
Abstract
Background
Malaysian government has currently no drug pricing regulation. Therefore, drug prices are determined by the market force. In Malaysia, dispensing doctors have dual roles in prescribing and dispensing medicines to patients. General practitioners in private clinics are legally permitted to dispense prescription drugs to their patients. Consequently, general practitioners and community pharmacists play a similar functional role in dispensing medicines to patients because system of dispensing separation is still lacking. This study aims to evaluate the perceptions of general practitioners toward issues of pharmaceutical price war, different bonus schemes provided by pharmaceutical companies, and to assess the selling prices of some prescription drugs.
Method
This study is a cross-sectional questionnaire-based study. Mail survey methodology was adopted in this study to elicit the information of perceptions of general practitioner toward pharmaceutical price war and the selling prices of the top 5 most common Group B prescription drugs in Malaysia. The development of the questionnaire was informed by previous studies Hassali et al. and Tan. All statistical analysis had been performed using Statistical Package for the Social Sciences version 17.0.
Results
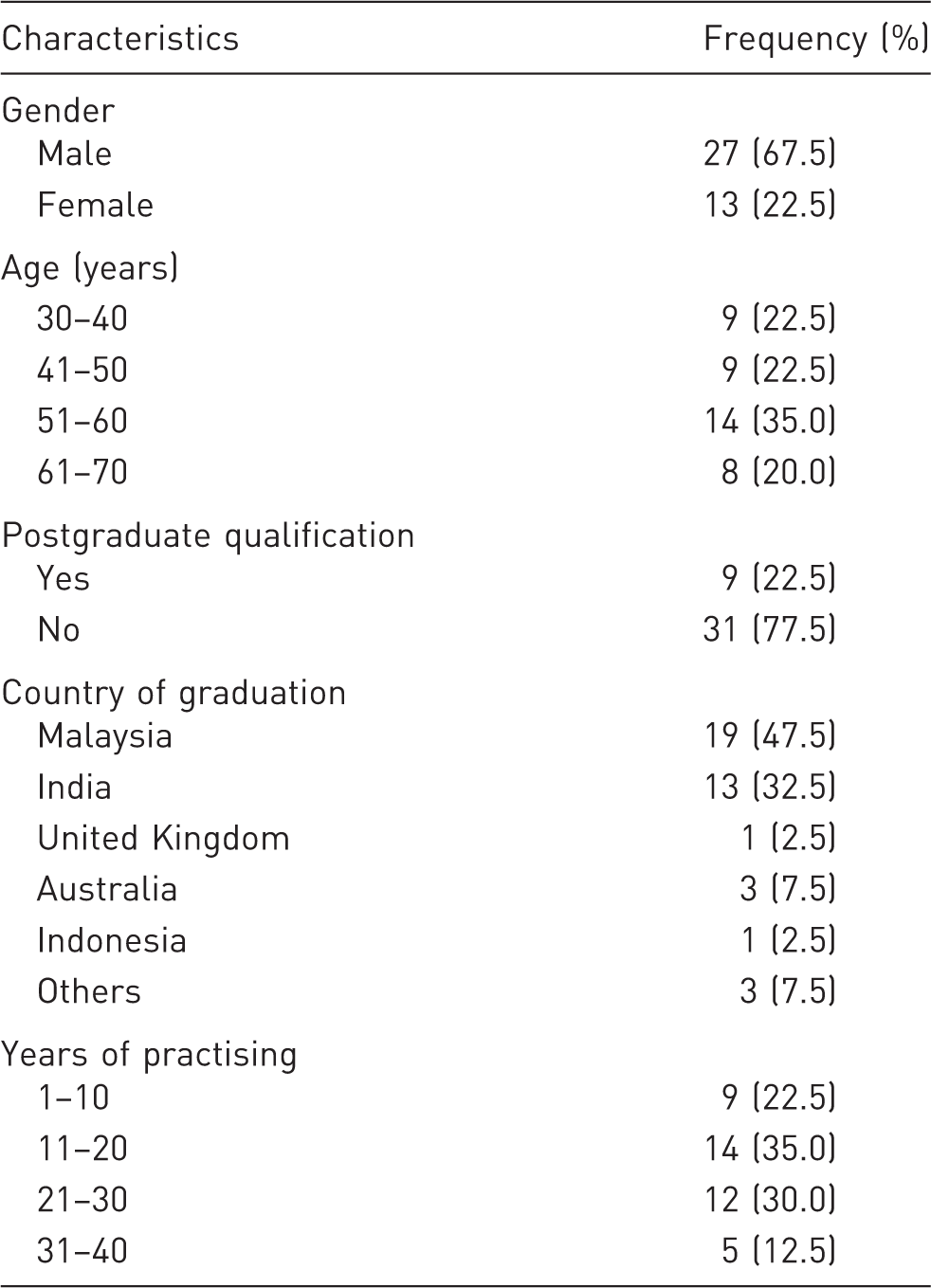
Of the 40 responses, (68%) were male participants. Forty percent of the respondents prescribed more than 40 prescriptions per day. Majority of the respondents (60%) strongly agreed that community pharmacies have created the phenomenon of pharmaceutical price war. And almost half of the respondents (45%) agreed that it is reasonable to have different bonus schemes based on the quantities ordered for pharmaceutical products. The price of Plavix® (Clopidogrel) has the highest variation among the prescription drugs (Ringgit Malaysia 94.0 ± 20.3). Lipitor® (Atorvastatin) has the least variation among the innovator drugs (Ringgit Malaysia 40.0 ± 1.6).
Conclusion
In order to preserve the viability of community pharmacies and general practitioners in the country, the authorities should monitor medicine prices especially at the private sector to ensure affordability and to ensure pricing of medicines are appropriate.
Introduction
Globally, most countries are facing the challenge of growing health care demand with limited available resources.1,2 Moreover, the drug prices and expenditure are steadily increasing over the years. Thus, it became more challenging to muddle through the demand and supply of pharmaceuticals. 3
Malaysian government has currently no drug pricing regulation.4–6 Therefore, drug prices are determined by the market force (i.e. pharmaceutical-free market). The healthy competition can stabilize drug prices especially in the private sector. Therefore, Ministry of Health (MOH) plays a role in only medicine procurement in the public sector. In private sector, due to the absence of drug price regulation in Malaysia, pharmaceutical companies, wholesalers, and health care professionals can set their own retail selling prices (RSPs).7–9 Consequently, this free pricing policy had reported to cause high markup of pharmaceutical products in Malaysia. 10 The median price ratio of innovator brand medicines was 16 times higher than International Reference Pricing. 11 Moreover, Hassali et al.7 reported that the retail prescription drug prices in Malaysia were 30.30–148.28% higher compared to Australia. Unlike Australia, which is practicing drug pricing policy, Hassali and colleagues also revealed that there were huge variations in prescription drug prices between retail pharmacies in Penang, Malaysia. Moreover, the study revealed that the price difference was up to 80% for the same brand of the medicine sold at different pharmacies in Penang. 7 Most of the pharmacies compete with each other by lowering medicine price in order to retain their regular customers. Therefore, same pharmaceutical products are sold at different prices at community pharmacies in Malaysia. 7
In Malaysia, dispensing doctors have dual roles in prescribing and dispensing medicines to patients. General practitioners (GPs) in private clinics are legally permitted to dispense prescription drugs to their patients. Consequently, GPs and community pharmacists play a similar functional role in dispensing medicines to patients because system of dispensing separation is still lacking. 12 However, GPs procured pharmaceutical products with better bonus deals compared to community pharmacies. Thus, GPs tend to gain higher profit margin especially in dispensing low-priced generic medicines. 11 In terms of disparity of drug pricing between community pharmacies and GPs, a recent study has revealed that there was a huge difference in pricing for common cold medicines between the two health care professionals. 13 Nevertheless, there was great gap between the community pharmacy and GPs toward the perception of current situation of intense competitive pharmaceutical price war, usage of generic medicines, and the disparities of medicine selling prices. In conjunction to the previous studies conducted with community pharmacists toward the issue of pharmaceutical price war,5,14 this study aims to evaluate the perceptions of GPs toward issues of pharmaceutical price war, different bonus schemes provided by pharmaceutical companies, and to assess the selling prices of some prescription drugs, in order to portray a true picture of pharmaceutical pricing in Malaysia.
Methodology
Design and sample
This study is a cross-sectional questionnaire-based study. Mail survey methodology was adopted in this study. Mail survey is considered less expensive compared to in-person interviews and telephone survey when involving a large sample.15–17 Moreover, mail survey is suitable to include lengthy questionnaires as respondents may have adequate time to answer it. 18 In line with these criteria, mail survey is the most suitable method to be adopted in this study to elicit the information of perceptions of GP toward pharmaceutical price war and the selling prices of the top 5 most common Group B prescription drugs in Malaysia. 19 According to the Malaysian Poison Act 1952, Group B Poisons only can be dispensed by a registered pharmacist in a licensed premise with a prescription. Group B Poisons comprise of antihypertensive medicines, cholesterol-lowering agents, cardiovascular medicines, and some other medicines that are indicated for some chronic diseases; Group C Poisons only can be dispensed by a registered pharmacist without prescription in a licensed premise. 20 In this study, self-addressed postage paid questionnaires and invitation letter explaining the purpose of the study were sent to GPs.
This quantitative study had been carried out in Penang. There are 420 GPs in Penang according to Pharmaceutical Service Division, MOH Malaysia. The study targeted GPs in private sector who were prescribing and dispensing cardiovascular and diabetes medicines to their patients. Hence, a total of 300 GPs was selected out of 420.
Survey instrument
The development of the questionnaire was informed by previous studies (Hassali et al., 2013 and Tan, 2014). The questionnaire comprised three parts. The first part aimed to collect the demographic data of the respondents. The second part included the statements pertaining to perceptions of GPs to issues pertaining pharmaceutical price war and different bonus schemes provided by pharmaceutical companies in Malaysia. The last part focused on the pricing of the selected five types of medicines that are highly sold in Malaysia.
Data analysis
All statistical analysis had been performed using Statistical Package for the Social Sciences version 17.0. Descriptive and inferential statistics were used in this study. Chi-square test was used to compare the demographic variables with the respondents’ generic medicine dispensing pattern and their perceptions toward pharmaceutical price war and different bonus schemes. A p value of less than 0.05 was considered to be statistically significant.
Results
A total of 40 out of the 300 questionnaires sent to the private GPs was received, giving a response rate of 13%. However, 20 mails could not reach the desired destinations due to the error in address writing or changing dwelling place.
Demographic data of participants
Demographic characteristics of the participants
Perceptions of GPs toward pharmaceutical price war, different bonus schemes offered and factors influencing procurement of medicines by GPs
The perceptions of respondents toward pharmaceutical price war and bonus schemes offered by pharmaceutical companies
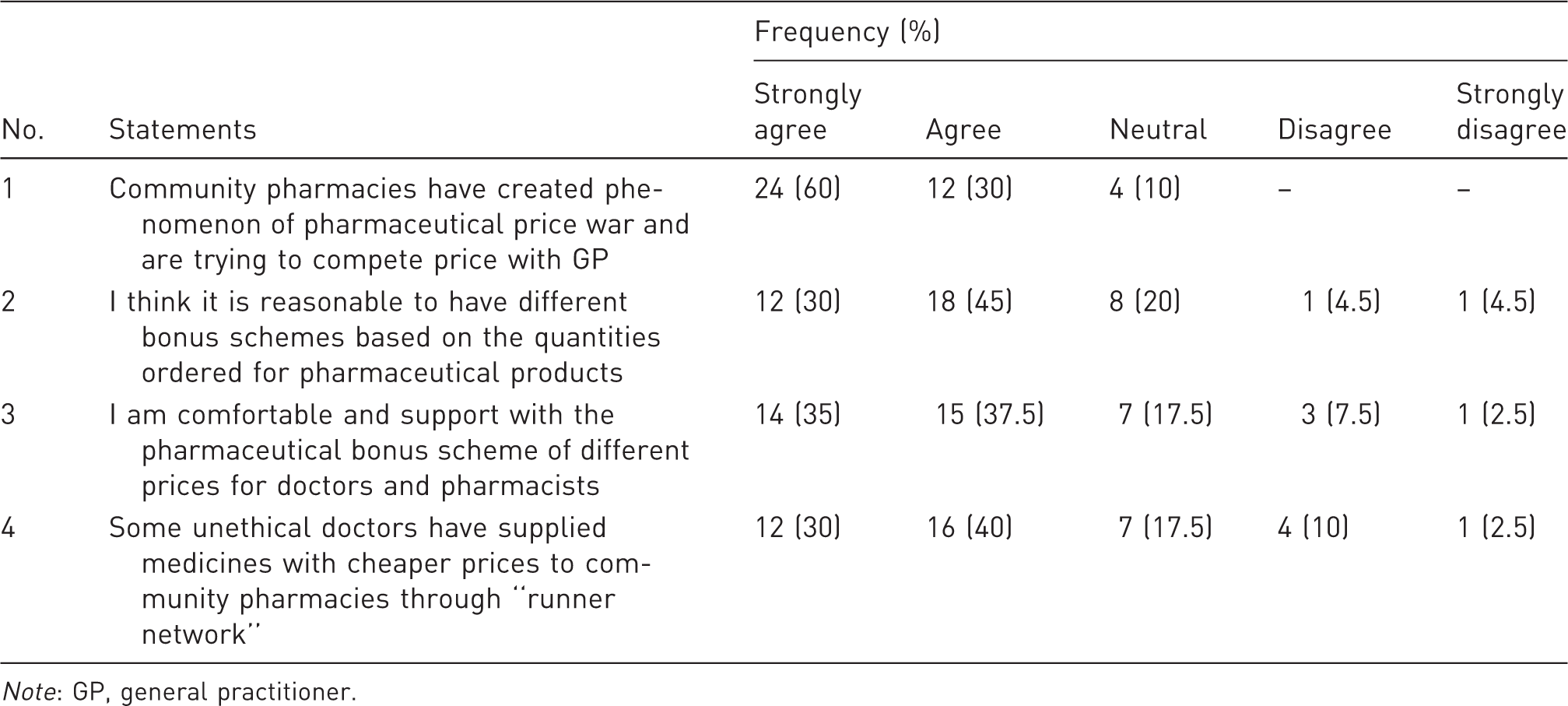
Note: GP, general practitioner.
The factors influencing procurement of medicines by GPs

Note: GP, general practitioner.
Comparison of prescription drugs’ pricing procured from GP (RM per strip)

Note: GP, general practitioner. RM, Ringgit Malaysia (conversion rates based on international exchange rate on 15 January 2013: 1 USD = 3.0107 RM).
Comparison of prescription drugs’ pricing between GP and community pharmacies (RM per strip)

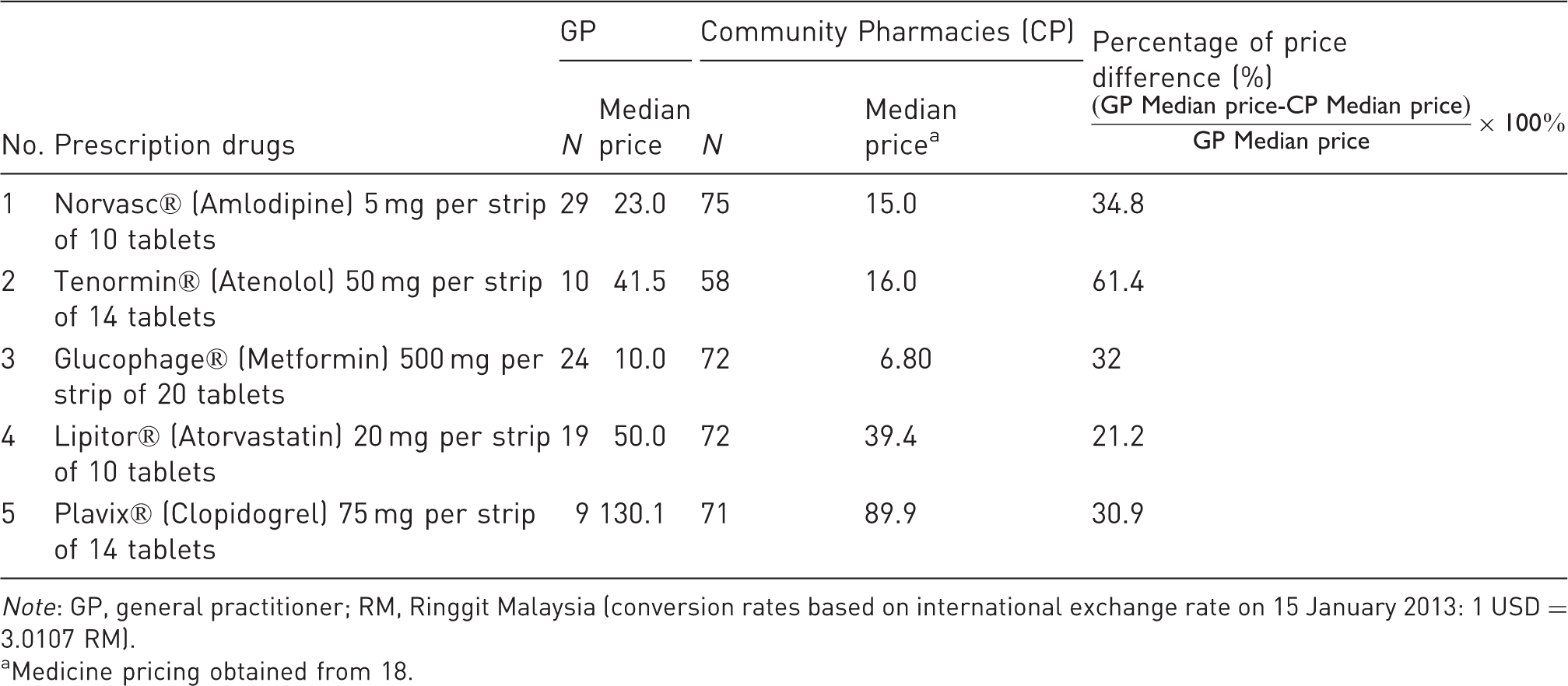
Note: GP, general practitioner; RM, Ringgit Malaysia (conversion rates based on international exchange rate on 15 January 2013: 1 USD = 3.0107 RM).
Medicine pricing obtained from 18.
Comparison of prescription drugs’ pricing procured from GP and RSP obtained by Pharmaceutical Services Division, Ministry of Health Malaysia in year 2011 (RM per tablet)


Note: GP, general practitioner; RSP, retail selling price; RM, Ringgit Malaysia (conversion rates based on international exchange rate on 15 January 2013: 1 USD = 3.0107 RM).
Discussion
Currently, there is no dispensing separation in Malaysia. Dispensing separation is defined as separation between prescribing and dispensing where prescribing activity is done by doctors, while dispensing activity is done by pharmacists. 21 A traditional “dispensing doctors” system in which GPs dispenses medications as a part of their professional practice is still the adopted model in Malaysia. 22 Obviously dispensing doctors have dual roles in prescribing and dispensing medicines to patients. This is because the 1952 Poison Act in Malaysia granted the right for registered medical practitioners to prescribe and dispense medications in their clinics. 23 In other words, GPs and doctors practising in the private sector in Malaysia can diagnose patients and also dispense the medications to them.
This consequence has created an intense competition between retail pharmacies and GPs to gain a share in the pharmaceutical market. 24 This pilot study had shown that almost all of the respondents perceived that community pharmacies have created phenomenon of pharmaceutical price war and were trying to compete price with GPs. This finding is in line with the findings of Hassali et al. study, where the community pharmacist lowers medicine prices in order to attract customers. 5 Gijsbrechts et al. reported that the unhealthy pharmaceutical price war has driven community pharmacy practice into a profit orientated business. 25 From the data obtained, the average medicine prices sold by GPs are more expensive compared to community pharmacies. This finding is in line with the findings of a study conducted by Alabid et al. in Penang, where they reported that the average medical cost for common cold was charged higher by GPs compared to the community pharmacy, with RM 19.02 and RM 14.35, respectively. 13 Hence, the profit margin of medication gained by GPs would be higher compared to the community pharmacies. Similar to our study findings, Chou et al. reported that the dispensing doctors in Taiwan earned huge profits from the types and amounts of drugs dispensed. 26 Surprisingly, community pharmacy sold Tenormin® at extremely low price compared to GPs with 61.4% difference (RM 41.5 vs. RM 16.0, respectively). Taking these observations into consideration, the possibility explanation for low price of Tenormin would be the stock obtained by community pharmacy was from parallel import.27–32 It is usual and normal to have price disparity of 20–30% between the GP and the community pharmacy; however, it would be unacceptable if the price difference reached 61.4% between the two health care services. Thus, the appropriate role of the Malaysian Pharmaceutical Service Division and other regulators in the oversight of the price difference between GPs and community pharmacy is yet to be defined.
In private sector, the difference in pricing of medicine is partly attributed to the different bonus schemes of products offered by pharmaceutical companies to the community pharmacies. Currently, the issue of different bonus schemes offered by pharmaceutical companies is being debated in Malaysia. Pharmaceutical companies often offer cheaper prices or extra quantities of pharmaceutical products if purchased in a bigger volume. 5 In our study, majority of the respondents agreed to have different bonus schemes based on the quantities ordered for pharmaceutical products. In general, pharmaceutical companies often have different bonus schemes to the health care providers as one of their marketing strategy. 33 The inducement to have lower cost of pharmaceutical products has indirectly forced health care providers to purchase pharmaceutical products in bigger quantities. Hence, the chain pharmacies and big health care institutions were able to gain the advantage from this marketing strategy by the pharmaceutical companies. Moreover, within the context of different bonus schemes, pharmaceutical companies also often offer pharmaceutical bonus scheme with different prices for doctors and pharmacists. In fact, the price of medications for the bonus schemes given by the Pharmaceutical companies to the GPs is much cheaper at the mega chains pharmacies. 34 In this study, majority of the respondents agreed to have bonus scheme with different prices for GPs and pharmacists. The intention of pharmaceutical company to have special price of pharmaceutical products to doctors, is to encourage doctors as prescribers to promote their pharmaceutical products. Hence as a business strategy, doctors would take it granted to have lower prices of pharmaceutical products in order to promote it. 34
However, community pharmacist as one of the important component in the health care system was not satisfied with the current scheme offered by pharmaceutical companies. In Malaysia, it is reported that some doctors sold bulk of medicines to the community pharmacy through runner network in order to gain fast profit. 35 Moreover, Hassali et al. revealed that this unfair bonus scheme had led to the development of runner network within pharmaceutical market. 5 In addition, few pharmaceutical companies have taken the initiative to step down some of the rewards to the doctors. 36 In Malaysia, recently there was a campaign slogan: “Say No to Inducement to Medical Prescribers” which was advocated by the Malaysian fraternity of community pharmacists in the year 2013. The main purposes of the campaign are to curtail the unethical practices by pharmaceutical companies and to diminish the advent of runner network which has ruined the pharmaceutical system in terms of product origin. 37
The Malaysian government offered Competition Act 2010 in the year 2010. The act was effective on business practice since 1st January 2012. Malaysia Competition Commission (MyCC) has taken the lead to enhance Its main role is to protect the competitive process for the benefit of businesses practice, consumers welfare and the economy. 38 The Competition Act 2010 prohibited certain abuse of dominant for examples price discrimination. Regarding medicine procurement, majority of respondents emphasized on the quality of medicine and also profit margin as important factors. Quality or profit margin may be germane decision parameters when medications are being prescribed. In fact, the appropriateness of a medicine should have a clear medical benefit and indication for the use rather than the profit margin. 39 While only 35% of the respondents considered the factor of Pharmaceutical companies product bonuses. In addition, healthcare professionals should remove personal gain and profit in the decision making of prescribing medicines. Besides that, most of the doctors (90%) prescribed generic medicine actively in their daily practice. A generic medicine is defined by the World Health Organization (WHO) as “a pharmaceutical product, usually intended to be interchangeable with an innovator product that is manufactured without a licence from the innovator company and marketed after the expiry date of the patent or other exclusive rights.” 40 When a medicine’s patent protection has finished, other pharmaceutical company can produce the same compounds found in the originator product using similar or different process. 41 In line with this report, Alabid et al. reported the same finding that GPs were prescribing more generic medicines. 13 Under Malaysian generic medicines policy in year 2006, Malaysia encourages generic prescribing, generic dispensing, generic substitution and generic medicine use in Malaysia. 42
Conclusion
The findings from this study highlighted that the pharmaceutical price war issue has caused negative impact to the community pharmacies and GPs in Malaysia. In order to preserve the viability of community pharmacies and GPs in the country, the authorities should monitor medicine prices especially at the private sector to ensure affordability and to ensure pricing of medicines are appropriate. In addition, under Malaysian Competition Act 2010, MyCC could play an important role in overcoming the unethical practices by pharmaceutical companies in offering different bonus schemes and price discrimination policy toward community pharmacies and GPs.
Limitations
The low response rate is the main limitation of this study. Nevertheless, this low response rate is relatively similar to previous studies conducted with GPs in private sector in Malaysia.43–45 Hence, generalization of the study finding to whole country is not possible. Moreover, there were a limited number of medicines included in this study. Therefore, the future studies should include more items of medicines to show the full data on pharmaceutical pricing among GPs in the country.
Footnotes
Funding
The authors would like to thank Malaysia Competition Commission (MyCC) for funding this project. This research would not be feasible without the financial support from MyCC Research Grants Programme (RGP).
Conflict of interest
None declared.