers and consumers, thereby exacerbating experiences of disrespect and abuse. 98
Through the application of SEM in this review, we can also understand that community norms, beliefs, and collective expectations form a social environment that shapes both women’s expectations and providers’ behaviour. Our findings identified community-level factors affecting RMC such as stigma, acceptance of disrespect and abuse, cultural expectations around childbirth, domestic violence, societal hierarchies, and gender discrepancies.62,63,68,76 Similarly another study identified barriers of RMC included limited women autonomy and empowerment, as well as the normalisation of mistreatment of women in society. 87 Interpreting these through SEM showed that socio-cultural norms operate as a bridge between structural conditions and individual experiences, reinforcing or challenging facility practices. 99 Thus, sociocultural drivers identified through SEM help clarify why even well trained providers may operate within culturally embedded patterns of care. 27
This review identified several facilitators of RMC. The primary facilitators identified include improving healthcare providers’ competency regarding RMC and implementing midwife-led continuity of maternity care. Healthcare providers’ understanding of RMC can be improved by educating them on the core principles of RMC. 6 This education includes providing women with clear information, supporting informed decisions, maintaining privacy, ensuring safety, delivering abuse-free care, and ensuring continuity of care with a familiar caregiver throughout perinatal period. 6 These core principles strengthen the midwife-led continuity of maternity care model, which prioritises women-centred care.
Midwifery-led continuity of care had a significant positive impact on maternal and neonatal health. 100 Evidences from low and middle income countries support expansion of midwife-led care models, which enhance respectful interactions, reduce unnecessary interventions, and improve birth experiences. 101 Although the effectiveness of Midwifery-led continuity of care in resource-limited settings is well-documented, evidence concerning its feasibility in under-resourced settings remains fragmented. 102 Healthcare systems should invest in midwife-led continuity of care, offer education about respectful care, and establish environments that allow midwives to practice to their full scope while prioritising women’s needs. 103
Limitations
This review used a rigorous method for gathering evidence, synthesising data, and organising findings. This is the first systematic review to explore barriers and facilitators of RMC in low-income countries. Although we implemented thorough searching strategies in five databases and reviewed the reference lists of systematic and other literature reviews, we may have missed some critical studies. As only studies published in English language were included, this review may have missed relevant studies published in other languages. Despite a comprehensive search across all low-income countries, no eligible studies were identified from Angola, Bangladesh, Benin, Bhutan, Burkina Faso, Burundi, Cambodia, Central African Republic, Chad, Djibouti, Eritrea, Gambia, Guinea, Haiti, Micronesia, Kiribati, Lao Peoples Democratic Republic, Lesotho, Liberia, Mali, Mauritania, Niger, Sao Tome and Principe, Senegal, Sierra Leone, Solomon Islands, Somalia, South Sudan, Timor-Leste, Togo, Yemen, Comoros, Democratic Republic of the Congo, Sudan, and Tuvalu. Consequently, insights from these countries are lacking, highlighting a significant gap in up-to-date evidence and the need for further research. Because most studies focused on facility-based experiences, there was limited insight from research on community-based births. Furthermore, the lack of a meta-analysis, together with the limited number of studies in certain categories, restricted the generalisability and interpretability of findings.
Conclusions
This review presented a synthesis of barriers and facilitators of RMC at the individual, interpersonal, organizational, policy, and socio-cultural levels using the SEM as a framework. This review found that barriers and facilitators to RMC were not only women-related but also influenced by healthcare provider behaviours, experiences in the workplace and society in which women lives and births. The main barriers identified were care providers’ limited knowledge, inadequate skills, and abusive behaviours. To improve providers’ proficiency in RMC, we recommend implementation of RMC core principles, particularly tailored to the context of low-income countries. 6 These principles include providing care that is free from abuse, attentive, informed consent, autonomous, confidential, equitable, safe, respectfully communicated, culturally sensitive, and offered in optimal birth setting. 6 These core principles were validated based on WHO quality of maternity care standards. 38
Administrators, policymakers, and healthcare facilities should consider the identified barriers and facilitators when planning further interventions. Higher education institutions should integrate RMC into pre-service educational programs related to maternity care. Healthcare institutions should ensure that maternity care providers receive updated education on RMC while on duty.
Supplemental material
Supplemental material - Overcoming barriers and harnessing facilitators: Respectful maternity care in least-developed countries - a systematic review
Supplemental material for Overcoming barriers and harnessing facilitators: Respectful maternity care in least-developed countries - a systematic review by Ephrem Yohannes, Gonfa Moti, Eshetu E. Chaka, Laura Gabriel, Debra K. Creedy, Carolyn Hastie in Women's Health
Supplemental material
Supplemental material - Overcoming barriers and harnessing facilitators: Respectful maternity care in least-developed countries - a systematic review
Supplemental material for Overcoming barriers and harnessing facilitators: Respectful maternity care in least-developed countries - a systematic review by Ephrem Yohannes, Gonfa Moti, Eshetu E. Chaka, Laura Gabriel, Debra K. Creedy, Carolyn Hastie in Women's Health
Supplemental material
Supplemental material - Overcoming barriers and harnessing facilitators: Respectful maternity care in least-developed countries - a systematic review
Supplemental material for Overcoming barriers and harnessing facilitators: Respectful maternity care in least-developed countries - a systematic review by Ephrem Yohannes, Gonfa Moti, Eshetu E. Chaka, Laura Gabriel, Debra K. Creedy, Carolyn Hastie in Women's Health
Supplemental material
Supplemental material - Overcoming barriers and harnessing facilitators: Respectful maternity care in least-developed countries - a systematic review
Supplemental material for Overcoming barriers and harnessing facilitators: Respectful maternity care in least-developed countries - a systematic review by Ephrem Yohannes, Gonfa Moti, Eshetu E. Chaka, Laura Gabriel, Debra K. Creedy, Carolyn Hastie in Women's Health
Footnotes
Acknowledgements
We extend our sincere gratitude to Ambo University and Griffith University School of Nursing and Midwifery for their generous permission to conduct this study.
Ethical considerations
This study is a systematic review of publicly available studies, and ethical approval was not required.
Authors’ contributions
EY was actively involved in the study’s design, drafting and conceptualisation. EY and GM engaged in article selection, data extraction, interpretation and analysis. CH, DC, LG, EE, and GM provided substantial feedback and contributed meaningfully to the refinement of the manuscript. All authors contributed to the critical revision and editing of the manuscript’s intellectual content. All authors have read and approved the final version of the manuscript. All authors agreed to be accountable for all aspects of the work, ensuring that any questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All relevant data to the review are included in the paper or uploaded as an additional file.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.