
Abstract
Obesity is a global health concern linked to prediabetes, hypertension, sarcopenia, osteoporosis, and cardiovascular disease. However, body mass index (BMI) has limited sensitivity, misclassifying over half of individuals with excess adiposity as having normal weight. Growing evidence identifies a subgroup with normal BMI (18.5–24.9 kg/m2) but elevated body fat (>25% in men, >30% in women), termed normal weight obesity (NWO). Women are at a two-to six-fold higher risk of developing NWO compared to men. To investigate this, an expert review of the literature was conducted utilizing PubMed, Scopus, and Google Scholar to explore the impact of excess adiposity in the context of NWO, emphasizing female physiology across the lifespan and its influence on skeletal muscle and bone health. Many women with NWO remain unaware of underlying hormonal or menstrual dysregulation until challenges arise with fertility or during mid-life transitions. Metabolic disturbances during perimenopause occur independently of obesity but are likely worsened by excess adiposity despite a normal BMI. In postmenopause, the shift from estradiol to estrone and overall estrogen reduction accelerates bone resorption, leading to declines in bone density and strength, and increased fracture risk. Genetic variations in fat distribution, lean mass, and body proportions further modify disease risk among racial and ethnic groups. In women, increased adipose tissue often occurs in the hips and gluteal regions, predisposing to fatty acid infiltration within muscle (myosteatosis), which has been associated with reduced muscle quality outcomes (e.g. muscular strength) and increased falls in older adults. Increasing skeletal muscle mass may improve adiponectin levels, supporting metabolic health, while leptin dysregulation promotes lipid accumulation and inflammation. Higher adiposity, as seen in NWO, impairs bone microstructure and increases fragility through inflammatory pathways. In conclusion, NWO is an underrecognized yet clinically significant condition that elevates women’s risk for metabolic, hormonal, muscoskeletal dysfunction despite a normal BMI.
Plain Language Summary
A person can appear to have a “normal” body weight while still carrying too much body fat. This condition is called normal weight obesity (NWO). Because BMI only measures weight relative to height, it often misses excess fat, meaning many people with health risks are labeled as “healthy.” Women are especially affected and are two to six times more likely than men to develop NWO. This review explains how NWO impacts women’s health across the lifespan. Even with a normal BMI, higher body fat can disrupt hormones, menstrual cycles, and metabolism. Many women do not notice these issues until they experience problems with fertility or begin the mid-life transition into perimenopause. During this stage, metabolic shifts occur regardless of weight, but excess fat can make symptoms worse. After menopause, the natural decline in estrogen speeds up bone loss. In women with NWO, this bone loss is intensified, raising the risk of low bone density, weaker bone structure, and fractures. Muscle health is also affected. Women often store fat around the hips and glutes, and this can lead to fat infiltrating the muscles. This reduces muscle strength and increases the chance of falls, especially in older age. Hormones released by fat tissue contribute as well. When muscle mass is low, beneficial hormones like adiponectin decrease, while higher fat levels can disrupt leptin, increasing inflammation.In summary, normal weight obesity is a hidden but serious condition for women, raising the risk of metabolic problems, hormonal imbalances, weaker muscles, and fragile bones—even when BMI appears normal. Understanding NWO is essential for better health screening and prevention.
1. Introduction
Obesity is a worldwide health crisis associated with prediabetes, hypertension, sarcopenia, osteoporosis, and cardiovascular disease. 1 This is traditionally classified using body mass index (BMI; body weight [kg]/height2 [ m2]), where obesity is defined as having a BMI of ≥30 kg/m2. The concept of evaluating body weight relative to height was first introduced in the early 19th century by Belgian mathematician Lambert Adolphe Jacques Quetelet. Originally termed the Quetelet Index, it was designed to describe the typical weight for a given height in adults for population-level studies to assess human growth, not to evaluate individual health status or adiposity. 2 In 1972, Keys and colleagues coined the term “body mass index” (BMI). While acknowledging that BMI only accounted for a fraction of the variance in adiposity and did not capture fat distribution, they proposed it as being “at least as good as any other relative weight index” for epidemiological use as an alternative to the height-and-weight tables utilized by insurance companies. 3 In the following decades, BMI was, and still is, widely used as a population screening tool for obesity and related health risks, with standardized cutoffs defining underweight (<18.5 kg/m2), normal weight (18.5–24.9 kg/m2), overweight (25–29.9 kg/m2), and obesity (≥30 kg/m2). 4
Early research reported BMI to have low sensitivity, failing to classify more than 50% of individuals who had excess adipose tissue as having obesity.
5
Thus, there is increasing recognition of a subset of individuals with a normal BMI (18.5–24.9 kg/m2) who also carry excess adipose tissue, as determined by assessment of percent body fat (>25% for men and >30% for women) – a condition known as Normal Weight Obesity (NWO).
6
Despite normal-weight BMI, people with excess adipose tissue still often suffer from comorbidities related to obesity and are at increased disease risk, making this an important paradox to study.
7
These health conditions, such as cardiovascular disease, Type 2 diabetes, inflammation, sarcopenia (low muscle mass and strength), and osteoporosis, have implications for longevity and quality of life (Figure 1). A primary challenge in addressing NWO clinically is the lack of a universal diagnostic consensus. While NWO is consistently defined by a BMI within the normal range (18.5–24.9 kg/m2), the threshold for “excess adiposity” varies widely across the literature. For women, percent body fat cutoffs are frequently cited as >30%,
6
but other studies utilize thresholds of >33% or >35% depending on the age and ethnicity of the specific cohort.8,9 Compounding this challenge, NWO can be a hidden condition, requiring assessments beyond body weight, ideally including body composition measures such as dual-energy X-ray absorptiometry (DXA), bioelectrical impedance analysis (BIA), or air displacement plethysmography). Notably, these can also yield varying estimations of fat mass, leading to inconsistent diagnoses. Women presenting with Normal Weight vs Normal Weight Obesity. The figure illustrates the physiological differences between a healthy individual with a normal body mass index (BMI) and an individual with normal weight obesity (NWO). The yellow dots within the muscle tissue of the NWO model represent myosteatosis, or pathological fat infiltration into the skeletal muscle. Created with BioRender.com.
Recent data suggest that an estimated 30 million Americans have NWO.5,8 Of particular concern, women are at two-to-six times higher risk of developing NWO compared to men.9–11 This disparity is likely further exacerbated in women as they age, due in part to visceral adipose tissue (VAT) accumulation and changes in skeletal muscle mass (SMM) throughout menopause transition. Hormonal shifts that women experience during perimenopause, notably a decline in estrogen, are associated with increased adiposity and subsequently, cardiometabolic health outcomes.10,11 Additionally, there is evidence that a higher body fat percentage may worsen perimenopausal symptoms, suggesting that NWO status could exacerbate the negative health changes that women already face.9–11 Although NWO is highly prevalent, the limitations of BMI as a measure of body composition mean that women with NWO may not receive the targeted education needed to address these risks.Given the rising prevalence of NWO and its substantial health implications, a more comprehensive understanding of the physiological consequences of NWO throughout the female lifespan is warranted. Accordingly, this review will explore the impact of excess adiposity in the context of NWO, with a specific focus on female physiology across different stages of the female lifespan and its effects on skeletal muscle and bone health.
1.1. Adipose tissue as a metabolic regulator
Adipose tissue is the largest endocrine organ in the body, producing adipokines that influence metabolism, appetite, insulin sensitivity, and whole-body homeostasis.12–14 The adipokines leptin and adiponectin in particular influence glucose regulation, lipid metabolism, and reproductive function and their dysregulation is associated with obesity-related cardiometabolic disease, including type 2 diabetes. 15 In addition to adipokines, adipocytes also produce proinflammatory cytokines, promoting chronic low-grade inflammation that further exacerbates cardiometabolic disease risk.8,15,16 Together, the endocrine and inflammatory effects of excess adiposity extend beyond cardiovascular health, influencing sex hormone signaling, skeletal muscle metabolism, and bone turnover, making adipose tissue a central regulator of women’s health. As such, consideration of the physiological implications of excess adiposity and adipokine and cytokine dysregulation across the female lifespan is imperative.
2. Materials and methods
To comprehensively synthesize the current understanding of NWO in women, we conducted a non-systematic expert review based on specialized synthesis of the literature. Given the narrative nature of this review, quality assessment of individual studies were evaluated conceptually, and efforts were made to include literature spanning diverse age groups, racial/ethnic populations, and body composition assessment methodologies.
3. Adipose tissue: influence on female health across the lifespan
In the United States, obesity rates are higher amongst women than men
17
and women with NWO may face an additional and often overlooked risk. Beginning in puberty, transitioning through reproductive years, and into postmenopause, women experience several unique hormonal shifts that, along with genetics, race, and lifestyle, directly coincide with adipose tissue storage and distribution.
18
Estrogen, a primary female-sex hormone, impacts adipose tissue deposition and accumulation of fat in subcutaneous, visceral, and non-adipose tissues.
19
As women transition from the cyclical hormonal patterns of premenopause into the widely variable and declining hormonal patterns of perimenopause,
20
into the postmenopausal phase, the overall shifts in estrogen across these phases are associated with increased accumulation of VAT and corresponding decreases in cardiometabolic health (Figure 2). Understanding the interplay between adipose tissue and female physiology amongst NWO is critical for preventing and mitigating cardiometabolic health risk. Adipose tissue distribution across the female lifespan. As estrogen fluctuates and eventually declines through the menopause transition, women often experience a decline in muscle size and composition (i.e. intramuscular fat accumulation) and reductions in bone density (indicated by the bullets under Estrogen on the left). Simultaneously, there is a common shift toward greater central adipose tissue accumulation. Note: While the visual representation shows a larger outward anthropometric size, women with NWO specifically maintain a “normal weight” outward appearance and BMI, while their internal body fat percentage and distribution shift abnormally. Created with BioRender.com.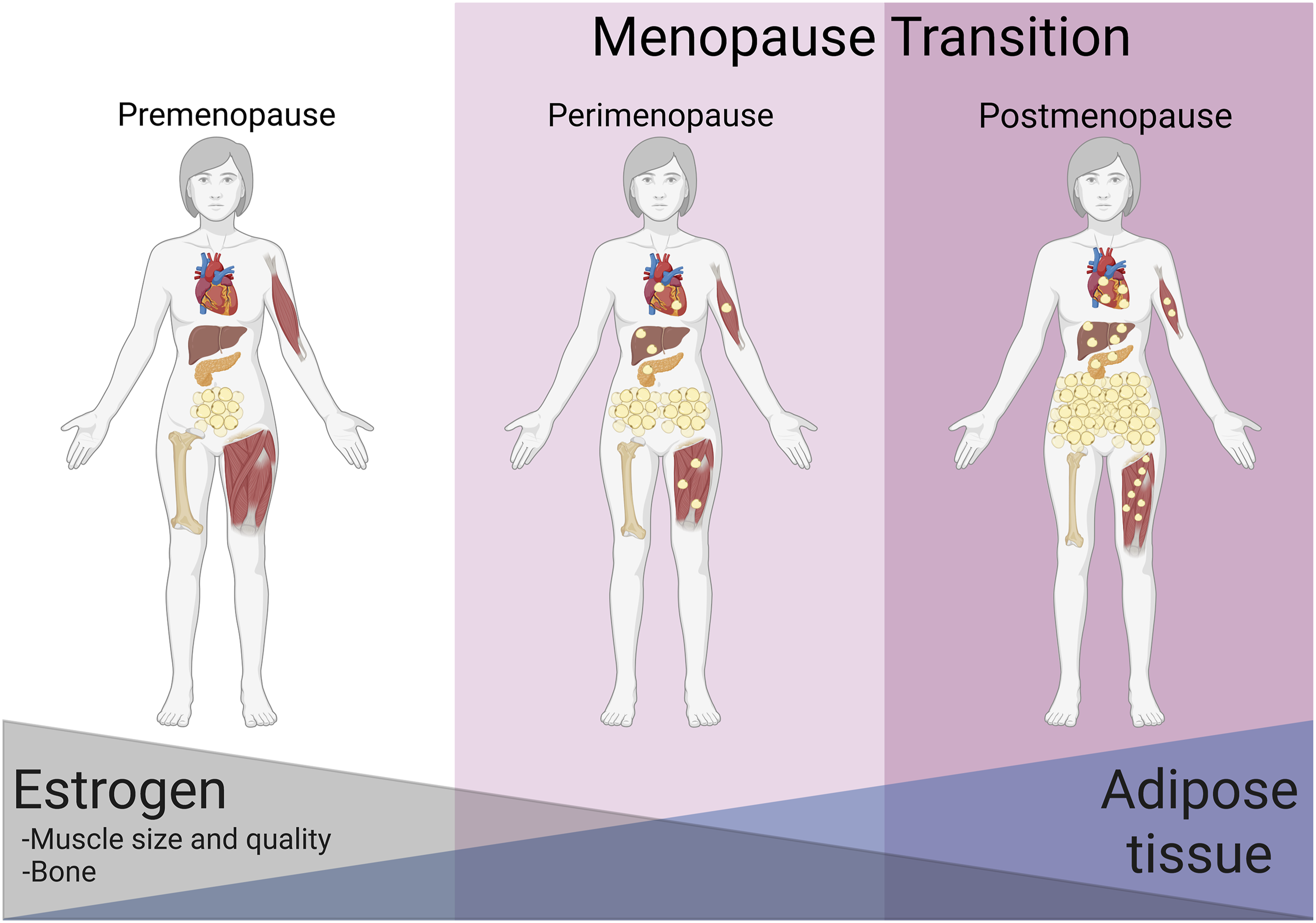
3.1. Premenopause: implications for health and reproduction
During premenopause, or the reproductive years, women have been reported to be at lower risk of cardiometabolic disease compared to men due to protective effects of high estrogen concentrations. 21 However, it is well recognized that obesity and NWO in women of reproductive age are associated with increased metabolic and disease risk. High total body and VAT contributes to chronic, low-grade, systemic inflammation, leading to disrupted metabolic homeostasis, insulin resistance, dyslipidemia, and other metabolic syndrome risk factors. Women with NWO have also been found to have lower lean mass, especially in the legs, than normal weight or overweight individuals without this condition (BMI>25 kg/m2; %BF>35%), contributing to lower metabolic rate and exacerbating cardiometabolic disease risk. 21
Less discussed in women with NWO is the potential for hormonal dysregulation, menstrual disorders, and fertility complications. In individuals with obesity, the combination of elevated leptin and reduced adiponectin disrupts the hypothalamic-pituitary-ovarian axis, contributing to menstrual irregularities and anovulation. 22 Increased estrogen production with obesity contributes to hormonal imbalances, which can lead to menstrual disturbances and greater prevalence and severity of menstrual symptoms.23,24 For example, high estrogen-to-progesterone ratio (i.e., estrogen dominance) is associated with heavier menstrual bleeding, dysmenorrhea, and irregular menstrual cycles. Furthermore, unopposed estrogen, as would occur in the presence of anovulation, can contribute to the development of more severe pathologies, including endometrial hyperplasia, endometrial polyps, and endometriosis. 25 Finally, elevated insulin levels lead to overproduction of androgens by the ovaries, creating a hyperandrogenic state characteristic of polycystic ovarian syndrome (PCOS). Elevated androgens not only interfere with ovulation but also promote VAT accumulation and chronic inflammation, and other risk factors for metabolic syndrome.22,26 Further research is needed to fully characterize sex-hormone implications, specifically in women with NWO.
A significant concern for women with NWO of reproductive age is lack of awareness. Many women with NWO are likely unaware of their heightened disease risk and may go unidentified by traditional health screenings due to their normal weight classification. Further, due to widespread use of hormonal contraception, underlying hormonal or ovulatory dysfunction often goes undetected, due to the artificial regulation or elimination of bleeds by exogenous hormones. 27 As such, lifestyle intervention may not be implemented, placing individuals with NWO at even greater risk for long-term health consequences than individuals classified as having obesity. Many women with NWO are also likely to be unaware of hormonal and menstrual dysregulation (due to masking by hormonal contraception or lack of education) until they experience difficulty conceiving and as they transition to mid-life.
3.2. Perimenopause: implications for menopause transition
There is a clear and well-documented fluctuation and eventual reduction in estrogen concentration during the menopause transition, which is often accompanied by an increase in adipose tissue mass and shift in peripheral adipose tissue storage towards central fat deposition.28–31 This shift towards VAT has consistently been associated with increased cardiometabolic risk, insulin resistance, inflammatory diseases, and cardiovascular disease. 32 This increase in disease risk and shift in adipose tissue storage is especially present in middle-aged women regardless of BMI. 33 This demonstrates a potentially more harmful perimenopause phase for women with NWO, who may be unaware of the changing risk with age/menopause.
Female hormones, particularly estrogen, play a crucial role in the endocrine function of adipose tissue. Estrogen impacts leptin secretion, which augments fat oxidation and regulates appetite. The hormonal dysregulation that occurs during perimenopause could contribute to the documented metabolic inflexibility, 33 inflammation, and weight gain during this transition. Similarly, the decline in adiponectin throughout perimenopause has been suggested as an indicator of metabolic syndrome. 34 Furthermore, menopausal symptoms have been linked with a significant reduction in quality of life and work productivity. 35 The proinflammatory nature of adipose tissue and endocrine dysregulation associated with perimenopause has been associated with greater occurrence and duration of hot flashes. 36 The metabolic dysregulation observed during perimenopause occurs independent of obesity, but having greater body fat, despite a normal BMI, likely exacerbates this disease risk.
3.3. Postmenopause: implications for aging
The postmenopausal period is marked by a significant reduction in ovarian estrogen production and a shift in the predominant circulating estrogen from estradiol to estrone, 37 which exacerbates VAT accumulation. This increase in abdominal fat heightens the risk for cardiovascular diseases, insulin resistance, and elevated inflammation.10,38,39 As the protective effects of premenopausal estrogen levels wane, the gap in disease risk between men and women narrows. 40 As demonstrated by a cross-sectional study of 634 postmenopausal women with normal BMI, those with NWO had double the odds of having at least two metabolic syndrome risk factors compared to those in the lowest tertile. 41 Reduced estrogen is also accompanied by an accelerated rate of bone resorption, leading to rapid declines in bone density and strength, heightening the risk of fragility fractures.42,43 These effects are compounded by the normal toll of aging, which starts to become more pronounced around this period, leading to further fat accumulation as well as declines in muscle size, muscle quality (i.e. intramuscular fat accumulation), and bone density.44,45 This is especially concerning for postmenopausal women, given that increases in VAT coupled with a decline in SMM and bone mineral density (BMD) are not accounted for in a traditional BMI model.
3.4. Racial and ethnic considerations
Adiposity-related disease risk varies across racial and ethnic populations and reflects a combination of biological, environmental, and sociocultural factors. Prevalence of NWO has predominately been evaluated in White populations, from North American and/or of European decent. Differences in body composition and body proportions (e.g., fat distribution, total and relative amounts of FM and SMM, limb-to-trunk proportions) can influence disease risk variation across populations. These biological differences may interact with cultural and environmental factors, including dietary patterns, physical activity/exercise, and socioeconomic conditions, which together influence overall disease risk and progression. Based on the lifespan trajectory outlined in the previous sections, identifying women who may be more susceptible to NWO could improve screening practices and inform prevention, treatment, and recommendations across the lifespan.
Asian: NWO is most prevalent in Asian populations. Up to a third of individuals in certain Asian ethnicities are considered to have NWO, 46 with the highest rates reported in South Asian ethnicities (30-40% of women classified as NWO).47,48 Women in these countries/of these Asian ethnicities have been reported to have higher prevalence of PCOS (3.5% vs. 1.6%), lower average age of menopause (46-49 years vs. 50-51 years), and younger age of endometrial cancer diagnosis (60 yrs vs. 67 years).49–51 Asian populations commonly have higher body fat percentages relative to BMI and those of South/Southeast Asian ethnicity, have a higher disposition for VAT, all contributing to higher incidence of cardiovascular disease risk factors during the menopause transition.48,52 The consistent underprediction of obesity based on traditional BMI metrics and observance of greater disease risk at lower BMI’s (i.e. NWO) in Asian populations has led to Asian specific BMI classifications that better represent associated disease risk in this population. 52 This may also improve identification and prevention of NWO and disease risk in Asian women.
Hispanic and White: For a given BMI, Hispanic women show tendencies toward central obesity (higher %trunk FM and trunk-to-limb FM ratio) compared to white women, who show tendencies toward higher indices of subcutaneous adipose tissue. 53 Reported prevalence of NWO in young Latin American (22%), and Brazilian (9%) women, suggest similar-to-lower rates than observed in the United States (33%).54–57 Higher prevalences may also be observed in older (>60yrs) Latin American women (Colombian); similar trends have been reported in postmenopausal White women.58,59 Collectively, NWO prevalence may be similar between Hispanic and White women, but abdominal obesity associated risks may be higher and of greater consideration for Hispanic women.
Black: Few studies have quantified NWO prevalence in Black populations. One study of individuals in Trinidad and Tobago reported a prevalence of 8% in young women (18-28 years) and hypothesized that diet and sedentary lifestyle had a greater contribution to NWO than genetic influences. 60 For a given BMI, Black women of reproductive age (16-33 years) tend to have lower metrics of FM and VAT, and higher metrics of muscle mass and BMD compared to both White and Hispanic women.30,53,61,62 Due to these factors, Black women may be at lower risk for NWO, compared to White and Hispanic women. While at potentially lower risk for NWO, obesity prevalence is high in Black women across all life stages and cardiometabolic risks are greater amongst Black women traversing perimenopause, compared to their White counterparts. 63 Further research is needed to quantify NWO in different racial/ethnic populations and determine how this influences health trajectory across the menopause transition.
European: Recent studies in European populations further highlight the presence and risks of NWO. Research indicates that young adult Slovak women with NWO exhibit unfavorable body composition and lifestyle habits compared to lean counterparts. 64 Specifically, physical activity has been reported as the main predictor of NWO (defined as >28% body fat) in young women (18-30 years) and are 48% less likely to have NWO if physical active >3 times/week. 65 Additionally, older Slovak women (38-59 years) with NWO demonstrate worsened lipid profiles, emphasizing that NWO is a cross-cultural risk factor across the lifespan. 66
4. Adipose tissue impact on skeletal muscle health
Large stores of adipose tissue are known to have negative effects on SMM, which, when considering total mass, is the largest organ for nutrient uptake. 67 Given that lower amounts of SMM are associated with metabolic dysfunction, one of the primary concerns associated with NWO is the deleterious effects on SMM, physical function, and muscle quality. Muscle quality represents the relationship between muscle force and total mass, reflecting various factors such as intramuscular fat accumulation, metabolic properties, thermoregulation, and myokine signaling/production. 68 Indeed, those with NWO have lower SMM and fat-free mass compared to normal weight lean counterparts.67,69 Research indicates that women with NWO have, on average, four kilograms less SMM compared to women with normal weight. 70 Further, a hallmark of NWO is the development of myosteatosis. This early compositional change leads to inflammation via the release of pro-inflammatory cytokines 71 and reduces muscular force production 67 leading to metabolic dysfunction and catabolism.
4.1. Adipose infiltration and muscle quality decline
Myosteatosis is a key mechanism of NWO that adversely affects muscle quality. This pathological phenomenon can occur between muscle and fascia (intercellular adipocyte deposition), between muscles within an individual muscle (intracellular adipocyte deposition) and within muscle cells (intramyocellular adipocyte deposition) alone. 72 Adipose infiltration into skeletal muscle has been linked to atrophy, increased anabolic resistance in sarcopenic muscle, myofibrosis and stiffness, insulin resistance, reduced muscle-specific force per unit of cross-sectional area, diminished neuromuscular activation, impaired muscle blood flow, localized secretion of proinflammatory adipokines and increased risk of lipotoxicity. 73 Myosteatosis appears to be more prevalent in women than men, with older women at an elevated risk. 72 Myosteatosis-induced inflammation compounds anabolic resistance that many older adults are already experiencing, increasing their risk of sarcopenia and physical injury. 72 Further, infiltration of fat between muscle fibers can lead to abnormal fiber orientation, reducing the muscle’s capacity for force production which can pose a risk for physical injuries and reduce quality of life. 74 In women, fat deposition is typically localized around the hips and gluteal area, making women more susceptible to fatty acid infiltration, as myosteatosis has been more commonly observed in the hip and gluteal muscles. These findings have also been linked to functional outcomes, such as more self-reported falls in older adults. 75 Overall, the severity of myosteatosis and its impact on SMM and function can vary, however; exercise and nutritional interventions have been shown to counteract its effects and improve muscle quality.72,76
4.2. Influence of adiponectin in muscle metabolism
Research highlights a strong association between increased physical activity, decreased FM, and elevated circulating adiponectin 77. Both exercise and nutritional interventions have been utilized by many populations to weight loss, and improvements in body composition, including reducing myosteatosis. A recent meta-analysis of exercise interventions showed reduced abnormal fat deposition and improved myosteatosis in older adults. 76 Further, exercise interventions have demonstrated efficacy in elevating both serum adiponectin levels and the expression of adiponectin receptors in skeletal muscle. 78 Recent research has explored whether increased SMM can increase adiponectin levels and thereby aid in metabolic regulation. It is speculated that chronic adiponectin signaling impacts calcium handling in skeletal muscle, since adiponectin regulates calcium concentrations, and therefore contractile capacity in humans. Increasing SMM levels may improve adiponectin concentrations and thereby aid in mitigating risk of metabolic dysregulation. Although the data are mixed, exercise interventions have been effective in increasing both serum adiponectin and adiponectin receptors in skeletal muscle. 78 Overall, research suggests a clear relationship between increased exercise, decreased body fat, and increased circulating adiponectin, although details regarding these relationships require further investigation.77,79 Ultimately, 79 prioritizing interventions that improve body composition or metabolic health, potentially mediated by adiponectin and increase SMM may serve as a crucial protective strategy for women with NWO, particularly as they navigate the metabolic vulnerabilities inherent to the menopause transition.
4.3. Leptin’s effect on metabolic dysfunction
Leptin receptors are present in skeletal muscle and play a crucial role in muscle bioenergetics. 80 Leptin activates AMPK in skeletal muscle, which in turn increases glucose uptake and fatty acid oxidation to prevent triglyceride storage and reduces risks of insulin resistance. 81 However, this regulatory mechanism appears to be impaired in individuals with obesity. For instance, leptin has been shown to stimulate fatty acid oxidation in muscle tissue from women with normal weight but fails to produce the same effect in those with obesity, suggesting the presence of peripheral leptin resistance in obesity. 82 Exercise, particularly resistance training, offers a promising intervention to counteract these metabolic disruptions. In previously sedentary postmenopausal women, resistance training has been shown to reduce systemic inflammation and leptin concentrations, potentially restoring leptin sensitivity and improving muscle bioenergetics. 83 Although women with NWO have a greater risk of developing pathophysiological changes in skeletal muscle that can lead to serious diseases, lifestyle modifications, such as diet and exercise can help counteract these adverse effects.
5. Adipose tissue impact on bone health
Bone tissue remodeling is tightly regulated through the processes of resorption (via osteoclasts), formation, and mineralization (via osteoblasts).84,85 These processes occur at various rates across the lifespan, determining net bone turnover, accretion, and mass.84–86 Net bone formation is favored during childhood and adolescence until peak bone mass is achieved, after which bone mass typically stabilizes (i.e., bone formation ≈ resorption) until age-related declines begin 86–88. Peak bone mass is a major predictor of osteoporosis risk later in life and is largely determined by genetics. 86 However, up to 40% can be influenced by environmental and lifestyle factors. 88 Women generally achieve a lower peak bone mass than men, and the menopausal transition accelerates bone loss through reduced mineralization and microarchitectural deterioration, placing women at greater risk of osteoporosis and fractures.86,88,89
5.1. Paradoxical relationship between adipose tissue and bone health
Adipocytes and osteoblasts are derived from the same mesenchymal cells. Consuming a suboptimal habitual diet characterized by excess energy intake with higher sugar and/or higher fat consumption can preferentially differentiate mesenchymal cells into adipocytes instead of bone forming osteoblasts.85–87 Furthermore, adipose tissue releases pro-inflammatory cytokines including tumor necrosis factor alpha (TNFα) and interleukin-6 (IL-6) which can increase bone resorption and/or weaken the bone microstructure, leading to increased fracture risk. 85 Despite this, the relationship between body weight/fat and bone fragility is complex. While low BMI/’underweight’ (≤18.5 kg/m2) is consistently associated with low bone mass90–92 and higher risk of fracture,90,93–96 ‘normal’ BMI (18.5 kg/m2 – 24.9 kg/m2),95,97–99 and in some cases ‘overweight’ (BMI: 25 kg/m2 – 29.9 kg/m2) and ‘obesity’ (BMI ≥30 kg/m2),98,100 have been associated with higher BMD. This paradoxical relationship may be explained by higher SMM which often accompanies clinical obesity, providing increased mechanical strain on the bone by resisting gravity, and by skeletal muscle during movement may promote this observed elevation in BMD.101–105 These factors, in some cases, can offset the negative inflammatory and metabolic effects of increased adiposity on bone.101–105 Importantly, since NWO is marked by lower SMM, quality, and function, 106 these potential protective mechanisms to bone are likely absent. Indeed, studies in women with NWO report inverse associations between body fat percentage and BMD, despite a ‘normal’ weight that is typically considered advantageous for bone health.107–110
5.2. Adipose tissue: influence on bone health across the lifespan
Evidence in adolescent girls demonstrates that higher adiposity is negatively associated with bone health outcomes. Indeed, adolescent girls presenting as overweight and obese (OW/OB) exhibit lower bone quality, strength, and mass,111–116 and blunted bone formation/turnover via lower osteocalcin compared to girls of normal-weight. This is concerning given that adolescence is a time in the lifespan marked by bone growth, and bone formation/turnover should be increased. 117 Adolescent girls with OW/OB have also been shown to have higher cortical porosity and lower thickness at certain skeletal sites, indicating impaired bone microstructure, despite higher BMD compared to girls of normal-weight and to those with anorexia nervosa (a population typically with increased fracture risk). 118 While research is relatively limited in youth with NWO, one study found lower skeletal robustness/development in children with NWO, which likely relates to a combination of excess body fat, VAT, and inadequate SMM. 119
Research evaluating the impact of excess adiposity on bone health in premenopausal adult women has previously indicated that greater VAT corresponds to a greater pro-inflammatory insult on bone.120–122 This type of fat distribution is also deleterious to BMD,100,120,123 and bone strength,123,124 and is associated with reduced rates of bone formation, 123 and increased risk of fracture.96,100,124,125 Women with higher VAT have been shown to have greater fat infiltration within bone marrow, which can increase bone fragility.121,126 In addition, 127 those with NWO have been found to exhibit elevated levels of parathyroid hormone and sclerostin, two systemic/circulating biomarkers indicative of increased bone resorption. 109 Young to middle adulthood is a period when bone mass should be maintained.86–88 In the absence of compensatory increases in lean mass (as seen in traditional obesity), a pro-inflammatory profile may be particularly detrimental 107 and could potentially contribute to an earlier decline in bone mass, although further research is needed in the context of NWO.
Menopause is often accompanied by body composition shifts characterized by decreases in SMM and increases in FM (especially VAT) that can have additional negative impacts on bone.128–130 Postmenopausal women with higher relative body fat and/or waist circumference (indicating a higher VAT percentage) tend to have lower BMD, increased risk of all-site and vertebral fractures, as well as hip fracture.96,125,131–133 In particular, women with NWO aged 50–69 years were at greater risk of having a lower BMD compared to women with normal-weight and lower body fat percentages. 110 In summary, higher adiposity (especially in the abdominal region/VAT), as seen in those with NWO, can impair the bone microstructure, increase bone fragility through inflammatory processes (i.e., TNFα and IL-6), and ultimately, increase the risk of fracture. 126 Importantly, most research on the relationship between adiposity and bone health has been conducted in populations with obesity in general, versus those with NWO. Future studies in women’s health should examine how fat distribution, rather than total body weight, influences bone microstructure and health across the lifespan.
6. Clinical implications and recommendations
Given the hidden risks associated with NWO, clinical screening and public health policies must evolve beyond BMI. Practitioners should consider incorporating accessible body composition assessments, such as BIA or DXA, into routine physicals, particularly for women throughout perimenopause. The assessment of body composition, particularly SMM and adiposity, is increasingly recognized as essential for understanding metabolic health, and represents a field of growing clinical and research interest. Recent efforts have emphasized the importance of harmonizing terminology and measurement approaches in body composition research and practice, with additional methodological standards currently under development to improve consistency and clinical translation.
From an intervention standpoint, regular resistance training is paramount. Resistance exercise directly targets the physiological deficits of NWO by increasing SMM, enhancing muscle quality, reducing myosteatosis, and providing mechanical loading to preserve BMD. In parallel, nutrition interventions aimed at optimizing protein intake and supporting muscle maintenance or accretion may further complement exercise-based strategies and improve body composition and metabolic health. Additionally, routine endocrine screening (e.g., lipid panels, fasting glucose, and sex hormone evaluations) can help identify subclinical metabolic dysfunction early. Notably, the Lancet Commission on diabetes and endocrinology recently updated their definition of clinical obesity to focus on physiological health metrics rather than anthropometry alone. 134 The adoption of these updated, health-centric diagnostic frameworks may eventually eradicate misclassifications like NWO, ensuring women receive appropriate preventative care regardless of their outward appearance. However, body composition assessment was not explicitly incorporated into these frameworks, which may limit their ability to fully address the challenge of identifying NWO.
7. Limitations
While this review comprehensively addresses the implications of NWO in women, several limitations in the existing literature must be acknowledged. First, the lack of a standardized definition for NWO (e.g., varying body fat cutoffs and assessment tools) makes direct comparisons between studies difficult. Second, much of the data evaluating the relationship between NWO, SMM, and bone health relies on cross-sectional designs, which limits the ability to establish true causality. Third, there is a distinct lack of longitudinal research tracking the progression of metabolic and musculoskeletal health in individuals with NWO specifically as they transition through the stages of menopause. Future research should prioritize prospective cohort studies to better elucidate these trajectories.
8. Conclusion
NWO is an underdiagnosed yet clinically important phenotype, particularly in women. Despite normal BMI status, NWO women are at elevated risk for cardiometabolic disease, hormonal dysregulation, impaired muscle mass, function, composition, and quality, and reduced bone strength. These risks are compounded by physiological changes that occur across the menopause transition. Most notably, the shift in sex hormones, redistribution of fat more viscerally, and loss of SMM amplify the consequences of NWO. The traditional reliance on BMI leaves many women with NWO undiagnosed until severe health consequences develop. Identifying and addressing NWO through body composition-focused screening is essential for improving early intervention and long-term health outcomes for women across the lifespan.
Footnotes
Acknowledgements
We wish to acknowledge the graduate and undergraduate students working with the researchers at the various institutions included in this author list that supported literature searches in preparation of this review.
Author contributions
Conceptualization: A.F., A.E.S.R., C.P.P. Writing – Original Draft: A.F., K.R.H., A.R.J., S.G., A.E.S.R., M.J.O., M.S., D.D.C., C.S., D.J.S., D.G.C. Writing – Review and Editing: A.F., K.R.H, S.G., A.E.S.R., M.J.O., A.J.C., P.A.B., J.E.M., R.N.D., D.D.C., C.S., D.J.S., D.G.C. Visualization: A.F., K.R.H., A.J.C., P.A.B., J.E.M., R.N.D., J.R.P. Supervision: A.F., A.R.J., A.E.S.R., D.D.C., C.P.P. Funding Acquisition: A.F.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: A.F. and A.E.S.R were supported by an Institutional Development Award (IDeA) from the National Institute of General Medical Sciences of the National Institutes of Health under Grant #P20GM152304 during preparation of this manuscript. The contents are solely the responsibility of the authors and do not necessarily reflect the official views of NIH.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Original data from the studies referenced in this review can be found in the original publications.
Use of artificial intelligence
Artificial intelligence (ChatGPT 5.3) was used to correct grammatical errors and improve sentence coherence. The authors reviewed and verified all content.