
Abstract
Belief updating is a relatively nascent field of research that examines how people adjust their beliefs in light of new evidence. So far, belief updating has been investigated in partly unrelated lines of research from different psychological disciplines. In this article, we aim to integrate these disparate lines of research. After presenting some prominent theoretical frameworks and experimental designs that have been used for the study of belief updating, we review how healthy people and people with mental disorders update their beliefs after receiving new information that supports or challenges their views. Available evidence suggests that both healthy people and people with particular mental disorders are prone to certain biases when updating their beliefs, although the nature of the respective biases varies considerably and depends on several factors. Anomalies in belief updating are discussed in terms of both new insights into the psychopathology of various mental disorders and societal implications, such as irreconcilable political and societal controversies due to the failure to take information into account that disconfirms one’s own view. We conclude by proposing a novel integrative model of belief updating and derive directions for future research.
Current political controversies in the West, as reflected in the debate over Brexit in England or discussions about the possible misconduct of President Donald Trump in the United States, reveal that conflicting parties seem to have diverging perspectives on such controversies and do not take into account information that contradicts their views, resulting in fairly divisive and irreconcilable controversies. We believe that much of this dilemma relates to how people construe their subjective reality and deal with information that disconfirms it. Specifically, people hold certain beliefs (which they usually assume to be true) that they use as a heuristic to evaluate new information. As a result, new information can be rejected if it does not match people’s prior beliefs. On the other hand, if new information is consistent with people’s prior beliefs, it is more likely to be integrated. The research area concerned with these problems is the relatively nascent field of belief updating. This article aims to provide a comprehensive review of several lines of research in this field and discusses implications that can be drawn from it. In particular, after presenting some prominent frameworks and experimental paradigms for the investigation of belief updating, we review what is known about the characteristics of belief updating in healthy people and in people with various mental disorders. We then aim to synthesize previous research in an integrative model of belief updating and discuss its implications in regard to both new insights into the psychopathology of mental disorders and societal issues. We conclude by critically evaluating the strengths and shortcomings of past research on belief updating and provide some suggestions for future work.
The Importance of Beliefs in Human Life
How beliefs modulate perception and well-being
It is becoming increasingly evident that people’s beliefs 1 significantly modulate their perception of—and response to—the world, affecting various aspects of life from decision-making to well-being. Evidence for this claim has been provided, for instance, by research into “motivated perception” (Lench, Smallman, Darbor, & Bench, 2014; Voss & Schwieren, 2015). For example, in a well-designed series of five experimental studies that included both explicit and implicit measures of perception, Balcetis and Dunning (2006) found that people’s perception of ambiguous visual stimuli was guided by top-down beliefs, meaning that they had the propensity to perceive a representation of the visual environment that was consistent with their desires. Further substantiating these findings, Leong, Hughes, Wang, and Zaki (2019) investigated the neurocomputational mechanisms of such motivated perception. Using a rewarded visual-categorization task, the authors found that top-down beliefs about expected reward biased perceptual judgments in that ambiguous images were more often labeled as corresponding to a reward-associated category. Beyond perception, performance has also been shown to be affected by beliefs, as demonstrated by research indicating enhanced cognitive abilities such as memory and creativity after sham, placebo-like treatment (Parker, Garry, Einstein, & McDaniel, 2011; Rozenkrantz et al., 2017; Weger & Loughnan, 2013).
Empirical support for the role of beliefs in well-being comes from several studies linking large-scale national health surveys with databases of well-being measures. These studies suggest that holding negative beliefs about aging in young adulthood is associated with up to a threefold higher likelihood of experiencing cardiovascular events 38 years later (Levy, Zonderman, Slade, & Ferrucci, 2009). Further, individuals reporting high levels of stress had a 43% increased risk of premature death, but only if they perceived stress as having a significant impact on health (Keller et al., 2012). In addition, individuals who perceived themselves as less physically active than others had up to a 71% higher mortality risk compared with individuals who believed they were more active than others, even after controlling for actual levels of activity (Zahrt & Crum, 2017). Likewise, Laferton, Fischer, Ebert, Stenzel, & Zimmermann (2020) found that individuals who hold negative beliefs about stress (e.g., believing that stress is uncontrollable) report more negative affect in relation to daily stress.
In addition to this mostly cross-sectional or longitudinal research, Crum, Salovey, and Achor (2013) provided more causal evidence for the influence of beliefs on the stress response. In a series of experimental studies, the authors manipulated the way participants thought about stress. Specifically, they established a “stress is debilitating” mind-set (suggesting detrimental effects of stress on health, performance, and learning/growth) in contrast to a “stress is enhancing” mind-set (suggesting beneficial effects of stress) and found that the latter was related to more adaptive cortisol profiles under acute stress. This implies that beliefs about stress significantly contribute to how people actually respond to acute stress (Crum et al., 2013). Building on this finding, another study demonstrated that a brief psychological intervention aimed at optimizing participants’ beliefs about stress (i.e., enhancing participants’ personal-control expectations) led to lower cortisol levels after acute stress than a gratitude intervention; however, the specificity of this effect was somewhat limited, given that a distraction task also lowered participants’ cortisol levels (Salzmann et al., 2018).
Other interesting insights into the link between beliefs and health have been provided by placebo research, in which expectations for symptom improvement have been found to contribute significantly to clinical outcomes after an inert treatment (i.e., placebo; for reviews, see, e.g., Petrie and Rief, 2019; Schedlowski, Enck, Rief, and Bingel, 2015). Pointing to a causal effect of participants’ expectations, some studies have found that manipulating participants’ treatment expectations experimentally (e.g., expecting to receive an analgesic drug vs. placebo) substantially influenced pain perception (Lund, Vase, Petersen, Jensen, & Finnerup, 2014; Schenk, Sprenger, Geuter, & Büchel, 2014). Intriguingly, another study demonstrated that positive treatment expectations boosted the analgesic effects of an opioid agonist, whereas negative treatment expectations diminished its analgesic effects (Bingel et al., 2011). Furthermore, neuroimaging studies have found that expectations modulate treatment-relevant neuronal processes even before treatment, and these modulations mediate treatment outcomes (Wager et al., 2004; Zilcha-Mano et al., 2019). Expanding our knowledge about the effects of expectations on pain perception, two neuroimaging studies revealed how the expectation of pain relief influenced the perception of pain at the neurobiological level: It was found that higher order brain regions acted on lower order brain regions to suppress the coding of the dissonance between expectation and perception (Jepma, Koban, van Doorn, Jones, & Wager, 2018; Schenk, Sprenger, Onat, Colloca, & Büchel, 2017). In other words, the brain matches its perception to its expectations, much like a self-fulfilling prophecy. Collectively, these findings highlight how human information processing, from sensory perception to decision-making, is significantly shaped by people’s beliefs. However, it should be noted that some of the research cited above used cross-sectional or longitudinal data, limiting the conclusions that can be drawn with respect to causality.
When beliefs make people vulnerable
The importance of beliefs is further emphasized by studies using clinical samples, indicating vulnerabilities in relation to dysfunctional 2 beliefs. For instance, research from behavioral medicine has shown that dysfunctional beliefs of patients about their illness can have adverse effects on symptom development and treatment success. In patients with coronary heart disease, for example, negative beliefs about the controllability and consequences of the disease predict worse symptom recovery from myocardial infarction (Petrie, Weinman, Sharpe, & Buckley, 1996) and reduced benefit from cardiac surgery (Juergens, Seekatz, Moosdorf, Petrie, & Rief, 2010; Kube, Meyer, et al., 2020). Even long-term mortality has been found to be increased for patients with dysfunctional illness perceptions (Barefoot et al., 2011). Similar results have been provided for patients with chronic obstructive pulmonary disease (Zoeckler, Kenn, Kuehl, Stenzel, & Rief, 2014), breast cancer (Nestoriuc et al., 2016), diabetes (Griva, Myers, & Newman, 2000; Mann, Ponieman, Leventhal, & Halm, 2009), and chronic pain (Cormier, Lavigne, Choinière, & Rainville, 2016). Beyond this mostly longitudinal research, other studies have used experimental designs to examine the influence of patients’ beliefs on the course of symptoms in a more causal manner. For example, two studies found that interventions aimed at modifying illness beliefs of people who had experienced a myocardial infarction were related to a faster rate of return to work than standard medical care (Broadbent, Ellis, Thomas, Gamble, & Petrie, 2009; Petrie, Cameron, Ellis, Buick, & Weinman, 2002). In line with these results are results from another study that showed that the optimization of preoperative expectations in patients undergoing coronary heart surgery led to less illness-related disability 6 months after the surgery than standard medical care. Because this expectation-optimization intervention was also superior to an unspecific supportive psychological intervention in terms of reducing disability, this study suggests a specific effect of patients’ expectations on symptom improvement (Rief et al., 2017).
Dysfunctional beliefs are also regarded as core features of almost all mental disorders. In major depression, for instance, it has been shown that dysfunctional expectations about one’s own abilities and the personal future predict the course of depressive symptoms and suicidal ideation (Backenstrass et al., 2006; Czyz, Horwitz, & King, 2016; Horwitz, Berona, Czyz, Yeguez, & King, 2017; Strunk, Lopez, & DeRubeis, 2006). More specifically, it has been found that people with depression hold negative global beliefs that elicit dysfunctional situation-specific expectations that then lead to the experience of depressive symptoms (Kube et al., 2018). In posttraumatic stress disorder (PTSD), dysfunctional beliefs in relation to the traumatic experience are assumed to be a core factor that contributes to the development and maintenance of the disorder (Ehlers & Clark, 2000). For instance, Murray (2018) showed that beliefs about being guilty after the survival of a traumatic event is very common among PTSD patients and is associated with higher PTSD symptom severity. Further evidence for the contribution of dysfunctional beliefs to the development and maintenance of mental health problems has been provided for social anxiety (D. M. Clark & Wells, 1995; Rapee & Heimberg, 1997), hypochondriasis (Barsky et al., 2001; Barsky, Coeytaux, Sarnie, & Cleary, 1993), obsessive-compulsive disorders (Hansmeier, Exner, Rief, & Glombiewski, 2016; Salkovskis et al., 2000; Shafran, Thordarson, & Rachman, 1996), eating disorders (Corstorphine, 2006; Konstantakopoulos et al., 2012; Waller, Dickson, & Ohanian, 2002), and schizophrenia (Lincoln, Mehl, et al., 2010; Moritz et al., 2010).
The evidence summarized in this brief introduction suggests that beliefs can influence the way people perceive the world and respond to it; further, in the case of dysfunctional beliefs, beliefs can make people vulnerable and can be associated with mental health problems. However, because of the limited number of experimental studies differentially manipulating beliefs, conclusions about a causal role of beliefs (e.g., with respect to the question of whether dysfunctional beliefs constitute a risk factor for mental disorders) need to be drawn with caution.
Belief Updating: The Integration of New Information Into Existing Beliefs
It should be kept in mind that people’s beliefs do not reflect the world as it actually is but rather their construction of it. In other words, beliefs construe a template through which people perceive themselves, other people, and the world in general. With this template in mind, beliefs are permanently tested against the background of new information and experiences. As illustrated in Figure 1, new information can either confirm or disconfirm prior beliefs, each resulting in different effects of the new information on previous beliefs. Anomalies in belief updating in light of new information, as found in some clinical populations, is an important part of this article.
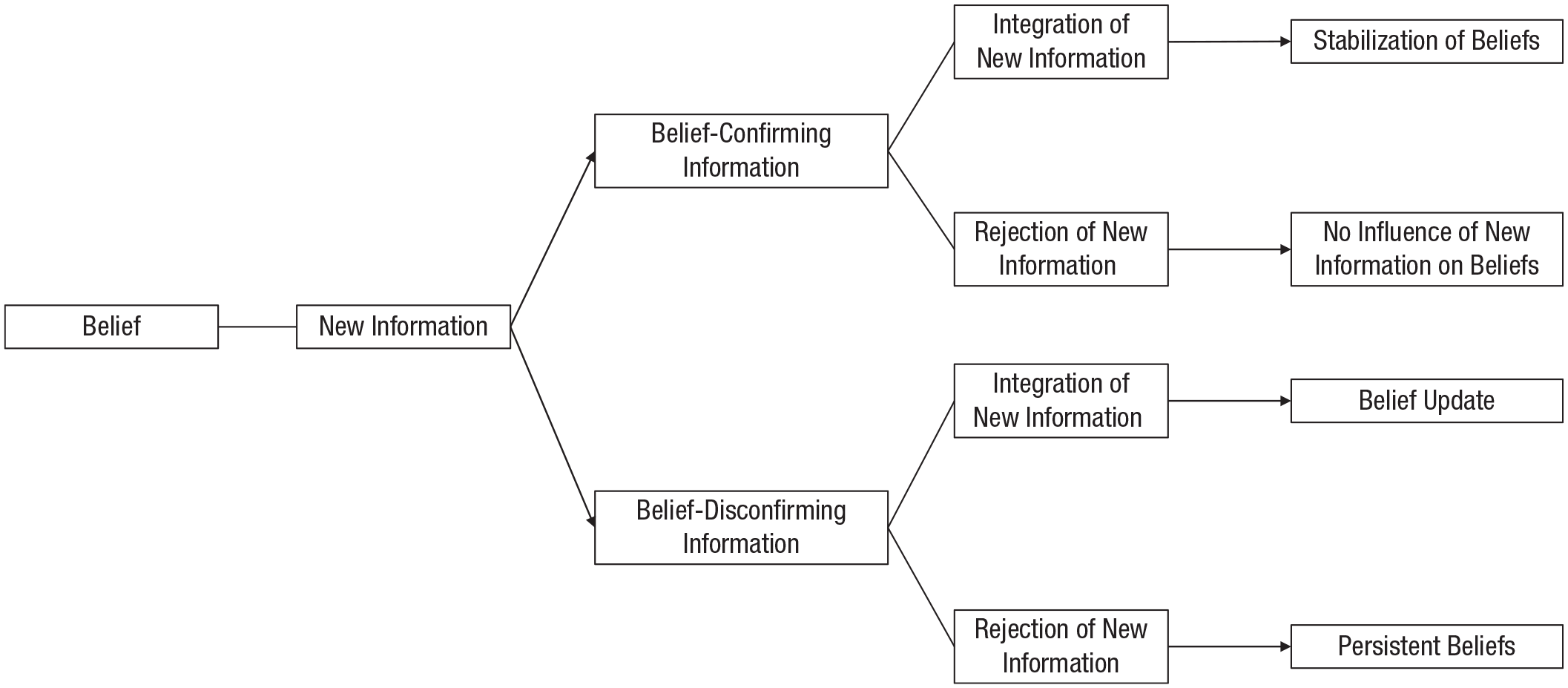
Schematic illustration of how new information can be integrated into existing beliefs.
The basic design of research studies in the field of belief updating includes a first assessment of participants’ beliefs before they receive new information (that can support or challenge their prior beliefs), followed by a second assessment of beliefs. Thus, this basic design enables researchers to examine the extent to which beliefs are updated after receiving new information. Researchers using this study design are often interested in relating specific patterns of belief updating to different psychological processes, such as anticipatory reactions, encoding or interpreting new information, and further processing or appraising new information. As illustrated in Figure 2, at each of these stages of information processing, experimental manipulations can be performed if researchers are interested in the influence of a particular psychological process on belief updating. As discussed later in this article, distortions in these psychological processes may lead to anomalies in belief updating, such as the persistent lack of belief updating or hasty changes in beliefs.
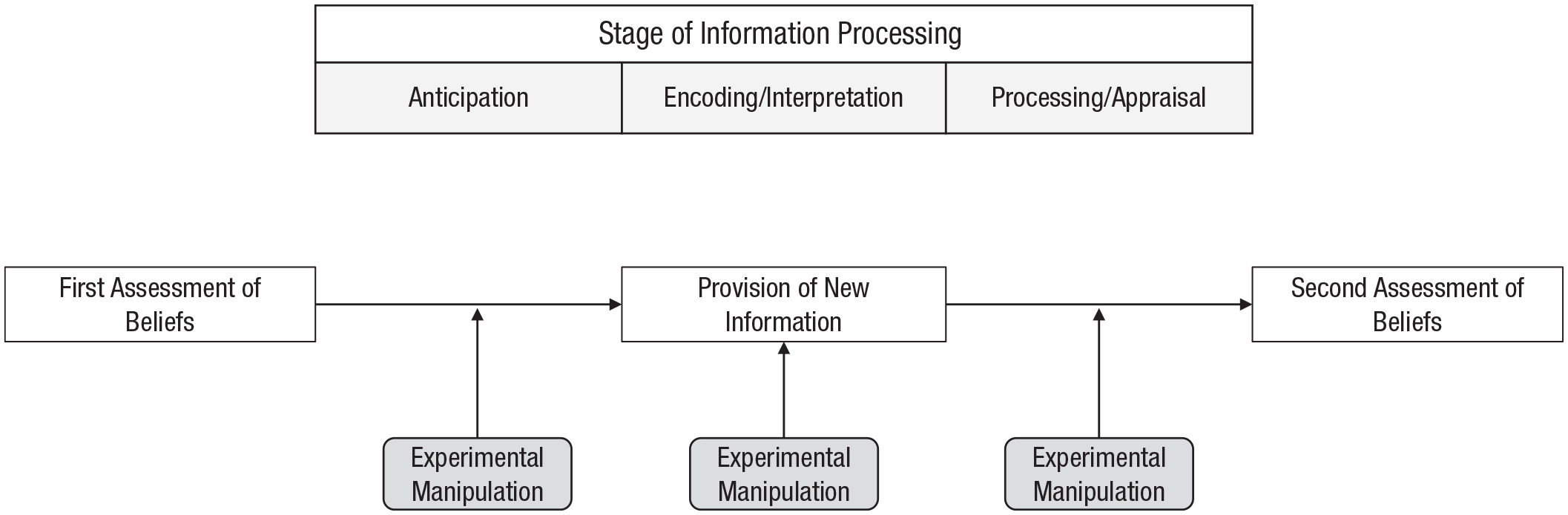
Illustration of the basic experimental paradigm for investigating belief updating. To examine particular patterns of belief updating, researchers use experimental manipulations that target different stages of information processing, such as anticipation, encoding, and further processing.
Before we discuss such abnormalities in comparison to belief updating in healthy people, we first introduce a powerful current theory of cognition and the brain, referred to as predictive processing, that has become increasingly important in the field of belief updating.
A prominent framework in the study of belief updating: predictive processing
The roots of the predictive-processing framework (PPF) go back to von Helmholtz (1867), who introduced the concept of unconscious inference, assuming that the human brain fills in visual information to make sense of a visual scene. In recent years, predictive processing has become a dominating theoretical framework in neuroscience and related areas interested in operating principles of the brain. One basic assumption of the PPF is that perception is inextricably linked to prediction, meaning that prior predictions bias perception, which in turn shapes posterior predictions. In particular, researchers using the PPF assume that the brain does not “passively” process incoming sensory signals; instead, it permanently generates predictions about expected sensory input that is then compared with prior predictions (A. Clark, 2013b; Huang & Rao, 2011; O’Reilly, Jbabdi, & Behrens, 2012). Any mismatches between prior predictions and actual sensory signals are referred to as prediction errors. Prediction errors normally provide corrective feedback and are used to update future predictions (referred to as belief updating). Appealing to the free-energy principle (Friston & Kiebel, 2009; Moran et al., 2013), neuroscientists suggest that the brain aims to adjust predictions such that prediction errors are minimized and incoming sensory information is optimally used (Barrett & Simmons, 2015). With active inference, people can also fulfill their predictions by acting on the world in such a way that prediction errors are minimized (Friston et al., 2015; Pezzulo, Rigoli, & Friston, 2015; Seth & Friston, 2016).
Precision plays a crucial role in active inference. As with all forms of Bayesian inference, the precision of various sources of sensory evidence—or indeed prior beliefs—can have a profound effect on belief updating (Ernst & Banks, 2002). These effects will become prescient later when we consider aberrant precision and the false inferences that accompany psychopathology. Simple examples here include inferring that something is there when it is not (i.e., hallucinations) or that something is not there when it is (i.e., agnosia). Technically, the key determinant of the rate of belief updating or evidence accumulation is the precision afforded to prior beliefs relative to sensory evidence (i.e., sensory prediction errors). In other words, a weakening of prior precision corresponds to a relative increase (or failure to attenuate) sensory precision and vice versa. To keep things simple, we describe this imbalance of precision in terms of prior precision (Pellicano & Burr, 2012). Psychologically, getting the right balance between prior and sensory precision has been associated with attention, such that attending to a particular source of sensory evidence enhances the corresponding precision of prediction errors and the accompanying rate of belief updating (Feldman & Friston, 2010; Kanai, Komura, Shipp, & Friston, 2015; Parr & Friston, 2019; Vossel, Mathys, Stephan, & Friston, 2015). From a neurobiological perspective, this is thought to be encoded by the excitability or postsynaptic gain of neuronal populations—superficial pyramidal cells—encoding prediction error. This aspect becomes important later when we discuss the pathophysiology of conditions such as schizophrenia and Parkinson’s disease, which usually involve an abnormality of neuromodulatory transmitter systems (e.g., dopamine). In short, a pathophysiology of neuromodulation may translate into a failure of belief updating as a result of aberrant precision control (A. Clark, 2013a; Haarsma et al., 2018; C. E. Palmer, Auksztulewicz, Ondobaka, & Kilner, 2019; C. J. Palmer, Seth, & Hohwy, 2015; Rae, Critchley, & Seth, 2019; Van de Cruys et al., 2014; Vuust, Dietz, Witek, & Kringelbach, 2018).
The PPF was originally developed in neuroscience and provided a new understanding of sensory processing and, more recently, infant learning (Köster, Kayhan, Langeloh, & Hoehl, 2020). In recent years, several clinical applications of the PPF have been proposed, for example, for mental disorders such as depression (Barrett, Quigley, & Hamilton, 2016; J. E. Clark, Watson, & Friston, 2018; Kube, Schwarting, Rozenkrantz, Glombiewski, & Rief, 2020), PTSD (Kube, Berg, Kleim, & Herzog, 2020; Linson & Friston, 2019; Wilkinson, Dodgson, & Meares, 2017), and psychosis (Corlett et al., 2019; Sterzer et al., 2018); persistent physical symptoms (Edwards, Adams, Brown, Parees, & Friston, 2012; Henningsen et al., 2018; Kube, Rozenkrantz, Rief, & Barsky, 2020; Van den Bergh, Witthöft, Petersen, & Brown, 2017); pain perception (Wiech, 2016); and placebo analgesia (Büchel, Geuter, Sprenger, & Eippert, 2014; Grahl, Onat, & Büchel, 2018; Ongaro & Kaptchuk, 2019). We refer to some of these clinical applications of the PPF later in this article when discussing certain distortions related to belief updating in clinical populations.
Relation of predictive processing and belief updating
Note that, to our knowledge, there is no widely accepted agreement on how the PPF precisely relates to belief updating; therefore, we briefly point out how we treat the two frameworks in relation to each other. Within the PPF, there is the idea of a predictive hierarchy, assuming that (the contents of) predictions differ in respect to the level of abstraction. That is, there are predictions at lower levels of the hierarchy that are close to the explanation of sensory stimuli (such as “This is a face”), whereas predictions at higher levels of the hierarchy reflect a higher degree of abstraction (such as “I like this person”; Bastos et al., 2012; Pezzulo, 2014). Whereas the former are thought to be mostly unconscious, the latter might be more accessible to conscious experience and reflect what researchers from other fields (including ourselves throughout this article) refer to as beliefs. Notably, much of our discussion rests on beliefs that we take to be propositional in nature. On the other hand, we appeal to Bayesian belief updating as a formal point of reference. In this setting, Bayesian beliefs are not necessarily propositional and could correspond to subpersonal beliefs—of the sort described by von Helmholtz in his treatment of perception as unconscious inference. Technically, this means Bayesian beliefs are just posterior probability distributions that are updated through some form of belief propagation.
In this article, we thus refer to belief updating as an application of the PPF with respect to the updating of higher-level predictions after the receipt of new information. Sources of information can vary from factual information received from other people or the environment to exteroceptive sensory information and interoceptive sensations (i.e., information from the inner milieu of the body). Note that when we discuss anomalies in belief updating later in this article, we appeal to the PPF as one application of a Bayesian framework (as opposed to invoking any generic Bayesian framework). We do so because the PPF is one of the most elaborated and compelling adoptions that has substantially improved our understanding of the human mind, both with regard to basic science and clinical applications. Further, with reference to the free-energy principle and active inference, the PPF introduces specific principles that will help us understand why people’s beliefs in some instances become resistant to updating and learning from new experience. However, we recognize that the distinction between Bayesian frameworks for belief updating in general and the PPF in particular is a fine line.
Characteristics of Belief Updating in Healthy People
Building on the frameworks presented above for the investigation of belief updating, we next review the literature on the characteristics of belief updating in people who are in good mental health. We then focus on distortions in belief updating that have been observed in clinical populations. Notably, this review is not meant to be exhaustive; when we invoke findings from specific areas of research, our aim is not to review the respective body of literature systematically or to cover all scientific controversies therein. Rather, we compile evidence from different psychological disciplines to examine how it contributes to the knowledge about belief updating.
The optimism bias
One particularly striking example of how healthy people integrate new information into their existing beliefs is the optimism bias that Tali Sharot and colleagues have studied extensively. According to this concept, (healthy) people’s beliefs about the future are often unrealistically optimistic and remain so despite disconfirmatory evidence. Remarkably, to maintain optimistic beliefs about the future, people selectively embrace information that favors their optimistic view while discarding information that contradicts it. In other words, people display asymmetric learning from new information according to whether it confirms their existing (biased) beliefs (Lefebvre, Lebreton, Meyniel, Bourgeois-Gironde, & Palminteri, 2017; Sharot, 2011; Sharot & Garrett, 2016). This has been demonstrated in a series of experimental studies (Garrett & Sharot, 2017; Sharot, Guitart-Masip, Korn, Chowdhury, & Dolan, 2012; Sharot, Kanai, et al., 2012; Sharot, Korn, & Dolan, 2011; Sharot, Riccardi, Raio, & Phelps, 2007). In these studies, a trial-by-trial belief-updating design was used: That is, participants were asked to estimate their risk for several adverse life events and then were presented with the real probabilities of encountering these events (i.e., the correct estimation). When then asked to reestimate their risk, participants preferably used this new knowledge when favorable, but not unfavorable, probabilities were presented. For example, an initial estimation of a 30% risk for cancer might be updated to 22% after a base rate of 20% (favorable information; large update), but an initial estimation of a 10% risk might be updated to 13% after the same base rate (unfavorable information; smaller update; Sharot & Garrett, 2016). Notably, this “good news–bad news” effect has also been found in research from behavioral economics, indicating that people do not make decisions solely on the basis of rationality (Eil & Rao, 2011).
A series of neuroimaging studies (Kuzmanovic, Jefferson, & Vogeley, 2016; Sharot et al., 2011; Sharot, Kanai, et al., 2012) elucidated the neural mechanisms of the optimistic bias and showed that undesirable information is coded differently than desirable information, which is thought to underlie the relative neglect of the integration of the former. Thus, overly optimistic beliefs are further reinforced by a selective filter that generates a feedback loop that facilitates the persistence of biased beliefs. A further study found that this optimistic bias in belief updating diminishes when people are under perceived threat: Both in participants with experimentally induced stress and in firefighters on duty, Garrett, González-Garzón, Foulkes, Levita, and Sharot (2018) found that under perceived threat, healthy people are more sensitive to bad news and better integrate it into their beliefs than in the absence of threat. The authors interpreted their findings in light of psychological flexibility, meaning that healthy people can flexibly adjust their otherwise optimistic belief-updating bias when situational circumstances require it.
Cognitive consistency and confirmation bias
According to theories from cognitive and social psychology, people strive for cognitive consistency, meaning that they aim to reduce contradictions between different beliefs. One of the most influential theories in this context is the theory of cognitive dissonance (Festinger, 1962). This theory proposes that holding conflicting cognitions is perceived as being aversive, resulting in the preference to reduce this cognitive dissonance by cognitive or behavioral strategies. To apply this theory to the terminology of belief updating, consider the example of a healthy person holding the belief that, overall, the world is safe. If this person were confronted with disconfirming information, such as reported crimes in the news, a conflicting cognition such as “Some people endanger safety” might come up. Because this cognition contradicts the belief in a safe world, the person may aim to reduce cognitive dissonance, for example, by thinking, “These things only happen to others. My personal world is safe.”
Relatedly, other lines of research from cognitive psychology have also dealt with the phenomenon of confirmation bias, which means that people have the propensity to interpret information in such a way that their preexisting beliefs are confirmed (Nickerson, 1998; Oswald & Grosjean, 2004). According to this concept, people generally assume that their beliefs are true, which is why they use their preexisting beliefs as a heuristic to evaluate new information. Further, people tend to use positive test strategies, meaning that they prefer strategies that are likely to confirm prior beliefs when integrating novel information (Klayman & Ha, 1987).
Note that we have moved beyond perceptual processing and now consider the problem of active inference (i.e., how to optimize belief updating when people are in charge of gathering the sensory evidence on which to base their beliefs). Active inference takes the view that the best way to gather data is to resolve uncertainty in relation to prior beliefs. Implicit in this formulation is a Bayes-optimal optimism bias. In other words, if people are gathering evidence for their models of the world, they will naturally tend to select those data that provide confirmatory evidence (Bruineberg, Kiverstein, & Rietveld, 2018). Crucially, active inference does not just deal with selecting sources of sensory information (e.g., which news channels to watch). There can also be mental actions in terms of deploying precision or attention to various modalities or hierarchical levels of inference (Limanowski & Friston, 2018). In other words, positive test strategies can also be manifested in the things that people attend to—and the things that they ignore—without any overt action.
Self-concept stability
Another bias in belief updating among healthy people has been revealed in social and personality psychology. It is well established in this field that people’s beliefs about themselves remain remarkably stable over time. One aspect contributing to this self-concept stability is that people selectively search for information that confirms their self-concept. In other words, people are inclined to search for information that is consistent with their beliefs about themselves. This inclination has been demonstrated by studying participants’ desire to receive feedback from social-interaction partners about their appraisal of the participants; it was found that people had a strong preference to receive feedback that they believed would be consistent with their self-concept (e.g., regarding self-perceived assertiveness and self-perceived emotionality; Swann & Read, 1981a, 1981b). Conversely, when people receive new information that is inconsistent with their self-concept, they are likely to reject it, which further contributes to self-concept stability (Markus, 1977; Markus & Wurf, 1987; Swann & Hill, 1982). With regard to the latter, one study, for instance, has shown that participants’ expectations for their performance were highly influenced by their preexisting level of self-esteem but not by novel performance feedback received during the task (McFarlin & Blascovich, 1981).
In another study, Korn, Prehn, Park, Walter, and Heekeren (2012) demonstrated that the valence of self-relevant information also influences belief updating. The authors showed that people update their beliefs about themselves after receiving social feedback from peers more toward desirable information than toward undesirable information, suggesting that healthy people are positively biased when integrating social feedback into their beliefs about themselves. Thus, collectively, research on self-concept suggests that belief updating in healthy people is biased toward the integration of (positive) self-concept-congruent information, whereas self-concept-discrepant information is disregarded, thereby maintaining the person’s self-perception.
Truth decay and posttruth: persistence of political attitudes
Insightful examples of how people selectively use novel information to update their beliefs can also be found in the literature on political attitudes. Research in this area suggests that people stick to their attitudes and opinions regardless of disproving facts (Taber, Cann, & Kucsova, 2009; Tappin, van der Leer, & McKay, 2017). This has been referred to as a truth decay, meaning that factual evidence is insufficiently taken into account in political opinion forming and decision-making (e.g., in elections; Kavanagh & Rich, 2018). Authors who assume that this truth decay has increased in recent years even speak of a “posttruth” era (Jasanoff & Simmet, 2017; Lewandowsky, Ecker, & Cook, 2017; Sismondo, 2017) or “postfactual” politics (Sayer, 2017) when characterizing the current (Western) political discourse. Prominent examples from current political discussions for the persistence of political beliefs despite disconfirmatory evidence are climate-change denial (G. T. Farmer & Cook, 2013; Häkkinen & Akrami, 2014; McCright & Dunlap, 2011), the “vaccination confidence gap” (Browne, Thomson, Rockloff, & Pennycook, 2015; Larson, Cooper, Eskola, Katz, & Ratzan, 2011; Tafuri et al., 2014), and the discussion about gun control in the United States (Rogowski & Tucker, 2018).
Research has revealed that the extent to which political beliefs are updated after receiving new information in relation to prior beliefs is influenced by party identification. For example, Swire, Berinsky, Lewandowsky, and Ecker (2017) conducted an experiment in November 2015 in which they used political statements Donald Trump made during his campaign, some of which were objectively false and some factual. When presented to participants, half of the statements were explicitly attributed to Trump, whereas the other statements were presented without attribution. Inaccurate statements were subsequently corrected, and factual statements affirmed, with a brief explanation. The authors found that when initially evaluating the veracity of both false and factual statements, Republican supporters of Trump believed the information more when it was attributed to Trump, whereas the opposite was found for Democrats and Republicans who did not support Trump (albeit to a lesser extent than Democrats). Immediately after being presented with the correction/affirmation of the statements, all participants updated their beliefs; strikingly, however, Trump supporters “rebelieved” in the misinformation a week later and partially forgot that factual information was true. The authors concluded from their findings that even if individuals update their political beliefs temporarily, they become oblivious to disconfirmatory evidence over time and use partisanship and political figures as heuristics to guide their evaluation of what is true or false. These findings are in line with other research that has provided evidence for biased belief updating in the context of political information (Ecker, Lewandowsky, Fenton, & Martin, 2014; Swire, Ecker, & Lewandowsky, 2017).
Now that we have reviewed the basic characteristics of belief updating in healthy people, we next turn to belief updating in clinical populations.
Between Persistence and Hasty Changes: Belief Updating in Clinical Populations
As discussed in the first part of this article, dysfunctional (i.e., overly negative) beliefs are regarded as core features of almost all mental disorders. Researchers have consequently been interested in whether such dysfunctional beliefs are adjusted if people with certain mental health problems receive new information that questions the validity of their beliefs. In this context, some interesting results have been provided over the years that converge on the finding that people with various mental disorders have difficulty updating disorder-specific dysfunctional beliefs.
Lack of updating disorder-specific beliefs
Depression
It is well established that people with depression hold negative beliefs about themselves, other people, and the future (“cognitive triad”) that lead them to interpret new information negatively (Beck, 1964; Beck, Rush, Shaw, & Emery, 1979). More recent research has demonstrated that such negative beliefs, once established, become resistant to updating, even if novel positive information is received. In one study, for instance, people were presented with brief descriptions of emotionally relevant situations (e.g., “The company you are working for needs to lay off many employees, and you are called in to see your boss”) and were asked to choose one of four interpretations that best fit with the scenario presented (Everaert, Bronstein, Cannon, & Joormann, 2018). Participants subsequently received additional information on the scenario that questioned their initial interpretation and suggested an alternative interpretation (e.g., “Your boss shares how upset he is about having to lay off his employees and states that he wants you to stay because of your collegiality and achievements”). The authors found that if the scenario initially suggested a negative interpretation, people with depressive symptoms had difficulty abandoning that interpretation even when subsequent information clearly favored a more positive interpretation. By contrast, depressive symptoms did not predict difficulties in revising initially positive interpretations after receiving novel negative information (Everaert et al., 2018). Similar results regarding the hesitant updating of negative interpretations in people with depressive symptoms have been provided by Liknaitzky, Smillie, and Allen (2017).
Extending these findings to the revision of negative performance-related expectations, other research found that people with major depression, unlike healthy subjects, maintained negative expectations for their performance despite disconfirming positive performance feedback (Kube, Rief, Gollwitzer, Gärtner, & Glombiewski, 2019). In contrast, another recent study found no differences between healthy people and people with depression in updating positive performance expectations after unexpectedly negative feedback (Kube, Kirchner, Rief, Gärtner, & Glombiewski, 2019).
Collectively, these findings suggest (a) that there are no pathologies in belief updating per se in depression but (b) that abnormalities in belief updating apply only to the revision of negative prior beliefs, consistent with the cognitive model of depression (Beck & Haigh, 2014; Beck et al., 1979). Moreover, when it comes to the updating of beliefs about the undesirable life events in the face of new factual information, research has demonstrated that the above-referenced optimism bias (which is typical of healthy people) is absent in people with depression (Garrett et al., 2014; Korn, Sharot, Walter, Heekeren, & Dolan, 2014). In other words, whereas healthy people maintain optimistic beliefs despite disconfirming negative information, depression is related to the opposite pattern—namely the persistence of negative beliefs despite novel positive information (rather than increased sensitivity to unexpectedly negative information).
Anxiety
Evidence for biased belief updating has also been provided in several domains of anxiety. Without claiming to be exhaustive, we present a few of these findings as examples below. For instance, social anxiety disorder (SAD), like depression, is characterized by a negative view of the self (e.g., beliefs about being uninteresting and embarrassing). One recent study examined how such negative beliefs about the self in SAD are updated when social feedback from others is received (Koban et al., 2017). The authors assessed beliefs about the self in people with SAD and healthy control subjects before asking them to perform a speech task in front of three judges on why they would be suited for a certain job. One of the judges was instructed to provide positive feedback, another negative, and the third was supposed to give neutral feedback. It was found that people with SAD updated their beliefs more in response to negative evaluative feedback, consistent with their negative view of the self; by contrast, healthy subjects updated their beliefs more in line with positive social feedback, which is in accordance with the well-established positivity bias in healthy people (Korn et al., 2012). Remarkably, this group difference endured at a 1-year follow-up, speaking to the long-term endurance of positively biased social learning about the self in healthy people, whereas this bias is absent or even reversed in people with SAD (Koban et al., 2017). This finding is consistent with other research showing an attentional bias of people with SAD toward negative social cues (Schultz & Heimberg, 2008) and the lack of a positive interpretation bias (Amir, Prouvost, & Kuckertz, 2012).
It has been well established in research on PTSD that the experience of a traumatic event dramatically violates people’s belief in a just and safe world, often leading to negative beliefs about the self, other people, and the world in general (Dalgleish, 2004; Woud, Kleim, & Cwik, 2019). To explain this dramatic change in people’s beliefs, the concept of overaccommodation has been introduced (Resick & Schnicke, 1992). Accommodation is treated as a process by which preexisting beliefs (e.g., “The world is safe”) are revised after receiving new information. Overaccommodation in this context is regarded as a maladaptive generalization of exceptions of the former belief to integrate disconfirmatory information as provided by the trauma, thus leading to overly negative beliefs such as “The world is never safe.” Such overly negative beliefs are then maintained despite positive disconfirmatory evidence (i.e., safety signals; Resick & Schnicke, 1992, 1993). This is consistent with research into extinction learning deficits in PTSD. For example, in one study, people with PTSD were fear-conditioned before their psychophysiological and functional MRI responses to extinction were assessed in two different contexts: a safety context and a danger context (Garfinkel et al., 2014). Somewhat counterintuitively, the authors provided evidence for both abnormally high fear in the safety context and abnormally low fear in the danger context in people with PTSD. The authors suggested that these findings point to a general deficit of people with PTSD in processing contextual information, which is consistent with other research linking PTSD to diminished cognitive flexibility in PTSD patients, that is, the reduced ability to adapt beliefs flexibly to the situational circumstances (Keith, Velezmoro, & O’Brien, 2015).
Similar effects of negative beliefs being resistant to updating can be found in panic disorder. Cognitive models of panic disorder assume that panic attacks result from catastrophic misinterpretations of bodily sensations, such as the belief “I’m dying of a heart attack” in the event of an increased heart rate (D. M. Clark, 1986). Strikingly, these catastrophic beliefs are maintained even though people with a panic disorder repeatedly experience that the feared event does not occur, for example, that they do not die. In fact, many people with panic disorder fear that the next panic attack is going to kill them, although this has not been the case with all other panic attacks to date. It has been proposed that such maintenance of catastrophic beliefs in panic disorder is due to safety-seeking behaviors, including both avoidance of (i.e., agoraphobic) situations and behaviors occurring within such situations that are intended to prevent feared catastrophes (D. M. Clark, 1999; Salkovskis, Clark, & Gelder, 1996; Salkovskis, Clark, Hackmann, Wells, & Gelder, 1999).
The same pattern of hesitant belief updating has been found in obsessive-compulsive disorder (OCD). For example, one study drew on the assumption of an overestimation of threat in OCD and asked people with OCD and healthy control subjects to estimate the likelihood of various disorder-related events, such as unintentionally being responsible for a burglary (e.g., door not locked properly). Participants also rated their personal vulnerability to experience each event type before they were presented with statistics displaying the average likelihood of these events. The authors found that, compared with the control subjects, people with OCD believed they were more vulnerable to these adverse events and updated their beliefs to a lower extent after receiving the correct statistics (Moritz & Pohl, 2009). This finding was replicated in another study (Moritz & Jelinek, 2009).
Psychosis
In a similar vein, delusional patients with schizophrenia appear to fail to take new disconfirmatory evidence into account to adjust their prior beliefs (Buchy, Woodward, & Liotti, 2007; Speechley, Ngan, Moritz, & Woodward, 2012; Woodward, Moritz, Cuttler, & Whitman, 2006; Woodward, Moritz, Menon, & Klinge, 2008). To investigate this phenomenon, Woodward and colleagues developed the bias-against-disconfirming-evidence task. In this task, 3 of which several variations exist, participants are presented with delusion-neutral scenarios (e.g., depicted in a picture) and are asked to rate the plausibility of four interpretations of the scenario. Participants are then shown new pictures that provide background information on the scenario and are requested to adjust their ratings. Two of the four interpretations appeared tenable initially but ultimately turned out to be implausible, one appeared untenable initially but later seemed to be most plausible, and one was never plausible. Researchers have repeatedly demonstrated that delusional patients and healthy subjects (but not nondelusional patients) had a bias to uphold their initial interpretation although it proved to be implausible ultimately (Buchy et al., 2007; Speechley et al., 2012; Woodward et al., 2006). This effect was particularly pronounced in the case of “strong” initial beliefs, that is, beliefs that were held with a high degree of confidence (Woodward et al., 2008).
Persistent physical symptoms
Stretching belief-updating abnormalities to people with persistent physical symptoms (PPS), researchers examined how people with PPS update worrisome beliefs about having an undetected serious disease. In one study, patients with PPS, patients with depression, and healthy people were asked to imagine that they would suffer from bothersome gastrointestinal problems (i.e., abdominal pain). Afterward, they received medical reassurance through an audiotaped doctor’s report stating clearly that the presence of a serious physical disease is highly unlikely according to the medical tests that were performed. The results showed that people with PPS, unlike healthy and depressed subjects, continued to worry about having a serious disease despite medical reassurance (Rief, Heitmuller, Reisberg, & Ruddel, 2006). Similar results have been provided by Donkin et al. (2006), Linton, Boersma, Vangronsveld, and Fruzzetti (2012), and Nijher, Weinman, Bass, and Chambers (2001).
All of these examples speak to the notion that people with certain mental health problems maintain such kinds of beliefs that reflect core features of the particular disorder despite disconfirmatory evidence. As we review next, however, there is also an opposite pattern of belief updating that has been reported in some clinical populations: hasty changes in beliefs 4 based on fairly thin evidence.
The other side: hasty changes in beliefs
Jumping-to-conclusion bias in psychosis
To explain the genesis and maintenance of unsubstantiated delusional beliefs in people with schizophrenia (e.g., the belief that one is being pursued by the Central Intelligence Agency because an unknown car is parked in front of the house), Hemsley and Garety (1986) introduced the hypothesis of a jumping-to-conclusion (JTC) bias. According to this hypothesis, deluded patients update their beliefs hastily in the direction of a feared event on the basis of remarkably little evidence. This hypothesized JTC bias has been empirically confirmed in a number of studies (Garety, Hemsley, & Wessely, 1991; Lincoln, Ziegler, Mehl, & Rief, 2010; Moritz & Woodward, 2005). In most studies that examined the JTC bias, a bead task was used. In this task, participants are presented with two glasses containing colored beads in different proportions (e.g., one glass containing 85% red beads and 15% blue beads and another glass containing 85% blue beads and 15% red beads). Glasses are then removed, and beads (one at a time) are drawn from one of the two containers; participants are unable to see from which of the containers each bead is drawn. After each bead, the participants’ task is to indicate whether they can determine from which container the bead was drawn. Deluded schizophrenic patients indicate that they are sure which glass the beads come from earlier than healthy and clinical-control subjects. Intriguingly, 40% to 70% of deluded schizophrenic patients state after the first bead that they know from which container the bead was drawn (Fear & Healy, 1997; Garety et al., 1991; Huq, Garety, & Hemsley, 1988).
More recently, it has been suggested that a liberal acceptance bias may additionally contribute to biased belief updating in schizophrenia, meaning that people with schizophrenia more readily accept ambiguous information and draw conclusions from it. In a well-designed series of experiments, Moritz and colleagues provided evidence for this hypothesis (Moritz & Woodward, 2004; Moritz, Woodward, Jelinek, & Klinge, 2008; Moritz, Woodward, & Lambert, 2007).
Belief updating in autism spectrum disorder
Autism spectrum disorder (ASD) is an umbrella term for a wide spectrum of symptoms that are characterized mainly by social and communication difficulties and repetitive and restrictive behaviors that vary in severity. One additional, often overlooked characteristic of ASD is more rational, consistent, and unbiased information processing and reasoning (G. D. Farmer, Baron-Cohen, & Skylark, 2017; Gosling & Moutier, 2018; South et al., 2014). For example, ASD participants are less susceptible to negative versus positive framing of choices (i.e., the framing effect; De Martino, Harrison, Knafo, Bird, & Dolan, 2008; Shah, Catmur, & Bird, 2016). This finding raises interesting questions regarding how individuals with ASD update their beliefs. Specifically, one could assume that such enhanced rationalism is reflected by an overly accurate (and less biased) updating of beliefs. To our knowledge, only one belief-updating task has been tested in individuals with ASD so far, and this was the optimistic-bias task (Kuzmanovic, Rigoux, & Vogeley, 2019) referenced above. Confirming the hypothesis of more rational belief updating in people with ASD (relative to healthy people), Kuzmanovic et al. (2019) showed that individuals with ASD displayed a reduced optimistic bias, as reflected in more equal updating of positive and negative news than the control group, which showed a significant tendency to integrate good—and disregard bad—news.
In a broader context, such a tendency to integrate new information equally, regardless of its valence, falls nicely within the predictive-processing account of ASD. In the past few years, researchers harnessed the PPF to provide a unifying theory of the otherwise unrelated ASD symptoms (Lawson, Rees, & Friston, 2014; Pellicano & Burr, 2012; Sinha et al., 2014; Van de Cruys et al., 2014). Beyond ASD’s two core symptoms (social-communication difficulties and restrictive, repetitive behaviors), which have seemingly no shared underlying mechanism, ASD often includes additional symptoms, such as sensory hypersensitivities, impaired sensorimotor coordination, insistence on sameness, and so forth (Leekam, Nieto, Libby, Wing, & Gould, 2007; Mostofsky et al., 2009; Rozenkrantz et al., 2015), all seemingly disparate from one another.
Viewed from the perspective of the PPF, ASD entails an imbalance in the precision afforded to incoming information relative to prior predictions, such that new information that does not match the prior information is constantly favored. Whether this is due to “weak” priors (i.e., priors that are afforded too little precision) or the enhanced precision of incoming information is subject to debate. Nonetheless, this framework nicely accounts for various ASD symptoms: Incoming sensory information is not attenuated by prior predictions, thus leading to sensory overflow (i.e., a failure to attenuate sensory precision); and weak priors regarding motor action and outcome (internal action models) may harm the ability to modulate a motor response after sensory input (e.g., following a moving object with one’s eyes), leading to impaired sensorimotor coordination. Furthermore, impaired social predictions may account for one of the social hallmarks of ASD—impaired theory of mind, which can be explained by the unpredictability of others’ responses and thoughts. Finally, a lack of predictability may lead to a constant experience of surprise and uncertainty. Repetitive behaviors and a need for structured routines (i.e., need of sameness) are thought to be coping mechanisms of such uncertainty (Lawson et al., 2014; Pellicano & Burr, 2012; Sinha et al., 2014; Van de Cruys et al., 2014). Taken together, current views suggest that individuals with ASD update their beliefs in a rational, information-driven manner, bypassing cognitive and psychological biases, which leads to more consistent—and often better—decision-making.
Belief updating in borderline personality disorder
Borderline personality disorder (BPD) is characterized by affective instability, impulsivity, and difficulties in social relationships. One core feature of BPD, which can be rephrased in terms of hasty changes in beliefs, is that people with BPD rapidly change the way they think about themselves and important others (American Psychiatric Association, 2013). With regard to the former, researchers have examined how beliefs about the self are updated after receiving social feedback. Applying the same social-interaction task with which a positivity bias in healthy people was previously revealed (Korn et al., 2012), Korn, La Rosée, Heekeren, and Roepke (2016b) found that people with BPD integrated undesirable social feedback for themselves to a greater extent than healthy subjects; that is, they updated their beliefs about themselves more strongly in a negative direction after a single negative experience.
Expanding on these findings, Liebke et al. (2018) used a virtual group-interaction paradigm (in which participants interacted with a group of computer-controlled avatars while being led to believe that these avatars represented real human coplayers) to investigate how people with BPD process social-feedback signaling either as social acceptance or rejection. The authors found that people with BPD adjusted their expectations of being socially accepted in response to negative but not positive social feedback. In a subsequent trust game, people with BPD behaved less cooperatively if they had previously received positive social feedback. Interpreting their findings from a clinical point of view, the authors suggested that the difficulties individuals with BPD have in relation to being socially accepted may hamper the formation of stable cooperative relationships and negatively affect interpersonal relationships (Liebke et al., 2018). In fact, people with BPD often have difficulties in social relationships; in particular, they are often torn between engaging in a very close relationship and breaking up. As a result, the relationships of individuals with BPD are often characterized by an “on-off” pattern, meaning that breakups are followed by reconciliation and being together again. These hasty changes in beliefs (e.g., from “My boyfriend is the best that ever happened to me” to “My boyfriend is a dishonest, bad person”) are often caused by information that is regarded as disconfirming “evidence” (e.g., seeing boyfriend talking to another woman), although other people may consider this information to be quite harmless. In line with these observations, recent studies have shown that BPD is also related to behavioral inconsistencies in social interactions and inconsistency in social decision-making (Preuss et al., 2016).
In other domains that are not core to BPD, there seem to be no abnormalities in belief updating in people with BPD compared with healthy people, as indicated in a study by Korn, La Rosée, Heekeren, and Roepke (2016a). In this study, the authors applied the above-referenced standard optimistic belief-updating task to people with BPD and healthy participants. They found that although people with BPD had more pessimistic baseline expectations of experiencing negative life events than healthy subjects, the two groups did not differ in updating their expectations; that is, they updated their estimates more toward desirable than toward undesirable information. Collectively, these findings suggest a nuanced picture of belief updating in BPD. Available evidence indicates that belief updating in people with BPD is not aberrant per se; rather, anomalies in belief updating seem to arise specifically from the asymmetric integration of social feedback. On the one hand, people with BPD rapidly update their beliefs if they receive negative social feedback; on the other hand, they have difficulty processing positive social feedback, which even contributes to interpersonal problems at a behavioral level.
Factors Contributing to Anomalies in Belief Updating
After discussing several examples of both the lack of belief updating and hasty belief updating in clinical populations, we next discuss factors that might underlie these anomalies in updating beliefs after receiving new information. In doing so, we also highlight whether there is evidence suggesting that these mechanisms are specific to certain conditions or whether they may also apply to healthy people.
Aberrant precision given to prior beliefs
With active inference, it is assumed that the degree of precision that is afforded to prior beliefs significantly influences the extent to which new information (i.e., prediction errors) is used to update beliefs. According to this view, research from computational psychiatry suggests that too much precision given to prior beliefs, accompanied by an attenuation of disconfirming information, might be a mechanism underlying the persistence of dysfunctional beliefs despite disconfirmatory evidence in various mental disorders (Adams, Huys, & Roiser, 2016; Friston, Stephan, Montague, & Dolan, 2014; Paulus, Feinstein, & Khalsa, 2019). Evidence for this strong-prior hypothesis has first been provided for psychosis: For example, Powers, Mathys, and Corlett (2017) demonstrated in an intricate approach that people who hear voices were more susceptible to conditioning-induced hallucinations; using neurocomputational modeling, they showed that this effect was based on strong perceptual priors. This finding was replicated by Benrimoh, Parr, Vincent, Adams, and Friston (2018) for auditory hallucinations. On the basis of these findings, the assumption of strong priors that override disconfirming sensory information has been discussed as a core feature of psychosis (Corlett et al., 2019; Sterzer et al., 2018). Similar to this aberrant-precision account of psychosis, it has been proposed that too much precision afforded to negative prior beliefs accounts for the lack of updating these beliefs despite positive experiences (i.e., prediction errors) in major depression (Barrett et al., 2016; J. E. Clark et al., 2018; Kube, Schwarting, et al., 2020).
Whereas too much precision afforded to priors is thought to contribute to persistent beliefs, we suggest that too little precision given to priors might contribute to the above-described phenomena of hasty changes in beliefs. This is consistent with current thinking in computational neuroscience, assuming that a low degree of precision in priors (i.e., weak priors) leads to a higher relative impact of sensory information (i.e., prediction errors) on the posterior predictions (Barrett & Simmons, 2015; Kanai et al., 2015; Paulus et al., 2019). Some empirical support for this idea can be found in research on autism, as described above. Additional support for the weak-prior hypothesis has been provided by research using dynamic causal modeling (e.g., in schizophrenia; Adams, Bauer, Pinotsis, & Friston, 2016; Bastos-Leite et al., 2014; Fogelson, Litvak, Peled, Fernandez-del-Olmo, & Friston, 2014).
In more general psychological terms, the assumption of weak prior beliefs that are highly susceptible to new information might be regarded as a form of belief fragility. That is, the less firmly people hold their beliefs, the more likely they use new information to update them. This corresponds well to some of the difficulties experienced by people with BPD, as discussed above. For instance, under the assumption that their beliefs about their relationships are fraught with uncertainty, it is understandable that people with BPD are highly sensitive to any new information that they feel is relevant to the stability of their relationship, both negative and positive (such as seeing the boyfriend with another woman vs. receiving a compliment from the boyfriend).
Although aberrant precision has so far been linked to anomalies in belief updating mostly in clinical populations, it is well conceivable that this link may also apply to healthy people under some circumstances. For example, applying the argument of aberrant precision to political attitudes, we suggest that too much precision given to prior beliefs might be an important mechanism underlying the maintenance of particular political beliefs despite disconfirmatory political news. In other words, if people hold political attitudes with a high degree of certainty, they tend to be skeptical about any information that contradicts their beliefs; hence, such information is likely to be ignored or given reduced weight.
Interpretation biases
Another mechanism that may underlie the persistence of dysfunctional beliefs despite disconfirmatory evidence is a biased interpretation of discrepant information. In particular, researchers have found that people with mental disorders have the tendency to interpret novel information through the lenses of their prior beliefs, thereby increasing the likelihood of confirming them. For example, as discussed above, people with major depression tend to interpret ambiguous situations negatively, especially if they contain self-referential information (Everaert, Podina, & Koster, 2017), and once negative interpretations have been established, they fail to use novel positive information to revise their interpretations (Everaert et al., 2018; Liknaitzky et al., 2017). Relatedly, research on affective forecasting has found that people with depression are biased in their prediction of their future affective states, meaning that they overestimate the anticipated presence of negative affect (Hoerger, Quirk, Chapman, & Duberstein, 2012; Marroquín & Nolen-Hoeksema, 2015; Radomsky, Wong, Dussault, Gilchrist, & Tesolin, 2019; Wenze, Gunthert, & German, 2012; Zetsche, Bürkner, & Renneberg, 2019). Similar interpretation biases have been found in patients with social anxiety: People with social anxiety favor negative interpretations of ambiguous social situations and tend to interpret unambiguous but mildly negative social events as catastrophes (Amin, Foa, & Coles, 1998; D. M. Clark & McManus, 2002; Stopa & Clark, 2000).
As with aberrant precision, interpretation biases may not be specific to clinical populations alone. In fact, there is a large amount of research in social and cognitive psychology on biased assimilation, which is conceptually very similar to the clinical research on interpretation biases. Specifically, according to the concept of biased assimilation, people’s interpretations of new information are assimilated into preexisting beliefs, thus sustaining and further “confirming” their beliefs (Lord & Taylor, 2009). For further discussion of persistent political beliefs in social and political sciences, readers may also be referred to the literature on attitude polarization (Boysen & Vogel, 2008; McHoskey, 1995; Munro & Ditto, 1997), resistance to persuasion (Tormala & Petty, 2004; Zuwerink & Devine, 1996), partisan bias (Bartels, 2002; Bullock, Gerber, Hill, & Huber, 2015), motivated reasoning (Redlawsk, 2002; Taber et al., 2009), and metacognitive sensitivity (Rollwage, Dolan, & Fleming, 2018).
Reappraisal
Cognitive reappraisal of disconfirmatory evidence is an additional factor that has been discussed as a contributor to the maintenance of dysfunctional beliefs (Rief & Glombiewski, 2016; Rief et al., 2015; Rief & Joormann, 2019). In particular, it has been suggested that people with mental disorders are prone to devaluing positive information that disconfirms disorder-specific negative beliefs by post hoc questioning of its credibility or considering it to be an exception rather than the rule. This negative reappraisal of disconfirming information resulting in a lack of belief updating has been referred to as “cognitive immunization” against disconfirming information. Experimental research has recently confirmed this hypothesis by indicating that modulating the appraisal of unexpectedly positive performance feedback affected how prior negative performance-related expectations were updated (Kube, Glombiewski, et al., 2019; Kube, Rief, et al., 2019). In these studies, people with depression worked on a performance test in which it is difficult for participants to evaluate whether they solved the tasks correctly. After the initial establishment of negative expectations, all participants received unexpectedly positive feedback for their performance. In people with depression, it was found that promoting the engagement in a post hoc devaluation of positive performance feedback (by informing participants that the test they were working on would not have proven to be valid and reliable) led to reduced expectation updating; in contrast, the inhibition of cognitive-immunization strategies (i.e., increasing the value of positive performance feedback) facilitated the updating of negative expectations in line with positive feedback (Kube, Glombiewski, et al., 2019; Kube, Rief, et al., 2019).
Another study indicated that the promotion of cognitive-immunization strategies in healthy people did not affect their adjustment of initial beliefs; that is, healthy people updated their expectations regardless of a reappraisal manipulation in line with positive performance feedback (Kube & Glombiewski, 2020). These findings suggest that the negative reappraisal of novel positive information is core to depression but is not typical of healthy people. However, it is conceivable that healthy people conversely use cognitive-immunization strategies to maintain their optimistic beliefs when confronted with bad news (Kube, Schwarting, et al., 2020; Sharot & Garrett, 2016).
Synthesis of Previous Research
Relating belief-updating anomalies to different stages of information processing
In the previous section, we compiled evidence of some factors that may contribute to certain anomalies in belief updating. Next, we aim to integrate these factors into the model of belief updating as a process of different stages of information processing. In doing so, we are facing an asymmetry in the depth with which the mechanisms of persistent beliefs versus hasty changes have been investigated so far: Although we were able to invoke a considerable amount of evidence of particular mechanisms underlying the lack of belief updating, little research to date has dealt with factors contributing to hasty changes in beliefs; accordingly, the latter is much less understood. Therefore, we consider these two phenomena separately.
With respect to persisting beliefs despite counterevidence, we identified three potential mechanisms that can be linked to different stages of information processing. First, the idea of hyperprecise prior beliefs, resulting in an increased weight given to them in relation to new information, can be linked to the stage of anticipation of new information. In other words, holding a belief with certainty implies that people anticipate to receive confirmatory rather than disconfirmatory information, or even actively search for information that fits into their beliefs, to put it in active-inference terms. Second, at the level of encoding/interpretation, research into interpretation biases and biased assimilation indicates that beliefs can be resistant to updating if people have a strong bias to reinterpret new information as a confirmation of their prior beliefs. Third, in terms of further processing and appraising new information, people may be inclined to uphold their beliefs if the validity of new information is questioned after the fact, as research on cognitive reappraisal suggests, leading to a disregard of disconfirmatory information so that beliefs are not altered. Figure 3 illustrates how factors underlying the lack of belief updating relate to different stages of information processing (i.e., anticipation, encoding, appraisal).
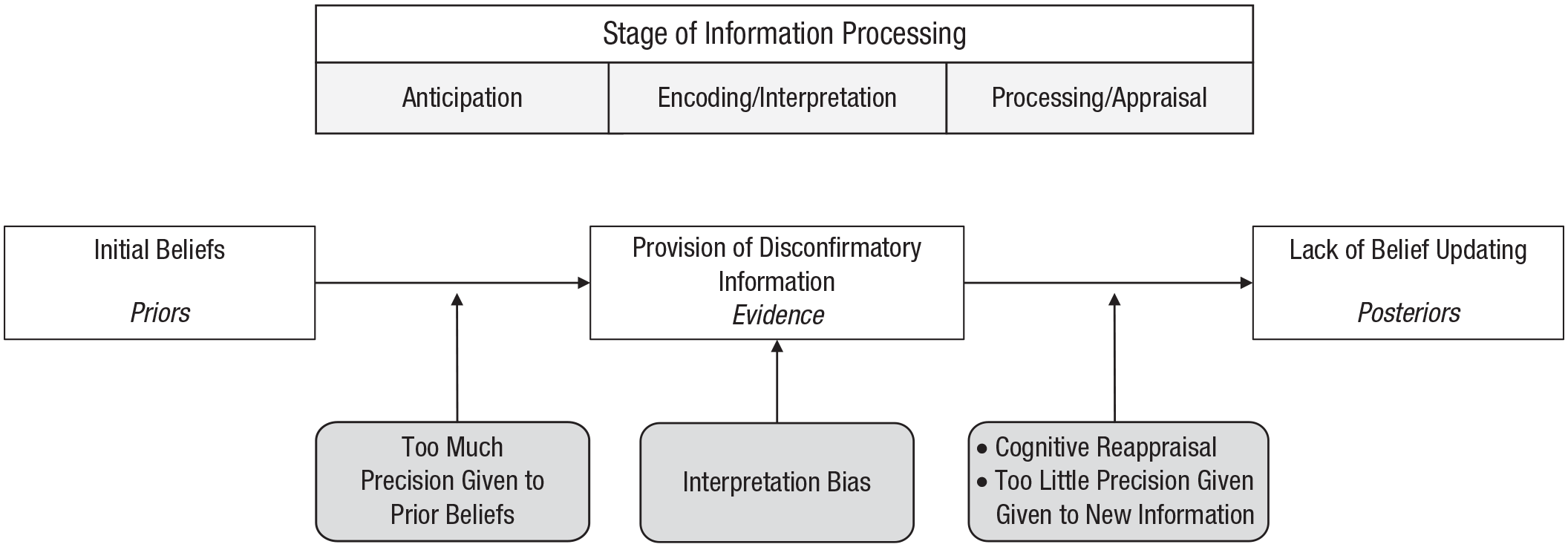
Factors contributing to the lack of belief updating at different stages of information processing. The Bayesian homologues of the belief-updating terminology are shown in italics.
From the discussion of hasty changes in beliefs, it emerged that little is known about particular mechanisms underlying this phenomenon. In terms of the different stages of information processing, past research allows only one cautious suggestion with reference to the PPF: Drawing on this framework, we assume that affording too little precision to prior beliefs leads to the posterior predictions being influenced by new information, whatever it may be, rather than by priors. However, given that little to date is known about mechanisms of hasty changes of beliefs, we refrain from including contributors to hasty changes of beliefs in a mechanistic or conceptual model.
An integrative model
As illustrated in Figure 4, we suggest that the degree of precision afforded to prior beliefs is a lens through which new information is perceived, interpreted, and appraised. In the case of strong priors (i.e., prior beliefs that are afforded high precision), belief updating is biased toward resistance to disconfirmatory information, as new information may be considered less informative or valid. By contrast, low precision afforded to prior predictions may bias perception toward new information such that posterior beliefs are strongly influenced by new information, formalized by the increased weight given to this new information (i.e., prediction error) and pronounced belief updating. Thus, the level of precision afforded to prior beliefs affects the perception of information and its appraisal, resulting in belief updating being tied to the priors (in the case of hyperprecise priors) or being influenced strongly by incoming input (in the case of weak priors).

Schematic illustration of how affording high versus low precision to prior beliefs and high versus low precision of new information influence belief updating.
As described previously, the valence of new information (i.e., good news vs. bad news) can critically influence belief updating. Thus, it may also affect the balance of precision given to priors and new information. Specifically, we noted that the computation of posterior beliefs is generally influenced by the relative weight of priors and new information. Valence comes into play here as follows. The precision afforded to new information, on the one hand, may depend on the source of incoming information. For example, one may trust one’s own observations more than others’ descriptions of them, thus resulting in more precision afforded to the former. On the other hand, the precision of new information may be determined according to its content, such as the valence of new information. Differentially weighing new information on the basis of its valence may then lead to some of the phenomena related to belief updating, as discussed above. For example, the optimism bias may be explained by assuming that healthy people, in general, afford high precision to positive information and low precision to negative information. This allows them to integrate new information asymmetrically into their beliefs (i.e., updating beliefs selectively in response to good news). In contrast, people with depression (as well as some other mental disorders) may show an opposite pattern: They afford little precision to unexpectedly positive information and thus only minimally update their initial beliefs.
Aside from valence, precision afforded to incoming information may also be evaluated on the basis of the confirmatory nature of its content (i.e., information supporting my initial beliefs will be weighed stronger than disconfirming information), its relevance, and other factors. As illustrated in Figure 4, we propose that this attribution of precision to new information occurs in a phase we call weighing: That is, people must first assess the information presented to them and categorize it in terms of good/bad, confirming/disconfirming, relevant/irrelevant, and so on, before assigning it a certain weight. This weight of new information is then matched with the precision-weighted priors to compute a posterior belief.
This integrative model is the first to our knowledge to connect the PPF with the belief-updating framework and to synthesize various, formerly unrelated lines of research into one coherent model. Specifically, it bridges neuroscientific research into the role of precision and psychological investigations of several biases in belief updating. Furthermore, this model provides a foundation from which to further investigate differences in belief updating between healthy people and people with certain mental health conditions. In particular, we propose that our model is suitable for explaining the aforementioned biases of belief updating in healthy people by assuming that, for instance, relatively high precision in optimistic future beliefs results in biased perception and appraisal of new information, hence leading to reduced belief updating in response to bad news. On the other hand, the model can explain the formation of pathologies in belief updating in that it suggests that abnormally high (or low) precision given to prior beliefs can result in the persistent lack of belief updating (or hasty updating of beliefs, respectively). Tying in with these ideas, we next discuss the implications of this account for the understanding of mental health and disorders in more detail.
Implications
Implications for the understanding of mental health as opposed to disorders
Integrating the phenomena discussed above, we suggest that belief updating in healthy people is quite volatile, meaning that it is biased toward the integration of information that fits into people’s preexisting assumptions in various domains. In particular, according to the literature on optimism bias and self-concept stability, we propose that belief updating in healthy people is driven by the valence of new information as well as by the desire for a stable, positive self-perception. In addition, the literature on attitude change has revealed that belief updating in healthy people is biased toward the integration of information that is consistent with core beliefs to make sense of the world, such as core political attitudes. In other words, if (healthy) people’s beliefs reflect an optimistic view of their personal future, their view of themselves, or basic assumptions about the world, beliefs are likely to be resistant to disconfirmatory information and updating. By contrast, in other domains, belief updating may be more sensitive to new information, especially if the adjustment of a particular belief is considered socially desirable, as suggested by research on social conformity (Asch, 1956; Bond & Smith, 1996; Larsen, 1974). This means that people are inclined to update their beliefs in line with new information if they consider it socially desirable. Collectively, research suggests that mental health is associated with the preferential integration of positive, self-concept-stabilizing information into one’s beliefs and the dismissal of information that is inconsistent with an optimistic view of the future, the self-concept, or core beliefs to make sense of the world.
Some of the biases in updating beliefs that are typical of healthy people (i.e., the optimistic bias) have been shown to be absent in people with clinical disorders, particularly depression and autism (Garrett et al., 2014; Korn et al., 2014; Kuzmanovic et al., 2019). More generally, available evidence suggests that as much as belief updating in healthy people is biased toward the confirmation of core beliefs of them (such as optimistic beliefs about the future and positive beliefs about the self), belief updating in mental disorders is biased toward the integration of information that is consistent with core beliefs of the respective disorder. That is, a belief seems to be particularly immune to updating if it is intertwined with core beliefs of the disorder, such as viewing oneself as being incapable in depression or the overestimation of threat in anxiety disorders. In other words, just as the nature of beliefs differs between people with certain mental disorders and healthy people, so does the nature of the information that is preferentially integrated (vs. disregarded). In both healthy people and people with clinical disorders, the (relative) immunity of core beliefs to disconfirmatory evidence might be accounted for by affording increased precision to prior beliefs or decreased precision to the incoming information (as illustrated in Fig. 4), although the content of the respective beliefs may differ considerably.
In other domains, healthy people and people with mental disorders may differ not only in terms of the contents of their beliefs but also mechanistically in the way new information is integrated. In particular, in cases in which prior beliefs are afforded overly low precision, they become highly susceptible to updating, as indicated, for example, for increased (in fact, more rational) belief updating in response to bad news in people with autism. In general, the phenomenon of hasty changes in beliefs as a consequence of weak priors as discussed for various clinical populations has, to our knowledge, not yet been reported for healthy people. Conversely, whereas in some cases increased precision of prior beliefs may also apply to healthy people, in some clinical conditions prior beliefs are so overly precise that they cause severe perceptual distortions, such as hallucinations in psychosis. Specifically, whereas perception in people who are in good mental health is normally influenced by both prior predictions and sensory evidence, it can be almost exclusively dominated by priors in psychotic hallucinations, resulting in a complete neglect of disconfirming sensory information. Similar accounts have been proposed for the experience of flashbacks in people with PTSD (Linson & Friston, 2019; Wilkinson et al., 2017) and medically unexplained physical symptoms (Edwards et al., 2012; Henningsen et al., 2018; Kube, Rozenkrantz, et al., 2020; Van den Bergh et al., 2017).
There is a compelling convergence of the mechanisms that underwrite attentional filtering (i.e., precision control) in terms of neuromodulation and psychopathology. A key example here is the ubiquitous role of the neuromodulator dopamine in various neurological and psychiatric conditions. For example, the primary deficit in Parkinson’s disease, leading to psychomotor poverty, is a dopaminergic deficit. Conversely, the most enduring synaptic hypothesis of schizophrenia suggests overactive dopamine neurotransmission (that is targeted by antipsychotics). A similar story might be told for oxytocin in autism. It has been noted previously that one of the most challenging computational issues in inference is estimating the precision or uncertainty afforded to (sensory) data. If this assumed role of precision is true, then psychopathologies that arise from aberrant precision control are quite understandable—as the most fragile computational challenge faced by the brain (A. Clark, 2013a; Hohwy, 2013).
Collectively, research into belief updating as reviewed in this article provides a new understanding of cognitive processes in mental health versus mental illness insofar as it suggests that healthy people and people with mental disorders differ not only in the nature of their beliefs but also in the way they integrate new information into their beliefs depending on the particular disorder. The relative precision of prior beliefs and incoming information is assumed to play a key role in this respect. These considerations—and the associated empirical evidence—do not allow any conclusions regarding whether belief-updating anomalies are a vulnerability factor of mental disorders or merely a consequence thereof (in terms of reflecting a clinical problem as a result from the disorder). To address this question, researchers would have to carry out longitudinal studies that allow crossed-lagged panel analyses.
In addition to contributing to the understanding of the psychopathology of some mental disorders, the clinical distortions in belief updating discussed above also have implications for psychological treatment. Specifically, as we highlighted in the introduction, dysfunctional beliefs significantly influence the severity and prognosis of various mental disorders, and so their resistance to updating and learning from new experience is particularly important from a clinical point of view. Accordingly, clinicians may aim to modify dysfunctional patterns of belief updating in their patients through cognitive-behavioral interventions. For example, because cognitive immunization against disconfirmatory evidence is regarded as an important obstacle when attempting to modify dysfunctional beliefs, future clinical research may develop psychological interventions aimed at inhibiting the engagement in cognitive-immunization strategies. A first proof-of-concept study in this context showed that it was possible to prevent people with depression from devaluing expectation-disconfirming positive information through cognitive-immunization-inhibiting strategies, thus facilitating the revision of negative expectations (Kube, Glombiewski, et al., 2019). It has also been shown that an optimistic view of the future can be trained in people with depression through optimism-enhancing interventions (Miranda et al., 2017). Another recent study demonstrated that such optimism training subsequently helped people with mild dysphoria to update their beliefs about future events more toward desirable information, thereby resembling the optimism bias that is typical of healthy people (Yoshimura & Hashimoto, 2020). However, the optimism training had no effects on belief updating in participants with either low or high dysphoria. We encourage researchers to continue this line of research to help people with mental health problems use novel information effectively to alter their dysfunctional beliefs.
To our knowledge, there has not yet been any research aimed at modifying the opposite pattern (i.e., hasty changes in beliefs). Given that affording too little precision to prior beliefs has been discussed as a possible contributor to pathology in the respective conditions, it may be worthwhile to develop and test interventions aimed at increasing confidence in prior beliefs and/or decreasing the precision given to new information.
Societal implications
In our view, the evidence summarized above on the characteristics of belief updating in healthy people also has implications for social and policy issues. For example, whereas the repeatedly referenced optimism bias may be adaptive in terms of mental health, it becomes problematic when people do not take information that threatens their livelihood seriously enough and fail to take necessary action. Sadly, this phenomenon can be observed in the context of climate change: Although scientific evidence is accumulating to document the devastating consequences of climate change, many people still deny the presence of man-made climate change and their responsibility to counteract it. Some evidence suggests that this, in addition to various other factors, may be due to the optimistic bias when confronted with bad news. Specifically, one study using eye tracking found that people with high trait optimism spent significantly less time attending to any information related to climate change, with particularly low fixation times if the arguments about climate change conveyed “bad news” (Beattie, Marselle, McGuire, & Litchfield, 2017). The authors also found that people with high dispositional optimism more likely recalled the arguments in terms of a debate between two opposing positions (as opposed to framing it as clear evidence) and were more confident that the consequences of climate change would not affect them personally (Beattie et al., 2017). Likewise, a study applying the belief-updating framework to information about climate change demonstrated that people who do not believe in the concept of man-made climate change updated their beliefs more toward good news (suggesting that the global rise of the average temperature may not be as dramatic as predicted) than toward bad news (suggesting that the global rise of the average temperature is even more dramatic than predicted; Sunstein, Bobadilla-Suarez, Lazzaro, & Sharot, 2017).
Thus, it seems that people are fleeing into tragic optimism when confronted with bad news about climate change, hoping that it may not become as horrific as science prognosticates or even denying man-made climate change fundamentally. Given that this individual bias—which is understandable from an individualistic point of view—in processing climate-change-related information contributes to collective inaction, it is a serious problem from a societal point of view. Most recent research suggests that this optimistic bias may also contribute to people’s difficulties in handling the current COVID-19 pandemic: A preliminary report from March 19, 2020, found that people from the United Kingdom, Germany, and the United States estimated the probability of getting infected with the virus—and of infecting others if infected themselves—as lower for themselves than for someone similar to them. Further, the authors linked this optimism to the estimated frequency of direct social contacts and to the necessity of—and difficulties in—reducing these contacts (Kuper-Smith, Doppelhofer, Oganian, Rosenblau, & Korn, 2020).
To return to the examples of current divisive and irreconcilable political controversies as discussed in the beginning of this article, another societal implication of biased belief updating might be derived. In particular, the phenomenon of truth decay discussed above must be considered alarming from a political and societal point of view. It is a crucial aspect of democratic systems that people are properly informed before making a political decision (e.g., in terms of voting for a particular party or person). If, however, there is the increasing tendency that people disregard information that does not fit into their view, this is dangerous for the state of democracy. It is inherent to political decisions that their correctness (in terms of, e.g., being more beneficial than harmful) can be confirmed or falsified by new information. We believe that in a healthy democracy new information should be considered thoroughly in examining past decisions, and if new information brings those decisions into question, they should be revised. Thus, from a political and societal perspective, beliefs should be updated if new information is available that disproves previous assumptions. Accordingly, from this perspective, we view the current developments regarding truth decay and “alternative facts” with great concern. Because “filter bubbles,” reductionism, vulnerability to “fake news,” and other features of social networks significantly contribute to this development, we believe that societies should discuss this development and the role of social networks in political decision-making more critically, particularly because more and more people base their political attitudes on information received on social networks. Future research on belief updating might contribute to this discussion by investigating how information can be provided such that people use it to examine the validity of their (political) beliefs critically.
Critical Assessment of Past Research and Future Directions
To our knowledge, this is the first review of belief updating that attempts to connect different lines of research and compare characteristics of belief updating in healthy and clinical samples. In our view, the field of belief updating is a fascinating area of research because it provides valuable insights into how people construct and update their subjective reality, including their views of themselves, other people, and the world in general. Great merits of past research can be seen in thorough experimental procedures derived from different theoretical backgrounds and have important implications for both clinical work and societal issues. Despite our enthusiasm, there are also a number of limitations of past research in this relatively nascent field that we discuss next in concert with some suggestions for future research.
The continuity of disconfirmatory information
As reviewed in this article, new information can be distinguished by whether it confirms or disconfirms previous assumptions. For the sake of simplicity, many researchers tended to regard confirmatory versus disconfirmatory information as binary concepts. However, because information can vary greatly in the extent to which it contradicts previous beliefs, we encourage researchers to develop experimental paradigms that allow taking the continuity of disconfirmatory information into account. An experimental paradigm that already considers this aspect is the one from Tali Sharot’s lab, which was used to study the optimism bias in healthy people as discussed above. A study on pain perception found that the relationship between the magnitude of the prediction error (indicating how large the difference between the predicted and actual outcome is) and the extent to which beliefs are updated is not linear but includes a “tipping point,” meaning that at some point the prediction error is so large that it is considered less reliable and thus entails reduced updating (Hird, Charalambous, El-Deredy, Jones, & Talmi, 2019). Continuing this line of research, researchers may examine the relationship between the magnitude of the prediction error and belief updating in domains beyond pain perception.
Belief updating as a dynamic phenomenon
Another limitation of previous research refers to the fact that belief updating is not a stable trait but varies dynamically on the basis of various factors. For example, Sharot and colleagues, using their optimistic-bias paradigm, found that the extent to which belief updating is biased toward the integration of desirable (vs. undesirable) information changes throughout the life span (Sharot & Garrett, 2016). Whereas the integration of good news remains stable over time, the discarding of bad news appears to be associated with younger age: Adolescents, to a larger degree than young adults, failed to integrate undesirable information, as revealed in a study by Moutsiana et al. (2013). This may contribute to the understanding of risk-taking in adolescence and have implications on educational risk-prevention programs at schools. When examining other age ranges, a U-shape curve is formed, such that the lowest optimistic bias in belief updating is seen in midlife, whereas younger (adolescents and young adults) and elderly individuals display higher resilience to the integration of bad news. Whether this age effect applies to belief updating in general or only to optimistic updating in particular remains an open question.
Beyond age, belief updating fluctuates depending on factors such as hormones and neurotransmitters, particularly dopamine. Administrating exogenous dopamine to healthy participants increased the discarding of bad news but had no significant effect on the integration of good news (Sharot, Guitart-Masip, et al., 2012), much like the effect seen in adolescents. Dopamine is involved in many neural processes, including the reward system, where it mediates the process of learning from reward and punishment (Pessiglione, Seymour, Flandin, Dolan, & Frith, 2006). Likewise, research on people with Parkinson’s disease has demonstrated that dopamine diminished learning from unwanted outcomes when the patients were on dopamine-containing medication (Frank, Seeberger, & O’Reilly, 2004), contributing to its effect on belief updating. Providing a different neurotransmitter, oxytocin (administered intranasally), led not only to the reduced integration of bad news but also to the increased integration of good news. This was explained by oxytocin’s role in promoting adaptation in social situations by modifying cognitive and emotional responses (Ma et al., 2016). In view of these various sources of influences on belief updating, we encourage researchers in the field to consider factors such as age, hormones, and neurotransmitters thoroughly in their studies and test whether this is a by-product of the optimistic bias or a genuine belief-updating trait.
The question of adaptivity
In this article, we presented the examples of persistent beliefs and hasty changes in a fairly descriptive manner. In our view, an underexplored aspect in this context is the more normative question of when it is adaptive for people to update their beliefs. So far, researchers have mostly investigated simply whether or not people updated their beliefs, and some patterns in this regard were considered “adaptive” and hence linked to mental health. This prompts the question of what adaptive means, and we believe that the answer may depend on the (scholarly) perspective of researchers. For instance, from a predictive processing point of view, it is adaptive to update beliefs if there is enough reliable evidence that disconfirms people’s prior beliefs relatively independent of the nature or content of a belief. By contrast, from a mental health perspective, belief updating would be regarded as adaptive when it helps people sustain their mental health. From this perspective, the content of the particular belief is very important in relation to the question of when it is adaptive to update it: There are some beliefs that can reasonably be considered dysfunctional, such as very negative beliefs about oneself (e.g., “I’m worthless”), whereas other types of beliefs can be assumed to be healthy, such as a mildly positive belief in one’s own abilities. From this standpoint, it would be adaptive to update dysfunctional beliefs and to maintain adaptive beliefs, each even on the basis of rather limited evidence. Additional perspectives to consider for the question of adaptivity might be an evolutionary-psychology perspective and a societal perspective.
Conclusions
To our knowledge, this is the first review of belief updating in mental health and illness. We pointed out that belief updating in healthy people is biased toward the integration of desirable information, self-concept-congruent information, and information that is consistent with a person’s view of the world in general. When examining phenomena related to belief updating in clinical populations, we examined two opposing phenomena: a persistent lack of updating disorder-specific beliefs and hasty changes of beliefs. We identified aberrant precision given to prior beliefs as a key aspect of pathology, which may account for both problematic phenomena depending on whether prior beliefs are afforded too much or too little precision. Building on previous research, we provided a synthesis of several lines of research and hope that this review inspires future research in the exciting field of belief updating, as it is highly relevant to several psychological disciplines.
Footnotes
Acknowledgements
We thank Lukas Haffert for valuable suggestions of relevant literature from political sciences; Dorina Winter for advice regarding borderline personality disorder; and Anne Suffel for helpful comments on a previous version of the article.
Transparency
Action Editor: Joshua Hicks
Editor: Laura A. King
Author Contributions
T. Kube and L. Rozenkrantz contributed equally to this work.