
Abstract
Background
Female sex workers (FSW) in South Africa are disproportionately impacted by HIV, yet daily oral pre-exposure prophylaxis (PrEP) initiation and continuation rates among FSW remain low. Long-acting injectable PrEP (LAI-PrEP) may alleviate many oral PrEP adherence challenges; however, LAI-PrEP remains largely unavailable in South Africa.
Objectives
Explore the multilevel contextual determinants likely to influence LAI-PrEP’s implementation among FSW to inform rollout strategies.
Design
Cross-sectional, qualitative study with in-depth interviews and focus group discussions.
Methods
From May to June 2024, 42 adult FSW not living with HIV and accessing services from two decentralized FSW delivery sites in eThekwini and Ehlanzeni participated in interviews (12 per study site; n=24 FSW total) and focus groups (1 per study site; n=18 FSW total). Four providers were also interviewed (2 per study site). Semi-structured guides, based on the Consolidated Framework for Implementation Research (CFIR), elicited client and provider perceptions of contextual factors hypothesized to influence future LAI-PrEP implementation, mapped to CFIR constructs through team-based, deductive thematic analysis.
Results
Many FSW conveyed strong acceptance and preferences for LAI-PrEP due to perceived advantages over oral PrEP including greater dosing privacy in clinical spaces, fewer dispensing intervals, and reduced stress from daily pill-taking. Providers perceived LAI-PrEP as a priority to augment existing HIV prevention services; however, financial investments, additional staff, and LAI-PrEP counseling training would be needed to enhance programmatic capabilities. Prioritization of non-discriminatory provider attitudes will be crucial to combat persistent racialized and economic inequities that exacerbate stigma against FSW in public healthcare facilities. Finally, decentralized delivery, utilizing community champions, and integrating LAI-PrEP with other health services emerged as promising strategies to ensure an equitable rollout of LAI-PrEP, assuming adequate global or national investment.
Conclusion
Findings suggest that LAI-PrEP is perceived by both potential recipients and deliverers to effectively address several barriers to oral PrEP continuation, making it a promising advancement in the landscape of HIV prevention. Implementation strategies that integrate identified stakeholder priorities and preferences, anticipated barriers, and existing programmatic strengths, will likely optimize LAI-PrEP rollout among a historically marginalized population in South Africa.
Introduction
South Africa continues to have one of the highest burdens of HIV globally, with a national HIV prevalence estimate of 12.7% in 2022. 1 Female sex workers (FSW) are disproportionately impacted by HIV, with a recent prevalence estimate of 53% across Southern and Eastern Africa, 2 and additional studies in South Africa suggesting comparably high burdens, with HIV prevalence ranging from 40% to 72%.3–5 Within the context of sex work, economic incentives and power imbalances can promote inconsistent condom use, 4 thereby increasing the incidence of HIV for FSW. Young FSW (18-24 years old) in particular experience disproportionately high incidence of HIV compared to older FSW.6,7 This age group often faces complex social pressures and discrimination from family members and sexual partners, diminished capacity to effectively negotiate condom use, and lower perceived HIV acquisition risks.3,6–9
Oral HIV pre-exposure prophylaxis (PrEP) has been shown to be extremely effective in preventing HIV acquisition. 10 Despite its efficacy, oral PrEP initiation and continuation rates among FSW remain low.4,11 A prior study among FSW in South Africa found oral PrEP persistence was approximately 50% just one month after initiation and less than 10% after a year. 4 The proportion of discontinuations relative to those who started on oral PrEP was highest among young FSW. 4 Common challenges associated with adhering to oral PrEP for FSW include the inconvenience of daily pill-taking, feeling stigmatized due to PrEP marketing historically targeting key populations, misconceptions around HIV transmission, and low social support.4,6,12 Furthermore, structural barriers among FSW have contributed to suboptimal oral PrEP uptake, adherence, and continuation, namely through food and housing insecurity, medication storage challenges, and difficulties accessing oral PrEP from healthcare facilities and other dispensing points.12–15
Long-acting injectable PrEP (LAI-PrEP) may help alleviate the continuation challenges associated with daily oral PrEP. 16 One form of LAI-PrEP, an integrase strand transfer inhibitor known as Cabotegravir long-acting (CAB-LA), is administered intramuscularly every 2 months. 17 CAB-LA was registered in South Africa by the South African Health Products Regulatory Authority (SAHPRA) in December 2022. 18 CAB-LA has been found to reduce the risk of HIV acquisition by 93-94% compared to a counterfactual placebo. 19 Additionally, a phase 3 clinical trial evaluating the efficacy of cabotegravir for HIV prevention (HPTN 084), showed an 88% reduction in HIV risk among women taking CAB-LA compared to women taking oral PrEP in seven Southern and Eastern African countries. 17 A subsequent, open-label phase (HPTN 084-01) found high acceptability and feasibility of CAB-LA implementation among adolescents in South Africa, Uganda, and Zimbabwe, as evidenced by no discontinuations due to intolerability or missed injection appointments. 20
A second form of LAI-PrEP, Lenacapavir, has been registered with SAHPRA as of October 2025. 21 Lenacapavir is an HIV-1 capsid inhibitor administered subcutaneously that has demonstrated high efficacy in preventing HIV infection when delivered biannually, with one phase 3 clinical trial reporting no incident HIV infections among the adolescent girls and young women who received it. 22 However, both CAB-LA and Lenacapavir have remained largely unavailable in South Africa except through clinical studies. FSW will likely be prioritized in the future rollout of LAI-PrEP, as the introduction of new PrEP products for key populations is a named objective in South Africa’s 2023-2028 National Strategic Plan for HIV, TB, and STIs. 23 Yet, existing scholarship to help guide this rollout, including data assessing acceptability, feasibility, and contextual determinants of LAI-PrEP implementation have been mostly described in non-FSW populations,24–28 higher-income settings,24,26–28 and/or other East and Southern African countries.23,25,29 The studies among East and Southern African women (including both FSW and non-FSW) found strong preferences for LAI-PrEP over oral PrEP due to daily pill-taking challenges, desires for community-led education to support decision-making, and several anticipated barriers to LAI-PrEP access including stigma from partners and/or healthcare workers and cost.23,25,29 Before LAI-PrEP is rolled out nationally among FSW in South Africa, there is a need to identify potential real-world constraints and strategies that will enable the integration of LAI-PrEP into existing health systems and service delivery models. 30 Using the Consolidated Framework for Implementation Research (CFIR) version 2.0, 31 the present cross-sectional, qualitative study aims to identify the contextual factors anticipated to influence LAI-PrEP implementation within an existing FSW-focused PrEP program in South Africa.
Methods
Study setting
This study was conducted at two TB HIV Care program sites in eThekwini and Ehlanzeni. TB HIV Care is a South African, non-profit organization and the largest national HIV prevention and treatment service provider for FSW. The site in eThekwini, located in the KwaZulu-Natal Province, operates in a predominantly urban setting (including the City of Durban and the surrounding metropolitan area) with three mobile clinics. The Ehlanzeni site, located in the Mpumalanga Province, serves both the peri-urban setting of Mbombela and the surrounding rural area with two mobile clinics.
Reflexivity statement
The research team consisted of 13 members from both the Johns Hopkins School of Public Health (JHSPH) in the United States and TB HIV Care in South Africa. The JHSPH members were led by an American PhD-level Principal Investigator with extensive research experience in HIV prevention in South Africa (KR), and the TB HIV Care members were led by a South African MD/PhD-level Principal Investigator and Chief Executive Officer of TB HIV Care with decades of experience in HIV prevention and treatment service optimization in South Africa (HH). The data collection team consisted of two female South African Research Assistants at TB HIV Care who are fluent in English, Zulu, and siSwati and trained in qualitative research methods and the CFIR framework (ND, NM). ND and NM were intentionally hired for this study due to their prior experience collecting quantitative and qualitative data at the study sites, as well as their shared nationality, language, and gender identity with the study’s participants. However, their affiliation with TB HIV Care as professional researchers may have impacted what participants shared during interviews and focus groups. Data analysis was led by a female, American Masters-level Research Assistant with prior outreach experience with FSW in the United States (EM), which may have influenced her analytical perspective and interpretations. EM spent five months at study sites between July and December 2024 to contextually ground herself in the research. Beyond this, all data collection and analytic materials were iteratively refined by ND and NM, rapid analysis templates were completed by ND and NM following each interview and focus group, and transcripts were divided amongst coders. The lived experiences of the other two coders (VC, AA), Canadian Masters-level Research Coordinators at JHSPH, may have influenced their coding and interpretation of transcripts, although both have prior experience conducting HIV prevention research in South Africa.
Data collection
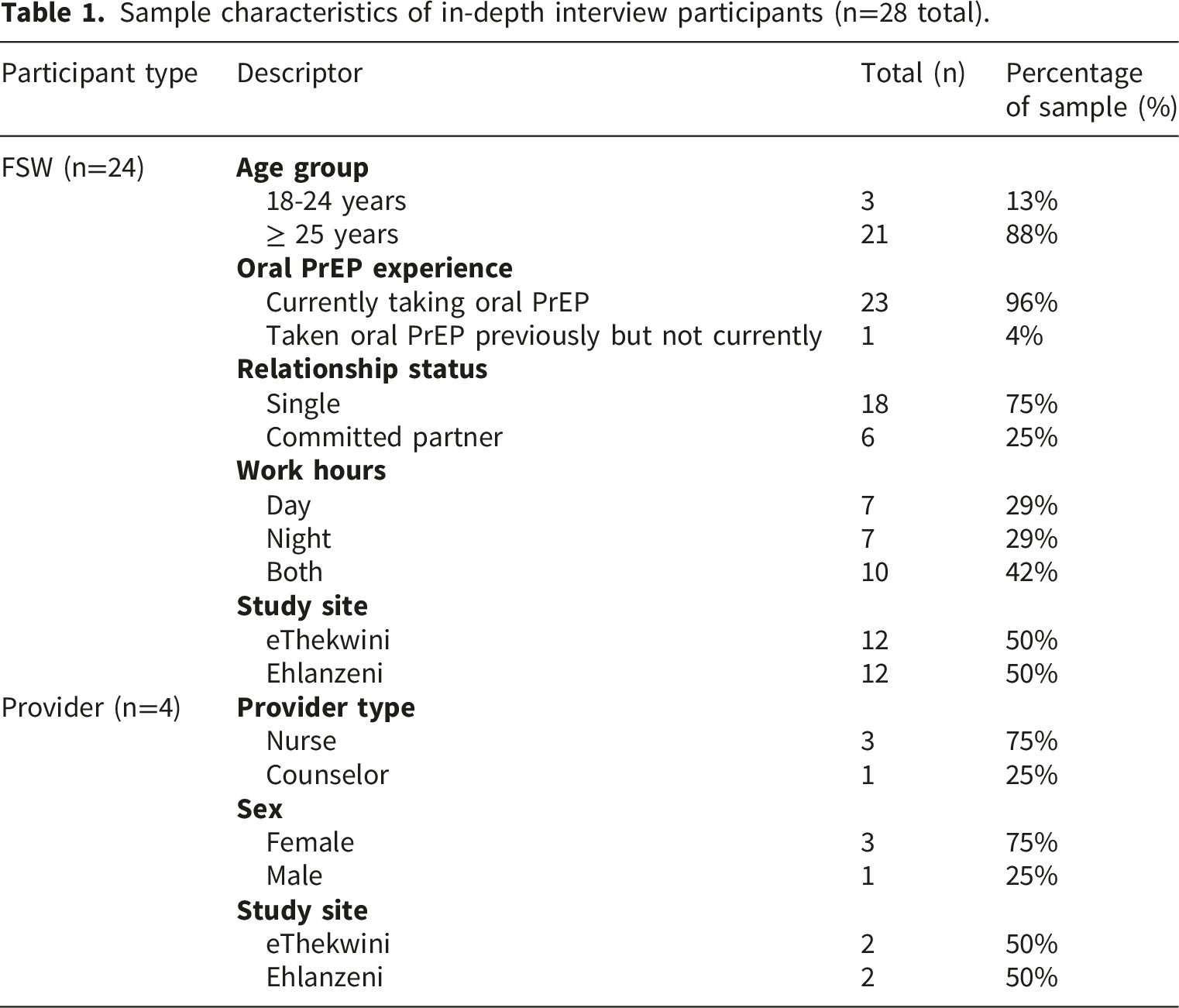
Between May and June 2024, semi-structured, cross-sectional qualitative data were collected at the two TB HIV Care FSW program sites. We utilized in-depth interviews (IDIs) and focus group discussions (FGDs) to elicit service-user and healthcare provider perceptions of factors that may influence LAI-PrEP implementation. In total, 42 FSW participated in interviews (12 per study site; n=24 FSW total) and focus groups (1 per study site; n=18 FSW total). Four providers were also interviewed (2 per study site). Each FSW participated in either an interview or focus group in order to capture diverse opinions and lived experiences. Eligibility criteria for FSW, ascertained via self-report, included being at least 18 years of age, identifying as a cisgender woman, not living with HIV, and currently accessing HIV prevention services from TB HIV Care. Two female South African Research Assistants (ND, NM), in collaboration with the TB HIV Care peer outreach team, used convenience sampling to recruit FSW during routine preventative services at the program sites and during mobile outreach. They introduced the study and its objectives and assessed willingness to participate prior to obtaining written informed consent. Recruitment efforts aimed to voluntarily enroll both younger (18-24 years) and older (25+ years) FSW, as well as those with varying levels of prior oral PrEP experience (never taken oral PrEP, taken oral PrEP previously but not currently, or currently on oral PrEP), seeking to include diversity in preferences and lived experiences. Interviewed providers, including one PrEP counselor and three nurses, were identified and voluntarily enrolled through the TB HIV Care FSW program at both study sites. Task-shifting policies in South Africa allow NIMART (Nurse-Initiated and Managed Antiretroviral Therapy)-authorized professional nurses to prescribe and dispense PrEP. 32
Interviews and focus groups were conducted either in the drop-in centers or in private rooms during outreach. No individuals other than the interviewers and participants were present during the interviews and focus groups. Interviews were conducted individually by one of the two South African Research Assistants (ND, NM) in English, Zulu, or siSwati, lasted approximately 60 minutes, and were audio-recorded. Focus groups were also conducted by the two South African Research Assistants (ND, NM), with one facilitating the discussion while the other recorded notes. Focus groups were conducted in Zulu or siSwati, lasted approximately 90 minutes, and were audio-recorded. Audio-recordings were professionally transcribed verbatim and translated into English for analysis. Transcripts were not returned to participants.
Semi-structured interview and focus group guides were derived from the CFIR version 2.0 domains and constructs (VC, KR) (Figure 1). Guides were not pilot-tested prior to data collection, but were reviewed and revised by the interviewers (ND, NM) and TB HIV Care peer outreach team to enhance the clarity and appropriateness of questions. CFIR is a determinants framework for assessing barriers and facilitators to the implementation of evidence-based interventions/practices across five domains: innovation characteristics, outer setting, inner setting, individual roles and characteristics, and the implementation process.
31
The CFIR was updated in 2022 to include additional constructs related to innovation recipients and health equity, such as features from the Capability-Opportunity-Motivation-Behavior model.
33
For both the interviews and focus groups with FSW, guides opened with a description of LAI-PrEP to ground the conversation and ensure all participants had a common understanding of this HIV prevention method. Because LAI-PrEP was not widely available in South Africa at the time of data collection, questions regarding the perceived capability or opportunity of FSW and providers to receive or deliver LAI-PrEP were guided by prompts focused on LAI-PrEP implementation through existing TB HIV Care service delivery channels. CFIR domains and constructs assessed during in-depth interviews and focus group discussions with FSW and providers.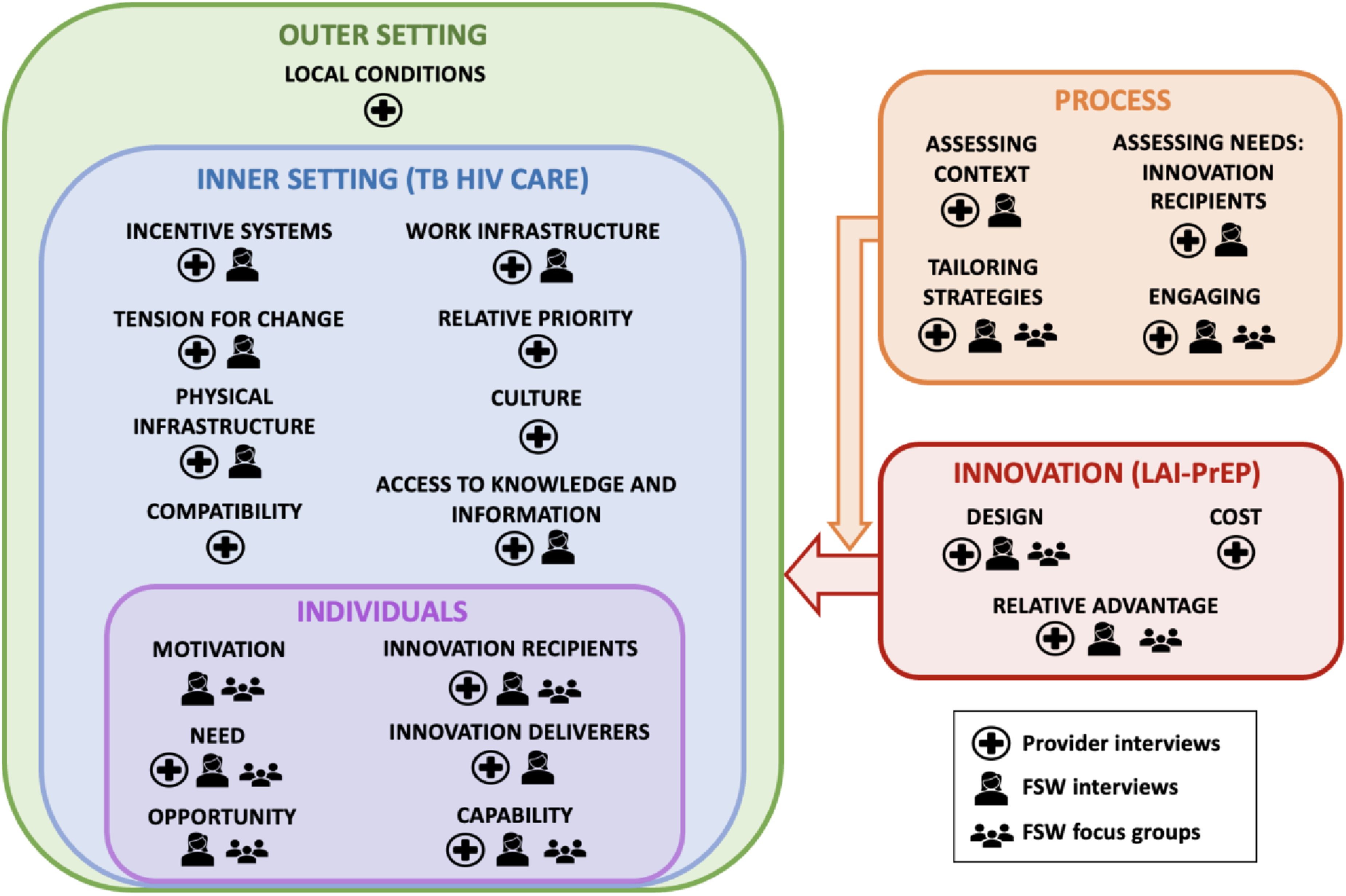
Interviews with FSW currently accessing HIV prevention services through TB HIV Care allowed for a more detailed exploration of individual oral PrEP experiences and LAI-PrEP service delivery preferences. All CFIR domains except for the Outer Setting were addressed, with a particular focus on the following topics: prior knowledge and perceptions of LAI-PrEP (Individuals: Need, Motivation, and Innovation Recipients), (dis)advantages of LAI-PrEP compared to oral PrEP (Innovation: Design and Relative Advantage), potential strategies for tailoring LAI-PrEP delivery to FSW (Process: Tailoring Strategies), preferences for delivery location and injection frequency (Process: Engaging and Assessing Context), and self-efficacy and anticipated barriers to LAI-PrEP adherence (Individuals: Capability and Opportunity) (Figure 1). Interviews with providers addressed all five CFIR domains, focusing on assessing their prior knowledge and perceptions of LAI-PrEP (Individuals: Innovation Deliverers; Inner Setting: Access to Knowledge and Information), opinions about integrating LAI-PrEP into their routine HIV prevention services for FSW (Inner Setting: Compatibility, Relative Priority, and Work Infrastructure), and anticipated challenges delivering LAI-PrEP to FSW in their respective practice settings (Inner Setting: Physical Infrastructure; Innovation: Cost) (Figure 1). Focus groups with FSW were conducted to assess prior knowledge and opinions of LAI-PrEP (Innovation: Design and Relative Advantage), motivations for and barriers to PrEP use (Individuals: Capability, Opportunity, Motivation, Need, and Innovation Recipients), and preferences for LAI-PrEP delivery features (Process: Tailoring Strategies and Engaging) (Figure 1). Results from focus groups were used to corroborate findings from interviews and inform attributes for a discrete choice experiment planned for a later phase of the study.
Thematic analysis
We used deductive, framework-guided thematic analysis to identify salient implementation determinants of LAI-PrEP across interviews (n=28) and focus groups (n=2). Three rapid analysis templates were created for interviews with FSW, focus groups with FSW, and interviews with providers (VC). These templates included key questions from the interview and focus group guides with designated space beneath each question to summarize major takeaways and were completed by the facilitator (ND, NM) within 48 hours of each interview and focus group. The templates were used to assess data saturation, rapidly identify themes, and inform the development of the qualitative codebook.
The initial codebook was structured around all five CFIR version 2.0 domains (innovation characteristics, implementation process, outer setting, inner setting, and individuals) and a sub-set of the associated constructs, including those that were present in the templates and in the close reading of two interview transcripts that were randomly selected (EM). We used standard code definitions from CFIR’s available qualitative tools that were adapted and specified for the present study as a team during group coding meetings. 34 This process involved the interviewers (ND, NM) and JHSPH research team (EM, CC, VC, AA, JGR, KR), allowing for clarification and standardization of code definitions, as well as the creation of inclusion and exclusion criteria. To ensure consistency in code application, we applied the initial codebook to text segments from two transcripts as a group, discussing and resolving conflicts through dialogue and consensus. After refining the codebook, we imported transcripts into Dedoose software to facilitate data organization and coding. 35 Each transcript was coded by one of three members of the JHSPH research team (EM, VC, AA), working independently. Weekly meetings with the larger JHSPH research team were held to allow for discussion of unclear transcript segments and appropriate code applications. Memos were used to document emerging themes from each transcript. Data saturation, which can generally be achieved in a heterogeneous sample with 12 to 20 interviews,36–38 was reached as no new codes or themes were identified by the end of the coding process.
Key themes were identified through close reading of coded excerpts in Dedoose, assessing code frequencies using Dedoose’s built-in code application chart, and clustering emerging themes by code and participant type. Thematic salience was determined based on both the frequency of themes and the depth of discussion by participants. We then deductively organized themes and illustrative quotes by participant types into a CFIR framework data matrix, comprising all five domains and the 22 identified constructs. Participants did not directly provide feedback on the findings; however, results were presented to TB HIV Care program staff and community advisory groups to obtain their input. The reporting of this study conforms to the Consolidated Criteria for Reporting Qualitative Research (COREQ) statement and checklist by Tong et al. 39
Ethical considerations
The present study and its materials were approved by the Johns Hopkins Bloomberg School of Public Health and the University of Pretoria Institutional Review Boards. All eligible participants participated in a private informed consent process with the qualitative interviewer using a written consent script (available in English, Zulu, or siSwati). This process covered information on the study and potential risks and benefits of participating. All individuals provided written consent prior to participating. FSW participants received 200 South African Rand (approximately 11 USD) as reimbursement for their time, which aligned with TB HIV Care procedures.
Results
Participants
Sample characteristics of in-depth interview participants (n=28 total).
Contextual influences: CFIR domains and constructs
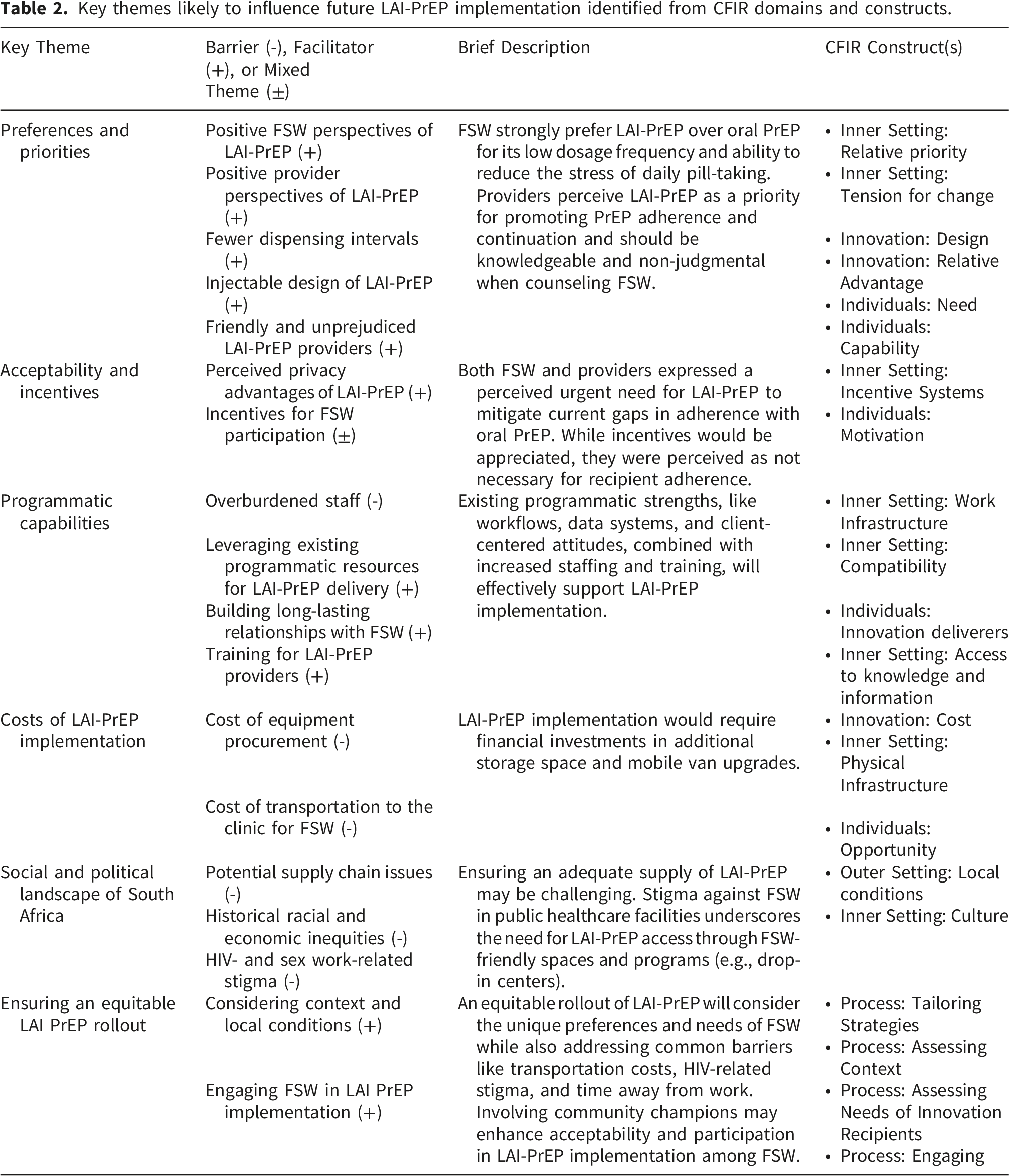
Key themes likely to influence future LAI-PrEP implementation identified from CFIR domains and constructs.
Preferences and priorities
Relatively few FSW had awareness of LAI-PrEP prior to the interviews. Nevertheless, when provided a description of LAI-PrEP by the interviewer, most expressed enthusiasm about LAI-PrEP, asserting greater alignment with their needs relative to daily oral PrEP. Specifically, participants reacted positively to the bimonthly frequency of LAI-PrEP injections, noting that it would reduce the stress and labor associated with daily pill-taking: “There are others who have stopped taking PrEP completely because they don’t understand why they need to take a pill every day to prevent them from taking a pill every day. We’ve been saying that we would prefer if there was an injection instead.” – FSW #20, 29-year-old working during the night in eThekwini
Many FSW also preferred an injectable formulation over pills, specifying physical challenges with swallowing pills or positive prior experiences with contraceptive injections: “Sometimes I take two pills at one go because I forget if I took the pill the day before or not. We are also taking the contraceptive injection, so I doubt we’ll forget to take the injection.” – FSW #4, 27-year-old working during the day in Ehlanzeni
Both FSW and providers strongly vocalized a perceived urgency for LAI-PrEP to improve HIV prevention efforts. LAI-PrEP was considered a less risky prevention method than oral PrEP since FSW often forget to take oral PrEP pills, particularly when drinking alcohol or traveling: “I think [LAI-PrEP]’s safer as well. If you have an accident, it’ll already be in you so you know that you will be protected.” – FSW #19, 46-year-old working during the night in eThekwini
Providers were excited to see a potential solution to oral PrEP adherence challenges and were receptive to administering LAI-PrEP injections: “We are ready. The injection will increase the number of people who take PrEP. Sex workers have also been asking if there is an injectable form for a long time now, so they will be happy when it’s available. Retention will also increase if the injection becomes available.” – Provider #4, Counselor
Many FSW and providers voiced a preference for prioritizing the implementation of LAI-PrEP over oral PrEP because of its longer-lasting protection from HIV and potential to address oral PrEP adherence challenges reported above. One provider highlighted the urgency for LAI-PrEP by sharing their perception of consistently high rates of new HIV infections: “There is no time to delay anything that prevents HIV. We have a very big challenge here in South Africa when it comes to HIV. The number of people being infected increases every day so prevention methods should come urgently.” – Provider #1, Nurse
However, many FSW also reported feeling comfortable selecting their own HIV prevention method and wanting both oral and injectable PrEP options available: “Different methods have different side effects. People might want to test different methods before they find what works for them. It’s a good thing to have options.” – FSW #4, 27-year-old working during the day in Ehlanzeni
Providers also emphasized the importance of maintaining their current oral PrEP program without interruptions to accommodate different FSW preferences.
Furthermore, when asked to describe the ideal characteristics of an LAI-PrEP provider, FSW preferred to receive LAI-PrEP from someone who is educated, kind, and non-judgmental: “They can be male or female as long as they are friendly. I’d like to feel comfortable around them. If they are rude I’ll be scared to talk to them about my issues.” – FSW #7, 32-year-old working during the night in Ehlanzeni
These preferences were underscored by requests from FSW in both eThekwini and Ehlanzeni to prioritize FSW sensitization training for providers: “I think instead of visiting us monthly, you need to train your team monthly. People mustn’t look down on us because we are doing this.” – FSW #19, 46-year-old working during the night in eThekwini
While most FSW expressed confidence in their perceived ability to attend regular injection appointments, some conveyed hesitancy towards potential side effects and required more information prior to committing. FSW requested additional educational materials and/or workshops to learn more about the injections:
“Interviewer: What factors or conditions should we consider before we make the injection available to you? What resources should we have to help women decide on the injection?
Interviewee: Pamphlets so that they can read up on it and see how it will help them.
Interviewer: Is there anything else we need to do to convince women to take the PrEP injectable?
Interviewee: You just need to talk to them. You can have group discussions.” – FSW #13, 46-year-old working during the day and night in eThekwini
Many FSW expressed intentions to adhere to LAI-PrEP long-term, unless severe side effects occurred (e.g., dizziness, heavy menstruation). However, others communicated a preference to wait and see how others respond/react to LAI-PrEP before receiving it themselves: “I’ll first see how [LAI-PrEP] affects others before I take it. I’ll ask the people who are taking it how their experience is and then I’ll take it from there.” – FSW #14, 38-year-old working during the day in eThekwini
Overall, most FSW preferred LAI-PrEP over oral PrEP. Those inclined to remain on oral PrEP described sentiments of mistrust towards a new drug or expressed preferences for autonomy in PrEP discontinuation if they were to experience side effects.
Acceptability and incentives
Generally, FSW endorsed LAI-PrEP as highly acceptable and better suited to their lifestyles than oral PrEP. Privacy emerged as a critical facilitator of acceptability. Many FSW valued LAI-PrEP as a more private HIV prevention method, as it would be a provider-administered formulation delivered in either clinical spaces or enclosed mobile vans rather than a user-controlled method used at home. Several FSW shared experiences of facing judgment and stigma from public health care facilities and/or partners and clients who saw them carrying oral PrEP bottles: “A woman who takes the injection is someone who is scared to tell their boyfriend that they are taking PrEP, so they hide the pills. No one will be able to tell that you just got the injection.” – FSW #11, 24-year-old working during the night in Ehlanzeni
The role of incentives differed greatly between FSW and providers. When asked if receiving incentives or rewards would motivate them to continue with LAI-PrEP, most FSW stated that while these would be appreciated, they would not be necessary for them to maintain adherence. Many FSW expressed that remaining HIV-negative would be a sufficient incentive to continue with LAI-PrEP. In fact, FSW were universally motivated to initiate LAI-PrEP once available in South Africa, primarily driven by a high perceived HIV acquisition risk: “This is a forever thing... I will only stop if I find out that I am HIV-positive because I’ll have to start taking ARVs. It’s till death do us part with PrEP and me.” –FSW #18, 43-year-old working during the day and night in eThekwini
Conversely, when asked about the role of incentives, all providers emphasized their importance in encouraging adherence: “I’ve noticed that [FSW] love gifts. Remember that we are talking about people who don’t have much... I think you should give them a token of appreciation just to say thank you for taking care of yourself.” – Provider #2, Nurse
Programmatic capabilities
The organization and general staffing levels of TB HIV Care would facilitate the integration of LAI-PrEP into clinical workflows. Providers in both eThekwini and Ehlanzeni reported that the current workflow for oral PrEP dispensing, including appointment reminders, HIV testing, and counseling, is efficient and has transportability to LAI-PrEP delivery. They also highlighted their use of a client database to support their track-and-trace efforts (monitoring appointment attendance and re-engaging clients in HIV services): “Not much is going to change because the injectable is also PrEP. There could also be a specific team that specializes in the PrEP injection... We have a team that can do that already who do tracking and tracing. They could take over the work of the PrEP injectable.”– Provider #4, Counselor
However, more staffing may be required to implement LAI-PrEP as providers already juggle many responsibilities: “No, I don’t think we’ll have time. Even the time we have now is not enough for us on a daily basis. There'll be more work added to the work that we have now. Maybe they should hire one more nurse who just deals with the injection.” – Provider #1, Nurse
Aside from adequate staffing and a capacitated, highly motivated workforce, providers insisted it would be feasible to implement LAI-PrEP at TB HIV Care. Their experienced staff, available resources, and long-established positive relationships with FSW would likely operate as preconditions to LAI-PrEP implementation success: “I think we have everything it takes to implement this injection. We've got nurses, they know how to use the injection, they are trained. They just need to be educated about the PrEP injection. I know our clients and they are not resistant to change. They love new things and they want to explore new things.” – Provider #1, Nurse
Providers reported that their unique approach to building relationships with FSW is a strength of their clinic that helps with promoting health-seeking behaviors: “If it was not for [TB HIV Care], I’m sure most of them would have been dead by now. It’s not easy for them to go to the [public] clinic. They don’t have time and there is a stigma around them. They are being discriminated against and bullied. [TB HIV Care] reaches out to them and it makes them feel confident.” – Provider #2, Nurse
At both study sites, we found a high perceived compatibility between LAI-PrEP implementation and existing TB HIV Care oral PrEP services and workflows. While one provider in Ehlanzeni mentioned concerns that shifting attention to LAI-PrEP may disrupt oral PrEP services, providers in eThekwini stated that they expect no interruptions in service delivery. A provider in Ehlanzeni also considered the perceived need to spend more time with clients during PrEP initiation visits to review and discuss the available PrEP options: “[LAI-PrEP] will disturb the staff because they will need to have knowledge on the injection. The peer educators will have to also know about the injection and will spend more time educating clients on PrEP options.” – Provider #1, Nurse
Lastly, access to knowledge and information regarding LAI-PrEP emerged as a critical conduit to successful LAI-PrEP implementation. Like FSW, all providers in the study requested additional information and training on LAI-PrEP and its delivery. Most providers reported previously hearing of LAI-PrEP, but did not yet feel comfortable providing counseling to FSW until they were more familiar with the injection and its side effects. “Training is needed. [Providers] need to understand the injectable PrEP. [Providers] need to know the side effects and everything. Both nurses and counselors need to be given training regarding the injectables.” – Provider #3, Nurse
Costs of LAI-PrEP implementation
The affordability of LAI-PrEP procurement and operating expenses was only explicitly explored in provider interviews. Providers highlighted the perceived necessity for several upgrades to their mobile vans, such as installing cooler boxes or fridges and upgrading to larger vans compatible with LAI-PrEP implementation requirements, but expressed a need for more information regarding LAI-PrEP implementation requirements: “We can’t put a large amount of injections in the cooler box. We usually have to travel back and forth in order to stock up rather than put a large amount in a cooler box. A fridge would be a great addition. I think that I can answer this properly when I know what is needed for the proper storage of the injection.” – Provider #3, Nurse
Additionally, clinics may need to procure injection equipment (e.g., cotton wool, alcohol wipes) for providers to use. Finally, providers advocated for fully subsidized LAI-PrEP implementation with no out-of-pocket costs to FSW, since they receive oral PrEP for free through the TB HIV Care program.
Providers emphasized several concerns about the clinic’s physical infrastructure, defined as the layout and configuration of the space and material features. To begin with, clinics would require additional storage space to accommodate the injections. Providers in both eThekwini and Ehlanzeni also discussed potentially upgrading to larger vans to accommodate the addition of LAI-PrEP to the decentralized delivery programs. In regions like eThekwini and Ehlanzeni, warm temperatures in the spring and summer months pose a challenge for CAB-LA implementation, specifically. While providers are currently able to store contraception injections in mobile vans using freezer packs, this system may need to be upgraded to accommodate longer delivery hours and a larger supply of injections.
Social and political landscape of South Africa
When asked about the available resources, policies, and funding environment in South Africa, two key implementation considerations were mentioned: first, maintaining stock of LAI-PrEP, and second, FSW experiences of discrimination at public healthcare facilities. Several providers brought up concerns about receiving an adequate supply of LAI-PrEP from the national government to meet demand, especially given current challenges with maintaining supply of oral PrEP: “We are currently out of stock of the tablets. If the government is struggling with delivering pills then they will probably also struggle with the injection.” – Provider #1, Nurse
Many providers also detailed the extent of discrimination and mistreatment FSW experience when trying to access HIV-related services at public healthcare facilities, leading FSW to access oral PrEP at FSW-friendly facilities like TB HIV Care. They emphasized that this discrimination is a result of healthcare workers’ and government officials’ judgment of FSW’s identities and labor instead of recognizing their unique vulnerabilities and needs: “I think that [decision-makers] don’t understand how things work in the organization and how sex workers work. We need to sometimes accompany the sex workers to public facilities because they are discriminated against there. Public healthcare workers don’t understand that we work differently from them.” – Provider #3, Nurse
Ensuring an equitable LAI-PrEP rollout
We found the process of encouraging participation in LAI-PrEP implementation to be perceived as a vital precursor for successful implementation. Generally, FSW expected that LAI-PrEP injection schedules would align with their lifestyles, anticipating no difficulties due to work restrictions or travel. TB HIV Care’s mobile van delivery services effectively address the barrier of transportation costs to the clinic, and one FSW noted that expanded injection hours could better accommodate varying work schedules.
Several FSW emphasized the need for educational outreach campaigns, especially in township areas, to raise awareness about LAI-PrEP. Additionally, many FSW expressed hesitations to be some of the first to receive LAI-PrEP, preferring to wait and hear feedback from trusted sources. Providers also suggested utilizing community champions to share their experiences using LAI-PrEP to build trust and encourage participation: “Retention needs a lot of campaigning and meetings where we discuss the importance of staying on PrEP. Having people already on PrEP share their experiences with it will encourage others to take PrEP.”– Provider #4, Counselor
Assessing the preferences and needs of FSW revealed key implementation considerations from the perspective of providers. One provider highlighted the highly mobile lifestyles of FSW, making further contact or follow-up visits challenging. Some FSW also travel outside of the province or the country for long periods of time. Furthermore, transportation to the clinic can be expensive, especially for those who live in townships further out of the city, resulting in a heavy reliance on the clinic’s mobile van services. However, providers highlighted the diverse needs and preferences of FSW, emphasizing the perceived necessity of offering multiple LAI-PrEP delivery methods to accommodate different circumstances: “Sex workers aren't the same. There are those who are used to working at their homes and would rather get services delivered to them. There are also sex workers who want to come to the clinic themselves because they don’t want to be seen entering a TB HIV Care car.” – Provider #3, Nurse
Finally, the results revealed several potential strategies that may overcome barriers and optimize the delivery and uptake of LAI-PrEP. Almost all FSW emphasized the need for decentralized delivery via mobile vans, which would help solve any transportation barriers, reduce time spent away from clients, and potentially reduce stigma experienced by FSW. In addition to using mobile vans, a few FSW suggested making LAI-PrEP available at private pharmacies to expand its accessibility: “Leaving the township to go to the city needs transport money, and sometimes we don’t have that. There is no TB HIV Care in the township, and the clinics aren’t like TB HIV Care. It would be nice to have easier ways to access PrEP when not in the city.” – P10, eThekwini FGD
Many FSW also voiced concerns about the potential side effects of LAI-PrEP, suggesting that education on the injections may help to overcome this barrier: “I’d like [providers] to give me knowledge of [LAI-PrEP] before I take it so that I know of its side effects and everything.” –FSW #12, 23-year-old working during the day and night in Ehlanzeni
Bundling LAI-PrEP appointments with other health services (e.g., family planning, sexually transmitted infection (STI) testing, condom distribution, primary care) also emerged as a preferred strategy to improve the accessibility of LAI-PrEP. Additional suggestions from FSW included implementing appointment reminder calls, creating WhatsApp support groups for FSW receiving injections, extending the clinics’ hours to accommodate FSW who work during the day, and creating educational pamphlets in several languages (e.g., Sesotho, siSwati, Tsonga). Furthermore, several FSW who frequently travel outside their province highlighted the value of receiving documentation of their prior injection dates to assist in the process of receiving LAI-PrEP at other organizations and/or in different provinces/countries.
Discussion
Four key insights relevant to future LAI-PrEP implementation with FSW emerged from this analysis. First, insights around preferences and priorities indicate a strong perceived need for and motivation to receive LAI-PrEP among FSW, revealing a gap in HIV prevention methods compatible with populations most affected by HIV in South Africa. Second, results around preferences, priorities, and acceptability suggest that LAI-PrEP may have the potential to overcome some of the common barriers to oral PrEP adherence that have emerged in South Africa and other high HIV prevalence settings. Third, pertaining to programmatic capabilities, providers expressed enthusiasm and urgency for LAI-PrEP, while also acknowledging the additional staffing, training, and infrastructure modifications required for successful implementation. Finally, we identified several considerations for ensuring an equitable LAI-PrEP rollout, including potential strategies to engage FSW and tailor LAI-PrEP delivery to their context and needs.
The high perceived need and enthusiasm for LAI-PrEP among FSW in our study suggests the potential for injectables to bridge the current gap between PrEP initiation and retention in real-world settings. Nearly all FSW found LAI-PrEP to be acceptable and stated intentions to receive LAI-PrEP once it is available, aligning with existing literature.22,25,26 Many FSW in our study valued the design of LAI-PrEP as an injection with a longer dosing interval, as it reduces the stress of daily pill-taking and is perceived as more effective than oral PrEP by some. The advantages that LAI-PrEP would provide in terms of providing longer-lasting protection from HIV transmission often outweighed the need for adherence incentives, further demonstrating high motivation to receive LAI-PrEP. Most FSW anticipated few challenges accessing or continuing LAI-PrEP if the injections are incorporated into the mobile van services, though many requested additional information and/or testimonies from other FSW before initiating. However, the continuation of decentralized PrEP delivery, including through mobile-based services, remains uncertain in South Africa given changes to US-administered foreign aid and subsequent disruptions to global HIV programs. Removing regular access to decentralized PrEP for FSW may re-introduce lack of privacy and clinic transportation costs as barriers to PrEP continuation. Consistent with published studies,25,29 FSW expressed the preference for multiple HIV prevention options to be available (i.e., both oral and injectable PrEP), allowing them to select the option that best aligns with their dynamic needs. Thus, offering multiple HIV prevention options may increase the likelihood of transitions between different PrEP formulations when FSW needs and/or circumstances evolve.
FSW highlighted the potential for LAI-PrEP’s design, when implemented within non-governmental, FSW-specific community programs, to alleviate a key barrier to oral PrEP adherence: HIV-related stigma. A private injection within a clinic or mobile van would offer greater dosing privacy/discretion and help eliminate the need to conceal daily PrEP use from friends, family, or sexual partners.25,40 Nevertheless, it will be important to clarify to FSW that although LAI-PrEP would be administered in private spaces, visible injection-site reactions like redness and subcutaneous nodules may occur. 22 Several FSW also noted that LAI-PrEP could help circumvent the harms of oral PrEP-related public misinformation, through which PrEP has been conflated with antiretroviral therapy and sex work. These results add to the growing evidence that HIV-related stigma may catalyze interest in LAI-PrEP.24,26,28
Many FSW in our study recounted experiences of discrimination at public healthcare facilities, leading FSW to seek HIV prevention services outside the public sector, at non-governmental organizations, like TB HIV Care, that offer greater tailoring to FSW preferences and achieve greater reach and acceptability. Similarly, one study found that FSW in Zambia preferred accessing PrEP through dedicated “FSW specialty clinics”, 28 while another identified feeling stigmatized as the second most common reason for discontinuing PrEP among FSW and men who have sex with men in South Africa. 41 However, FSW-specific programs in Southern Africa, particularly those focused on PrEP, are increasingly facing uncertainty due to unprecedented cuts in foreign assistance for HIV. In response, the South African government has recently announced a substantial increase in HIV funding for research and healthcare services in an effort to offset gaps in funding and reinforce national HIV prevention efforts. 42 South Africa has also announced a bid to produce Lenacapavir locally, 43 which may prevent broader implementation of CAB-LA due to its comparatively higher costs and exclusion from the National Essential Medicines List.44,45 In the meantime, beginning as early as this year, Lenacapavir procured by the Global Fund is scheduled to be introduced at government healthcare facilities only.46–48 Therefore, it will be crucial to characterize how the client-centered, inclusive culture of FSW-specific programs can be translated to public facilities to prevent PrEP discontinuations.
The present study also examined implementation determinants from the perspective of South African providers. Across both study sites, providers voiced enthusiasm for LAI-PrEP, viewing it as a better HIV prevention method for FSW than oral PrEP. However, they highlighted the need for more information and training on LAI-PrEP before its implementation. Because oral PrEP is currently the only form of PrEP widely available in South Africa, providers requested additional training on how to effectively counsel FSW on PrEP options so that FSW can make informed choices. Moreover, geographic differences emerged in terms of LAI-PrEP’s ability to be compatible with current workflows. Ehlanzeni providers expected more disruptions to current services and workflows from the addition of LAI-PrEP delivery, whereas eThekwini providers felt that little to no changes would need to be made to accommodate LAI-PrEP. This difference could be attributed to several clinic-level differences, with the eThekwini study site having a dedicated FSW program space (separate from other key population programs) and a larger number of mobile van teams. Additionally, providers at both sites believed that existing infrastructure such as client databases and track-and-trace systems could be expanded to include LAI-PrEP clients, although these efforts may be undermined by funding disruptions.
Lastly, this study has important implications for planning an equitable and efficient delivery of LAI-PrEP among FSW in South Africa. The results support the tailoring of LAI-PrEP implementation strategies to meet FSW and provider needs while leveraging programmatic and clinic-based strengths. We found varying individual preferences regarding where to receive LAI-PrEP (i.e., mobile van or clinic), highlighting the need to have both delivery modalities available. This aligns with existing literature that advocates for making adaptations to innovations based on client contexts. 49 In addition to several tailoring strategies, such as providing education on LAI-PrEP side effects and integrating other health services with LAI-PrEP appointments, FSW and providers emphasized focusing on community empowerment, a key facilitator to PrEP uptake as suggested by Mantsios et al. 50 FSW requested WhatsApp support groups, which have been shown to have a strong association with oral PrEP continuation among South African FSW, 51 as well as community workshops to communicate and learn from others. Several FSW recommended supplemental sensitization training for innovation deliverers, consistent with Evens et al.’s findings. 28 Utilizing trusted community champions to share their experiences receiving PrEP injections also emerged repeatedly as a potential strategy to increase LAI-PrEP acceptability.
A major strength of this study is our use of the CFIR for instrument development, data collection, and analysis, which allowed for a standardized and theory-driven assessment and interpretation of numerous multilevel contextual factors. The CFIR also enabled us to conduct a prospective assessment of LAI-PrEP implementation within an established FSW HIV prevention program, equipping future implementers to proactively address the anticipated barriers and act upon the anticipated preferences and facilitators identified from our study. Secondly, we obtained nuanced insights from the inclusion of both FSW with varied lived experiences with HIV prevention programming and providers with extensive familiarity delivering PrEP, across two distinct contexts in South Africa. Finally, the interviews and focus groups were conducted in two different geographic contexts among both older and younger FSW, allowing for a greater diversity of perspectives to emerge.
Limitations
However, there are several limitations of the study. Interviews and focus groups were not designed with the intention of capturing distinct perspectives and instead served to complement one another during data analysis. Additionally, since LAI-PrEP was not yet widely available in South Africa at the time of the study, our findings may not be fully representative of the experiences and challenges that FSW and providers may face during national rollout. Another limitation is the small number of FSW in the younger age category (n=3) due to recruitment challenges (e.g., differences in work hours, social spaces, networks), limiting our ability to make comparisons across age groups. Future research should investigate how LAI-PrEP implementation preferences and determinants among FSW may differ across age groups, particularly as young FSW remain at elevated risk of HIV compared to their older counterparts. 7 Similarly, because uptake of oral PrEP among FSW at both study sites has been very high, we experienced difficulty recruiting FSW who had little or no prior experience with oral PrEP. Using convenience sampling to recruit FSW who were already accessing TB HIV Care HIV prevention services may have also overrepresented women who are adherent to oral PrEP and/or are experiencing fewer barriers to care. Additional studies should explore perspectives from FSW not currently taking oral PrEP, to further understand the impact LAI-PrEP may have on reaching underserved FSW. Finally, the small number of providers interviewed (n=4) limited our ability to evaluate thematic saturation within this group, and findings from these interviews should be interpreted with this limitation in mind. Because we interviewed clinic-based providers, insights into outer setting implementation determinants were therefore limited. More research is needed to elicit perspectives from key informants within the National and KwaZulu-Natal Departments of Health, as well as from South African policymakers.
Conclusion
The present study characterizes key contextual factors across multiple levels likely to influence future LAI-PrEP implementation within existing FSW HIV prevention programs in South Africa. Taken together, findings from the Individuals and Innovation domains highlight the strong acceptability and perceived relative advantage of LAI-PrEP among both FSW and providers due to its potential to overcome current barriers to oral PrEP uptake/continuation, including daily pill-taking burdens and HIV-related stigma. Moreover, we found some hesitancy surrounding side effects, along with a high community investment and interest in education around LAI-PrEP. As LAI-PrEP implementation is scaled up, findings from the Process domain suggest that approaches to engaging FSW should prioritize intensifying community-based educational outreach, integrating LAI-PrEP into a decentralized service, enhancing client-centeredness, and mobilizing community champions, although current changes in HIV funding structures and plans to introduce LAI-PrEP at public healthcare facilities may pose limitations. Within the Inner Setting, it will be critical to integrate LAI-PrEP within existing health services, leverage existing programmatic resources, and provide LAI-PrEP counseling training to providers, without disrupting current workflows and oral PrEP delivery. The evidence-based implementation of LAI-PrEP for historically marginalized communities at high risk of HIV may increase both the equity and effectiveness, and ultimately the real-world impact, of LAI-PrEP in South Africa.
Footnotes
Acknowledgements
The authors gratefully acknowledge the participants and TB HIV Care program staff who generously shared their time and experiences to make this research possible.
Ethical considerations
The study and its materials were approved by the Johns Hopkins Bloomberg School of Public Health (approval: IRB00027224) on December 12th, 2023, and the University of Pretoria Institutional Review Boards (approval: 647/2023) on November 22nd, 2023. This study was designed and implemented in partnership with TB HIV Care. All research activities had local relevance and were conducted to the highest possible ethical standards, with culturally appropriate informed consent processes and study materials developed with local partners and available in three languages.
Consent to participate
All participants participated in a private informed consent process with the interviewer using a written consent script (available in English, Zulu, or siSwati). This process covered information on the study and potential risks and benefits of participating. All participants provided written informed consent to conduct and publish the study. To minimize risks of psychological and physical harm, and to ensure the dignity, privacy, and confidentiality of study participants, all study staff completed sensitivity training on working with sex workers. Recruitment was conducted alongside the programmatic outreach team during the delivery of routine health services in an effort to minimize the potential for discrimination or incrimination, as sex work remains illegal in South Africa.
Author contributions
K.R. oversaw the conception and design of the study in collaboration with V.C., S.S., S.B., A.R., H.H., J.S., and M.M. Study implementation and data collection was led in South Africa by H.H., J.S., M.M., C.S., N.D., and N.M. Data analysis was led by E.M. in collaboration with K.R., C.C., V.C., A.A., J.G.R., N.D., and N.M. Manuscript writing was led by E.M. with K.R., L.K.B., C.C., J.G.R., S.B., and S.S. providing analytic support and critically reviewing the manuscript. All authors reviewed, revised, and approved the final version of the manuscript presented for publication.
Funding
The authors disclose receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a 2023 developmental grant from the Johns Hopkins University CFAR, an NIH-funded program (P30AI094189) supported by: NIAID, NCI, NICHD, NHLBI, NIDA, NIA, NIGMS, NIDDK, NIMHD. Other sources of support include the National Institute of Mental Health (K.R.: K01MH129226, L.K.B.: K01MH130244, S.S.: R01MH121161, S.B.: P30MH136919), the National Institute on Minority Health and Health Disparities (A.R.: K01MD020002), and the National Institute of Allergy and Infectious Diseases (S.B.: R01AI170249, C.C.: T32AI102623). Content is solely the responsibility of the authors and does not represent official NIH views.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available upon reasonable request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.