
Abstract
Social psychologists fighting prejudice and clinical psychologists fighting depression have long been separated by the social–clinical divide, unaware that they were facing a common enemy. Stereotypes about others leading to prejudice (e.g., Devine, 1989) and schemas about the self leading to depression (e.g., A. T. Beck, 1967) are fundamentally the same type of cognitive structure. According to the integrated perspective on prejudice and depression, negative stereotypes (i.e., schemas) are activated in a Source, who expresses prejudice toward the Target, causing the Target to experience depression. This linking of prejudice and depression (i.e., “comorbid” prejudice and depression) can occur at the societal level (e.g., Nazis’ prejudice causing Jews’ depression), the interpersonal level (e.g., an abuser’s prejudice causing an abusee’s depression), and the intrapersonal level (e.g., a person’s self-prejudice causing his or her depression). The integrated perspective addresses several longstanding paradoxes, controversies, and questions; generates new areas of inquiry; and spotlights specific methods and findings that have direct cross-disciplinary applications in the battle against prejudice and depression. Ironically, some interventions developed by depression researchers may be especially useful against prejudice, and some interventions developed by prejudice researchers may be especially useful against depression.
“I really hate ________. I hate the way ________ look. I hate the way ________ talk.”
What belongs in the blanks? This statement could express prejudice toward a stigmatized group: “I really hate Black people,” “I hate the way gay men look,” or “I hate the way Jews talk.” Although highly plausible, this solution is wrong. In fact, this is a depressed patient talking about herself: “I really hate me. I hate the way I look. I hate the way I talk.” The ease with which these seemingly disparate solutions can be interchanged hints at a fundamental connection between prejudice and depression. We reveal and explore that connection in this article.
Depression or Prejudice?
Contemplate this Holocaust survivor’s description of her concentration camp:
Some people just went crazy. They started talking to themselves. They walked back and forth. The Nazis just wanted people to die there from hunger and disease. . . . We all lost a lot of weight. We were there for 3 months and if we had been there for another 3 months, I don’t think anybody would have survived. . . . I cried a lot. I didn’t want to live any more. (Bluma, n.d.,)
Is this an example of depression or prejudice? Your answer depends on your perspective, which is strongly influenced by your subdiscipline. For example, the depression and misery of the prisoners in the camp is probably more salient if you are a clinical psychologist, whereas the prejudice and hate of the Nazis may be more salient if you are a social psychologist. Depression and prejudice were comorbid in concentration camps within separate players: the victims and perpetrators. The Jews’ depression was caused by the Nazis’ prejudice (Fig. 1).

Prejudice and depression in the Holocaust. Depression and prejudice were comorbid in concentration camps. The Nazis’ prejudice caused the Jews’ depression.
As a final example, imagine a young boy growing up in the United States. Like anyone else, he learns negative societal stereotypes: Black people are criminal, Jews are greedy, and gay men are immoral. As he grows older, he realizes that he belongs to one of those stereotyped groups—he is gay. An outgroup becomes his ingroup, but that metamorphosis does not make the negative stereotypes disappear. He still has well-rehearsed notions that gay men are immoral, disgusting, and dirty. These newly self-relevant stereotypes devastate this young boy—the disdain formerly turned outward toward others is now turned inward on himself as well. He is troubled and tormented by these thoughts and feelings. He is miserable and withdraws from activities, avoiding his friends and family. He hates himself.
What term would you use to label the psychological phenomenon in this vignette: depression or prejudice? Again, your answer to this question likely depends on your background. If you are a clinical psychologist, you probably see this as depression—the young man hates himself because of well-rehearsed negative schemas. If you are a social psychologist, you probably see this as prejudice—the young man hates a social group because of well-rehearsed negative stereotypes. At what point does the cognitive structure in this story end its tenure as a prejudicial stereotype and convert to a depressive schema?
These two examples demonstrate comorbidity of depression and prejudice, first in a situation, then in a single person. This anecdotal comorbidity highlights an underlying connection, and this article proposes a single, wider perspective that unites depression and prejudice in one model.
The Elephant of Deprejudice
Some have previously crossed the clinical–social divide to understand depression and prejudice (e.g., Abramson, 1988; A. T. Beck, 1999; Dykman & Abramson, 1990; Hatzenbuehler, Nolen-Hoeksema, & Dovidio, 2009; Herek, Gillis, & Cogan, 2009; Hollon & Garber, 1990). But no theorist has built a strong framework across this divide that helps others cross it. To date, work on depression and work on prejudice have proceeded primarily in parallel, with little intersection. We liken these parallel lines of research to the parable of the blind men and the elephant. In this story, two blind men disagree on the nature of an elephant, because they each feel a different part of it. One man feels the elephant’s leg and believes the elephant resembles a pillar, but the other feels its trunk and believes the elephant resembles a snake. Depression and prejudice are both pieces of a greater elephant in the room. We name this elephant deprejudice, which is a portmanteau of depression and prejudice. We argue that depression researchers and prejudice researchers will benefit from expanding the scope of their perspectives to consider each other’s work. In this article, we present the integrated perspective on prejudice and depression, in which we propose that prejudice and depression are not bifurcated problems, but two links in a causal chain that starts with one core cognitive process: stereotyping.
Definitions and Parameters
Depression long has been viewed as a heterogeneous disorder (e.g., Abramson, Alloy, & Hogan, 1997; Freud, 1917; Kraepelin, 1913). We focus on those depressions driven primarily by negative cognitions that people have about themselves (e.g., A. T. Beck, 1967; A. T. Beck & Alford, 2009) or that others have about them. We are neither addressing nor seeking to explain those depressions driven primarily by neurochemical, genetic, or inflammatory processes. Some processes like inflammation, however, may be triggered by negative cognitions or their consequences, such as stress, violence, or deprivation (see A. H. Miller, Maletic, & Raison, 2009). Thus, in such cases, negative cognitions may be the distal cause of depression that is proximally driven by biological processes (e.g., inflammation).
Schemas, stereotypes, and cognitive perspective
Beck’s highly influential cognitive model implicates distorted or dysfunctional thinking in all psychological disturbances (e.g., A. T. Beck, 1967; J. S. Beck, 2011; A. T. Beck & Alford, 2009). This model emphasizes the path from a stimulus (A), to cognitions (B), to subsequent emotions and behavior (C). For example, in depression, when a client’s boyfriend fails to call him (A), it automatically activates the client’s negative self-schema, like “I’m worthless” (B), which leads to depressive emotions and behavior—he feels bad and shuts himself in his room (C). Beck’s model implicates the intermediate cognitive component—automatically activated negative self-schemas—as the crucial contributing factor to depressive emotions and behavior.
The cognitive model of depression translates directly to cognitive accounts of prejudice (e.g., Devine, 1989). For example, Devine’s model proposes that when someone encounters a Black person (A), it automatically activates stereotypes about Black people (B), leading to prejudicial emotions and behavior (C). Like Beck’s model, Devine’s model implicates the intermediate cognitive component—automatically activated stereotypes—as the crucial contributing factor to prejudicial emotions and behavior. According to these cognitive perspectives, both depression and prejudice stem from underlying dynamic knowledge structures: negative schemas about the Self and negative stereotypes about Others, respectively.
Stereotypes
We see no compelling reason for the distinction between stereotypes studied by prejudice researchers and schemas studied by depression researchers. A careful examination of the literature reveals them to be the same type of cognitive structure. Both schemas about the Self and stereotypes about Others are well-rehearsed, automatically activated cognitive structures (depression: Bargh & Tota, 1988; A. T. Beck, 1967; A. T. Beck & Alford, 2009; Eaves & Rush, 1984; Fiske, 1998; Wenzlaff, Wegner, & Roper, 1988; prejudice: Devine, 1989; Dunn & Spellman, 2003; Hamilton & Trolier, 1986; Hilton & von Hippel, 1996). These structures are often infused with affective valence, have behavioral implications, vary in their accuracy, bias information processing, and are difficult to change (depression: Abramson et al., 2002; A. T. Beck & Alford, 2009; Gotlib, Krasnoperova, Yue, & Joormann, 2004; prejudice: Devine, 1989; Hamilton & Sherman, 1994; Hilton & von Hippel, 1996).
Indeed, the distinction between stereotypes and schemas is more apparent than real, and it creates a semantic barrier that is more a matter of custom and tradition than a conceptually or empirically justified conclusion. As such, this distinction impedes scientific progress (see Ranganath, Spellman, & Joy-Gaba, 2010). A primary goal of this article is to reveal benefits derived from removing this somewhat arbitrary distinction, which amounts to a jangle fallacy (Kelley, 1927). A jangle fallacy occurs when people think that two concepts, such as stereotypes and schemas, are different because they have different names, when in fact they may actually be equivalent (Kelley, 1927). By current conceptualizations, a stereotype is a schema about a group of people. Given the conceptual equivalence of schema and stereotype, we propose slightly expanding the definition of stereotype, so that the term can also refer to cognitions about a single person. Stereotype is an apt word in both cases, because it connotes something that may be untrue, is ethically and morally problematic, and should be overcome (Devine, 1989; see also A. T. Beck, 1988).
Specifically, we define stereotype as a cognitive link between two social or personal concepts (e.g., the Self, social groups, identities, attributes, traits, behaviors) that are not defining features for one another (Allport, 1954; Devine, 1989). For example, if dark skin is the defining feature for being Black, then the link between dark skin and the Black racial group is not a stereotype. But, a link between Black and poor is a stereotype, even if there is a correlational, causal, or cultural connection. Stereotyping is the application of a stereotype (Bodenhausen & Wyer, 1985; Devine, 1989; Hamilton & Sherman, 1994), inferring one characteristic (e.g., worthless) from the other (e.g., me). See a few graphic examples of stereotype links in Figure 2.
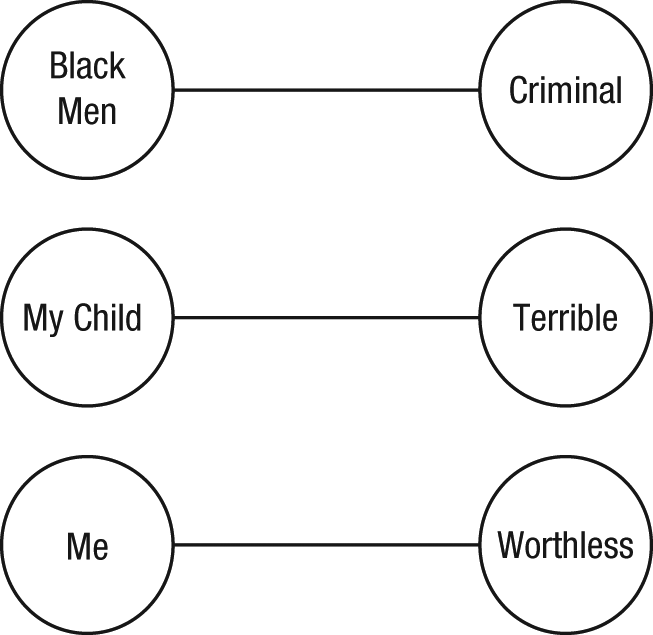
Stereotypes. A stereotype is a cognitive link between two human concepts (e.g., the Self, social groups, identities, attributes, traits, behaviors) that are not defining features for one another. A stereotype can be about a single person or a group of people, and a stereotype can exist in the mind of only one person or be socially shared by a group of people. Stereotypes are automatically activated, oversimplified, overgeneralized, difficult to change, and strongly influence emotions, judgments, and behavior.
A stereotype can be almost any thought that oversimplifies a person or group, although we will focus primarily on negative, well-rehearsed, automatically activated stereotypes. There are several relevant characteristics of stereotypes to note:
Stereotypes can be socially shared (i.e., consensual, collective) or exist in the mind of only one person (i.e., nonconsensual, individual; see Ashmore & Del Boca, 1979; Stangor & Schaller, 1996).
Stereotypes can be based on a prominent group membership (e.g., a woman stereotyping herself as nurturant because of her gender), based on a mundane characteristic (e.g., someone stereotyping a man as Irish because he has red hair), or be unrelated to social group (e.g., a wife stereotyping her husband as lazy).
Stereotypes can link people to characteristics that are negative (e.g., criminal), neutral (e.g., enjoys basketball), or positive (e.g., good at math). Even positive stereotypes can have undesirable negative sequelae, because they set up unfair expectations (see shifting standards; Biernat & Vescio, 2002; McCabe & Brannon, 2004).
Although some stereotypes may reflect correlated features in the world, they are very often inaccurate, oversimplified, fixed overgeneralizations (Judd & Park, 1993). Also, “it is possible for a stereotype to grow in defiance of all evidence,” developing where no real correlations exist (Allport, 1954; p.189; see Hamilton & Gifford, 1976).
Stereotypes are often plausible, compelling, and vivid. They often result in internal, stable, and global attributions about the target of the stereotype (Abramson, Seligman, & Teasdale, 1978; Allport, 1954; A. T. Beck & Alford, 2009; Pettigrew, 1979).
Stereotypes lead to heuristics and biases of information processing, emotions, behavior, judgment, attention, interpretation, and memory (e.g., Hertel & Mathews, 2011; Kahneman, Slovic, & Tversky, 1982; Nisbett & Ross, 1980).
It is easier to create a new stereotype than to change an existing one (L. Ross, 1977).
Someone may whole-heartedly believe an activated stereotype, or it may be in direct opposition to his or her consciously endorsed beliefs (Devine, 1989).
Stereotypes and the emotions and behaviors they engender vary along an intensity continuum, from merely activating a brief thought or subtle emotion to evoking extreme violence.
In sum, a stereotype can be about many people or only one person, and it can exist in the minds of many people or only one person. Eliminating the jangle fallacy with this definitional modification of stereotype is the crux of our argument. It is a small, simple adjustment, but it may have large, powerful implications. Whether the literature has historically called them schemas or stereotypes, these structures have the same psychological, cognitive, and existential essence.
The Integrated Perspective on Prejudice and Depression
Building on our definition of stereotype, we return to the Holocaust to identify key parameters in the integrated perspective. The Holocaust has had a strong and enduring influence in the field of psychology. Milgram (1965), for example, studied forces that encourage people to deliver inescapable electric shocks to another person, and Seligman (1975) studied the psychological effects of receiving inescapable shocks. These are microcosms of the concentration camp experience in psychology laboratories—Milgram examined the source of oppression and prejudice, and Seligman examined the target of that oppression and prejudice.
Sources and Targets
The research programs above illustrate key concepts in the integrated perspective: the Source (i.e., the person or people who hold the stereotype) and the Target (i.e., the person or people the stereotype is about) of stereotyping. We classify each Source and Target as either the Self or an Other. Matching our definitional parameters above, an Other can be a group (e.g., all Nazis, all Black people) or a single person (e.g., an abusive parent, a hated classmate). Every stereotype needs both a Source and a Target, just as a transitive verb needs both a subject and an object.
Following stereotype activation, Sources often exhibit emotions such as disdain, disgust, hate, and anger and behaviors like disdainful avoidance of and aggression toward the Target. In other words, Sources often express prejudice. Sources direct prejudice toward Targets, and in response, Targets often experience despair, sadness, anhedonia, depletion, stigma, and hopelessness and exhibit behaviors like social withdrawal, shameful avoidance, and even catatonia. In other words, Targets often experience depression. See Figure 3.

Sources and Targets of stereotyping. Sources have stereotypes about Targets. When the stereotype is activated, Sources express prejudice, which causes depression in Targets. The term deprejudice describes comorbid depression and prejudice, which can occur at the intrapersonal, interpersonal, and societal levels.
As noted earlier, both a Source and a Target can be either a group or a person: prejudice from a group toward another group (e.g., Nazis toward Jews), prejudice from one person toward another person (e.g., an abusive parent toward his/her child), prejudice from a group toward one person (e.g., a nation toward its leader), prejudice from one person toward a group (e.g., a lone wolf terrorist toward the government), or even prejudice from one person toward himself or herself (e.g., a man toward himself).
The Deprejudice Quadruplex
The possible combinations of Sources (Self or Other) and Targets (Self or Other) of stereotyping yield four cells, each denoting a distinct role: the Prejudice Perpetrator, the Prejudice Victim, the Beckian Depressive, and the Observer. These roles are represented in the deprejudice quadruplex (Fig. 4). Although the quadruplex displays these roles in boxes, it does not imply that people fall neatly into only one of them. For clarity, we discuss each cell of the quadruplex in its purest form, although people may span multiple cells (e.g., be both a Prejudice Victim and a Beckian Depressive simultaneously).
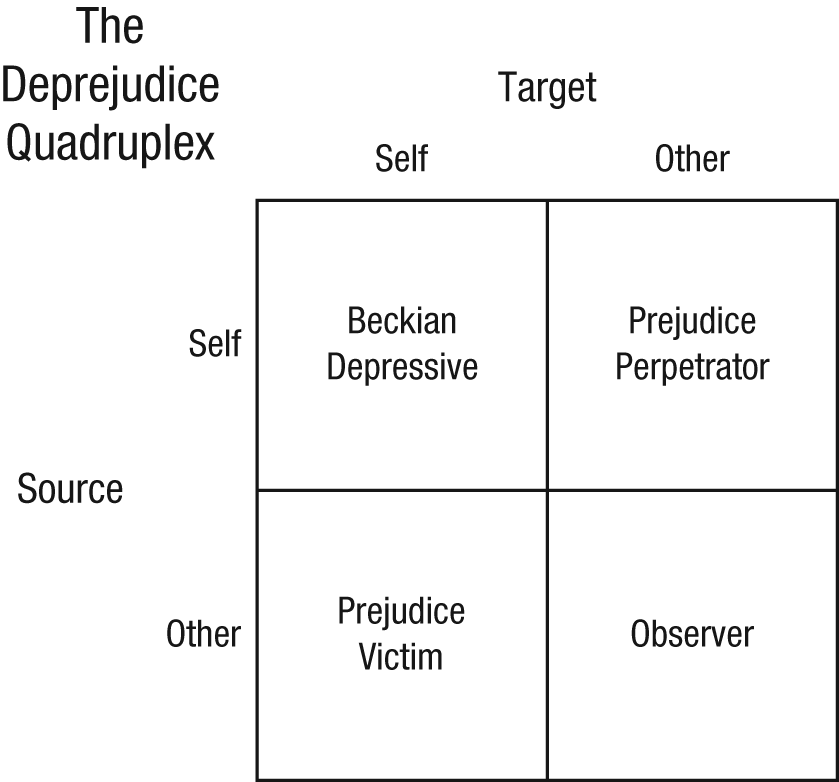
The deprejudice quadruplex. The integrated perspective unifies the cognitive components of depression and prejudice as one cognitive process: stereotyping. Stereotyping involves two players, the Source and Target, who can either be the Self or an Other, yielding four possible roles.
Prejudice Perpetrator—Source of stereotyping: Self/Target of stereotyping: Other
When one is in the role of a Prejudice Perpetrator, the Source of bias is the Self, but the Target is an Other. Encountering a Target activates the Source’s stereotype about that Target, which produces prejudicial emotions and behavior (Allport, 1954; Devine, 1989; Hamilton & Trolier, 1986). Prejudice Perpetrators often express prejudice, including emotions such as anger, hate, disdain, and disgust (Dasgupta, DeSteno, Williams, & Hunsinger, 2009; Hudepohl, Parrott, & Zeichner, 2010; Mackie, Devos, & Smith, 2000; Taylor, 2007; Terrizzi, Shook, & Ventis, 2010; Van de Ven, Bornholt, & Bailey, 1996). Behaviors range from simple avoidance and reduced eye contact, to discrimination, to the extremes of violence, such as bullying and hate crimes, including murder (e.g., Agerström & Rooth, 2011; Berrill, 1992; Bertrand & Mullainathan, 2004; Craig, 2002; Cuddy, Fiske, & Glick, 2007; Dasgupta & Rivera, 2006; Dovidio, Kawakami, Johnson, Johnson, & Howard, 1997; Drwecki, Moore, Ward, & Prkachin, 2011; Farrell & Jones, 1988; Green et al., 2007; Herek, 2009; Katz-Wise & Hyde, 2012; Kumpulainen et al., 1998; McConnell & Leibold, 2001; Nansel et al., 2001; Parrott & Zeichner, 2005).
The Nazis exemplify classic Prejudice Perpetrators. Other examples of Prejudice Perpetrators are people who express mild, subtle prejudice and people who are abusive because of negative stereotypes about their victims (but not abusers who lash out because of other disturbances). Like someone expressing outgroup prejudice, abusers often have negative stereotypes about the person they mistreat (e.g., “my child is a rotten kid,” “my wife is an idiot”), experience emotions such as anger and disgust, and express behaviors ranging from avoidance to violence (A. T. Beck, 1999; for a review, see Seng & Prinz, 2008; Wilson, Rack, Shi, & Norris, 2008). All Prejudice Perpetrators are expressing prejudice toward an Other that arises from a stereotype.
Children can learn outgroup stereotypes at a young age from a variety of societal influences (e.g., parents, schools), becoming Prejudice Perpetrators before they may develop values that oppose stereotyping and prejudice (Hirschfeld, 1995; Mackie, Hamilton, Susskind, & Rosselli, 1996; see Devine, 1989). Implicit but unintended stereotyping and prejudice are frequently at odds with a Prejudice Perpetrator’s explicit beliefs and values that oppose prejudice (Devine, 1989). This discrepancy often produces guilt and activates efforts to reduce the expression of prejudice (Amodio, Devine, & Harmon-Jones, 2007; Devine, Monteith, Zuwerink, & Elliot, 1991; Monteith, 1993). Of course, sometimes implicit stereotyping and prejudice are consistent with a Prejudice Perpetrator’s explicit beliefs and values, as with hate groups such as the Ku Klux Klan, Nazis, groups of bullies, gangs, and so on.
Hate crimes tear apart lives and families (e.g., the mutilations and murders of James Byrd, Sakia Gunn, Lawrence King, Matthew Shepard, Kelly Thomas). The reported rates of hate crimes based on race, religion, and orientation have risen for the last 20 years in the United States and around the world (e.g., Bleich, 2011; Disha, Cavendish, & King, 2011; Gerstenfeld, 2010; Herek, 1989). In the United States, 20% of lesbian, gay, or bisexual (LGB) people report experiencing crimes against themselves or their property based on their orientation, and in 2009 there were over 7500 reported hate crimes on the basis of race, religion, nationality, orientation, or disability (Berrill, 1992; FBI’s Uniform Crime Reporting Program, 2010; Herek, 2009). Prejudice-based bullying is a rampant problem, sometimes even escalating to homicide (e.g., Daniel Ausborne, Lawrence King; see Berlan, Corliss, Field, Goodman, & Austin, 2010; Peskin, Tortolero, & Markham, 2006).
Lastly, genocide expresses the most extreme hatred and has thrived as a prejudice-driven atrocity throughout human history. Since 1900, our species has lost at least 25.2 million lives to genocide (in Bosnia, Burundi, Cambodia, Guatemala, Indonesia, Iran, Namibia, the Nazi Holocaust, Nigeria, Pakistan, Paraguay, Rwanda, Sudan, Tibet, Turkey, Ukraine, and the USSR). Wars and other conflicts rooted in prejudice have even greater death tolls. Whatever their intensity or scale, a Prejudice Perpetrator is the Source of stereotyping and prejudice directed at an Other: the Prejudice Victim.
Prejudice Victim—Source of stereotyping: Other/Target of stereotyping: Self
When one is in the role of a Prejudice Victim, the Source of bias is an Other, and the Target is the Self. As Targets, Prejudice Victims often experience depression, which can include sadness, depletion, anhedonia, hopelessness, social withdrawal, or even catatonia. Prejudice Victims also experience stigma (Goffman, 1963), a state of personal disgrace and devaluation, which is a crucial component of a Target’s depression.
Following our model definitions, Prejudice Victims can be targeted because of a group membership, such as race or orientation, or they may be targeted irrespective of group membership, as with children in abusive homes. Victims of abuse, rape, domestic violence, bullying, and hate crimes, members of stigmatized groups, and Holocaust prisoners exemplify the Prejudice Victim, often experiencing massive victimization from an Other, resulting in depression (Alloy, Abramson, Smith, Gibb, & Neeren, 2006; Cogan, 1996; Hershberger & D’Augelli, 1995; Kaltiala-Heino, Rimpelä, Marttunen, Rimpelä, & Rantanen, 1999; Koss, 1983; Ullman & Brecklin, 2002). Bullying victims have increased rates of clinical depression, severe suicidal ideation, and other mental health problems (e.g., Hershberger & D’Augelli, 1995; Kaltiala-Heino et al., 1999). Also, they often ruminate, constantly replaying insults they receive in their minds (Cooper, 2011; Hampel, Manhal, & Hayer, 2009). Despite some work showing that their stigmatized group membership protects Black American’s self-esteem (e.g., Crocker & Major, 1989), many researchers argue that Black Americans have high rates of depression that are concealed by racial biases in diagnosis and lower rates of seeking mental health services (e.g., Carrington, 2006; Conner et al., 2010; Frye & Liem, 2011; Leo, Sherry, & Jones, 1998). In fact, most (if not all) stigmatized groups have higher rates of depression than do nonstigmatized groups (e.g., racial minorities: Bradford, Newkirk, & Holden, 2009; Chou, Asnaani, & Hofmann, 2012; Cress & Ikeda, 2003; Guarnero & Flaskerud, 2008; Riolo, Nguyen, Greden, & King, 2005; lesbians/gay men: Guarnero & Flaskerud, 2008; Hetrick & Martin, 1987; Meyer, 2003; Oetjen & Rothblum, 2000; and women: Angold, Costello, & Worthman, 1998; Cyranowski, Frank, Young, & Shear, 2000; Nolen-Hoeksema, 1990; for a review, see Hyde, Mezulis, & Abramson, 2008).
In addition to formally diagnosed depression, Prejudice Victims may also experience other negative mental health outcomes such as post-traumatic stress disorder (D’Augelli, Grossman, & Starks, 2006; Yehuda, Kahana, Southwick, & Giller, 1994). Discrimination and other stressors on stigmatized groups correspond to decreased self-esteem and increased stress, anxiety, rumination, and depletion (Broman, 1997; Chou et al., 2012; Díaz, Ayala, Bein, Henne, & Marin, 2001; Friedman, Williams, Singer, & Ryff, 2009; Hatzenbuehler, Nolen-Hoeksema, et al., 2009; Inzlicht, McKay, & Aronson, 2006; Kessler, Mickelson, & Williams, 1999; Mays & Cochran, 2001; Meyer, 2003; Wei et al., 2010; Williams, Neighbors, & Jackson, 2008; see Neisen, 1993). These effects depend on how the Prejudice Victims react to the discrimination and how strongly they identify with their social group (McCoy & Major, 2003; McLaughlin, Hatzenbuehler, & Keyes, 2010). Even in the absence of any actual discrimination, stigmatized group members’ expectations about the stereotypes Others hold (i.e., meta-stereotypes) relate to lower self-esteem and more negative emotions (Vorauer, Main, & O’Connell, 1998; see Vorauer & Kumhyr, 2001).
Because their Sources of prejudice are an Other, if Prejudice Victims escape from their Prejudice Perpetrators, their depressive symptoms may decrease or even resolve. Also, escape may manifest as Targets “fighting back” against the stereotypes and prejudice, which is analogous to “reactance” against aversive events (Wortman & Brehm, 1975). Fighting back may involve confronting specific proximal Prejudice Perpetrators or confronting the distal Prejudice Perpetration by creating bigger, societal change, as in civil rights movements. A Prejudice Victim facing escapable prejudice or a brief flash of negativity will likely experience fewer negative symptoms than someone facing inescapable prejudice, like a subject in a learned helplessness study (e.g., Abramson et al., 1978; Seligman, 1975). Helplessness born in the face of inescapable prejudice matches the helplessness born in the face of inescapable shocks.
Just as homicide and genocide are the extreme expressions of a Prejudice Perpetrator, the dire life-ending behavior of a Prejudice Victim is suicide. For Prejudice Victims, escape remains focal in suicidal behavior—suicide provides a path to get away from the hatred they face, driven by despair and desire to escape. In the United States, the recent surge in suicides of bullying and cyber-bullying victims (e.g., Tyler Clementi, Carl Hoover, Megan Meier) embodies this escapist suicide (e.g., Baechler, 1979; Maris, 1992). Suicidal Prejudice Victims lack a desire to harm themselves—they merely want to escape the harm they face from Others.
Beckian Depressive—Source of stereotyping: Self/Target of stereotyping: Self
We see how in him (the melancholic) one part of the ego sets itself over against the other, judges it critically, and, as it were, takes it as its object.
Social psychologists historically have studied the Prejudice Perpetrator and Prejudice Victim. As such, their perspectives are generally silent on the inhabitant of the quadruplex’s upper left cell—the person who has negative stereotypes about himself or herself. These people, however, are all too familiar to clinical psychologists and psychiatrists. They have depression driven by negative stereotypes about the Self, and they are featured in Beck’s cognitive model of depression (A. T. Beck, 1967; A. T. Beck & Alford, 2009). To recognize Aaron Beck’s seminal contributions, we named the inhabitant of this cell the Beckian Depressive.
Beckian Depressives may have developed their negative self-stereotypes in various ways. (See also the “Movement Within the Quadruplex” section.) Cognitive theorists of depression (e.g., J. S. Beck, 2011; A. T. Beck & Alford, 2009; Gibb et al., 2001; Rose, Abramson, Hodulik, Halberstadt, & Leff, 1994) have highlighted adverse early experiences with significant others, such as being called stupid or ugly by a parent or being unfavorably compared with siblings, as potent contributors to formation of negative self-stereotypes. Describing these prototypic cases from the perspective of the deprejudice quadruplex, the future Beckian Depressive (e.g., a child) is a Prejudice Victim who internalizes the negative stereotypes directed at him or her by a Prejudice Perpetrator (e.g., a parent). Similarly, although given less attention by cognitive theorists of depression (but see Hatzenbuehler, Nolen-Hoeksema et al., 2009), members of stigmatized groups (e.g., African-American children) may internalize negative stereotypes directed at them by Prejudice Perpetrators based on their group membership (see Clark & Clark, 1939). Alternatively, a child may develop negative self-stereotypes as a result of failure experiences, with no input from a Prejudice Perpetrator (see A. T. Beck & Alford, 2009). Also, people may learn negative stereotypes about a stigmatized group (e.g., the homeless), which become self-relevant when they acquire membership in that group (e.g., become homeless themselves). In addition, temperamental (e.g., Mezulis, Hyde, & Abramson, 2006) and even biological (e.g., Beck, 2008; Disner, Beevers, Haigh, & Beck, 2011) factors may contribute to formation of negative self-stereotypes. Finally, some people may develop negative self-stereotypes for reasons not currently understood.
Ironically, the integrated perspective unites contemporary Beckian and earlier Freudian perspectives on depression. Beck, who was originally a Freudian, developed his cognitive model in part as a reaction against psychoanalytic accounts of depression that emphasized “anger turned inwards” (A. T. Beck & Alford, 2009; Freud, 1917, p. 246). The integrated perspective, however, offers a reconstruction of this psychoanalytic notion. The Beckian Depressive’s negative self-stereotypes create prejudice against the Self, which can be construed as “anger turned inwards.” Anger is not the only relevant emotion that can turn inward—different stereotypes will give rise to different prejudicial emotions, like pity (e.g., Rosenthal & Gudeman, 1967). Although Freud invoked different processes than those featured here, our reconstruction of his perspective captures an essential feature of some Beckian Depressives. More generally, the Freud quotation above captures the core of Beck’s model—negative self-judgment—and the integrated perspective highlights and defines that parallel.
The integrated perspective adds to other perspectives on Beckian Depression by emphasizing the Source and the Target as two separate players within one person. Beckian Depressives are not “just” depressed—they are expressing prejudice directed toward the Self that causes their depression. Playing the role of both Source and Target, Beckian Depressives combine and compound the negative emotions and behaviors of the Prejudice Perpetrator and Prejudice Victim within a single person. The Source expresses prejudice, hate, anger, and disdain, and the Target experiences depression, depletion, sadness, hopelessness, and stigma. Continuing the Holocaust analogy, the Beckian Depressive’s two players resemble a Nazi handcuffed to a Jew within one person—the hater and the hated, unable to escape one another. The discomfort and horror of this pairing captures the essence of severe depression due to hateful prejudice against one’s Self.
The Beckian Depressive’s two players bring to mind a paradox of depression first identified by Abramson and Sackeim (1977). They noted that the self-blame and the perceptions of helplessness commonly found in depressed people seem contradictory and confusing. Why should depressed people blame themselves for events they believe they cannot control? The apparent contradiction, however, is resolved within the integrated perspective. The blame arises from the Source, whereas the perceptions of helplessness arise from the Target. With both players in one body, Beckian Depressives may exhibit seemingly contradictory cognitions, emotions, and behaviors.
Understanding both players is key to helping Beckian Depressives, although clinical psychologists cannot easily disconnect them because they reside in a single person (but see the two-chair technique; Greenberg, 1979). As our previous review reveals, however, the study of Prejudice Perpetrators (i.e., “pure” Sources) and the study of Prejudice Victims (i.e., “pure” Targets) can offer insights about each discrete player. Stigma, for instance, is a feature of Targets that was previously unspecified in descriptions of Beckian Depression. Stigma reduces a Target “from a whole and usual person to a tainted, discounted one” (Goffman, 1963, p. 3), a fitting characterization of stigma in a Beckian Depressive. Just as Prejudice Victims can be the Target of a stereotype because of their group membership or for no apparent reason, so too can a Beckian Depressive’s self-stereotype relate to group membership or not. Likewise, the prejudice regulation efforts and guilt often seen in “everyday” Prejudice Perpetrators are also relevant to Beckian Depressives. The integrated perspective sheds light on many of these parallels.
Just as Prejudice Perpetrators’ behaviors and emotions can range from subtle, mild prejudice to blatant, extreme prejudice, Beckian Depressives also show great variability in severity. Less extreme Beckian Depressives may only express mild prejudice toward themselves. In contrast, the most extreme Beckian Depressives may engage in acts of aggression and violence toward the Self, as in self-punishment and nonsuicidal self-injury (Forrest & Hokanson, 1975; Nock, Joiner, Gordon, Lloyd-Richardson, & Prinstein, 2006; Paykel, 1971; Rosenthal & Gudeman, 1967). Like extreme Prejudice Perpetrators, these Beckian Depressives are acting out violence from the Source to the Target (this may occur most in severely depressed people with borderline personality disorder, see Kellogg & Young, 2006). These extreme Beckian Depressives may cut or mutilate their bodies, like a hate criminal mutilating a hated minority. Alternatively, such Beckian Depressives may cut or mutilate themselves to reduce the intense negative emotions they experience as Targets of their self-directed prejudice (see Klonsky, 2011, and Nock & Prinstein, 2004, for a discussion of the distress-reducing function of nonsuicidal self-injury).
For any Source, the most extreme expression of hostility is to kill the Target. Beckian Depressives may commit suicide motivated by hatred of the Self, just as Prejudice Perpetrators may commit homicide motivated by hatred of an Other. For the Source within a Beckian Depressive, hateful suicide is the ultimate hate crime—a self-homicide. Like the Prejudice Victim, however, a Beckian Depressive may also commit escapist suicide, in which the Target commits suicide to escape. Whereas some commit escapist suicide to escape physical pain and suffering, Beckian Depressives may also try to escape aversive self-awareness (see Baumeister, 1990; Maris, 1992). For the Beckian Depressive, subtypes of suicidal behavior (hateful vs. escapist) separate by which player drives the suicide. Is the act driven by the Source’s prejudice or the Target’s desire to escape from that prejudice? Who holds the knife—the Source or the Target?
Past Criticisms and Proposed Distinction: Beckian Depressive vs. Prejudice Victim
As we have elaborated, the Prejudice Victim differs from the Beckian Depressive. We mentioned the jangle fallacy earlier, and these distinct subtypes bring to mind its counterpart, the jingle fallacy (Thorndike, 1904). A jingle fallacy occurs when people think that two different phenomena are the same because they are given the same label (e.g., “clinical depression”).
In this vein, the integrated perspective addresses a bitter controversy in the field of depression. Specifically, Coyne has long criticized cognitive theories of depression (e.g., Abramson, Metalsky, & Alloy, 1989; A. T. Beck, 1967, 1987), arguing that they obscure the degree to which “depression occurs in depressing circumstances” and downplay the role of negative environments in creating and maintaining depressive cognitions (Coyne, 1992, p. 233; Coyne & Gotlib, 1983, 1986; see also Krantz, 1985). The deprejudice quadruplex helps reconcile Coyne’s criticisms with cognitive theories of depression.
Coyne’s admonishment is fitting for “pure” Prejudice Victims, who become depressed without any negative self-stereotypes. For such pure Prejudice Victims, prejudice from an Other creates a toxic environment (e.g., chronic brutalization, overwork, low access to rewards, social ostracism) that, in turn, produces depression. There is no necessary negative cognition about the Self within the Prejudice Victim — the Source is an Other. Nevertheless, some Prejudice Victims may internalize the negative stereotypes directed at them and become Beckian Depressives as well (again, see our discussion of internalization in the “Movement Within the Quadruplex” section later in this article). In such cases, it is as important to highlight the internalized negative stereotype (cognitive perspective) as it is to highlight the negative environment that may continue to fuel the negative stereotype and the depression (Coynian perspective). Also, some people may self-stereotype with little or no environmental input, residing mainly in the Beckian Depressive cell. In these latter cases, Coyne’s criticism is not warranted.
Each of the possibilities above has different features and may require different treatment considerations. Some theorists have already recognized that depression can come from an Other, suggesting a differential diagnosis for Targets of societal prejudice who exhibit depressive symptoms (e.g., Poussaint, 1990; Vontress, Woodland, & Epp, 2007). The integrated perspective joins these theorists, declaring that the Prejudice Victim is distinct from the Beckian Depressive.
Observer—Source of stereotyping: Other/Target of stereotyping: Other
The Observer resides in the final cell of the deprejudice quadruplex and observes stereotyping from an Other toward an Other. Observers could be scientists or clinicians, observing a participant’s or patient’s stereotyping, or a lay bystander, perhaps a child observing a parent’s stereotyping. Observers may also be “active” Observers who intervene and try to stop the stereotyping and prejudice.
The Observer cell is often a starting point for acquiring stereotypes. Observational learning and modeling are implicated in the formation of outgroup stereotypes (Ashmore, 1970; Mackie et al., 1996; cf. Hirschfeld, 1995). A child may learn to self-stereotype by adopting a cognitive style similar to that of his or her parent (i.e., modeling; Alloy et al., 2001). Even subtle forms of social influence can affect an Observer’s cognitions. For example, people can even “catch” depressive symptoms from their roommates (contagious depression, Joiner, 1994). In a similar vein, talking to depressed people on the phone can increase depressive symptoms (Coyne, 1976). As Observers learn stereotypes and begin to express prejudice toward Targets, they move to another cell of the quadruplex, becoming Sources.
Movement Within the Quadruplex
One special advantage of the deprejudice quadruplex is its ability to illuminate possible movement from one cell to another. Indeed, considering these issues provides a useful perspective on stereotype acquisition and yields insights into other areas of research. For instance, depression research and prejudice research have historically overlapped most explicitly in one area—the study of internalized prejudice (e.g., see Herek et al., 2009). “Internalized prejudice” is based on the idea that members of stigmatized groups internalize prejudice directed at them by society, which causes depression. Evidence for internalized prejudice usually involves correlating depression with ingroup prejudice in members of stigmatized groups (e.g., Herek et al., 2009; Igartua, Gill, & Montoro, 2003; Szymanski, Chung, & Balsam, 2001).
We identify two distinct developmental pathways that could lead to what the extant literature calls internalized prejudice. On the one hand, Prejudice Victims may become Beckian Depressives when they adopt negative stereotypes that Others directed at them, as the internalized prejudice literature most commonly assumes. We will call this internalization. On the other hand, recall the antigay young man from the beginning of this article who realized he was gay. Nothing was internalized there—the pivotal event was his group membership change. He was a Prejudice Perpetrator and became a Beckian Depressive when his preexisting stereotypes became self-relevant (Fig. 5). By using one term, internalized prejudice, to encapsulate these two theoretically distinct phenomena, the current literature is making another jingle fallacy. The integrated perspective uncovers this jingle, and we will now explore each of these two pathways in turn. In so doing, we will review findings from the internalized prejudice literature where we think they fit best, but keep in mind that these correlational findings could reflect either internalization or preexisting stereotypes becoming self-relevant (or a combination of both). Future research should disentangle these developmental trajectories empirically.
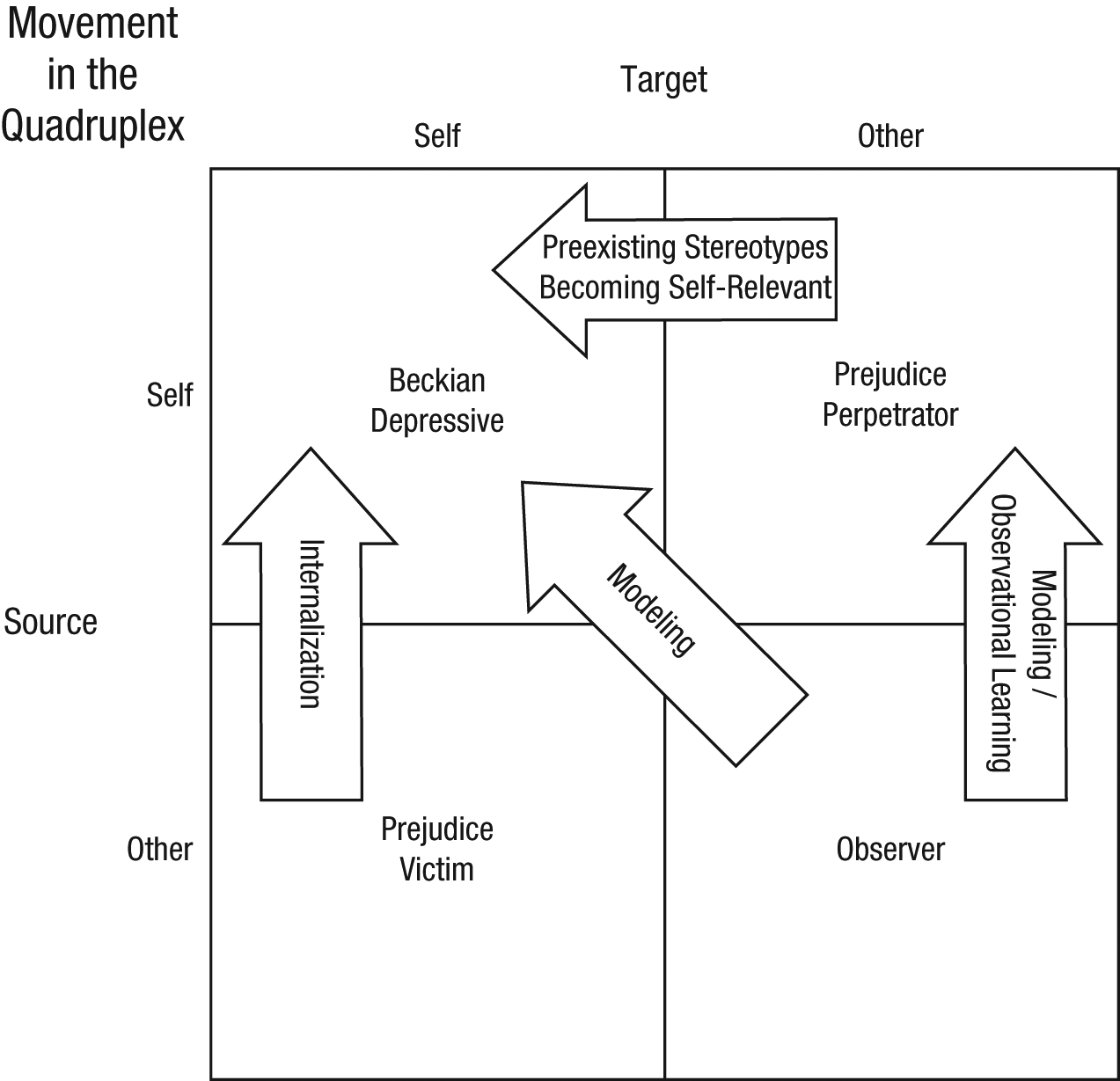
Movement in the Deprejudice Quadruplex. An Observer may acquire stereotypes by modeling or observational learning to become a Source. A Prejudice Victim can internalize negative stereotypes and move into the Beckian Depressive cell. If Prejudice Perpetrators become members of a stigmatized group they negatively stereotype, their preexisting stereotypes become self-relevant, making them Beckian Depressives.
Many theorists discuss internalization, noting that people may acquire negative self-stereotypes because of adverse experiences in early life (e.g., A. T. Beck & Alford, 2009; Rose et al., 1994; see Clark & Clark, 1939). Also, stigmatized group members (e.g., “self-hating Jews”) often self-stereotype or display implicit outgroup favoritism, consistent with internalization (e.g., Hogg & Turner, 1987; Jost, Banaji, & Nosek, 2004; Latrofa, Vaes, Cadinu, & Carnaghi, 2010; Poussaint, 1983). Abuse victims may also internalize their abusers’ negative stereotypes about them. We predict that extreme self-prejudice and violence are most likely to occur following internalization of extreme prejudice, like abuse or hate crimes. Prejudice Perpetrators (e.g., abusers) may generate more violent, hateful thoughts, which Prejudice Victims internalize to become Beckian Depressives with more violent, hateful self-stereotypes (Rose et al., 1994). A “spontaneous” Beckian Depressive, who develops negative self-stereotypes without internalization, may be less likely to generate such extreme stereotypes, emotions, and behaviors.
Contrast internalization to the other pathway, when preexisting stereotypes become self-relevant. If Prejudice Perpetrators endorse negative stereotypes about a group and then acquire membership in that group, it “turns their prejudice inwards,” causing Beckian Depression. Self-hating LGB people provide prototypical examples of this process. Most LGB people realize their stigmatized status at puberty or later, long after they have learned pernicious anti-LGB stereotypes. These preexisting negative stereotypes then apply to the Self following the group membership change. Indeed, depression in LGB people is strongly tied to their own anti-LGB prejudice (Hatzenbuehler, Dovidio, et al., 2009; Herek et al., 2009; Igartua et al., 2003; Simon, Glässner-Bayerl, & Stratenwerth, 1991; Szymanski et al., 2001).
Realizing that one is gay, lesbian, or bisexual is only one example of a situation in which preexisting stereotypes may become self-relevant. Imagine a woman in the workforce who has stereotypes that unemployed people are lazy, stupid, and incompetent. When she loses her own job, her negative stereotypes about unemployed people suddenly apply to herself, adding to her job loss. Also, many thin Prejudice Perpetrators against the obese probably retain their negative obesity stereotypes when they unexpectedly gain weight. This is one explanation for the strong anti-obesity prejudice observed in obese people and the relationship between obesity and depression (see Cramer & Steinwert, 1998; Markowitz, Friedman, & Arent, 2008; Puhl & Heuer, 2009; Wang, Brownell, & Wadden, 2004). No stigmatized status is more appropriate to consider than the one the luckiest of us will all acquire: old age. People with more negative age stereotypes will likely have higher rates of depression as they get older. Mental disorders, physical disability, homelessness, and having a sexually transmitted infection are all stigmatized statuses someone can gain despite having negative stereotypes about those groups.
The extant literature jingles these different pathways to Beckian Depression—internalization and preexisting stereotypes become self-relevant—as internalized prejudice, but their essences are different. One pathway begins in the Prejudice Victim cell, whereas the Other begins in the Prejudice Perpetrator cell. Internalization involves adopting new self-relevant stereotypes from Others, not preexisting stereotypes becoming self-relevant.
In addition to being Beckian Depressives, people who have internalized or whose preexisting stereotypes became self-relevant are likely Prejudice Victims as well, facing prejudice from Others. Facing prejudice on multiple fronts may drive these people to more severe depression. Considering these issues, L. E. Ross, Doctor, Dimito, Kuehl, and Armstrong (2007) developed a successful intervention for LGB people specifically targeted at prejudice from Others and the Self. Also, Robinson and Bacon (1996) developed a treatment program for overweight women that helped them break down their personal stereotypes as Sources, face prejudice from Others as Prejudice Victims, and adjust their eating and exercise habits (i.e., working to dissociate them from the stigmatized group—the obese). Beckian Depressives who have internalized or whose preexisting stereotypes became self-relevant may span multiple cells of the quadruplex, and their therapy should fight stereotyping on all battlefronts.
Applications: Joining Forces in the Battle Against Stereotyping
We now review some methods for fighting negative stereotypes about Others or the Self, culled from both clinical and social psychological traditions. By uniting depression and prejudice in one larger model, the integrated perspective provides a framework for identifying methods and findings from each discipline that can help the other. Ironically, some interventions developed by depression researchers may be especially useful for reducing Prejudice Perpetration, and some methods developed by prejudice researchers may be especially useful against Beckian Depression. This “armamentarium sharing” is a key contribution of the integrated perspective.
Crucial to the battle against stereotyping is the distinction between automatic and controlled processes (see Devine, 1989). Many stereotype reduction techniques attempt to “fight fire with fire” through the use of automatic, nonintentional methods to reduce automatic, nonintentional stereotyping (e.g., Araya, Akrami, Ekehammar, & Hedlund, 2002; Clerkin & Teachman, 2010; Olson & Fazio, 2006; for reviews, see Blair, 2002; Hertel & Mathews, 2011; Paluck & Green, 2009; Shalev & Bargh, 2011). Nevertheless, many theorists propose that long-term stereotype change requires people to “fight fire with water” through the use of controlled, effortful processing to override and restructure automatic stereotyping (Barber & DeRubeis, 1989; A. T. Beck & Alford, 2009; Devine, 1989; Devine, Forscher, Austin, & Cox, 2012; Devine & Monteith, 1993; S. R. Levy, 1999). We start by discussing these effortful, controlled methods, especially cognitive behavior therapy (CBT). Applying CBT interventions to Prejudice Perpetration is a powerful contribution of the integrated perspective. Also, the prejudice literature offers insights into some unintended consequences of effortful armaments like CBT, illuminating some difficulties that CBT may have with Beckian Depression. And finally, we will explore a variety of automatic and nonintentional techniques that can reduce stereotyping without conscious effort or intention.
The controlled, effortful armamentarium against stereotyping
CBT is an effective, empirically supported intervention that harnesses effortful processing to override and restructure stereotypes. Based on Beck’s cognitive model, CBT focuses on changing how a Source’s stereotypes are activated and applied in order to change the feelings and behaviors that follow. We provide a basic overview of CBT, but for more extensive reviews, see A. T. Beck (2005), J. S. Beck (2011), Hollon (2003), Hollon and Shelton (2001), or Hollon and Dimidjian (2009). For a CBT perspective on societal Prejudice Perpetration, see A. T. Beck (1999). For a perspective on deprejudice within romantic couples, see A. T. Beck (1988).
Although originally developed for Beckian Depressives, CBT is highly relevant for Prejudice Perpetrators. One crucial difference, however, is motivation. Most Beckian Depressives in therapy are intrinsically or extrinsically motivated to reduce their self-directed prejudice, whereas few seek therapy to reduce their other-directed prejudice. Nevertheless, there is substantial evidence that many Prejudice Perpetrators are motivated to reduce their prejudice (e.g., Amodio et al., 2007; Monteith, 1993; Plant & Devine, 2009), and CBT for Prejudice Perpetration may be well suited to these people. In fact, Devine and colleagues (2012) developed a successful Prejudice Perpetrator intervention with many conceptual parallels to CBT. Like CBT, their intervention taught Sources to be aware of their automatic thoughts and to intentionally deploy a variety of cognitive techniques against automatic stereotyping. Further exploring CBT for Prejudice Perpetration is an important outgrowth of the integrated perspective.
Distancing and experimentation
Two prominent CBT techniques are distancing and experimentation. Distancing involves stepping back and viewing automatic stereotypes as hypotheses to be tested, rather than self-evident truths. After failing an exam, a man may have an automatic thought that he “is a moron,” and most often, he will merely accept that thought as true (A. T. Beck & Alford, 2009). But distancing teaches him that, rather than accepting that thought de facto, he can distance himself from it and evaluate it as one among other hypotheses—for instance, that he is not a moron (see also the “Mindfulness-based training” section later in this article).
Distancing is often the precursor to experimentation, in which a Source tests the validity of his or her stereotype. With guidance, he or she designs and conducts an “experiment” to test competing hypotheses (e.g., “I can’t do anything right,” “I can do some things right”). Because the stereotypes are usually overgeneralizations, the results of the “experiment” generally counter the stereotype and support a more balanced perspective. Also, enacting experimentation behaviors without explicitly testing hypotheses produces comparable cognitive change (see Jacobson et al., 1996).
An intervention could use distancing to teach Prejudice Perpetrators to view their negative stereotypes (e.g., “Old people are dumb”) as hypotheses to be tested, rather than self-evident truths. Experimentation then tests that hypothesis, for instance, by meeting a group of old people and evaluating how many of them are smart or dumb. Presumably, the abundance of smart senior citizens will support the “Not all old people are dumb” hypothesis, thus countering the stereotype. Experimentation may be one method of instantiating the contact hypothesis, which proposes that, under the right conditions, increasing contact between groups could dispel group stereotypes (Allport, 1954).
Thought records
Closely related to the techniques above is the dysfunctional thought record (J. S. Beck, 2011; Greenberger & Padesky, 1995). When people experience an unwanted thought or emotion, they write down each component of the cognitive model for that situation (the activating event, the automatic stereotypic thoughts, and the consequential emotions and behaviors). They then evaluate the evidence for and against the activated stereotype, generate alternative hypotheses, and examine the real implications if the stereotype were true. In the end, the goal is to choose the most accurate and adaptive perspective on the situation, which is typically a new, balanced cognition. People interested in reducing their Prejudice Perpetration can work with a thought record to keep track of their automatic stereotypic thoughts (e.g., “Jews are greedy”), then generate examples that support and refute the stereotype in a methodical, scientific way.
Mindfulness-based training
Closely related to distancing, mindfulness has begun to infiltrate the CBT armamentarium (e.g., Dimidjian, Kleiber, & Segal, 2010; Leahy, 2010; Segal, Teasdale, & Williams, 2004). According to Bishop et al. (2004), “In a state of mindfulness, thoughts and feelings are observed as events in the mind, without over-identifying with them and without reacting to them in an automatic, habitual pattern of reactivity . . . Thus, mindfulness is thought to enable one to respond to situations more reflectively (as opposed to reflexively)” (p. 232). This corresponds to the distinction between automatic stereotypes and explicit beliefs in the prejudice literature—automatic stereotype activation does not imply an explicit belief or intuition about reality (see Devine, 1989). Rather than assuming automatically activated stereotypes are true or have meaning or relevance, people can learn that sometimes a stereotype is just activated, and they can let it pass without reacting to it or acting on it (see Segal, Williams, & Teasdale, 2002; Segal, Teasdale, & Williams, 2004).
Countering overgeneralized attributions
Sources often make attributions about Targets that are global, stable, and internal (e.g., “All Mexicans are completely lazy and always will be,” “I am completely worthless and always will be”). To fight stereotyping, it is crucial to change these overgeneralizations to more specific, unstable, concrete thoughts (e.g., “One Mexican didn’t complete his work one day,” “I made a mistake the other day”). In CBT, attenuating global attributions reduces dysphoria and rumination in mild-to-moderately depressed people (e.g., A. T. Beck, Rush, Shaw, & Emery, 1979; Watkins, Baeyens, & Read, 2009), and the same techniques should help reduce other-stereotyping and prejudicial behaviors and emotions in Prejudice Perpetrators. Similarly, situational attribution training also reduces generalizations by encouraging situational, rather than dispositional, attributions about Targets (Stewart, Latu, Kawakami, & Myers, 2010).
Prevention
“One does not get rid of mass plagues afflicting humankind, including the plague of mental and emotional disorders, by attempts at treating the individual,” (Albee, 1985). As this quotation implies, wide-scale prevention efforts are necessary to eliminate “mass plagues.” To this end, depression researchers have begun to use CBT programs to successfully prevent depression, even in people at high risk for it (e.g., Clarke et al., 2001; Garber et al., 2009; see also Horowitz, Garber, Ciesla, Young, & Mufson, 2007).
New CBT-based stereotyping prevention programs could help children identify and correct budding negative stereotypes about Others and about the Self, thus short-circuiting the development of pernicious stereotypes. Teaching children to understand and overcome automatic stereotyping may preempt both Beckian Depression and Prejudice Perpetration (see Hertel & Mathews, 2011; see also Cogan, 1996). Also, such prevention programs may arm Observers to recognize others’ stereotyping, then intervene against it. For instance, Lamb, Bigler, Liben, and Green (2009) developed a successful intervention that taught children aged 5–10 years to challenge sexist remarks from Others. Challenging an Other’s self-stereotyping and self-prejudice would be an exciting extension of this work.
Further, recall the integrated perspective’s notion that Prejudice Perpetrators become Beckian Depressives when their preexisting stereotypes become self-relevant. Preventing formation of negative stereotypes about groups (e.g., “obese people are lazy”) among children will decrease their risk for future depression when some inevitably become members of such groups (e.g., become obese themselves). In sum, by affecting stereotypes and mental habits early, we can help future generations with their own mental health and their treatment of others.
Cognitive depletion: An unintended consequence of effortful armaments
Unsurprisingly, effortful/controlled techniques like CBT require a considerable amount of effortful, controlled mental processing. Extended mental effort, however, can lead to cognitive depletion (i.e., ego depletion, self-control depletion, cognitive control depletion, willpower depletion), which refers to the idea that people have a limited capacity for effortful processing, like a reservoir that can be emptied from overuse. Someone can become depleted in a variety of ways: stress, rumination, lack of blood sugar, completing difficult cognitive tasks, stigma (i.e., being a Target), or actively trying to regulate bias (Beevers, 2005; Gailliot, Baumeister, et al., 2007; Gailliot, Plant, Butz, & Baumeister, 2007; Inzlicht et al., 2006; Macrae, Bodenhausen, Milne, & Jetten, 1994). One might say that depression is synonymous with depletion—many common symptoms of depression (e.g., fatigue, low energy) resemble cognitive depletion, and A. T. Beck and Alford (2009) noted that some writers have characterized depression as a “depletion syndrome.”
When people are cognitively depleted, their stereotypes exert more power on their emotions and behavior, as in the stereotype rebound effect. After trying to suppress stereotypic thoughts, people are depleted and ironically stereotype more in subsequent tasks (Macrae et al., 1994; Monteith, Spicer, & Tooman, 1998; see also Abramowitz, Tolin, & Street, 2001; Wenzlaff & Wegner, 2000; Wenzlaff et al., 1988). Psychologists already note the importance of restructuring, rather than suppressing, unwanted thoughts (e.g., J. S. Beck, 2011; Wenzlaff & Wegner, 2000). Nevertheless, effortful regulatory processes like CBT may be depleting and may cause an ironic rebound in stereotyping over the short term. In fact, the stereotype rebound effect may explain “sticking points”—when people have difficulty progressing with effortful stereotype change methods like CBT.
Counteracting depletion
There are a number of simple ways to counteract rebound effects and refill the cognitive control reservoir. No biologist would be surprised that glucose has been implicated as one source of fuel that powers cognitive control, and consumption of a glucose drink can reduce depletion-related impairments (Baumeister & Tierney, 2011; Gailliot, Baumeister, et al., 2007). After the glucose is metabolized, however, people often experience a “sugar crash” and feel worse than they did before—consideration of glucose should occur within a wider framework of examining diet and cognitive function.
Aside from diet, manipulating lay theories about cognitive control can help reduce depletion psychologically. In four studies, Job, Dweck, and Walton (2010) demonstrated that depletion is moderated by lay theories about cognitive control. Rather than being a biological or psychological imperative, depletion partly depends on whether people believe their capacity for cognitive control is a limited resource. When people believe their cognitive control reservoirs have a never-ending water supply (on their own or following an experimental manipulation), they experience less cognitive depletion (Job et al., 2010). Perhaps this lay theory is a core cognition that psychologists should address as a precursor to effortful stereotype change techniques.
The automatic, nonintentional armamentarium against stereotyping
Intentional, effortful processing may be essential for changing stereotypes in the long term (Barber & DeRubeis, 1989; J. S. Beck, 2011; A. T. Beck & Alford, 2009; Devine, 1989; Devine & Monteith, 1993; S. R. Levy, 1999). But, psychologists have also amassed a vast arsenal of techniques that can reduce bias without conscious effort or intention, at least in the short term (e.g., Araya et al., 2002; Olson & Fazio, 2006; Shalev & Bargh, 2011; for reviews, see Blair, 2002; Devine et al., 2012; Hertel & Mathews, 2011; Paluck & Green, 2009). This work may be especially useful for people whose depletion may decrease or even preclude their ability to engage in effortful stereotype reduction techniques like CBT: for example, depressed people. In fact, depressed people have difficulty with tasks requiring effortful information processing, but they perform normally on automatic tasks (Austin, Mitchell, & Goodwin, 2001; Hartlage, Alloy, Vázquez, & Dykman, 1993; Hasher & Zacks, 1979; W. R. Miller, 1975). Further, nonintentional techniques may be fitting for Sources who are unmotivated to change their stereotypes. Many such techniques have been shown to reduce bias in the short-term, and translating those reductions to long-term change is an exciting empirical opportunity (see Devine et al., 2012).
Priming
Memories, goals, or concepts can be primed consciously or subliminally and can have large effects on cognition, emotion, and behavior. Priming control-related words, for example, increases self-control and reduces bias expressed toward a Target (Araya et al., 2002). Implicitly priming positive stereotypic traits about old age (e.g., wisdom) improves memory performance in older people, whereas priming with negative stereotypic traits (e.g., senility) worsens memory performance (B. Levy, 1996). Finding ways to prime people with concepts, memories, exemplars, or goals that refute their stereotypes may noneffortfully reduce their stereotyping (e.g., Dasgupta & Greenwald, 2001; see Shalev & Bargh, 2011).
In a racial bias task, Wittenbrink, Judd, and Park (2001) primed people with one of two environmental contexts: either a “ghetto” building or a church. When primed with the ghetto building, people displayed the typical racial bias pattern found without a context prime, but the church attenuated the race bias. If a Beckian Depressive self-stereotypes herself as incompetent, a therapist can find ways to prime her with specific situations in which she had been competent in the past (which are sometimes difficult for her to recall). Perhaps the therapist will advise this Beckian Depressive to put up pictures of a former job or hobby that made her feel competent or assign her a computerized priming task as part of her therapy homework. Making memories of her competence more salient should reduce her self-stereotype of incompetence.
Such techniques should be tailored to the particular situation and applied thoughtfully. For example, the priming of positive attributes that a Beckian Depressive thinks are unattainable can increase dysphoria (e.g., Higgins, Bond, Klein, & Strauman, 1986), and the implication that Targets have only positive traits makes Prejudice Perpetrator interventions fail (Brauer, Er-rafiy, Kawakami, & Phills, 2012). When executed properly, however, many different priming techniques can change stereotypes using less effort than controlled thought monitoring and replacement.
Implicit learning
Whereas priming makes existing cognitive structures more salient, other implicit techniques can break down existing associations or build new ones. Implicit learning occurs without intention and often without awareness (Reber, 1967, 1969; for a review, see Goschke, 1997). This nonintentional learning may be a strong contributor to the development of stereotypes, and it can be adapted to change stereotypes as well.
Implicit learning can change someone’s stereotypic bias without the Source’s intention to do so (e.g., Olson & Fazio, 2006; Plant, Peruche, & Butz, 2005; for a review see Hertel & Mathews, 2011). Plant and colleagues’ (2005) implicit learning paradigm, for example, was able to break down stereotypic associations between race and criminality. People responded to a pattern of stimuli in which race cues and criminality cues were uncorrelated, which reduced automatic racial bias in shooting decisions. This training altered people’s automatically activated stereotypes up to at least 24 hr later, and its effects generalized to the activation of other racial stereotypes. Whereas Plant and colleague’s paradigm weakened existing negative stereotypes, Olson and Fazio (2006) developed a paradigm that built new positive associations. Using pictures and pleasant words, this paradigm harnessed the basic principles of classic conditioning to implicitly build positive associations with the Black racial group. People were unaware of the conditioning pattern during the task, but they displayed less automatic race bias immediately after the task and 2 days later.
Implicit learning paradigms can be adapted to change a variety of other- or self-stereotypes. Using pictures of a Beckian Depressive and negative or positive associates, for instance, a therapist could devise a program that builds self–positivity associations and breaks down self–negativity associations. Implicit learning is a powerful component in the development of stereotypes, and psychologists can wield it as a powerful weapon against those same stereotypes.
Embodiment
Cognitions, emotions, and perceptions relate closely to the body (for a review, see Niedenthal, Barsalou, Winkielman, Krauth-Gruber, & Ric, 2005). Indeed, A. T. Beck and Alford (2009) argued that depression is more than “just” a mood or affective disorder—it is a disorder deeply connected to the body. Likewise, prejudice is closely tied to avoidance, and, accordingly, approach behaviors can reduce stereotyping and prejudice. In one paradigm, for example, people pull a computer joystick closer to their bodies when they see pictures of Black people. This approach behavior reduces implicit race bias without intention or awareness, and it improves subsequent interracial interactions (Kawakami, Phills, Steele, & Dovidio, 2007). In another paradigm, people hold a pen in their teeth, which (unbeknownst to them) induces a smile when they view pictures of Black men, reducing their implicit race bias (Ito, Chiao, Devine, Lorig, & Cacioppo, 2006). Actions as simple as pushing down or up on a desk and nodding the head “yes” or shaking it “no” can alter attitudes about Targets (Cacioppo, Priester, & Berntson, 1993; Wells & Petty, 1980). Embodiment is not a panacea for stereotyping, but these techniques (and many others) can help “chip away” at negativity, both in the social arena and in the clinic. Sometimes the body is the door to the mind.
Perceived variability
A key feature of stereotyping is low perceived variability (i.e., low representational complexity, high homogeneity/low heterogeneity) of Targets (see also the “countering overgeneralized attributions” section). In fact, some theorists assert that stereotyping and low perceived variability are virtually interchangeable constructs (Brauer & Er-rafiy, 2011; Linville, 1998; Richards & Hewstone, 2001). Accordingly, experimentally increasing the perceived variability of a Target reduces Prejudice Perpetration toward that Target (e.g., Brauer & Er-rafiy, 2011; Brauer et al., 2012; Er-rafiy, Brauer, & Musca, 2010; Ryan, Judd, & Park, 1996). Greater perceived variability of the Self correlates with less extreme self-directed affect and may produce some invulnerability to depression (Linville, 1985, 1987). Manipulating a Target’s perceived variability has not yet been extensively explored outside of the Prejudice Perpetrator context, but researchers have manipulated the perceived variability of the Self (see Margolin & Niedenthal, 2000). Increasing the variability of Sources’ perceptions of Targets reduces stereotyping and prejudice and may be a fundamental step in fighting stereotyping in the clinical and social realms.
Researchers have increased perceived variability of Targets in a number of ways. For example, displaying a poster that emphasizes a mixture of positive and negative traits about a social group reduces prejudice and discrimination toward members of that group at least 2 weeks later (Brauer et al., 2012; Er-rafiy et al., 2010). Translating this method to a clinical context, a therapist could work with a Beckian Depressive to create a collage of positive and negative traits they possess, similar to the posters used by Brauer, Er-rafiy, and colleagues. When a Target is seen as complex (as opposed to homogenous), positive and negative characteristics can coexist and complement, rather than contradict and dominate. Translating perceived variability interventions for Prejudice Perpetration into interventions for Beckian Depression promises to be fruitful.
Conclusion
By widening the lens through which we view prejudice and depression, the integrated perspective on prejudice and depression reveals fundamental connections that are not evident with a narrower lens. Breaking down arbitrary semantic barriers, we define stereotype as a link between two human concepts, about a group or a person, in the mind of a group or a person. Stereotypes are often oversimplified, overgeneralized, and fixed. The integrated perspective allows us to examine the sequelae of stereotyping from a unified viewpoint, in domains as diverse as concentration camps in Eastern Europe during the Holocaust to depression clinics in the United States today.
A Source’s prejudice causes a Target’s depression. Comorbid depression and prejudice—deprejudice—can take many forms. In a Beckian Depressive, when both the Source and Target of stereotyping are the Self, we can see deprejudice within a single person. The integrated perspective may be very useful in interpersonal contexts, such as couples therapy. Understanding that an abusive wife (the Prejudice Perpetrator) has negative stereotypes about and prejudice against her husband (the Prejudice Victim) that cause his depression may improve treatment outcomes for the couple’s deprejudice (see also A. T. Beck, 1988). Looking at Prejudice Perpetrators and Prejudice Victims allows examination of deprejudice between multiple people in a wider societal context.
The deprejudice quadruplex also provides insight into stereotype acquisition, whether it involves an Observer learning or modeling stereotypes or a Prejudice Victim internalizing them. Also, a Prejudice Perpetrator’s preexisting stereotypes can become self-relevant. A powerful contribution of the integrated perspective is its facilitation of cross-disciplinary applications. Because prejudice and stereotyping are everyday terms that connote something to be overcome, using the integrated perspective’s terminology with Beckian Depressive clients may improve their therapy outcomes (A.T. Beck, personal communication, July 14, 2010). Also, depression researchers and prejudice researchers can be powerful allies. Each camp has much to gain from raiding the armory the other has amassed in the war against stereotyping.
There are other potentially interesting outgrowths of our definition of stereotype. A stereotyping perspective may illuminate other disorders involving negative stereotypes (e.g., anxiety) and their treatments. Further, the discussion herein has focused largely on negative stereotypes, but as we mentioned earlier, positive stereotypes also can be highly problematic. Positive self-stereotypes may contribute to other disorders, like narcissism. Other functions of stereotyping, such as derogating others to increase self-esteem, may be interesting to explore within the integrated perspective (e.g., Fein & Spencer, 1997; see also scapegoating, e.g., Katz, Glass, & Cohen, 1992).
Reducing stereotyping at the personal and societal level is more than a moral and ethical imperative—it is a health imperative as well. Those studying depression and prejudice have pursued discrete lines of research, unaware of many parallels between their literatures and unaware that they have been working long and hard to fight a common enemy—stereotyping. The integrated perspective builds a bridge so that researchers can raid one another’s arsenals and thereby pack a greater punch against these personal and societal ills. We hope that by blurring some lines, our model creates a clearer picture.
Footnotes
Acknowledgements
We thank Janet Hyde for her enthusiasm for and comments on these ideas throughout their gestation. We thank her and Paula Niedenthal for their comments on a previous version of this article and Judy Harackiewicz for teaching us about the jingle and jangle fallacies. We also thank Carlie Allison, Abigail Bitter, Ben Dykman, Amanda Eggen, Patrick Forscher, Matt Huston, Tharchin Jairamdas, Molly Maier, Kristen Merkitch, Gary Naud, Matt Phillippi, Magdalena Rychlowska, Rachel Salk, Dominika Swistun, Gino Tassara, and Nicole Velez for their contributions to this article.
Declaration of Conflicting Interests
The authors declared that they had no conflicts of interest with respect to their authorship or the publication of this article.